- An overview of PNH: Pathophysiology, New Diagnostic Guidelines and EQA

Содержание
- 2. Paroxysmal Nocturnal Haemoglobinuria Clinical aspects of PNH New ICCS Guidelines EQA and PNH testing
- 3. Incidence and Prevalence of PNH in Britain Yorkshire population 3,742,835 (2001 census) Incidence 1.3/ million/ year
- 4. PNH – Triad of Clinical Features Haemoglobinuria Intravascular haemolysis ? disabling symptoms abdominal pain dysphagia erectile
- 5. Proteins Deficient from PNH Blood Cells CD59, CD90, CD109 CD55 CD58 CD59 CD48 CD52 PrPc CD16
- 6. Why does PNH occur? PNH clones Lack complement regulatory molecules and therefore probably “weakened” Have no
- 7. Relative Growth Advantage in PNH Normal stem cells GPI-deficient (PNH) stem cells
- 8. Relative Growth Advantage in PNH
- 9. Relative Growth Advantage in PNH
- 10. Relative Growth Advantage in PNH
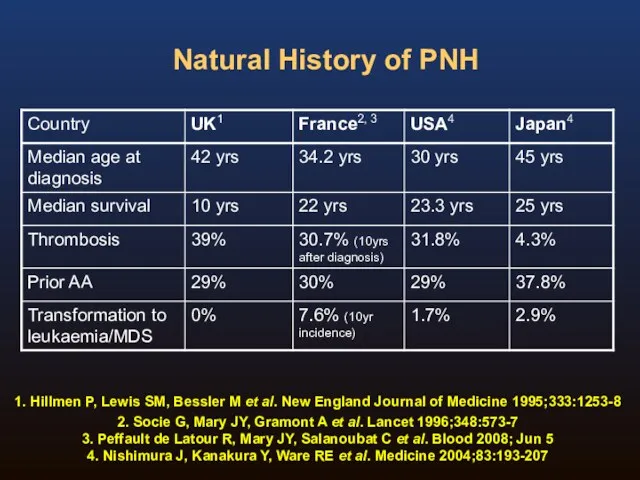
- 11. Natural History of PNH Four publications detailing four groups on the natural history of the disease:
- 12. Natural History of PNH 1. Hillmen P, Lewis SM, Bessler M et al. New England Journal
- 13. Paroxysmal Nocturnal Haemoglobinuria: A Chronic Disabling and Life-Threatening Disease (1,2) Estimated 4,000 – 6,000 patients in
- 14. Normal red blood cells are protected from complement attack by a shield of terminal complement inhibitors
- 15. Symptoms and relationship to nitric oxide scavenging Dysphagia, abdominal pain & erectile failure completely resolved during
- 16. Haemolysis and Nitric Oxide Red blood cell destruction during haemolysis releases cell-free haemoglobin (1) Cell-free haemoglobin
- 17. Chronic Haemolysis is the Underlying Cause of Progressive Morbidities and Mortality of PNH (1-5) Fatigue /
- 18. Renal Damage in PNH Chronic haemolysis and cell-free plasma haemoglobin lead to chronic kidney disease in
- 19. Budd-Chiari syndrome Superior Sagittal Sinus Thrombosis Classical sites of venous thrombosis in PNH
- 20. PNH Clone Size and Thrombosis (excluding warfarin prophylaxis patients) Hall C et al. Blood 2003;102(10):3587-3591. 0
