- Infertility. CSMU sub-faculty of Obstetrics & Gynecology

Содержание
- 2. Definitions: Infertility is defined as the failure of a couple of reproductive age to conceive after
- 3. Synonyms and related keywords: infertility, lack of pregnancy, fertility, in vitro fertilization, conception problems, pregnancy problems,
- 4. Infertility is considered primary when it occurs in a woman who has never established a pregnancy
- 5. Fertility is defined as the capacity to reproduce or the state of being fertile. This term
- 6. Incidence: Infertility affects approximately 15% of couples of reproductive age. In recent years, there has been
- 7. The origin of infertility is similarly due to male or female factors; the causes are multiple.
- 8. Causes of Male Infertility Low sperm count; normally, men produce at least 20 million sperms per
- 9. Causes of Male Infertility: Poor shape (known as 'morphology'), so that an individual sperm is unable
- 10. Causes of Female Infertility Hormonal disorders; as a result, egg follicles might not grow within the
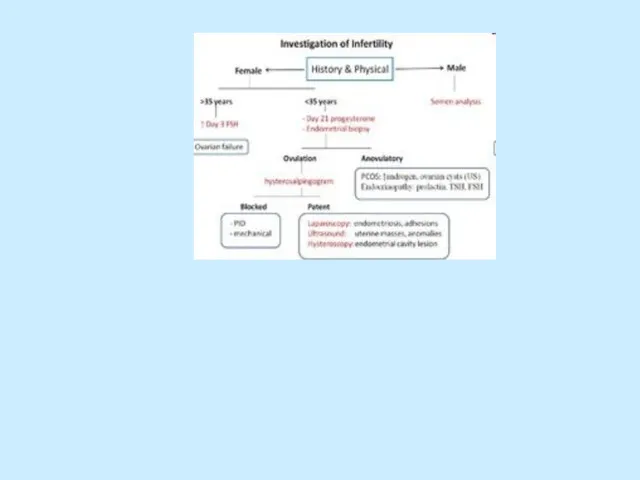
- 11. Evaluation. History and physical examination Semen analysis Sperm–cervical mucus interaction (postcoital testing) Testing for ovulation Evaluation
- 12. History: frequency and timing of intercourse character of menstruation, information regarding to impotence, dyspareunia, the use
- 13. Physical examination BP, PR, body T. Height and weight to calculate the body mass index (body
- 14. Physical examination: The abdominal examination should be directed to the presence of abnormal masses at the
- 15. After the completion of all these steps no abnormality or cause of infertility can be identified
- 16. Gynecological examination Evaluation of hair distribution, clitoris size, Bartholin glands, labia majora and minora, and any
- 17. Gynecological examination The evaluation of the cervix should include a Papanicolau test (Pap smear) and cultures
- 18. Bimanual examination: the direction of the cervix and the size and position of the uterus in
- 19. Pelvic ultrasonographic scan to establish an early diagnosis of adnexal masses; to determine the size and
- 20. Semen analysis The semen sample should be collected after a period of abstinence of at least
- 21. Semen analysis Normal parameters: Volume - 2-5 mL pH - 7.2-7.8 Sperm concentration - 20 million
- 22. Azoospermia - absence of sperm that could be related to congenital absence or bilateral obstruction of
- 23. Asthenozoospermia indicates sperm motility of less than 50%. Extreme temperatures and delayed analysis after sperm collection
- 24. Hypospermia indicates a decrease of semen volume to less than 2 mL per ejaculation. Hyperspermia indicates
- 25. Semen analysis: If abnormalities are present, the patient should be referred to a urologist specializing in
- 26. The postcoital test (PCT or Huhner test) Allows direct analysis of sperm and cervical mucus interaction
- 27. PCT (continuation) A satisfactory test is one in which more than 10 motile spermatozoa are seen
- 28. PCT (continuation) Possible reason of an unsatisfactory test: azospermia (no spermatozoa in ejaculate), poor inherent spermatozoa
- 29. PCT (continuation) Other causes include: - cervical stenosis, - hypoplastic endocervical canal, - coital dysfunction
- 30. PCT (continuation) a finding of 5–10 progressively motile spermatozoa per high-power field and clear acellular mucus
- 31. The sample can also be assessed for pH, mucus cellularity, WBC, ferning.
