- Bacteria – the causative agents of respiratory tract diseases

Содержание
- 2. DIPHTHERIA Is acute infectious disease caused by Corynebacterium diphtheriae and characterized by a primary lesion, usually
- 3. DIPHTHERIA The disease was first described in the 5th century BC by Hippocrates. The bacteria was
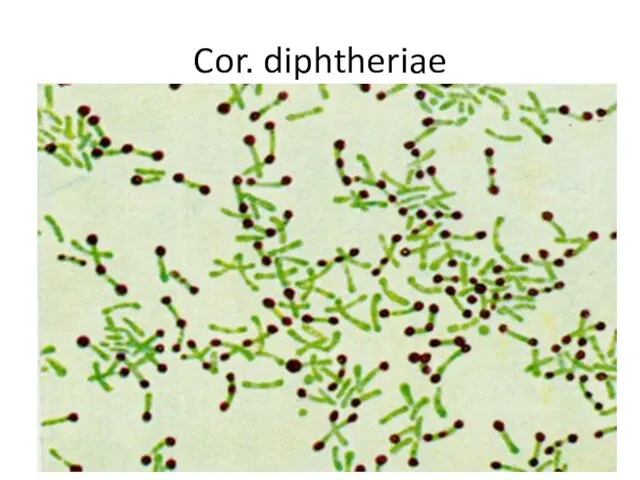
- 4. Cor. diphtheriae
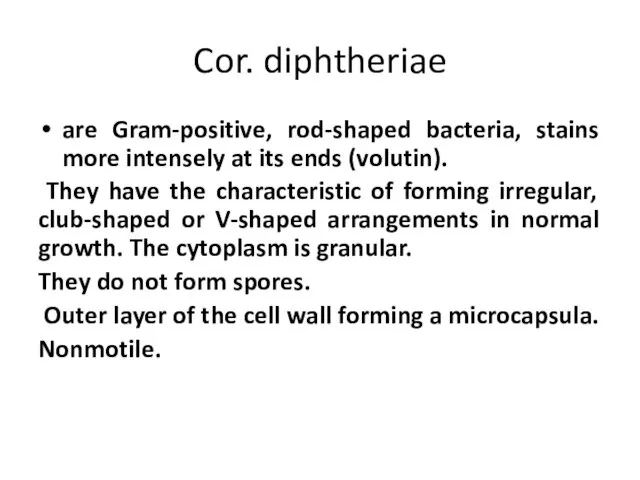
- 5. Cor. diphtheriae are Gram-positive, rod-shaped bacteria, stains more intensely at its ends (volutin). They have the
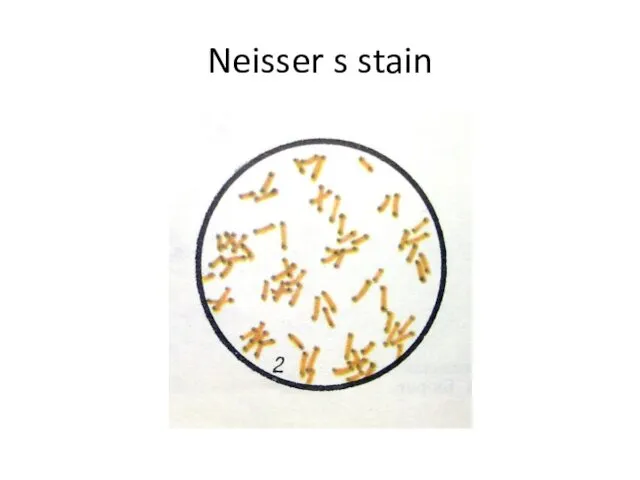
- 6. Neisser s stain
- 7. C. diphtheriae is a gram-positive, non-motile rods or somewhat pleomorphic organism. The club-shaped forms are long
- 8. Physiology of Cor. diphtheriae Aerobes or facultative anaerobes T opt = 37º C Grows readily on
- 9. C. diphtheriae grows much more readily on coagulated serum agar, on whose slope there is a
- 10. Physiology of Cor. diphtheriae Glucose «+» Do not coagulate milk Do not break down urea Indol
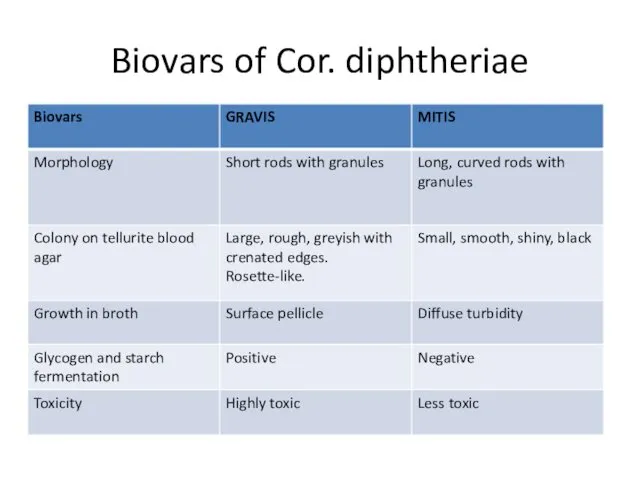
- 11. Biovars of Cor. diphtheriae
- 12. Tellurite agar Gravis Mitis
- 13. The gravis type form relatively large, grayish flat, rough colonies with radial lines and a wavy
- 14. Antigens K – antigen , type specific, thermolabile, surface protein. O – antigen , group specific,
- 15. Resistance Cor. diphtheriae are relatively resistant to harmful environmental factors. They survive for 1 year on
- 16. Diphtheria toxin Is a protein with 2 subunits: A – have enzymatic activity B- is responsible
- 17. Diphtheria toxin The toxigenicity of the Cor. diphtheriae depends on the presence in it of corynephages
- 18. Diphtheria toxin
- 19. Virulence Factors and Pathogenesis of Diphtheria The serious effects of diphtheria in man are caused by
