- Cardiology/EKG Board Review

Содержание
- 2. Objectives Review general method for EKG interpretation Review specific points of “data gathering” and “diagnoses” on
- 3. EKG
- 4. EKG – 12 Leads Anterior Leads - V1, V2, V3, V4 Inferior Leads – II, III,
- 5. 11 Step Method for Reading EKG’s “Data Gathering” – steps 1-4 1. Standardization – make sure
- 6. 11 Step Method for Reading EKG’s “Diagnoses” 5. Rhythm 6. Atrioventricular (AV) Block Disturbances 7. Bundle
- 7. Heart Rate Regular Rhythms
- 8. Heart Rate Irregular Rhythms
- 9. Intervals Measure length of PR interval, QT interval, width of P wave, QRS complex
- 10. QTc QTc = QT interval corrected for heart rate Uses Bazett’s Formula or Fridericia’s Formula Long
- 11. Axis
- 12. Rhythm 4 Questions 1. Are normal P waves present? 2. Are QRS complexes narrow or wide
- 13. Types of Arrhythmias Arrhythmias of sinus origin Ectopic rhythms Conduction Blocks Preexcitation syndromes
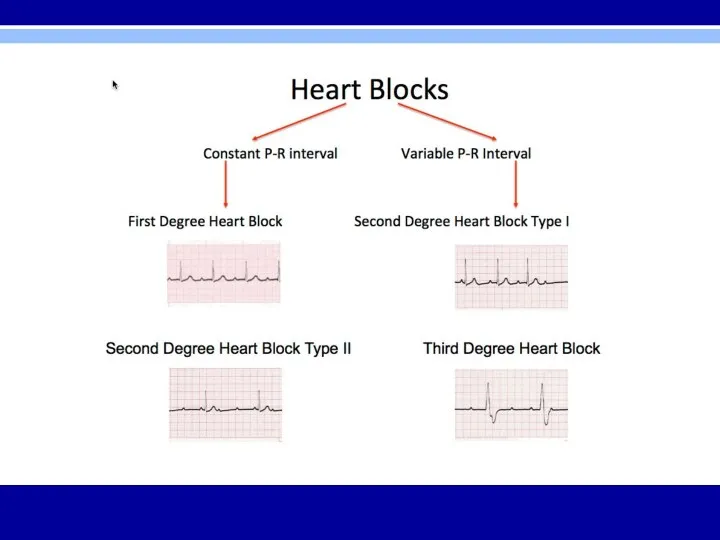
- 14. AV Block Diagnosed by examining relationship of P waves to QRS complexes First Degree – PR
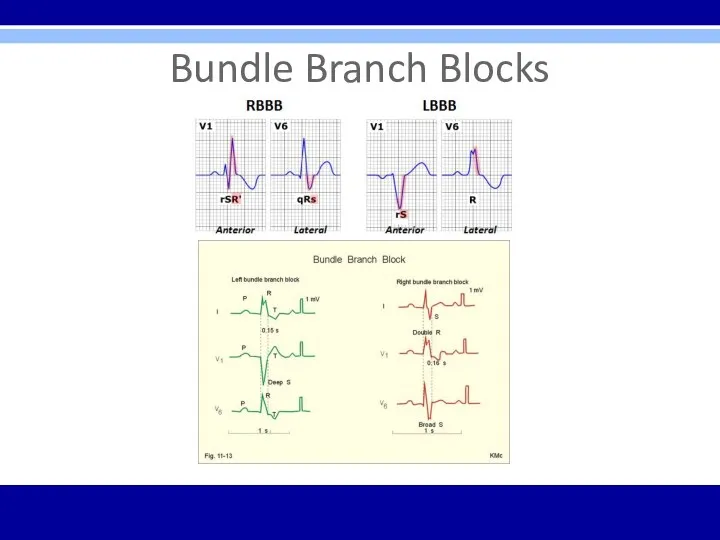
- 16. Bundle Branch Blocks Diagnosed by looking at width and configuration of QRS complexes
- 17. Bundle Branch Blocks RBBB criteria: 1. QRS complex > 0.12 seconds 2. RSR’ in leads V1
- 18. Bundle Branch Blocks
- 19. Hemiblocks Diagnosed by looking at right or left axis deviation Left Anterior Hemiblock 1.Normal QRS duration
- 20. Bifascicular Block RBBB with LAH RBBB – QRS > 0.12 sec and RSR’ in V1 and
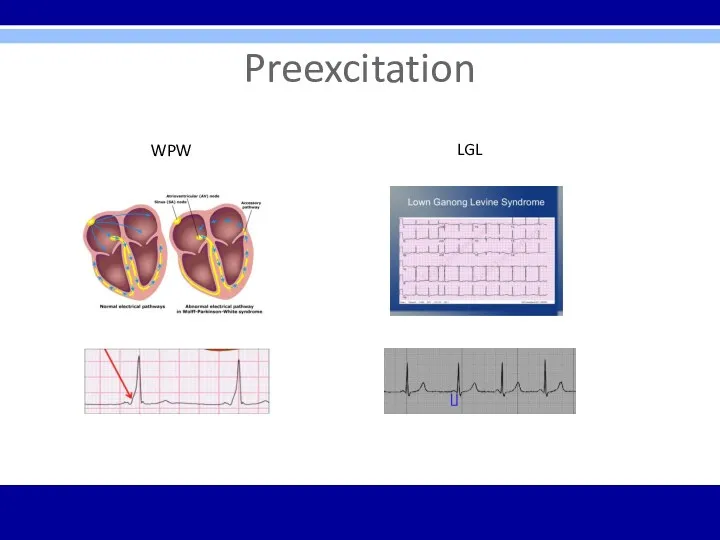
- 21. Preexcitation Wolff-Parkinson-White (WPW) Syndrome 1. PR interval 2. Wide QRS complexes 3. Delta waves seen in
- 22. Preexcitation WPW LGL
- 23. Supraventricular Arrhythmias PSVT- regular; P waves retrograde if visible; rate 150-250 bpm; carotid massage: slows or
- 24. Supraventricular Arrhythmias
- 25. Rules of Aberrancy
- 26. Ventricular Arrhythmias Torsades de Pointes PVC’s
- 27. Atrial Enlargement Look at P waves in leads II and V1 Right atrial enlargement (P pulmonale)
- 28. Ventricular Hypertrophy Look at the QRS complexes in all leads Right ventricular hypertrophy (RVH) 1. RAD
