- Bronchial asthma in children (treatment)

Содержание
- 2. Plan of the lecture 1. INDICATIONS for HOSPITALIZATION 2. Exacerbation treatment 3. MEDICATIONS for basic therapy
- 3. INDICATIONS for HOSPITALIZATION Severe attack Poor efficacy for 2-6 hours of treatment Children with high mortality
- 4. Exacerbation treatment at ambulatory stage Inhaling short-acting β2-agonist every 20 min during the hour through matured
- 5. Asthma exacerbation treatment algorithm in hospital
- 8. MEDICATIONS for basic therapy of BA Membrane stabilizers of mast cells: derivates of chromolicate acid -
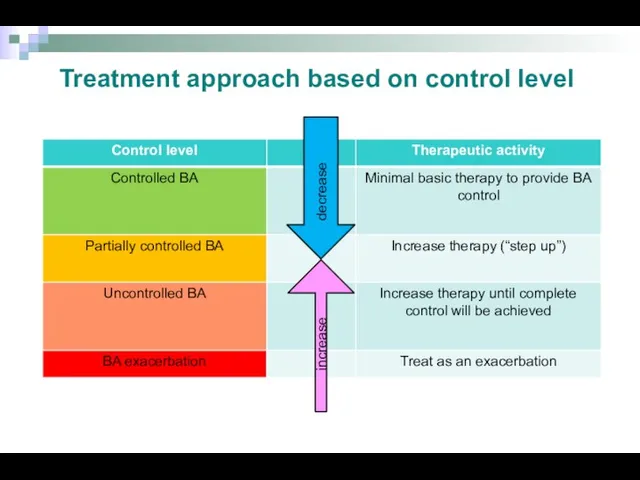
- 9. decrease increase Treatment approach based on control level
- 10. Обострение БА. Критерии тяжести + SCS + urgent allergologist consulting/ hospitalization Urgent hospitalization! Short acting bronchodilators
- 11. Clinic recommendations of children allergology and immunology 2010 (Ukraine)based on GINA (2009) Therapy increasing
- 12. Step therapy of BA Step 1, including reliever medication usage per need, is assigned only for
- 13. Step therapy of BA At step 3 is recommended combination of IGCS in low dosage together
- 14. Step therapy of BA Monotherapy of BA without GCS is prohibited because it increases significantly mortality
- 15. How to perform basic therapy in children with BA? To define control level of disease To
- 16. Sustaining treatment of BA: Chromons Sodium chromoglycate, Sodium nedocromil Activity mechanism: suppress inflammatory mediator releasing from
- 17. Sustaining treatment of BA: Leikotriens antagonists Антагонисты лейкотриенов Zafirlukast, Montelukast Activity mechanism: Leukotriens receptors blockage in
- 18. Beclomethasone dipropionate, Budesonide, Fluticasone propionate Activity mechanism: inflammatory process suppression in respiratory tract They are the
- 19. Equipotent day IGCS dosages Эквивалентность (эквипотентность) препаратов определяли на основе их сравнительной эффективности. Адаптировано из: GINA
- 20. Sustaining therapy of BA: Long-acting β2-agonists (LABA) SALMETEROL, FORMOTEROL Activity mechanism: produce bronchial smooth muscle relaxation
- 21. Why combined therapy is more effective in BA? Respiratory tract inflammation Smooth muscle dysfunction Symptoms/Exacerbation Respiratory
- 22. Fixed combinations of IGCS +LABA Fluticasone propionate + Salmeterol (Seretide) from 4 years old Budesonide +
- 23. Place of antileukotrien (AL) medications in therapy of BA GINA recommendations Toddlers Controlled BA Partially controlled
- 24. Normal variability of inspiratory flow Variability of inspiratory flow can provide inaquality of medication distribution Spirometric
- 25. Flowmetric curves in BA patient in repeating respiratory attempts Normal variability of inspiratory flow Variability of
- 26. Devices for inhalation of medications Metered dosed aerosol inhaler (MDAI) Meterd aerosol inhaler with spacer (MDAI+
- 27. Technology of inhalation with MDAI Stand up to increase mobility of diaphragm Take off cap from
- 28. MDAI (metered dosed aerosol inhaler) Spacer usage considerably decrease medication deposition in oral cavity and pharynx
- 29. Optimal technology of aerosol inhalation through spacer is deep slow inhale or two calm deep inhales
- 30. Special spacers are babyhalers They are supplied by the one side valve, that prevent loosing of
- 31. MDPI (metered dosed powder inhaler) Usage of MDPI doesn’t demand synchronizing of inhaling with inhaler activation.