- 20. DIPHTHERIA Sources of infection are patients and carriers. The disease is transmitted by an air-droplet route.
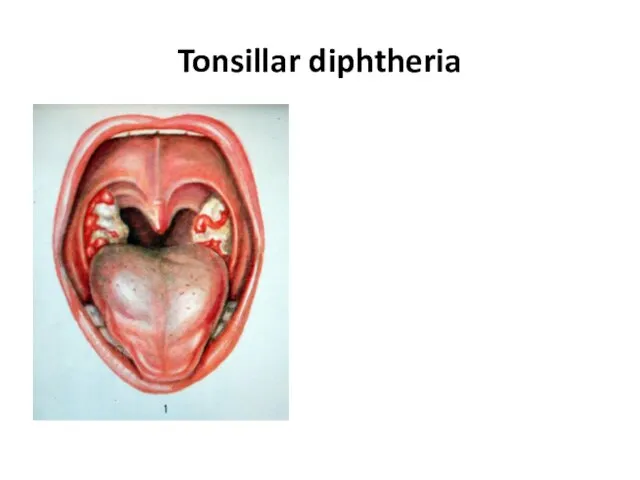
- 21. Diphtheria. Clinical Manifestations The typical membrane on the throat or on other parts of the body,
- 22. Clinical forms 1. Anterior nasal diphtheria, in which the membrane appears inside the nostrils. Almost no
- 23. Tonsillar diphtheria
- 24. Clinical forms 4. Laryngeal diphtheria - usually resulting from the spread of the infection downward from
- 25. Diphtheria. Microbiological Diagnosis SPECIMENS. Swabs from the nose, throat, or other suspected lesions must be obtained.
- 26. Diphtheria. Microbiological Diagnosis Bacterioscopical examination Preparation of smears (Gram and Neisser staining) - Gram-positive rods. The
- 27. Diphtheria. Microbiological Diagnosis Bacteriological examination 1. Inoculation of blood- tellurite agar (Klauberg medium) 2. Subculture on
- 28. Diphtheria. Treatment and Prevention Only diphtheria antitoxin can neutralize diphtheria exotoxin, and it can do so
- 29. Diphtheria toxoid (for stimulating antitoxin production) AB – tetracycline, erythromycin antitoxin
- 30. Pertussis-diphtheria vaccine Diphtheria toxoid Pertussis-diphtheria-tetanus vaccine
- 32. The genus Mycobacterium belongs to the family Mycobacteriaceae. Mycobacterium contains about 50 species that are normally
- 44. The cell wall is more complex than in any other bacterium. It is characterized by a
- 50. Tuberculosis. Clinical Manifestations The initial lesion of tuberculosis occurs at the site of implantation of the
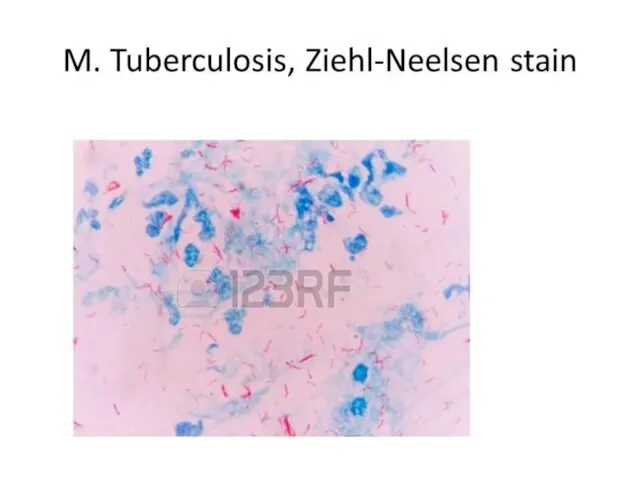
- 51. Tuberculosis. Microbiological Diagnosis SPECIMENS. Sputum should be collected into sterile wide-mouthed, screw-capped glass or plastic pots.