- 29. Myocardial Infarction Dx – Hx, PE, serial cardiac enzymes, serial EKG’s 3 EKG stages of acute
- 30. Q Waves Criteria for significant Q waves Q wave > 0.04 seconds in duration Q wave
- 31. Localizing MI on EKG Inferior infarction – leads II, III, aVF Often caused by occlusion of
- 32. Localizing MI on EKG
- 33. ST segment Elevation Seen with evolving infarction, Prinzmetal’s angina Other causes – J point elevation, apical
- 34. Electrolyte Abnormalities on EKG Hyperkalemia – peaked T waves, prolonged PR, flattened P waves, widened QRS,
- 35. Drugs Digitalis Therapeutic levels – ST segment and T wave changes in leads with tall R
- 36. EKG ∆’s in other Cardiac Conditions Pericarditis – Diffuse ST segment elevations and T wave inversions;
- 37. EKG ∆’s in Pulmonary Disorders COPD – low voltage, right axis deviation, and poor R wave
- 38. EKG ∆’s in Other Conditions Hypothermia – Osborn waves, prolonged intervals, sinus bradycardia, slow atrial fibrillation,
- 39. Utter Confusion Verify lead placement Repeat EKG Repeat standardized process of EKG analysis- starting over from
- 40. Arrhythmia Indications to Consult Cardiology Diagnostic or management uncertainty Medications not controlling symptoms Patient is in
- 41. Care Considerations Prior to Cardiology Consult Thorough Hx and PE Basic labs EKG and repeat EKG
- 42. Pacemaker Considerations Third-degree (complete) AV block Symptomatic lesser degree AV block or bradycardia Sudden onset of
- 43. Osteopathic Considerations Treatments – Lymphatics – thoracic inlet, abdominal diaphragm, rib raising, lymphatic pumps Sympathetics (T1-T6)
- 44. Clinical Cases/EKG’s
- 45. Case 1 53 year old caucasian female with 4 day hx of severe central chest pain
- 46. Case 1 Diagnosis? EKG findings?
- 47. Case 1 Acute anterior ST-elevation MI with “tombstone” or “fireman’s hat” in V1-V4 Tx? Localization?
- 48. Case 1 PCI stenting of LAD Post-procedure = resolving ST elevation; loss of ominous tombstone effect;
- 49. Case 2 45 yo male presents with acute SOB s/p long vacation in Paris PMHx -
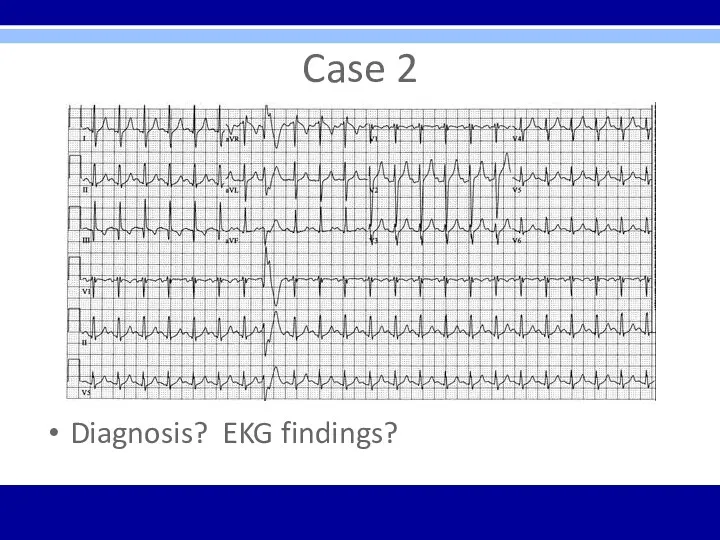
- 50. Case 2 Diagnosis? EKG findings?