- 32. Inhalation technology by MDPI Prepare inhaler according instruction Perform exhalation Tightly cope mouth piece by lips
- 33. Multidisk (Diskus, Accuhaler) Mouth piece Rod Blister, contained 60 medication doses Free tape Wheel of dose
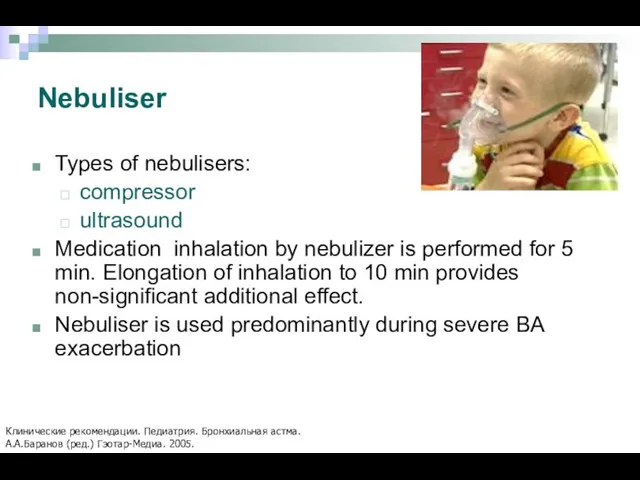
- 34. Nebuliser Types of nebulisers: compressor ultrasound Medication inhalation by nebulizer is performed for 5 min. Elongation
- 35. Nebuliser working scheme Сжатый воздух Inhaled aerosol Mouth piece with exhaling valve Exhaled air Клапан вдоха
- 36. Choice of inhaling device for children 1. GINA 2007: www.ginasthma.org 2. Клинические рекомендации. Педиатрия. Бронхиальная астма.
- 37. Medications for nebulizer therapy Ventolin (in nebula 2,5 ml/2,5 mg in undiluted form) Berodual (solution for
- 38. Asthma control is the main physician task Адаптировано из: GINA 2007: www.ginasthma.org
- 39. Allergen specific immune therapy Nowadays is the only effective treatment method that provides changing of natural
- 41. Скачать презентацию
Plan of the lecture
1. INDICATIONS for HOSPITALIZATION
2. Exacerbation treatment
3.
Plan of the lecture
1. INDICATIONS for HOSPITALIZATION
2. Exacerbation treatment
3.
INDICATIONS for HOSPITALIZATION
Severe attack
Poor efficacy for 2-6 hours of treatment
Children with
INDICATIONS for HOSPITALIZATION
Severe attack
Poor efficacy for 2-6 hours of treatment
Children with
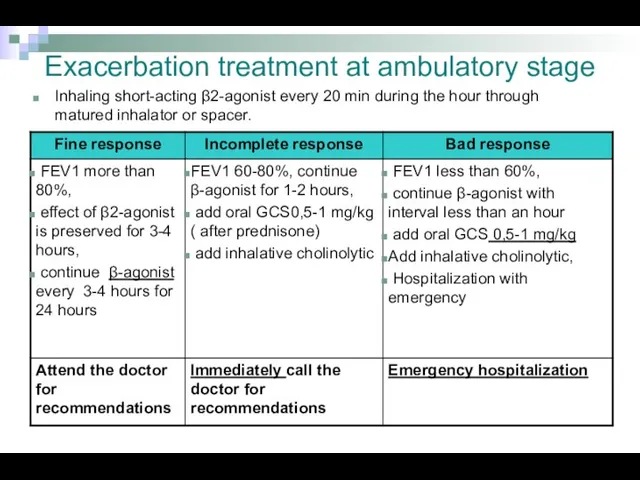
Exacerbation treatment at ambulatory stage
Inhaling short-acting β2-agonist every 20 min during
Exacerbation treatment at ambulatory stage