- 32. Testing for ovulation: 1.measuring a rise in basal body temperature (BBT), 2.identifying an elevation in the
- 33. 1.The basal body temperature (BBT) After ovulation, rising progesterone levels increase the basal temperature by approximately
- 34. 2.Midluteal phase progesterone level Is another test to assess ovulation a concentration greater than 3.0 ng/mL
- 35. 3.Urine LH kits Unlike the rise in BBT and serum progesterone concentrations, which are useful for
- 36. 4.Endometrial biopsy An endometrial biopsy evaluates the response of the endometrium to progesterone. The test is
- 37. Endometrial biopsy (continuation) A luteal phase defect may result from inadequate estrogen priming, progesterone secretion, or
- 38. Evaluation of tubal patency Tubal patency can be evaluated by hysterosalpingography (HSG) and/or by chromopertubation during
- 39. The hysterosalpingogram (HSG): Shows uterine and fallopian tube contour and tubal patency. It is performed in
- 40. Diagnostic laparoscopy: assesses peritoneal and tubal factors (endometriosis and pelvic adhesions)
- 41. Treatment of cervical infertility An abnormal PCT because of chronic cervicitis: doxycycline 100 mg by mouth
- 42. Treatment of uterine factors Congenital absence of the uterus and vagina (Rokitansky-Küster-Hauser syndrome) - surrogate mother
- 43. Tubal factor infertility: tubal cannulation, microsurgical tubocornual reanastomosis, IVF.
- 44. Treatment of anovulation: stimulation of multiple ovarian follicles: clomiphene citrate (CC), human menopausal gonadotropins (hMG), purified
- 45. Clomiphene Citrate (CC) The standard dose of CC is 50 mg PO qd for 5 days,
- 46. Human menopause gonadotropins (hMG) Brand Names: Humegon, Organon, Pergonal, Serono, Repronex contains 75 U of FSH
- 47. Luteal phase defects: intramuscular or intravaginal progesterone until the luteoplacental shift occurs at 8–10 weeks gestational
- 48. Treatment of Hyperprolactinemia: Inducing of ovulation : Bromocriptine in starting dose 2.5 mg each bedtime. CC
- 49. ASSISTED REPRODUCTIVE TECHNOLOGIES: Gamete intrafallopian transfer (GIFT): extraction of oocytes is followed by the transfer of
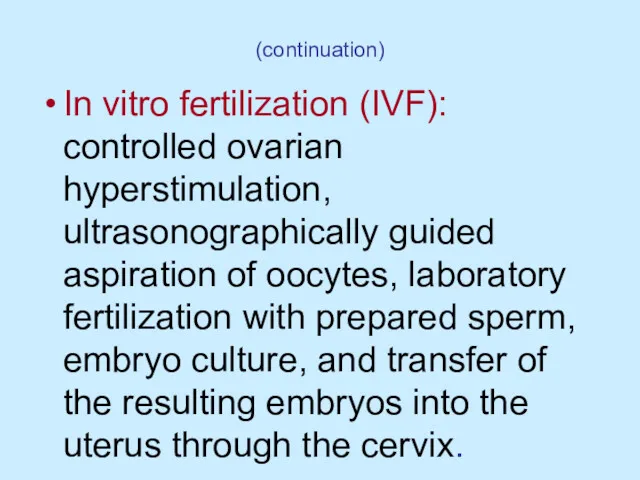
- 50. (continuation) In vitro fertilization (IVF): controlled ovarian hyperstimulation, ultrasonographically guided aspiration of oocytes, laboratory fertilization with
- 51. A mature, unfertilized egg.
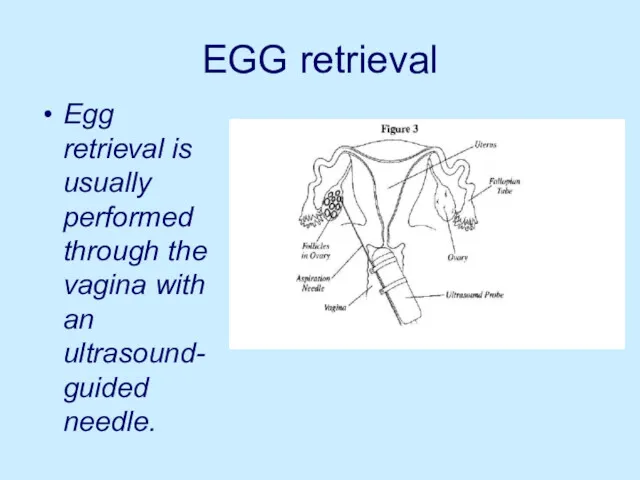
- 52. EGG retrieval Egg retrieval is usually performed through the vagina with an ultrasound-guided needle.