- 51. Case 2 Acute PE with sinus tachycardia, a PVC, and S1Q3T3 pattern
- 52. Case 3 72 yo male presents to the office for evaluation prior to cataract surgery No
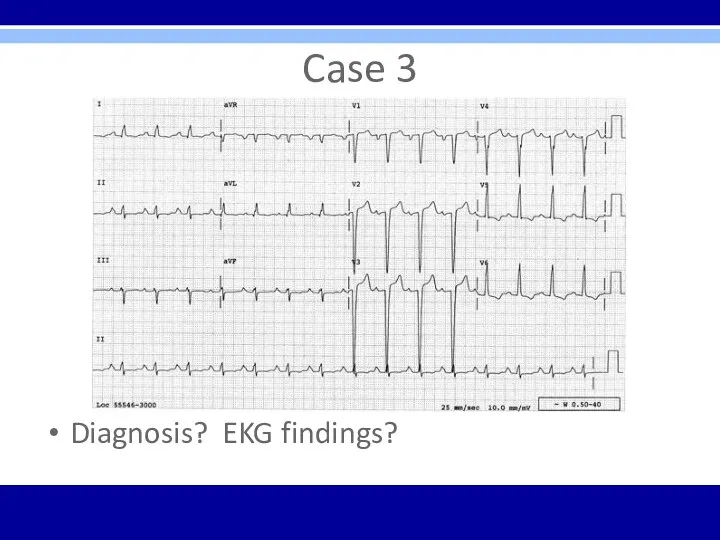
- 53. Case 3 Diagnosis? EKG findings?
- 54. Case 3 LVH – QRS voltage criteria in precordial leads and repolarization changes in V5, V6
- 55. Case 4 27 yo female presents to the ED with c/o chest discomfort and palpitations after
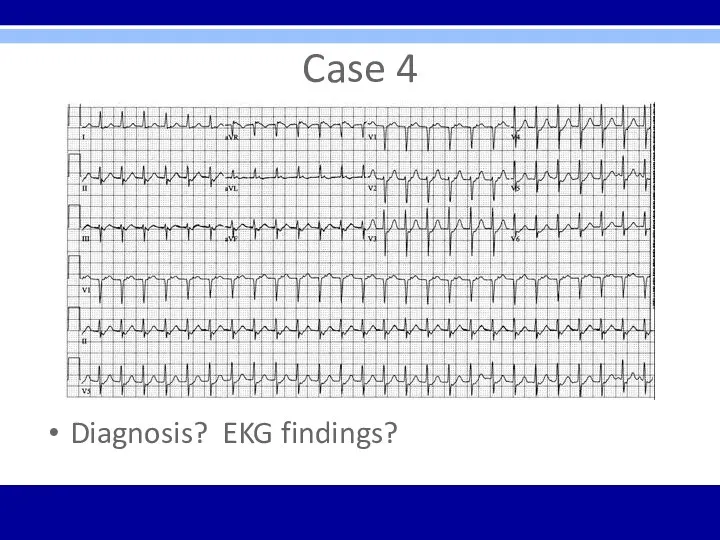
- 56. Case 4 Diagnosis? EKG findings?
- 57. Case 4 SVT – regular, narrow-QRS tachycardia, rate of 160 bpm
- 58. Case 5 46 yo male presents to ED with c/o severe HA persisting over 5 hours
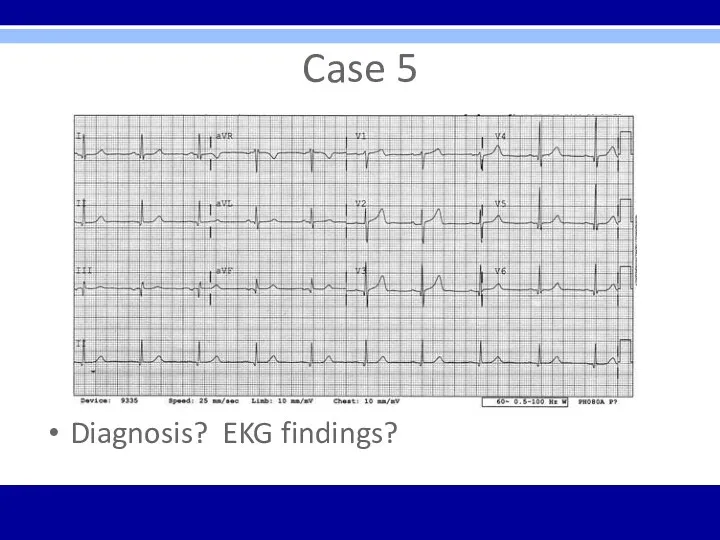
- 59. Case 5 Diagnosis? EKG findings?