- 21. Laboratory Investigation of PNH Flow cytometry immunophenotyping is the method of choice for PNH testing Diagnosis
- 22. Background In 2008 the Clinical Cytometry Society sponsored a workshop on PNH testing Approximately 100 attendees
- 23. The disease is rare and most labs have limited experience in PNH testing Clinical documents have
- 24. Consensus Committee Michael J Borowitz, MD, PhD Johns Hopkins Fiona E Craig, MD University of Pittsburgh
- 25. ICCS PNH Testing Guidelines Borowitz M, Craig F, DiGiuseppe J, Illingworth A, Rosse W, Sutherland R,
- 26. Recommendations in the ICCS PNH Testing Guidelines Document Recommendations tried to strike a balance between the
- 27. Contents Of The Document Rationale and History Clinical Indications Methodology Routine testing High sensitivity testing RBC
- 28. Methodology Sample issues Comparison of RBC and WBC testing Reagents Analytical approaches Routine vs high sensitivity
- 29. Red Cell Analysis: Routine testing ADVANTAGES Relatively straightforward Best way to identify Type II cells RBC
- 30. Routine Red Cell Analysis: Reagents For historical reasons, CD55 and CD59 are most commonly used CD59
- 31. Red cell testing CD58PE CD55 PE CD55 PE CD59 Fitc CD59 PE CD59 Fitc
- 32. Leucocyte Analysis: Routine testing Granulocyte PNH clone probably gives most accurate estimate of PNH clone size
- 33. Leucocyte Analysis: Reagents CD55 and CD59 were used historically but these are not optimal CD16, CD66b,
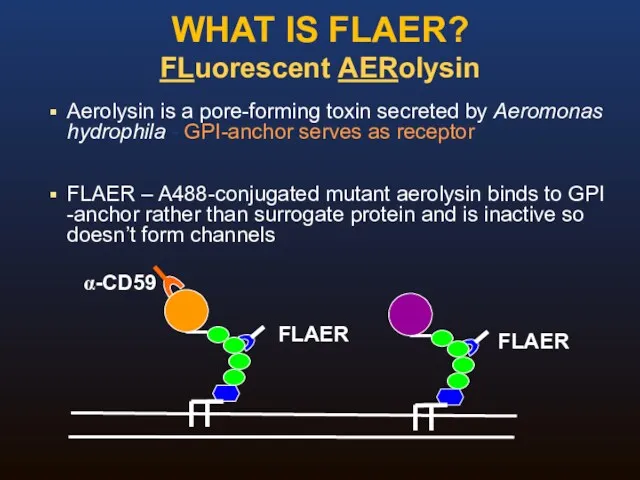
- 34. WHAT IS FLAER? FLuorescent AERolysin Aerolysin is a pore-forming toxin secreted by Aeromonas hydrophila - GPI-anchor
- 35. Original formulation was lyophilized, requiring aliquoting and freezing Reconstituted FLAER was unstable Stability problems better with
- 36. STABILITY OF FLAER Courtesy Andrea Illingworth
- 37. Routine Analysis: Summary Adequate for detection of all cases of hemolytic PNH White cell analysis necessary
- 38. High Sensitivity Assays: Special concerns Need to collect more events Requirement for an extensive study of
- 39. Guideline Summary I Broad agreement on the need for a consensus guideline Document reviews and clarifies