- 52. Tuberculosis. Microbiological Diagnosis PCR. The polymerase chain reaction should provide an extremely specific, sensitive, and rapid
- 53. Tuberculosis. Microbiological Diagnosis BACTERIOLOGICAL EXAMINATION. As tubercle bacilli grow very slowly, they are readily overgrown by
- 54. Tuberculosis. Microbiological Diagnosis PRICE METHOD. This is the rapid technique of the bacteriological diagnosis of tuberculosis.
- 55. Tuberculosis. Microbiological Diagnosis ALLERGIC SKIN TEST (the Mantoux test). In the Mantoux test, tuberculin, the solution
- 56. Tuberculosis. Microbiological Diagnosis SEROLOGICAL EXAMINATION. The immune response in tuberculosis is predominantly cell-mediated, and detection of
- 57. The three key first-line drugs used for previously untreated patients are isoniazid, rifampicin, and pyrazinamide. Ethambutol
- 61. Скачать презентацию
DIPHTHERIA
Is acute infectious disease caused by Corynebacterium diphtheriae and characterized by
DIPHTHERIA
Is acute infectious disease caused by Corynebacterium diphtheriae and characterized by
DIPHTHERIA
The disease was first described in the 5th century BC by Hippocrates.
DIPHTHERIA
The disease was first described in the 5th century BC by Hippocrates.
Cor. diphtheriae
Cor. diphtheriae
Cor. diphtheriae
are Gram-positive, rod-shaped bacteria, stains more intensely at its ends
Cor. diphtheriae
are Gram-positive, rod-shaped bacteria, stains more intensely at its ends
Neisser s stain
Neisser s stain
C. diphtheriae is a gram-positive, non-motile rods or somewhat pleomorphic organism.
C. diphtheriae is a gram-positive, non-motile rods or somewhat pleomorphic organism.
Physiology of Cor. diphtheriae
Aerobes or facultative anaerobes
T opt = 37º C
Grows
Physiology of Cor. diphtheriae
Aerobes or facultative anaerobes
T opt = 37º C
Grows
C. diphtheriae grows much more readily on coagulated serum agar, on
C. diphtheriae grows much more readily on coagulated serum agar, on
Physiology of Cor. diphtheriae
Glucose «+»
Do not coagulate milk
Do not break down
Physiology of Cor. diphtheriae
Glucose «+»
Do not coagulate milk
Do not break down
Biovars of Cor. diphtheriae
Biovars of Cor. diphtheriae

Tellurite agar
Gravis
Mitis
Tellurite agar
Gravis
Mitis
The gravis type form relatively large, grayish flat, rough colonies with
The gravis type form relatively large, grayish flat, rough colonies with
Antigens
K – antigen , type specific, thermolabile, surface protein.
O – antigen
Antigens
K – antigen , type specific, thermolabile, surface protein.
O – antigen
Resistance
Cor. diphtheriae are relatively resistant to harmful environmental factors.
They survive for
Resistance
Cor. diphtheriae are relatively resistant to harmful environmental factors.
They survive for
Diphtheria toxin
Is a protein with 2 subunits:
A – have enzymatic
Diphtheria toxin
Is a protein with 2 subunits:
A – have enzymatic
Diphtheria toxin
The toxigenicity of the Cor. diphtheriae depends on the
Diphtheria toxin
The toxigenicity of the Cor. diphtheriae depends on the
Diphtheria toxin
Diphtheria toxin
Virulence Factors and Pathogenesis of Diphtheria The serious effects of diphtheria
Virulence Factors and Pathogenesis of Diphtheria The serious effects of diphtheria
DIPHTHERIA
Sources of infection are patients and carriers.