Inhaling short-acting β2-agonist every 20 min during
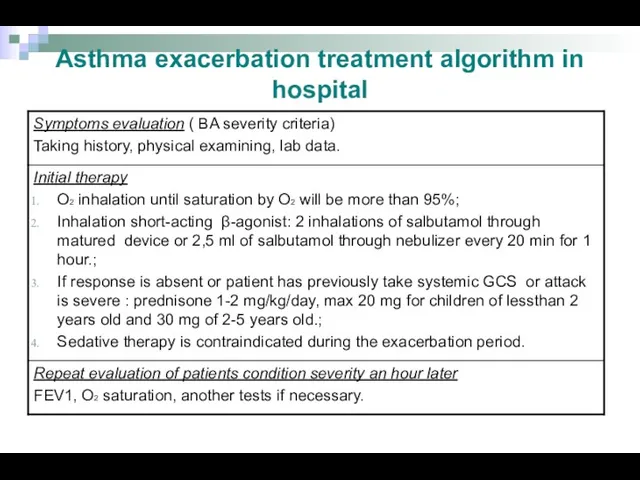
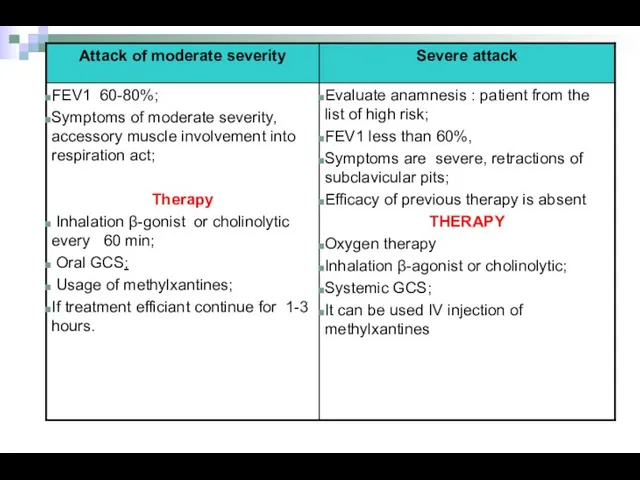
Asthma exacerbation treatment algorithm in hospital
Asthma exacerbation treatment algorithm in hospital

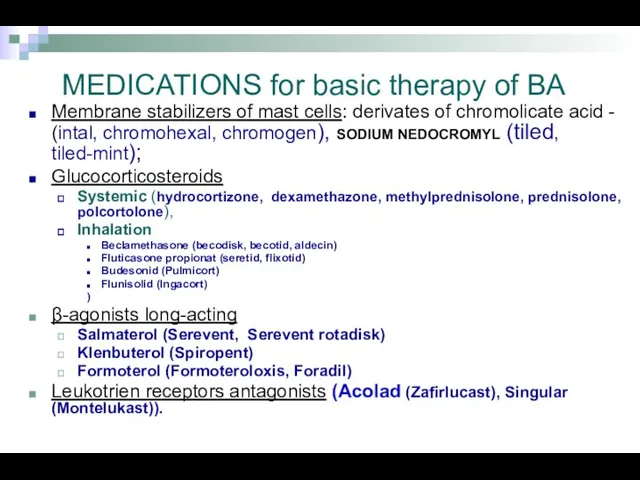
MEDICATIONS for basic therapy of BA
Membrane stabilizers of mast cells:
MEDICATIONS for basic therapy of BA
Membrane stabilizers of mast cells:
decrease
increase
Treatment approach based on control level
decrease
increase
Treatment approach based on control level
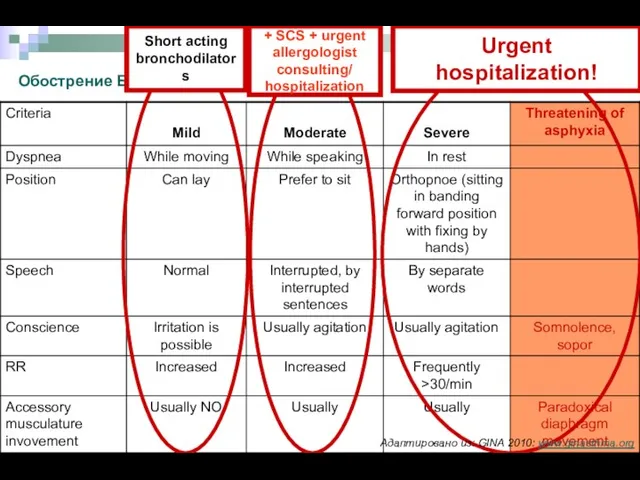
Обострение БА. Критерии тяжести
+ SCS + urgent
allergologist
consulting/
hospitalization
Urgent
hospitalization!
Short acting
Обострение БА. Критерии тяжести
+ SCS + urgent
allergologist
consulting/
hospitalization
Urgent
hospitalization!
Short acting
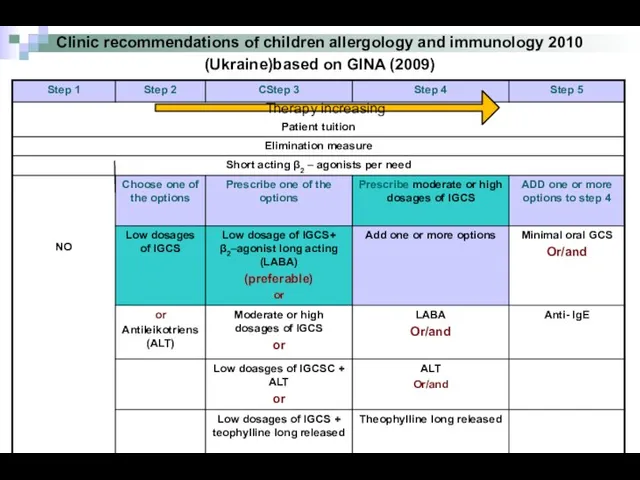
Clinic recommendations of children allergology and immunology 2010 (Ukraine)based on GINA (2009)
Clinic recommendations of children allergology and immunology 2010 (Ukraine)based on GINA (2009)
Step therapy of BA
Step 1, including reliever medication usage per need,
Step therapy of BA
Step 1, including reliever medication usage per need,
Step therapy of BA
At step 3 is recommended combination of IGCS
Step therapy of BA
At step 3 is recommended combination of IGCS
Step therapy of BA
Monotherapy of BA without GCS is prohibited because
Step therapy of BA
Monotherapy of BA without GCS is prohibited because
How to perform basic therapy in children with BA?