- 40. Guideline Summary II Granulocyte analysis provides better estimate of size of PNH clone than RBC analysis
- 41. Guideline Summary III For high sensitivity WBC analysis, essential to use an antibody for gating, and
- 42. EQA For PNH testing What kind of scheme? Screening vs high sensitivity (MRD) testing What material?
- 43. EQA For PNH testing What kind of scheme? ‘rare disease’ testing What cells to test? Single
- 44. EQA For PNH testing Screening vs high sensitivity (MRD) testing Screening (~1%) MRD 0.01% Methodology Standardised
- 45. EQA For PNH testing What material? Small groups: exchange of known fresh patient samples Large International
- 46. EQA For PNH testing Educational aspects? Scoring/performance issues? How to assess performance? Poor performance – educational
- 48. Скачать презентацию
Paroxysmal Nocturnal Haemoglobinuria
Clinical aspects of PNH
New ICCS Guidelines
EQA and PNH testing
Paroxysmal Nocturnal Haemoglobinuria
Clinical aspects of PNH
New ICCS Guidelines
EQA and PNH testing
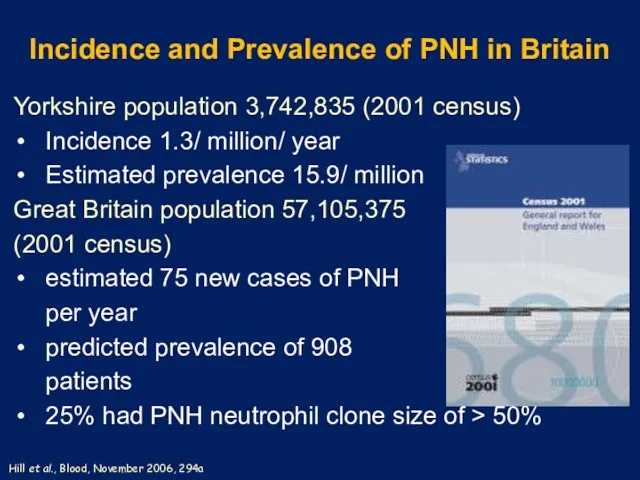
Incidence and Prevalence of PNH in Britain
Yorkshire population 3,742,835 (2001 census)
Incidence
Incidence and Prevalence of PNH in Britain
Yorkshire population 3,742,835 (2001 census)
Incidence
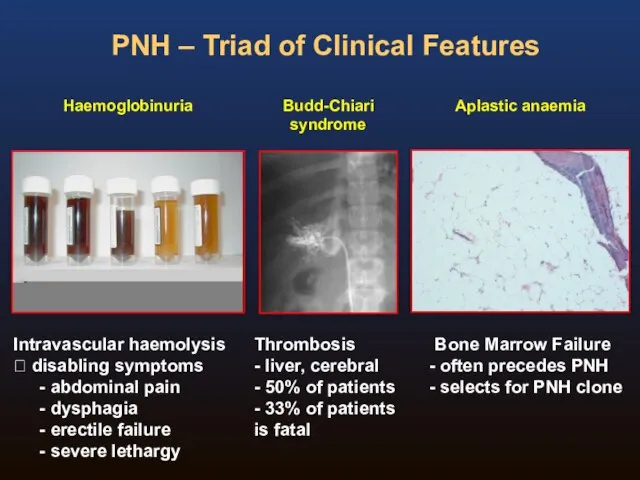
PNH – Triad of Clinical Features
Haemoglobinuria
Intravascular haemolysis
? disabling symptoms
abdominal pain
PNH – Triad of Clinical Features
Haemoglobinuria
Intravascular haemolysis
? disabling symptoms
abdominal pain
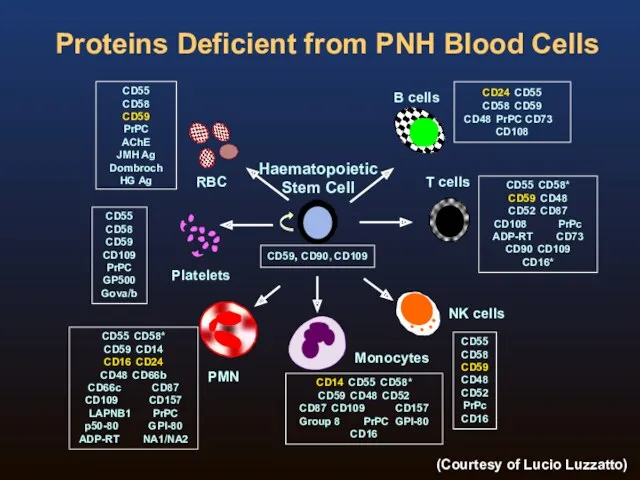
Proteins Deficient from PNH Blood Cells
CD59, CD90, CD109
CD55
CD58
CD59 CD48
CD52
PrPc
CD16
CD24 CD55
CD58 CD59
CD48 PrPC CD73 CD108
CD55
CD58
CD59
CD109
PrPC
GP500
Gova/b
CD55
CD58
CD59
PrPC
AChE
JMH
Proteins Deficient from PNH Blood Cells
CD59, CD90, CD109
CD55
CD58
CD59 CD48
CD52
PrPc
CD16
CD24 CD55
CD58 CD59
CD48 PrPC CD73 CD108
CD55
CD58
CD59
CD109
PrPC
GP500
Gova/b
CD55
CD58
CD59
PrPC
AChE
JMH
Why does PNH occur?
PNH clones
Lack complement regulatory molecules and therefore probably
Why does PNH occur?