- 60. Case 5 Normal EKG
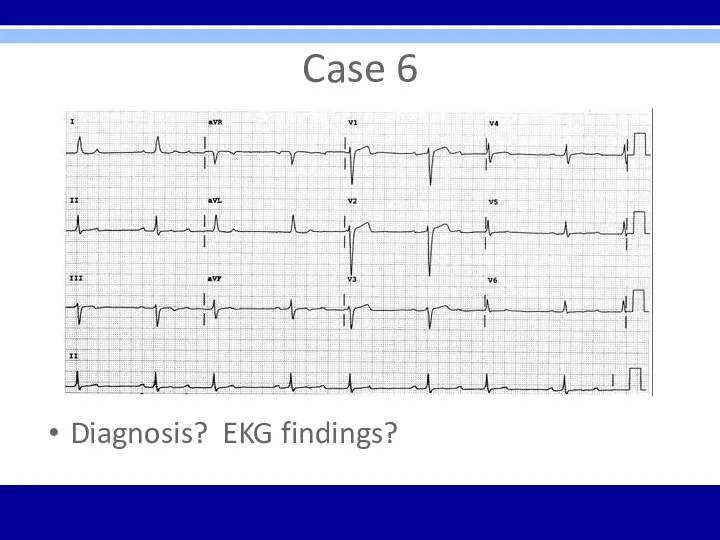
- 61. Case 6 56 yo female presents to family physician with c/o light-headedness and occasional flutter in
- 62. Case 6 Diagnosis? EKG findings?
- 63. Case 6 Second degree AV block – Mobitz Type I – Wenckebach (specifically 3:2 AV Wenckebach
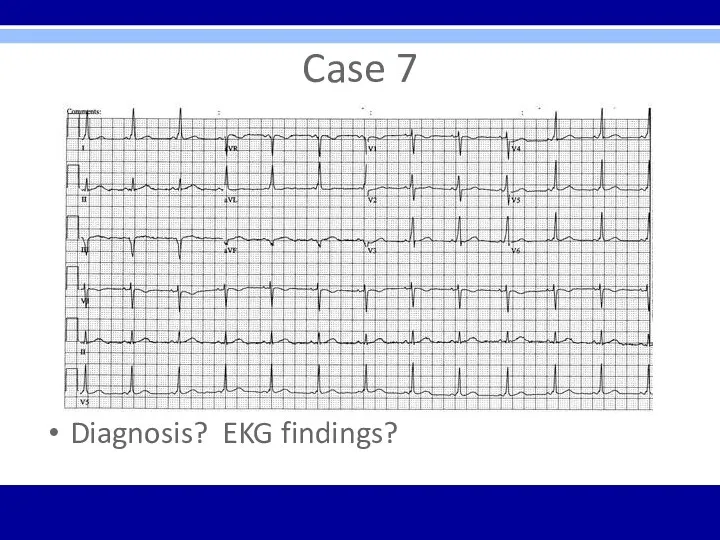
- 64. Case 7 28 yo male presents for commercial driver’s license (CDL) evaluation No complaints VSS; asymptomatic;
- 65. Case 7 Diagnosis? EKG findings?
- 66. Case 7 Typical preexcitation (WPW) pattern Short PR interval and delta waves in many leads Tx
- 67. Case 8 32 yo male presents to ED with c/o feeling sick for the last 6
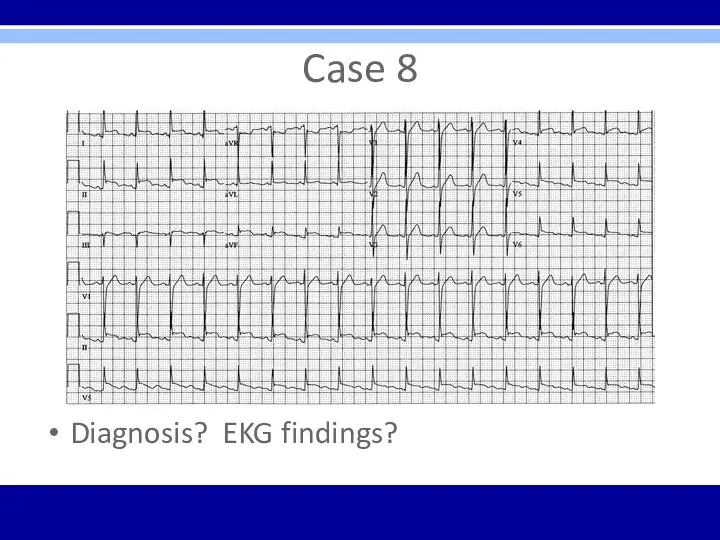
- 68. Case 8 Diagnosis? EKG findings?
- 69. Case 8 Acute pericarditis – diffuse ST elevation with PR segment depression is diagnostic
- 70. Case 9 67 yo male presents to his cardiologist for out-patient 6 week post-hospital visit Previous
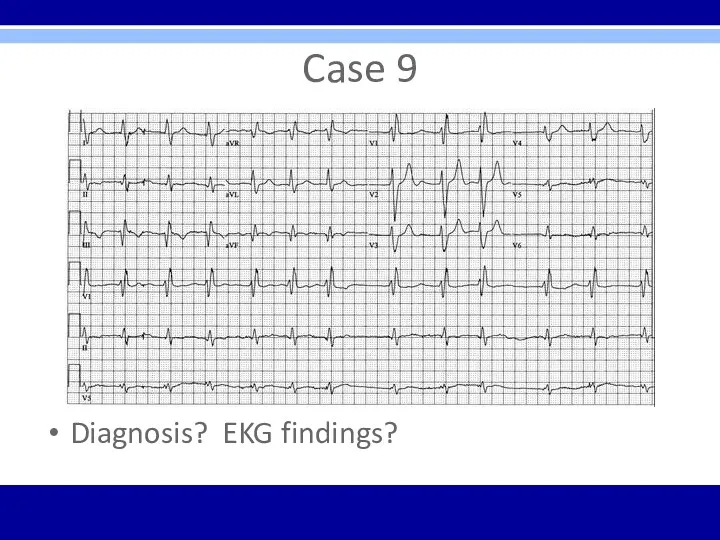
- 71. Case 9 Diagnosis? EKG findings?