- 53. A fertilized egg that has divided once and is now a two-cell embryo.
- 54. Embryo transfer is performed through the cervix.
- 55. Indications for in vitro fertilization: Tubal conditions Endometriosis Unexplained infertility Male factor infertility Uterine malformations
- 56. ASSISTED REPRODUCTIVE TECHNOLOGIES (continuation) intracytoplasmic sperm injection: single spermatozoon is injected into each oocyte, and the
- 57. Intracytoplasmic sperm injection
- 58. Indications for Intracytoplasmic Sperm Injection Very low numbers of motile sperm. Severe teratospermia. Problems with sperm
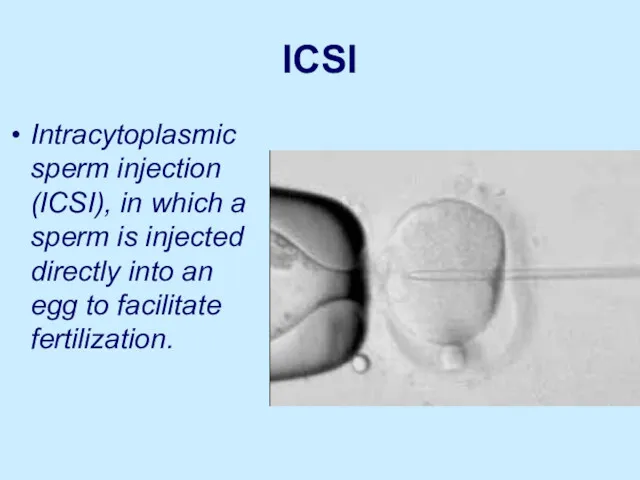
- 59. ICSI Intracytoplasmic sperm injection (ICSI), in which a sperm is injected directly into an egg to
- 60. ICSI involves injecting sperm directly into the egg
- 61. Controlled ovarian hyperstimulation (protocol): CC is given on days 5–9 of the menstrual cycle in dose
- 62. Controlled ovarian hyperstimulation (continuation): CC/hMG combinations - The hMG is given for 2–7 days after the
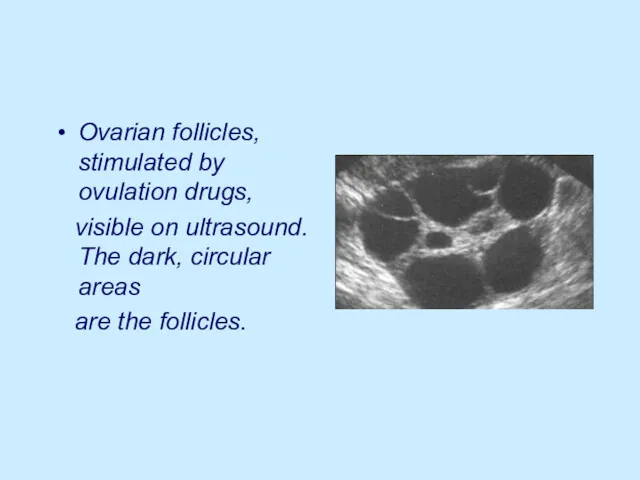
- 63. Ovarian follicles, stimulated by ovulation drugs, visible on ultrasound. The dark, circular areas are the follicles.
- 67. Скачать презентацию
Definitions:
Infertility is defined as the failure of a couple of
Definitions:
Infertility is defined as the failure of a couple of
Synonyms and related keywords:
infertility, lack of pregnancy, fertility, in vitro fertilization,
Synonyms and related keywords:
infertility, lack of pregnancy, fertility, in vitro fertilization,
Infertility is considered primary when it occurs in a woman who
Infertility is considered primary when it occurs in a woman who
Fertility is defined as the capacity to reproduce or the
Fertility is defined as the capacity to reproduce or the
Incidence:
Infertility affects approximately 15% of couples of reproductive age. In recent
Incidence:
Infertility affects approximately 15% of couples of reproductive age. In recent
The origin of infertility is similarly due to male or
The origin of infertility is similarly due to male or
Causes of Male Infertility
Low sperm count; normally, men produce at least
Causes of Male Infertility
Low sperm count; normally, men produce at least
Causes of Male Infertility:
Poor shape (known as 'morphology'), so that an
Causes of Male Infertility:
Poor shape (known as 'morphology'), so that an
Causes of Female Infertility
Hormonal disorders; as a result, egg follicles
Causes of Female Infertility
Hormonal disorders; as a result, egg follicles
Evaluation.