PNH clones
Lack complement regulatory molecules and therefore probably
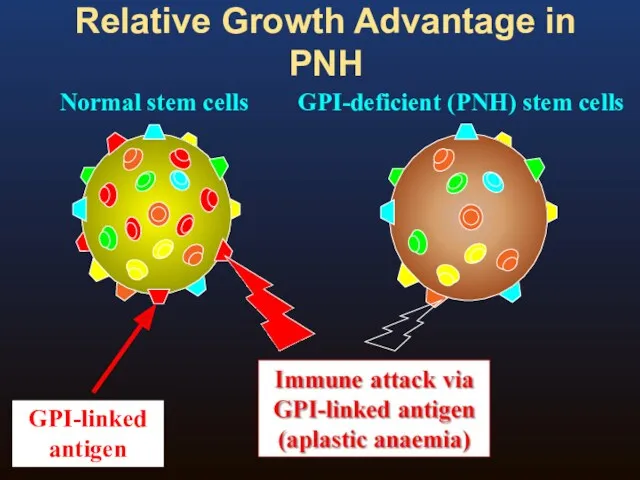
Relative Growth Advantage in PNH
Normal stem cells
GPI-deficient (PNH) stem cells
Relative Growth Advantage in PNH
Normal stem cells
GPI-deficient (PNH) stem cells
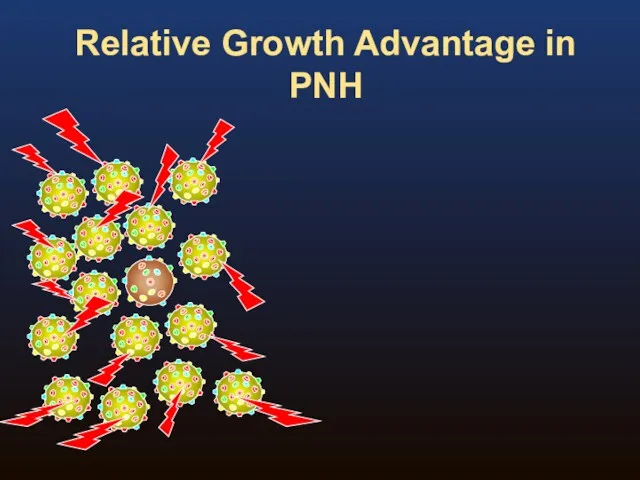
Relative Growth Advantage in PNH
Relative Growth Advantage in PNH
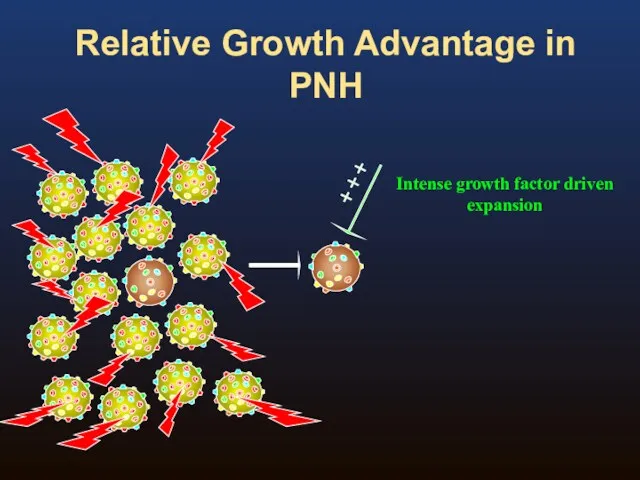
Relative Growth Advantage in PNH
Relative Growth Advantage in PNH
Relative Growth Advantage in PNH
Relative Growth Advantage in PNH
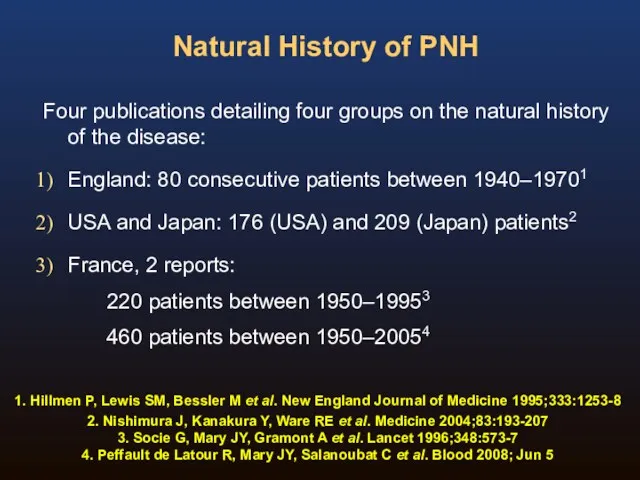
Natural History of PNH
Four publications detailing four groups on the natural
Natural History of PNH
Four publications detailing four groups on the natural
Natural History of PNH
1. Hillmen P, Lewis SM, Bessler M et
Natural History of PNH
1. Hillmen P, Lewis SM, Bessler M et
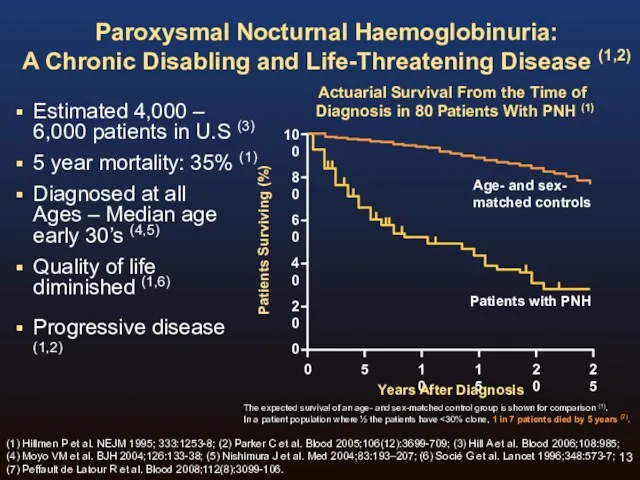
Paroxysmal Nocturnal Haemoglobinuria:
A Chronic Disabling and Life-Threatening Disease (1,2)
Estimated 4,000 –
Paroxysmal Nocturnal Haemoglobinuria:
A Chronic Disabling and Life-Threatening Disease (1,2)
Estimated 4,000 –
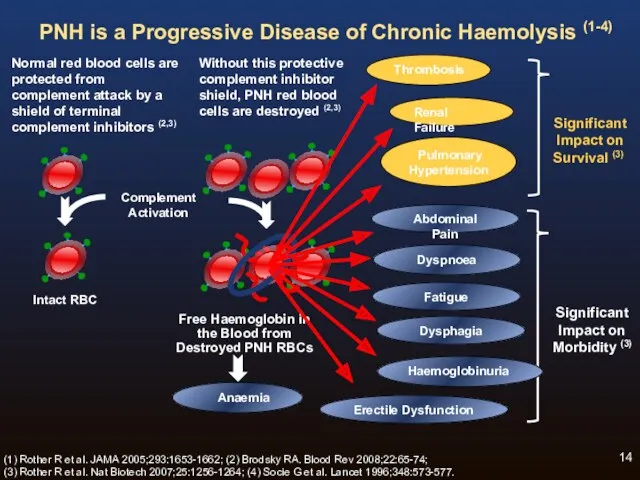
Normal red blood cells are protected from complement attack by a
Normal red blood cells are protected from complement attack by a
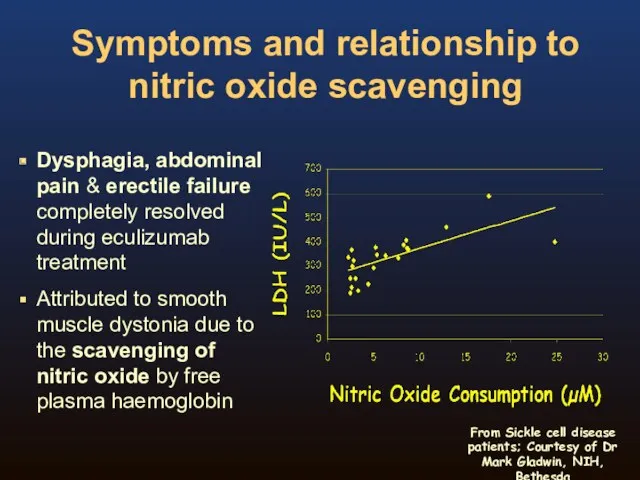
Symptoms and relationship to nitric oxide scavenging
Dysphagia, abdominal pain & erectile
Symptoms and relationship to nitric oxide scavenging
Dysphagia, abdominal pain & erectile
Haemolysis and Nitric Oxide