- 72. Case 9 Atrial fibrillation – irregularly irregular without P waves RBBB – wide QRS with rsR’
- 73. Case 10 79 yo male brought to ED via EMS with chest pain, SOB, and near-syncope
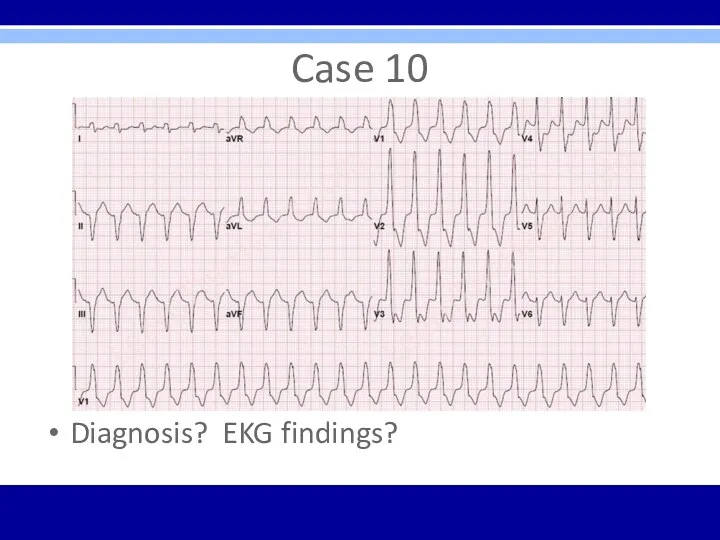
- 74. Case 10 Diagnosis? EKG findings?
- 75. Case 10 Monomorphic sustained ventricular tachycardia (VT) – could rapidly deteriorate into VF, torsades de pointes,
- 76. Case 11 82 yo female admitted to acute care hospital secondary to chest pain PMHx –
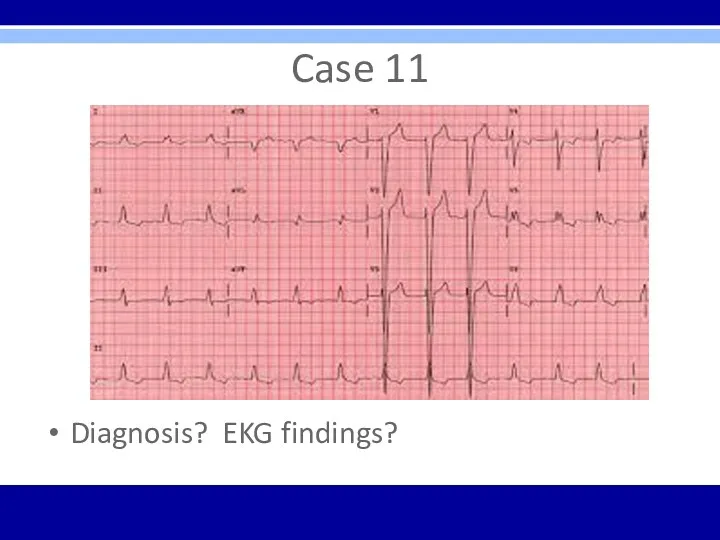
- 77. Case 11 Diagnosis? EKG findings?
- 78. Case 11 LBBB – wide QRS; broad, notched R wave in V5, V6 and I with
- 79. Case 12 59 yo male presents to ED diaphoretic and in distress PMHx – HTN, ESRD,
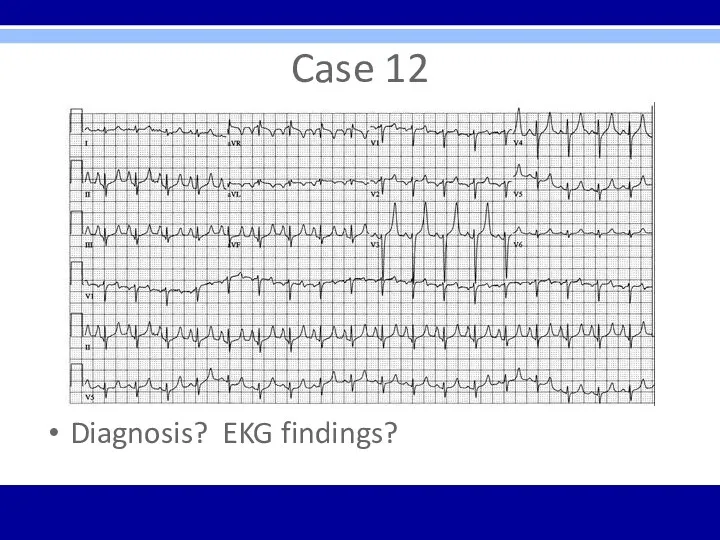
- 80. Case 12 Diagnosis? EKG findings?