To define control
How to perform basic therapy in children with BA?
To define control
Sustaining treatment of BA:
Chromons
Sodium chromoglycate, Sodium nedocromil
Activity mechanism: suppress inflammatory
Sustaining treatment of BA:
Chromons
Sodium chromoglycate, Sodium nedocromil
Activity mechanism: suppress inflammatory
Sustaining treatment of BA:
Leikotriens antagonists
Антагонисты лейкотриенов
Zafirlukast, Montelukast
Activity mechanism: Leukotriens receptors
Sustaining treatment of BA:
Leikotriens antagonists
Антагонисты лейкотриенов
Zafirlukast, Montelukast
Activity mechanism: Leukotriens receptors
Beclomethasone dipropionate, Budesonide, Fluticasone propionate
Activity mechanism: inflammatory process suppression in
Beclomethasone dipropionate, Budesonide, Fluticasone propionate
Activity mechanism: inflammatory process suppression in
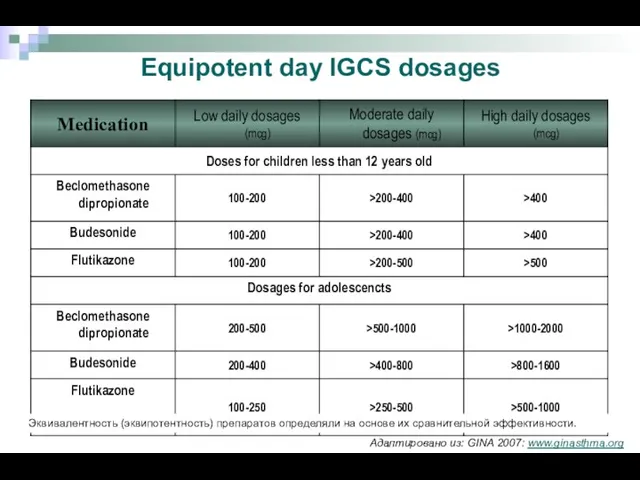
Equipotent day IGCS dosages
Эквивалентность (эквипотентность) препаратов определяли на основе их сравнительной
Equipotent day IGCS dosages
Эквивалентность (эквипотентность) препаратов определяли на основе их сравнительной
Sustaining therapy of BA:
Long-acting β2-agonists (LABA)
SALMETEROL, FORMOTEROL
Activity mechanism: produce bronchial smooth
Sustaining therapy of BA:
Long-acting β2-agonists (LABA)
SALMETEROL, FORMOTEROL
Activity mechanism: produce bronchial smooth
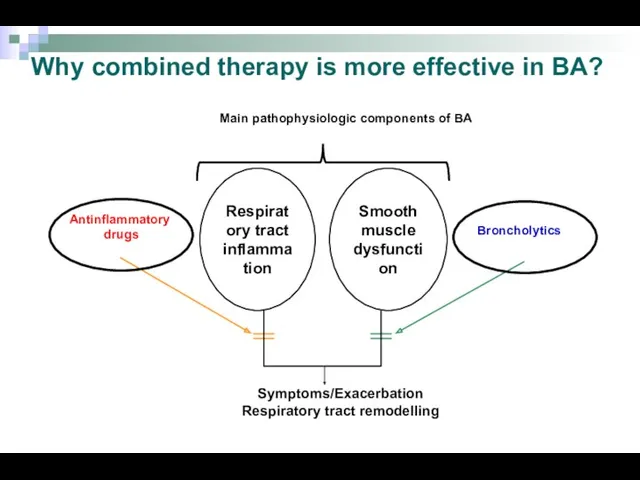
Why combined therapy is more effective in BA?
Respiratory tract
inflammation
Smooth muscle
dysfunction
Symptoms/Exacerbation
Respiratory
Why combined therapy is more effective in BA?