Red blood cell destruction during haemolysis releases
cell-free
Haemolysis and Nitric Oxide
Red blood cell destruction during haemolysis releases cell-free
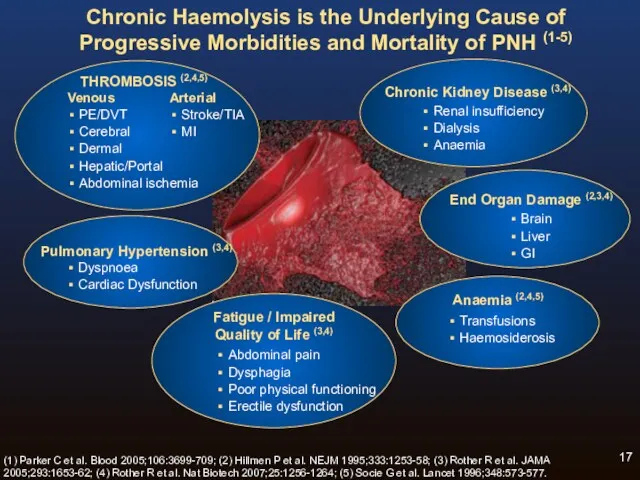
Chronic Haemolysis is the Underlying Cause of Progressive Morbidities and Mortality
Chronic Haemolysis is the Underlying Cause of Progressive Morbidities and Mortality
Renal Damage in PNH
Chronic haemolysis and cell-free plasma haemoglobin lead
to
Renal Damage in PNH
Chronic haemolysis and cell-free plasma haemoglobin lead to
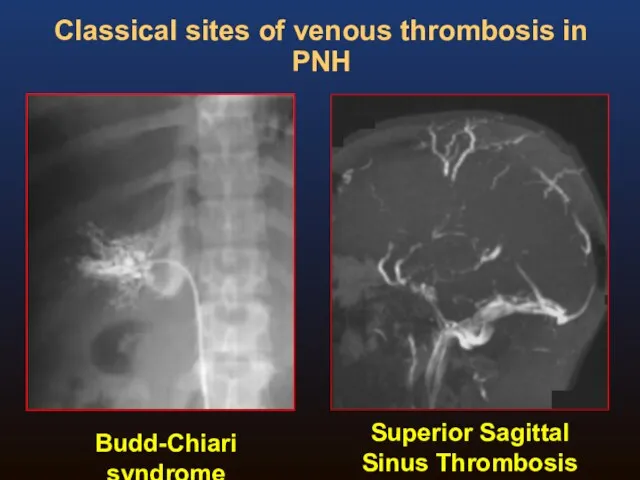
Budd-Chiari syndrome
Superior Sagittal Sinus Thrombosis
Classical sites of venous thrombosis in PNH
Budd-Chiari syndrome
Superior Sagittal Sinus Thrombosis
Classical sites of venous thrombosis in PNH
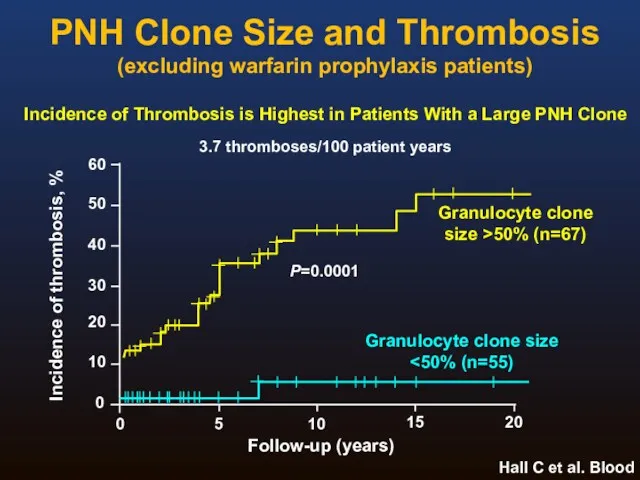
PNH Clone Size and Thrombosis
(excluding warfarin prophylaxis patients)
Hall C et al.
PNH Clone Size and Thrombosis
(excluding warfarin prophylaxis patients)
Hall C et al.
Laboratory Investigation of PNH
Flow cytometry immunophenotyping is the method of choice
Laboratory Investigation of PNH
Flow cytometry immunophenotyping is the method of choice
Background
In 2008 the Clinical Cytometry Society sponsored a workshop on PNH
Background
In 2008 the Clinical Cytometry Society sponsored a workshop on PNH
The disease is rare and most labs have limited experience in
The disease is rare and most labs have limited experience in
Consensus Committee
Michael J Borowitz, MD, PhD
Johns Hopkins
Fiona E Craig, MD
University
Consensus Committee
Michael J Borowitz, MD, PhD
Johns Hopkins
Fiona E Craig, MD