The disease is transmitted by
DIPHTHERIA
Sources of infection are patients and carriers.
The disease is transmitted by
Diphtheria. Clinical Manifestations
The typical membrane on the throat or on
Diphtheria. Clinical Manifestations
The typical membrane on the throat or on
Clinical forms
1. Anterior nasal diphtheria, in which the membrane appears inside
Clinical forms
1. Anterior nasal diphtheria, in which the membrane appears inside
Tonsillar diphtheria
Tonsillar diphtheria
Clinical forms
4. Laryngeal diphtheria - usually resulting from the spread of
Clinical forms
4. Laryngeal diphtheria - usually resulting from the spread of

Diphtheria. Microbiological Diagnosis
SPECIMENS. Swabs from the nose, throat, or other suspected
Diphtheria. Microbiological Diagnosis
SPECIMENS. Swabs from the nose, throat, or other suspected
Diphtheria. Microbiological Diagnosis
Bacterioscopical examination
Preparation of smears (Gram and Neisser staining) -
Diphtheria. Microbiological Diagnosis
Bacterioscopical examination
Preparation of smears (Gram and Neisser staining) -
Diphtheria. Microbiological Diagnosis
Bacteriological examination
1. Inoculation of blood- tellurite agar (Klauberg
Diphtheria. Microbiological Diagnosis
Bacteriological examination
1. Inoculation of blood- tellurite agar (Klauberg
Diphtheria. Treatment and Prevention
Only diphtheria antitoxin can neutralize diphtheria exotoxin, and
Diphtheria. Treatment and Prevention
Only diphtheria antitoxin can neutralize diphtheria exotoxin, and
Diphtheria toxoid (for stimulating antitoxin production)
AB – tetracycline, erythromycin
antitoxin
Diphtheria toxoid (for stimulating antitoxin production)
AB – tetracycline, erythromycin
antitoxin
Pertussis-diphtheria vaccine
Diphtheria toxoid
Pertussis-diphtheria-tetanus vaccine
Pertussis-diphtheria vaccine
Diphtheria toxoid
Pertussis-diphtheria-tetanus vaccine
The genus Mycobacterium belongs to the family Mycobacteriaceae. Mycobacterium contains about
The genus Mycobacterium belongs to the family Mycobacteriaceae. Mycobacterium contains about

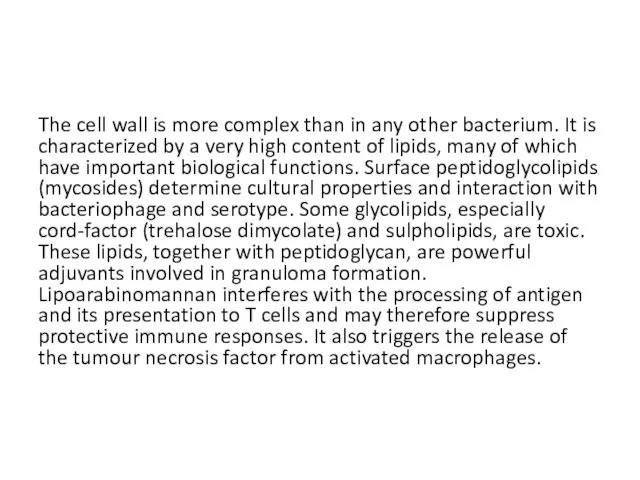
The cell wall is more complex than in any other bacterium.
The cell wall is more complex than in any other bacterium.