History and physical examination
Semen analysis
Sperm–cervical mucus interaction (postcoital testing)
Testing for
Evaluation.
History and physical examination
Semen analysis
Sperm–cervical mucus interaction (postcoital testing)
Testing for
History:
frequency and timing of intercourse
character of menstruation,
information regarding to impotence,
History:
frequency and timing of intercourse
character of menstruation,
information regarding to impotence,
Physical examination
BP, PR, body T.
Height and weight to calculate the body
Physical examination
BP, PR, body T.
Height and weight to calculate the body
Physical examination:
The abdominal examination should be directed to the presence of
Physical examination:
The abdominal examination should be directed to the presence of
After the completion of all these steps no abnormality
After the completion of all these steps no abnormality
Gynecological examination
Evaluation of hair distribution, clitoris size, Bartholin glands, labia
Gynecological examination
Evaluation of hair distribution, clitoris size, Bartholin glands, labia
Gynecological examination
The evaluation of the cervix should include a Papanicolau
Gynecological examination
The evaluation of the cervix should include a Papanicolau
Bimanual examination:
the direction of the cervix and the size and position
Bimanual examination:
the direction of the cervix and the size and position
Pelvic ultrasonographic scan
to establish an early diagnosis of adnexal masses; to
Pelvic ultrasonographic scan
to establish an early diagnosis of adnexal masses; to
Semen analysis
The semen sample should be collected after a period
Semen analysis
The semen sample should be collected after a period
Semen analysis
Normal parameters:
Volume - 2-5 mL
pH - 7.2-7.8
Sperm concentration
Semen analysis
Normal parameters:
Volume - 2-5 mL
pH - 7.2-7.8
Sperm concentration
Azoospermia - absence of sperm that could be related to congenital
Azoospermia - absence of sperm that could be related to congenital
Asthenozoospermia indicates sperm motility of less than 50%. Extreme temperatures and
Asthenozoospermia indicates sperm motility of less than 50%. Extreme temperatures and
Hypospermia indicates a decrease of semen volume to less than 2
Hypospermia indicates a decrease of semen volume to less than 2
Semen analysis:
If abnormalities are present, the patient should be referred
Semen analysis:
If abnormalities are present, the patient should be referred
The postcoital test (PCT or Huhner test)
Allows direct analysis of
The postcoital test (PCT or Huhner test)
Allows direct analysis of
PCT (continuation)
A satisfactory test is one in which more than 10
PCT (continuation)
A satisfactory test is one in which more than 10
PCT (continuation)
Possible reason of an unsatisfactory test:
azospermia (no spermatozoa in ejaculate),
poor
PCT (continuation)
Possible reason of an unsatisfactory test:
azospermia (no spermatozoa in ejaculate),
poor
PCT (continuation)
Other causes include:
- cervical stenosis,
- hypoplastic endocervical
PCT (continuation)
Other causes include:
- cervical stenosis,
- hypoplastic endocervical
PCT (continuation)
a finding of 5–10 progressively motile spermatozoa per high-power field
PCT (continuation)
a finding of 5–10 progressively motile spermatozoa per high-power field
The sample can also be assessed for pH, mucus cellularity,
The sample can also be assessed for pH, mucus cellularity,
Testing for ovulation:
1.measuring a rise in basal body temperature (BBT),
2.identifying
Testing for ovulation:
1.measuring a rise in basal body temperature (BBT),
2.identifying
1.The basal body temperature (BBT)
After ovulation, rising progesterone levels increase
1.The basal body temperature (BBT)
After ovulation, rising progesterone levels increase
2.Midluteal phase progesterone level
Is another test to assess ovulation
a concentration
2.Midluteal phase progesterone level
Is another test to assess ovulation
a concentration
3.Urine LH kits
Unlike the rise in BBT and serum progesterone
3.Urine LH kits
Unlike the rise in BBT and serum progesterone
4.Endometrial biopsy
An endometrial biopsy evaluates the response of the endometrium
4.Endometrial biopsy
An endometrial biopsy evaluates the response of the endometrium
Endometrial biopsy (continuation)
A luteal phase defect may result from inadequate estrogen
Endometrial biopsy (continuation)
A luteal phase defect may result from inadequate estrogen
Evaluation of tubal patency
Tubal patency can be evaluated by hysterosalpingography (HSG)
Evaluation of tubal patency
Tubal patency can be evaluated by hysterosalpingography (HSG)
The hysterosalpingogram (HSG):
Shows uterine and fallopian tube contour and tubal
The hysterosalpingogram (HSG):
Shows uterine and fallopian tube contour and tubal
Diagnostic laparoscopy:
assesses peritoneal and tubal factors (endometriosis and pelvic adhesions)
Diagnostic laparoscopy:
assesses peritoneal and tubal factors (endometriosis and pelvic adhesions)
Treatment of cervical infertility
An abnormal PCT because of chronic cervicitis: doxycycline
Treatment of cervical infertility
An abnormal PCT because of chronic cervicitis: doxycycline
Treatment of uterine factors
Congenital absence of the uterus and vagina (Rokitansky-Küster-Hauser
Treatment of uterine factors
Congenital absence of the uterus and vagina (Rokitansky-Küster-Hauser
Tubal factor infertility:
tubal cannulation,
microsurgical tubocornual reanastomosis,
IVF.