University
ICCS PNH Testing Guidelines
Borowitz M, Craig F, DiGiuseppe J, Illingworth A,
ICCS PNH Testing Guidelines
Borowitz M, Craig F, DiGiuseppe J, Illingworth A,
Recommendations in the ICCS PNH Testing Guidelines Document
Recommendations tried to strike
Recommendations in the ICCS PNH Testing Guidelines Document
Recommendations tried to strike
Contents Of The Document
Rationale and History
Clinical Indications
Methodology
Routine testing
High sensitivity testing
RBC vs
Contents Of The Document
Rationale and History
Clinical Indications
Methodology
Routine testing
High sensitivity testing
RBC vs
Methodology
Sample issues
Comparison of RBC and WBC testing
Reagents
Analytical approaches
Routine vs high sensitivity
Methodology
Sample issues
Comparison of RBC and WBC testing
Reagents
Analytical approaches
Routine vs high sensitivity
Red Cell Analysis: Routine testing
ADVANTAGES
Relatively straightforward
Best way to identify Type II
Red Cell Analysis: Routine testing
ADVANTAGES
Relatively straightforward
Best way to identify Type II
Routine Red Cell Analysis: Reagents
For historical reasons, CD55 and CD59 are
Routine Red Cell Analysis: Reagents
For historical reasons, CD55 and CD59 are
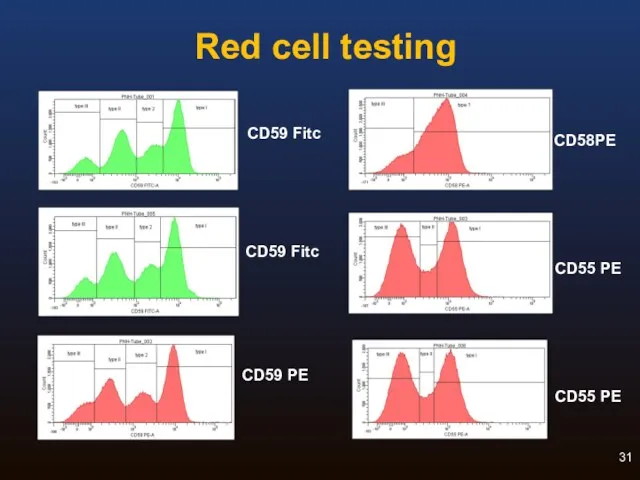
Red cell testing
CD58PE
CD55 PE
CD55 PE
CD59 Fitc
CD59 PE
CD59 Fitc
Red cell testing
CD58PE
CD55 PE
CD55 PE
CD59 Fitc
CD59 PE
CD59 Fitc
Leucocyte Analysis: Routine testing
Granulocyte PNH clone probably gives most accurate estimate
Leucocyte Analysis: Routine testing
Granulocyte PNH clone probably gives most accurate estimate