Respiratory tract
inflammation
Smooth muscle
dysfunction
Symptoms/Exacerbation
Respiratory
Fixed combinations of IGCS +LABA
Fluticasone propionate + Salmeterol (Seretide) from 4
Fixed combinations of IGCS +LABA
Fluticasone propionate + Salmeterol (Seretide) from 4
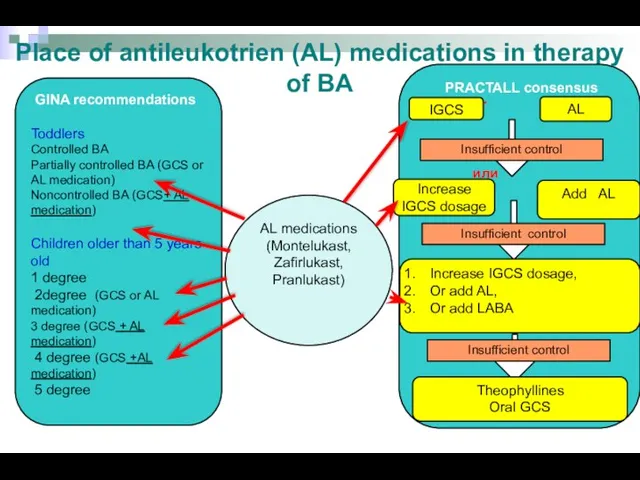
Place of antileukotrien (AL) medications in therapy of BA
GINA recommendations
Toddlers
Controlled
Place of antileukotrien (AL) medications in therapy of BA
GINA recommendations
Toddlers
Controlled
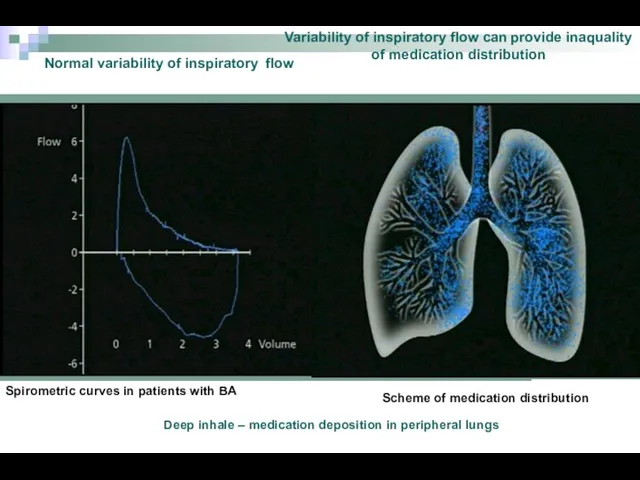
Normal variability of inspiratory flow
Variability of inspiratory flow can provide inaquality
Normal variability of inspiratory flow
Variability of inspiratory flow can provide inaquality
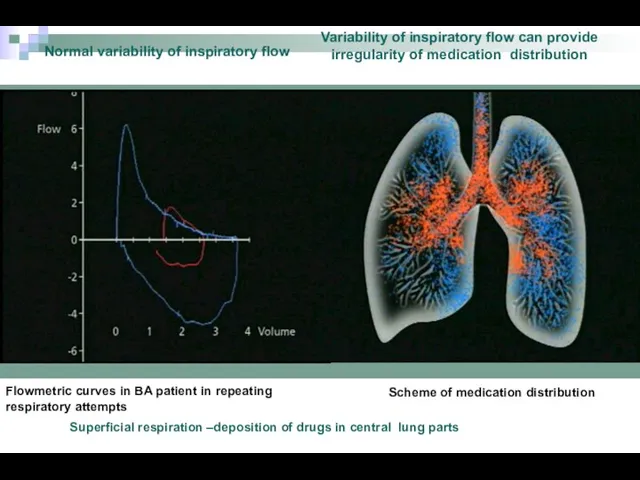
Flowmetric curves in BA patient in repeating respiratory attempts
Normal variability
Flowmetric curves in BA patient in repeating respiratory attempts
Normal variability
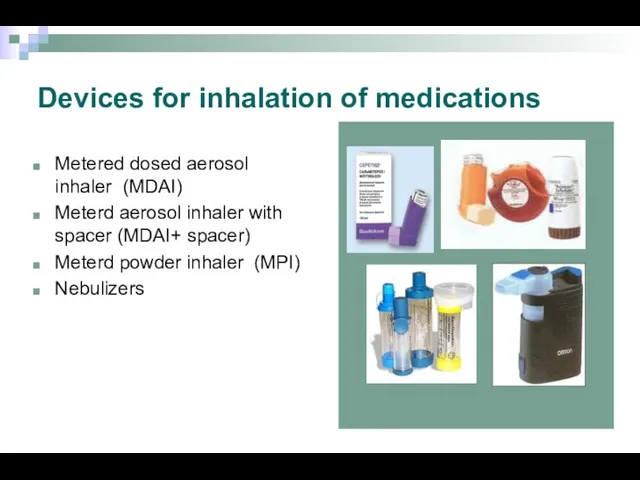
Devices for inhalation of medications
Metered dosed aerosol inhaler (MDAI)
Meterd aerosol inhaler
Devices for inhalation of medications
Metered dosed aerosol inhaler (MDAI)
Meterd aerosol inhaler
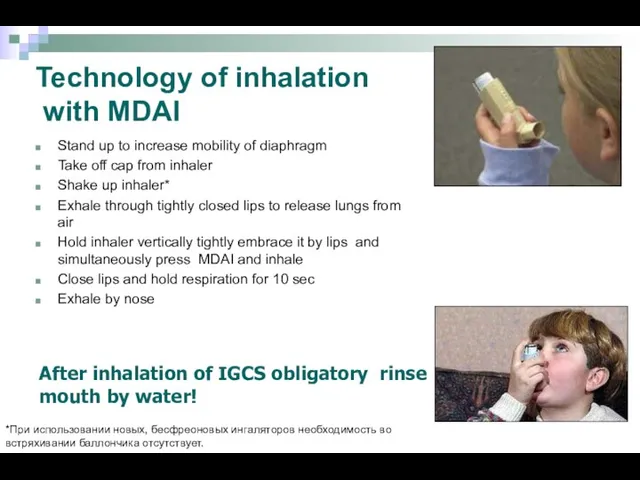
Technology of inhalation
with MDAI
Stand up to increase mobility of
Technology of inhalation
with MDAI
Stand up to increase mobility of
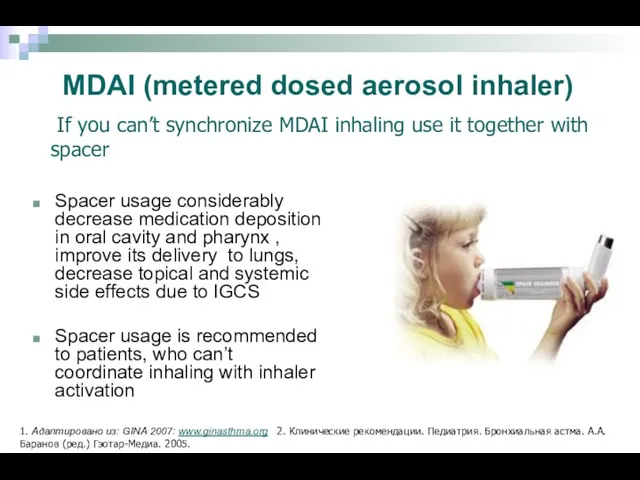
MDAI (metered dosed aerosol inhaler)
Spacer usage considerably decrease medication deposition in oral
MDAI (metered dosed aerosol inhaler)
Spacer usage considerably decrease medication deposition in oral