- 81. Case 12 Hyperkalemia – tall peaked T waves present throughout; other progressive EKG changes may follow
- 82. Bonus Case 18 yo male undergoing military physical exam and evaluation prior to boot camp No
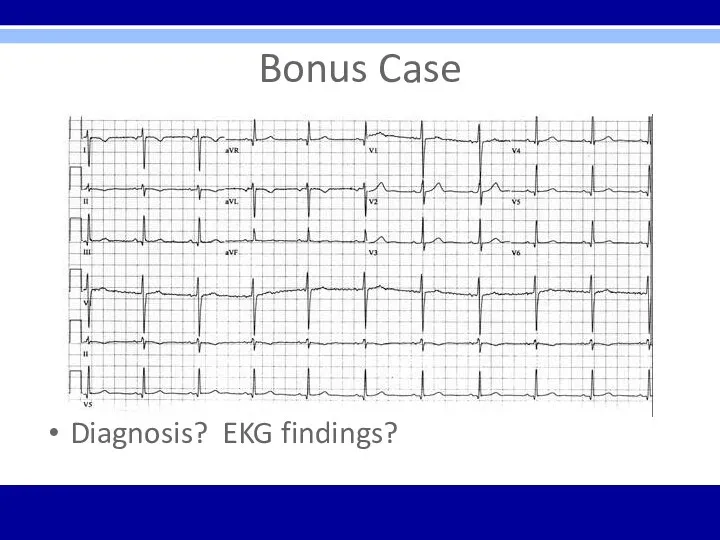
- 83. Bonus Case Diagnosis? EKG findings?
- 84. Bonus Case Reversed arm leads – inverted P waves in lead I with normal R wave
- 85. Board Exam Points EKG’s likely to have 1 main finding Clinical case likely included with each
- 86. Questions?
- 88. Скачать презентацию
Objectives
Review general method for EKG interpretation
Review specific points of “data gathering”
Objectives
Review general method for EKG interpretation
Review specific points of “data gathering”
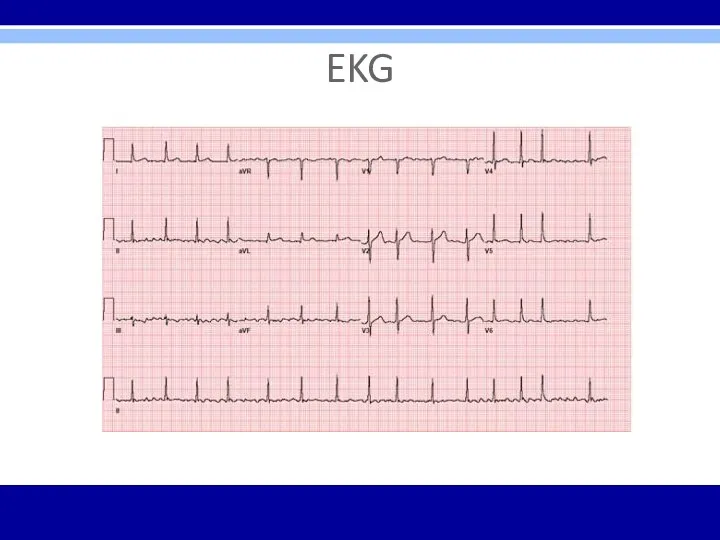
EKG
EKG
EKG – 12 Leads
Anterior Leads - V1, V2, V3, V4
Inferior Leads
EKG – 12 Leads
Anterior Leads - V1, V2, V3, V4
Inferior Leads
11 Step Method for Reading EKG’s
“Data Gathering” – steps 1-4
1. Standardization
11 Step Method for Reading EKG’s
“Data Gathering” – steps 1-4
1. Standardization
11 Step Method for Reading EKG’s
“Diagnoses”
5. Rhythm
6. Atrioventricular (AV) Block Disturbances
7.
11 Step Method for Reading EKG’s
“Diagnoses”
5. Rhythm
6. Atrioventricular (AV) Block Disturbances
7.