Leucocyte Analysis: Reagents
CD55 and CD59 were used historically but these
Leucocyte Analysis: Reagents
CD55 and CD59 were used historically but these
WHAT IS FLAER?
FLuorescent AERolysin
Aerolysin is a pore-forming toxin secreted by Aeromonas
WHAT IS FLAER?
FLuorescent AERolysin
Aerolysin is a pore-forming toxin secreted by Aeromonas
Original formulation was lyophilized, requiring aliquoting and freezing
Reconstituted FLAER was unstable
Stability
Original formulation was lyophilized, requiring aliquoting and freezing
Reconstituted FLAER was unstable
Stability
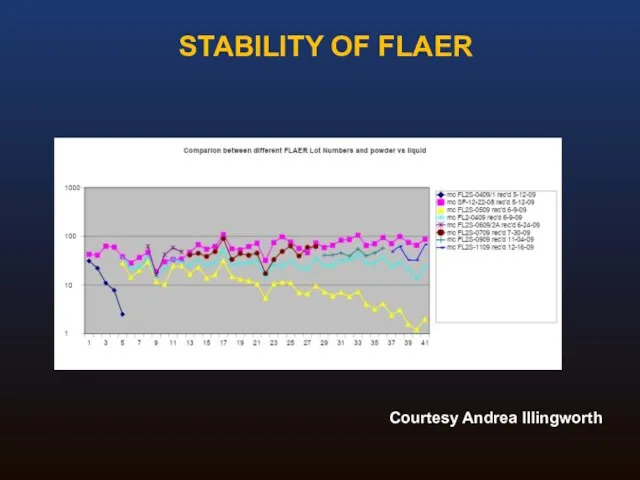
STABILITY OF FLAER
Courtesy Andrea Illingworth
STABILITY OF FLAER
Courtesy Andrea Illingworth
Routine Analysis: Summary
Adequate for detection of all cases of hemolytic PNH
White
Routine Analysis: Summary
Adequate for detection of all cases of hemolytic PNH
White
High Sensitivity Assays: Special concerns
Need to collect more events
Requirement for an
High Sensitivity Assays: Special concerns
Need to collect more events
Requirement for an
Guideline Summary I
Broad agreement on the need for a consensus guideline
Document
Guideline Summary I
Broad agreement on the need for a consensus guideline
Document
Guideline Summary II
Granulocyte analysis provides better estimate of size of PNH
Guideline Summary II
Granulocyte analysis provides better estimate of size of PNH
Guideline Summary III
For high sensitivity WBC analysis, essential to use an
Guideline Summary III
For high sensitivity WBC analysis, essential to use an
EQA For PNH testing
What kind of scheme?