Tubal factor infertility:
tubal cannulation,
microsurgical tubocornual reanastomosis,
IVF.
Treatment of anovulation:
stimulation of multiple ovarian follicles:
clomiphene citrate
Treatment of anovulation:
stimulation of multiple ovarian follicles:
clomiphene citrate
Clomiphene Citrate (CC)
The standard dose of CC is 50 mg PO
Clomiphene Citrate (CC)
The standard dose of CC is 50 mg PO
Human menopause gonadotropins (hMG)
Brand Names: Humegon, Organon, Pergonal, Serono, Repronex
contains
Human menopause gonadotropins (hMG)
Brand Names: Humegon, Organon, Pergonal, Serono, Repronex
contains
Luteal phase defects:
intramuscular or intravaginal progesterone until the luteoplacental shift occurs
Luteal phase defects:
intramuscular or intravaginal progesterone until the luteoplacental shift occurs
Treatment of Hyperprolactinemia:
Inducing of ovulation : Bromocriptine in starting dose
Treatment of Hyperprolactinemia:
Inducing of ovulation : Bromocriptine in starting dose
ASSISTED REPRODUCTIVE TECHNOLOGIES:
Gamete intrafallopian transfer (GIFT): extraction of oocytes is
ASSISTED REPRODUCTIVE TECHNOLOGIES:
Gamete intrafallopian transfer (GIFT): extraction of oocytes is
(continuation)
In vitro fertilization (IVF): controlled ovarian hyperstimulation, ultrasonographically guided aspiration of
(continuation)
In vitro fertilization (IVF): controlled ovarian hyperstimulation, ultrasonographically guided aspiration of
A mature, unfertilized egg.
A mature, unfertilized egg.
EGG retrieval
Egg retrieval is usually performed through the vagina with an
EGG retrieval
Egg retrieval is usually performed through the vagina with an
A fertilized egg that has divided once and is now a
A fertilized egg that has divided once and is now a
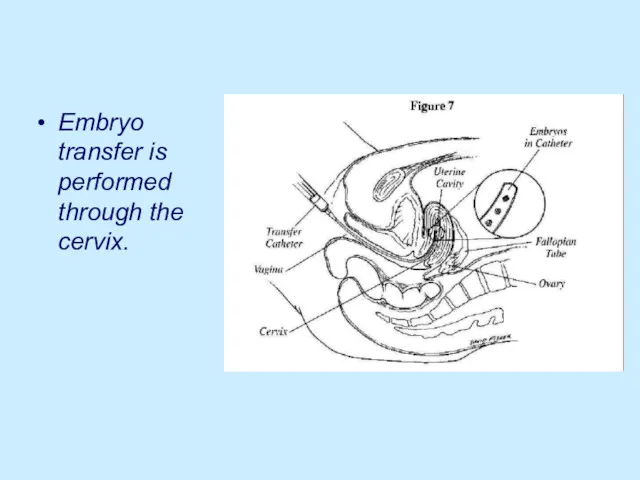
Embryo transfer is performed through the cervix.
Embryo transfer is performed through the cervix.
Indications for in vitro fertilization:
Tubal conditions
Endometriosis
Unexplained infertility
Male
Indications for in vitro fertilization:
Tubal conditions
Endometriosis
Unexplained infertility
Male
ASSISTED REPRODUCTIVE TECHNOLOGIES (continuation)
intracytoplasmic sperm injection: single spermatozoon is injected into
ASSISTED REPRODUCTIVE TECHNOLOGIES (continuation)
intracytoplasmic sperm injection: single spermatozoon is injected into
Intracytoplasmic sperm injection
Intracytoplasmic sperm injection
Indications for Intracytoplasmic Sperm Injection
Very low numbers of motile sperm.