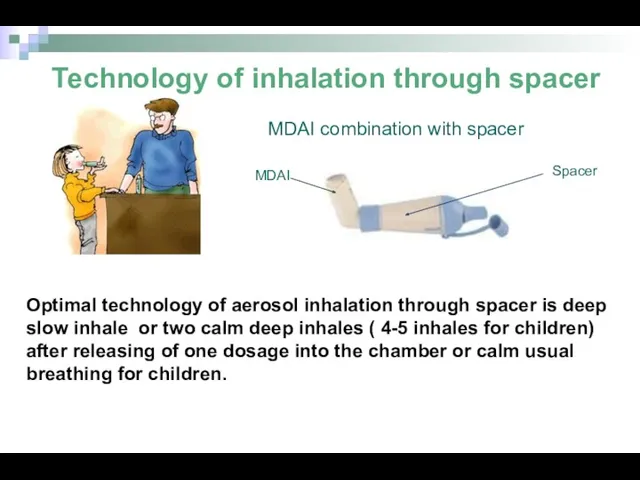
Optimal technology of aerosol inhalation through spacer is deep slow inhale
Optimal technology of aerosol inhalation through spacer is deep slow inhale
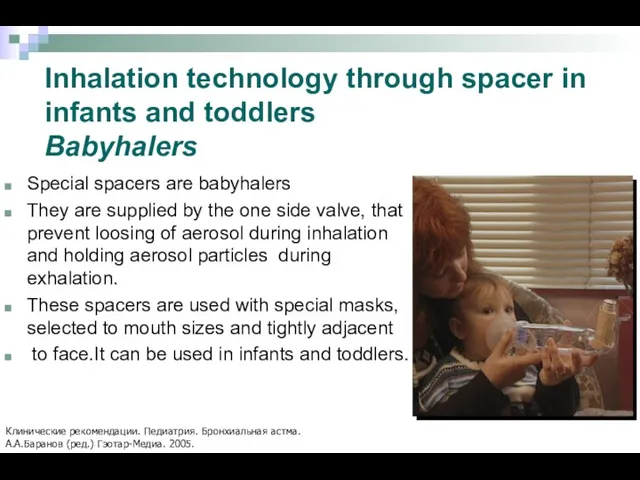
Special spacers are babyhalers
They are supplied by the one side valve,
Special spacers are babyhalers
They are supplied by the one side valve,
MDPI (metered dosed powder inhaler)
Usage of MDPI doesn’t demand synchronizing of
MDPI (metered dosed powder inhaler)
Usage of MDPI doesn’t demand synchronizing of
Inhalation technology by MDPI
Prepare inhaler according instruction
Perform exhalation
Tightly cope mouth piece
Inhalation technology by MDPI
Prepare inhaler according instruction
Perform exhalation
Tightly cope mouth piece
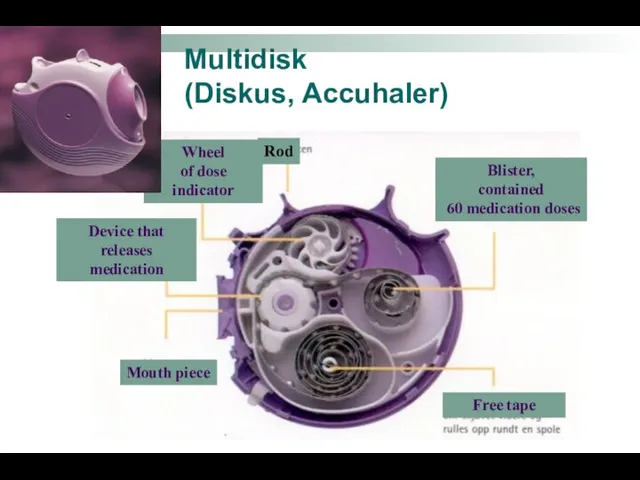
Multidisk
(Diskus, Accuhaler)
Mouth piece
Rod
Blister,
contained
60 medication doses
Free tape
Wheel
of dose indicator
Device that
Multidisk
(Diskus, Accuhaler)
Mouth piece
Rod
Blister,
contained
60 medication doses
Free tape
Wheel
of dose indicator
Device that
Nebuliser
Types of nebulisers:
compressor
ultrasound
Medication inhalation by nebulizer is performed for 5
Nebuliser
Types of nebulisers:
compressor
ultrasound
Medication inhalation by nebulizer is performed for 5
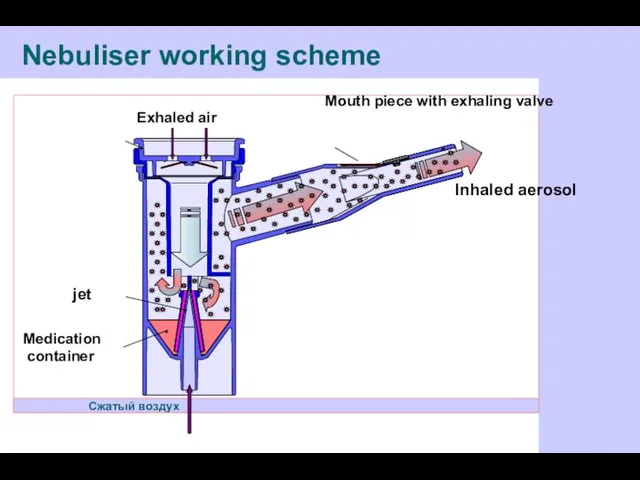
Nebuliser working scheme
Сжатый воздух
Inhaled aerosol
Mouth piece with exhaling valve
Exhaled air
Клапан вдоха
jet
Medication
Nebuliser working scheme
Сжатый воздух
Inhaled aerosol
Mouth piece with exhaling valve
Exhaled air
Клапан вдоха
jet
Medication
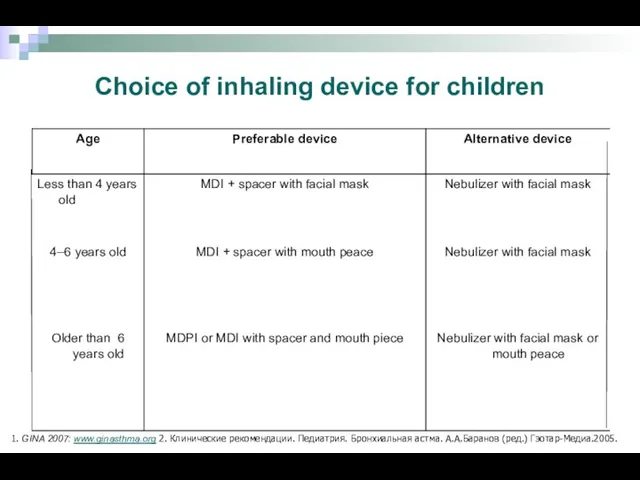