Screening vs high sensitivity (MRD)
EQA For PNH testing
What kind of scheme?
Screening vs high sensitivity (MRD)
EQA For PNH testing
What kind of scheme?
‘rare disease’ testing
What cells to
EQA For PNH testing
What kind of scheme?
‘rare disease’ testing
What cells to
EQA For PNH testing
Screening vs high sensitivity (MRD) testing
Screening (~1%)
MRD
EQA For PNH testing
Screening vs high sensitivity (MRD) testing
Screening (~1%)
MRD
EQA For PNH testing
What material?
Small groups: exchange of known fresh patient
EQA For PNH testing
What material?
Small groups: exchange of known fresh patient
EQA For PNH testing
Educational aspects?
Scoring/performance issues?
How to assess performance?
Poor performance –
EQA For PNH testing
Educational aspects?
Scoring/performance issues?
How to assess performance?
Poor performance –
 Травмы органов и тканей челюстнолицевой области у детей
Травмы органов и тканей челюстнолицевой области у детей Вирус гепатита А (ВГА, HAV)
Вирус гепатита А (ВГА, HAV) Загальна характеристика вірусних гепатитів. Вірусні гепатити з фекально-оральним механізмом зараження
Загальна характеристика вірусних гепатитів. Вірусні гепатити з фекально-оральним механізмом зараження Патофизиология системы внешнего дыхания
Патофизиология системы внешнего дыхания Жүйелі аурулар және зат алмасу ауруларында ауыз қуысы кілегей қабығының зақымдануы. Клиникасы, диагностикасы, емі
Жүйелі аурулар және зат алмасу ауруларында ауыз қуысы кілегей қабығының зақымдануы. Клиникасы, диагностикасы, емі Лучевая анатомия позвоночника
Лучевая анатомия позвоночника Лямблиоз
Лямблиоз Эргономические основы организации рабочего места врача-стоматолога. Работа врача с помощником в четыре руки
Эргономические основы организации рабочего места врача-стоматолога. Работа врача с помощником в четыре руки Антенатальды кезеңдегі инвазивті тексеру
Антенатальды кезеңдегі инвазивті тексеру Национальный институт рака им. Дж. Паскале
Национальный институт рака им. Дж. Паскале Хроническая венозная недостаточность
Хроническая венозная недостаточность Холиномиметические средства (Лекция № 4)
Холиномиметические средства (Лекция № 4) Сarec cистема, Cad/Cem система, свойства, применение
Сarec cистема, Cad/Cem система, свойства, применение Работа в очаге туберкулёзной инфекции
Работа в очаге туберкулёзной инфекции Пиодермии. Этиология. Классификация. Клиника
Пиодермии. Этиология. Классификация. Клиника Физиология эндокринной системы
Физиология эндокринной системы Жинақталған салыстыру. Бонферронидің түзетуімен. Стьюдент белгісі
Жинақталған салыстыру. Бонферронидің түзетуімен. Стьюдент белгісі Образ врача. Нравственные принципы профессии врача
Образ врача. Нравственные принципы профессии врача Дегидрогеназалардың нуклеотидті. Коферменттері. НАД, НАДФ, ФАД нуклеозидті коферменттер
Дегидрогеназалардың нуклеотидті. Коферменттері. НАД, НАДФ, ФАД нуклеозидті коферменттер Кожные проявления аллергии. Клинические аспекты и принципы лечения
Кожные проявления аллергии. Клинические аспекты и принципы лечения Роль медицинской сестры в преодолении деформации личности онкологических больных разных возрастов
Роль медицинской сестры в преодолении деформации личности онкологических больных разных возрастов Комплексна оцінка здоров’я населення. Методика вивчення та оцінка чинників, що впливають на здоров’я населення
Комплексна оцінка здоров’я населення. Методика вивчення та оцінка чинників, що впливають на здоров’я населення Принцип действия лазерного луча. Терапия сосудистых патологий
Принцип действия лазерного луча. Терапия сосудистых патологий Задачи принципы организации диетического питания
Задачи принципы организации диетического питания Развитие медицины в России в 19 веке. Хирургия
Развитие медицины в России в 19 веке. Хирургия Сердце. Основные диагностические алгоритмы
Сердце. Основные диагностические алгоритмы Зәр және жыныстық жүйесінің қатерсіз және қатерлі ісіктері
Зәр және жыныстық жүйесінің қатерсіз және қатерлі ісіктері Всемирный день здоровья
Всемирный день здоровья