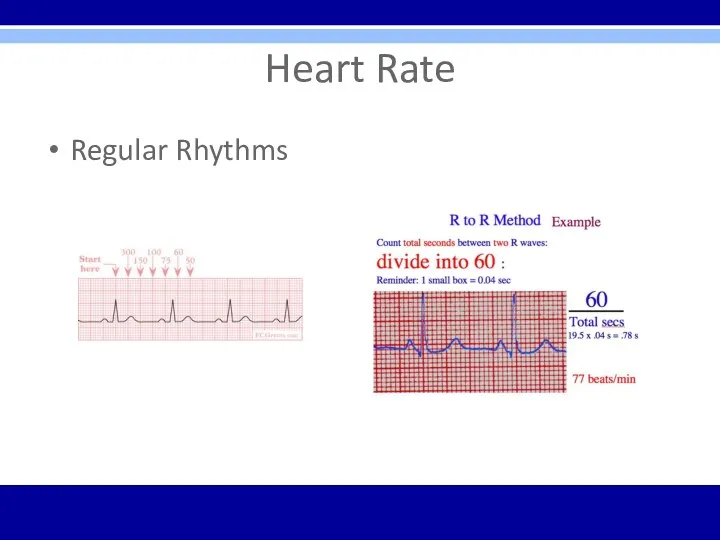
Heart Rate
Regular Rhythms
Heart Rate
Regular Rhythms
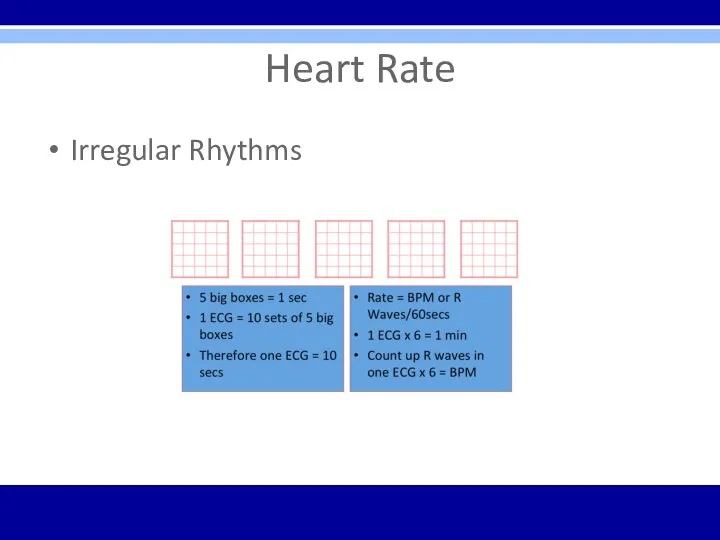
Heart Rate
Irregular Rhythms
Heart Rate
Irregular Rhythms
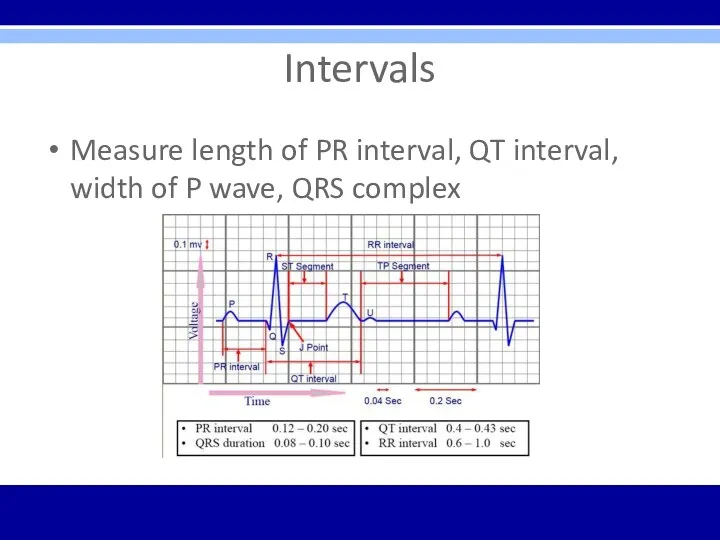
Intervals
Measure length of PR interval, QT interval, width of P wave,
Intervals
Measure length of PR interval, QT interval, width of P wave,
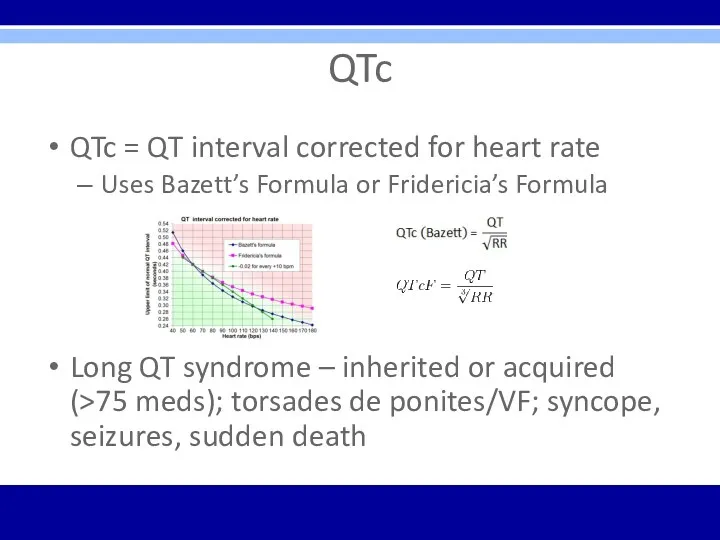
QTc
QTc = QT interval corrected for heart rate
Uses Bazett’s Formula or
QTc
QTc = QT interval corrected for heart rate
Uses Bazett’s Formula or
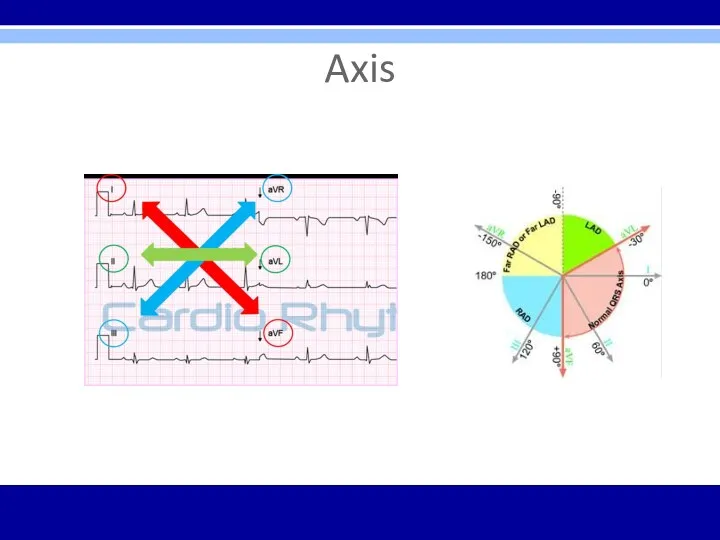
Axis
Axis
Rhythm
4 Questions
1. Are normal P waves present?
2. Are QRS complexes narrow
Rhythm
4 Questions
1. Are normal P waves present?
2. Are QRS complexes narrow
Types of Arrhythmias
Arrhythmias of sinus origin
Ectopic rhythms
Conduction Blocks
Preexcitation syndromes