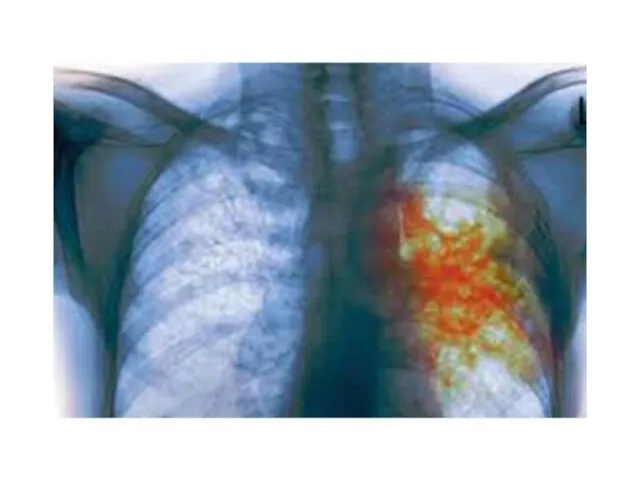
Tuberculosis. Clinical Manifestations
The initial lesion of tuberculosis occurs at the site
Tuberculosis. Clinical Manifestations
The initial lesion of tuberculosis occurs at the site
Tuberculosis. Microbiological Diagnosis
SPECIMENS. Sputum should be collected into sterile wide-mouthed, screw-capped
Tuberculosis. Microbiological Diagnosis
SPECIMENS. Sputum should be collected into sterile wide-mouthed, screw-capped
Tuberculosis. Microbiological Diagnosis
PCR. The polymerase chain reaction should provide an extremely
Tuberculosis. Microbiological Diagnosis
PCR. The polymerase chain reaction should provide an extremely
Tuberculosis. Microbiological Diagnosis
BACTERIOLOGICAL EXAMINATION. As tubercle bacilli grow very slowly, they
Tuberculosis. Microbiological Diagnosis
BACTERIOLOGICAL EXAMINATION. As tubercle bacilli grow very slowly, they
Tuberculosis. Microbiological Diagnosis
PRICE METHOD. This is the rapid technique of the
Tuberculosis. Microbiological Diagnosis
PRICE METHOD. This is the rapid technique of the
Tuberculosis. Microbiological Diagnosis
ALLERGIC SKIN TEST (the Mantoux test). In the Mantoux
Tuberculosis. Microbiological Diagnosis
ALLERGIC SKIN TEST (the Mantoux test). In the Mantoux
Tuberculosis. Microbiological Diagnosis
SEROLOGICAL EXAMINATION. The immune response in tuberculosis is predominantly
Tuberculosis. Microbiological Diagnosis
SEROLOGICAL EXAMINATION. The immune response in tuberculosis is predominantly
The three key first-line drugs used for previously untreated patients are
The three key first-line drugs used for previously untreated patients are

 ЕГЭ по истории. Лекции IX – XV века
ЕГЭ по истории. Лекции IX – XV века Проект Московская творческая интеллигенция в дни Великой Отечественной Войны
Проект Московская творческая интеллигенция в дни Великой Отечественной Войны Калмыки в XVII – XVIII вв
Калмыки в XVII – XVIII вв Постиндустриальное общество в странах запада
Постиндустриальное общество в странах запада Страны Запада в 20-х годах
Страны Запада в 20-х годах Формирование Древнерусского государства
Формирование Древнерусского государства Подготовка к сочинению Путешествие на поле славы
Подготовка к сочинению Путешествие на поле славы Каролингская империя
Каролингская империя Становление древнерусского государства
Становление древнерусского государства Русь в период монгольского вторжения и нашествия крестоносцев в XIII веке
Русь в период монгольского вторжения и нашествия крестоносцев в XIII веке Внешняя политика России в 1725-1762 годы
Внешняя политика России в 1725-1762 годы корен.перелом1942-1943
корен.перелом1942-1943 Тест по теме : Образование славянских государств.
Тест по теме : Образование славянских государств. Волгоград - Сталинград - город-герой
Волгоград - Сталинград - город-герой Советская культура в конце 1920-х – начале 1930-х гг. Культурная революция
Советская культура в конце 1920-х – начале 1930-х гг. Культурная революция Казахское ханство в период правления хана Тауке
Казахское ханство в период правления хана Тауке Урок в 5 классе Вавилонский царь Хаммурапи и его законы
Урок в 5 классе Вавилонский царь Хаммурапи и его законы Московские приказы
Московские приказы Аркаим. Укреплённое поселение эпохи средней бронзы рубежа III—II тыс. до н. э
Аркаим. Укреплённое поселение эпохи средней бронзы рубежа III—II тыс. до н. э Новолипецкий металлургический комбинат в годы войны
Новолипецкий металлургический комбинат в годы войны Формирование территории России
Формирование территории России Животные на войне
Животные на войне Отмена крепостного права
Отмена крепостного права Город Курск
Город Курск Цена Великой Победы. Московское сражение
Цена Великой Победы. Московское сражение Боги Древней Греции
Боги Древней Греции Одетые камнем внеклассное мероприятие к дню Сталинградской битве.
Одетые камнем внеклассное мероприятие к дню Сталинградской битве. СССР в 1953-1964 гг. (тест)
СССР в 1953-1964 гг. (тест)