Choice of inhaling device for children
1. GINA 2007: www.ginasthma.org 2. Клинические
Choice of inhaling device for children
1. GINA 2007: www.ginasthma.org 2. Клинические
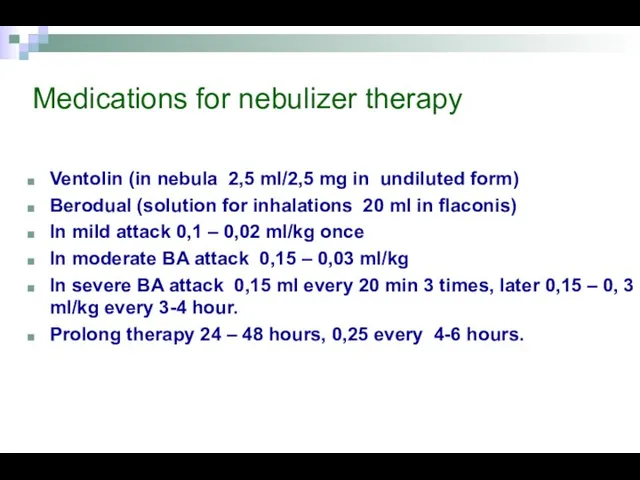
Medications for nebulizer therapy
Ventolin (in nebula 2,5 ml/2,5 mg in undiluted
Medications for nebulizer therapy
Ventolin (in nebula 2,5 ml/2,5 mg in undiluted
Asthma control is the main physician task
Адаптировано из: GINA 2007: www.ginasthma.org
Asthma control is the main physician task
Адаптировано из: GINA 2007: www.ginasthma.org
Allergen specific immune therapy
Nowadays is the only effective treatment method that
Allergen specific immune therapy
Nowadays is the only effective treatment method that
 Механическая асфиксия. Понятие о гипоксии
Механическая асфиксия. Понятие о гипоксии Экзогенный аллергический альвеолит
Экзогенный аллергический альвеолит Травмы, травматизм
Травмы, травматизм Медициналық сақтандырудың ерекшеліктері
Медициналық сақтандырудың ерекшеліктері Пища трех энергий. Здоровая пища
Пища трех энергий. Здоровая пища Балалардағы және қарт кісілердегі пневмонияның ерекшеліктері, визуалды әдістері
Балалардағы және қарт кісілердегі пневмонияның ерекшеліктері, визуалды әдістері Braster pro-иновационная система обследования молочной железы
Braster pro-иновационная система обследования молочной железы Бронхиальная астма. ХОБЛ
Бронхиальная астма. ХОБЛ Периоды родов. Изменения в матке во время родов
Периоды родов. Изменения в матке во время родов Психофизические особенности детей с задержкой психического развития и умственной отсталостью