Severe teratospermia.
Problems
Indications for Intracytoplasmic Sperm Injection
Very low numbers of motile sperm.
Severe teratospermia.
Problems
ICSI
Intracytoplasmic sperm injection (ICSI), in which a sperm is injected directly
ICSI
Intracytoplasmic sperm injection (ICSI), in which a sperm is injected directly
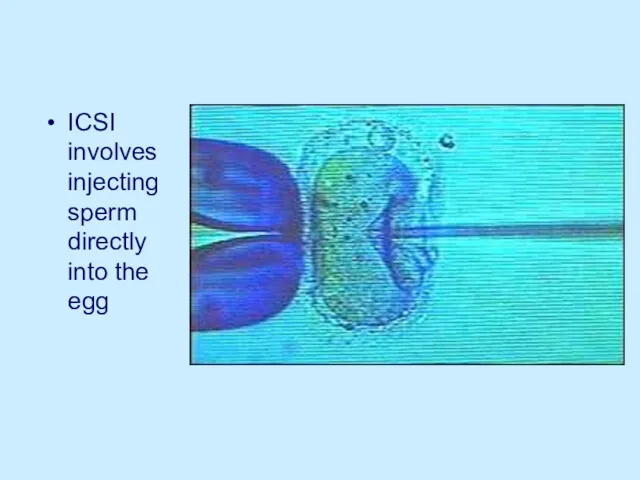
ICSI involves injecting sperm directly into the egg
ICSI involves injecting sperm directly into the egg
Controlled ovarian hyperstimulation (protocol):
CC is given on days 5–9 of
Controlled ovarian hyperstimulation (protocol):
CC is given on days 5–9 of
Controlled ovarian hyperstimulation (continuation):
CC/hMG combinations - The hMG is given for
Controlled ovarian hyperstimulation (continuation):
CC/hMG combinations - The hMG is given for
Ovarian follicles, stimulated by ovulation drugs,
visible on ultrasound. The dark,
Ovarian follicles, stimulated by ovulation drugs,
visible on ultrasound. The dark,
 Породы домашних животных
Породы домашних животных Эволюция человека
Эволюция человека презентация Углеводы. Липиды
презентация Углеводы. Липиды Собака породы Джек Рассел Терьер
Собака породы Джек Рассел Терьер Краткая история развития биологии. Методы исследования биологии
Краткая история развития биологии. Методы исследования биологии Необычные рыбы
Необычные рыбы Сообщество, биоценоз, биогеоценоз , экосистема, биотоп
Сообщество, биоценоз, биогеоценоз , экосистема, биотоп Система растений и животных — отображение эволюции
Система растений и животных — отображение эволюции презентация Венерические заболевания
презентация Венерические заболевания Железы внутренней и смешанной секреции
Железы внутренней и смешанной секреции Растительность Приморского края
Растительность Приморского края Весна
Весна Зрение. Чтобы видеть, нам нужен свет
Зрение. Чтобы видеть, нам нужен свет Тип Членистоногие
Тип Членистоногие Особенности растений семейства Крестоцветные
Особенности растений семейства Крестоцветные Вегетативная нервная система в норме и патологии
Вегетативная нервная система в норме и патологии Сезім мүшелері Тері
Сезім мүшелері Тері Лягушка. Чудесное превращение
Лягушка. Чудесное превращение Физиология системы выделения. Почки
Физиология системы выделения. Почки Оценка заданий ОГЭ по биологии с развёрнутым ответом
Оценка заданий ОГЭ по биологии с развёрнутым ответом Семейство Кошачьи
Семейство Кошачьи Идентификационные признаки семейства окуневых рыб
Идентификационные признаки семейства окуневых рыб Дистанционное обучение. Презентация: Законы Г. Менделя.
Дистанционное обучение. Презентация: Законы Г. Менделя. Водоросли – низшие растения
Водоросли – низшие растения Роль минеральных веществ в жизнедеятельности клетки
Роль минеральных веществ в жизнедеятельности клетки Бионика и биотехнология
Бионика и биотехнология Размножение, его виды. Бесполое размножение
Размножение, его виды. Бесполое размножение Поняття мікроеволюції
Поняття мікроеволюції