Психофизические особенности детей с задержкой психического развития и умственной отсталостью Аллергия. Противоаллергические средства
Аллергия. Противоаллергические средства Питание как фактор здоровья (диета и нутрициология)
Питание как фактор здоровья (диета и нутрициология) Закаливание организма и двигательная активность
Закаливание организма и двигательная активность Грип та ГРВІ
Грип та ГРВІ Заболевания желудочно-кишечного тракта
Заболевания желудочно-кишечного тракта Травмы груди, живота, таза
Травмы груди, живота, таза Стирание твердых тканей зуба, физиологическое, патологическое
Стирание твердых тканей зуба, физиологическое, патологическое Низкопотоковая анестезия и анестезия по закрытому контуру
Низкопотоковая анестезия и анестезия по закрытому контуру Эндометрит
Эндометрит Blood circulation
Blood circulation Обучение по новому оборудованию Е5. Особенности персонального комбинированного стимулятора. Проффесиональный массаж
Обучение по новому оборудованию Е5. Особенности персонального комбинированного стимулятора. Проффесиональный массаж Род сальмонеллы
Род сальмонеллы Артериальная гипертензия
Артериальная гипертензия Заболевания кишечника
Заболевания кишечника Статистический анализ показателей здоровья населения и здравоохранения Менделеевского района
Статистический анализ показателей здоровья населения и здравоохранения Менделеевского района Противовирусные препараты
Противовирусные препараты Сердечно-легочная реанимация
Сердечно-легочная реанимация Жастан асқан балаларды рациональды тамақтандыру принциптері
Жастан асқан балаларды рациональды тамақтандыру принциптері