Types of Arrhythmias
Arrhythmias of sinus origin
Ectopic rhythms
Conduction Blocks
Preexcitation syndromes
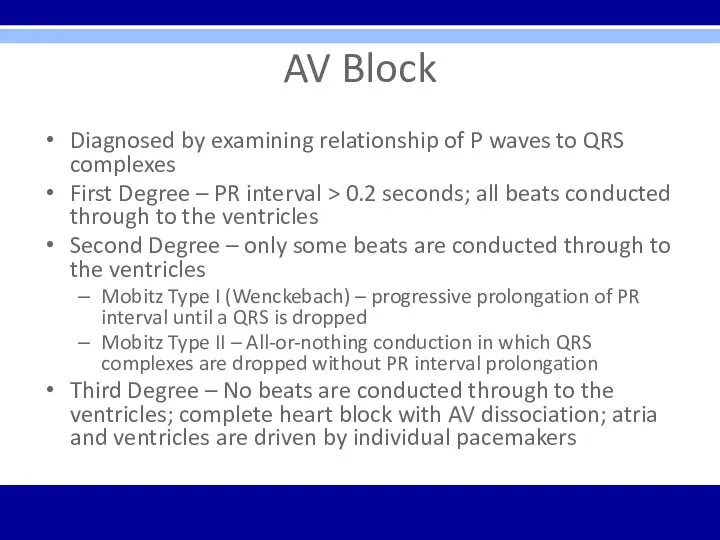
AV Block
Diagnosed by examining relationship of P waves to QRS complexes
First
AV Block
Diagnosed by examining relationship of P waves to QRS complexes
First
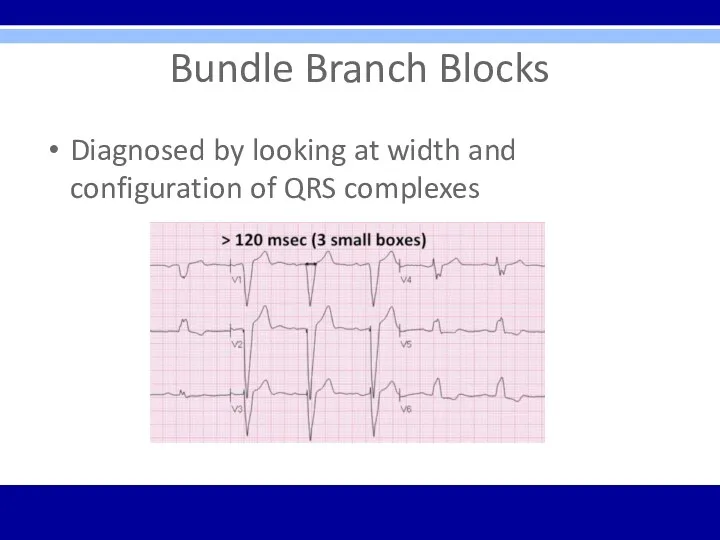
Bundle Branch Blocks
Diagnosed by looking at width and configuration of QRS
Bundle Branch Blocks
Diagnosed by looking at width and configuration of QRS
Bundle Branch Blocks
RBBB criteria:
1. QRS complex > 0.12 seconds
2. RSR’ in
Bundle Branch Blocks
RBBB criteria:
1. QRS complex > 0.12 seconds
2. RSR’ in
Bundle Branch Blocks
Bundle Branch Blocks
Hemiblocks
Diagnosed by looking at right or left axis deviation
Left Anterior Hemiblock
1.Normal
Hemiblocks
Diagnosed by looking at right or left axis deviation
Left Anterior Hemiblock
1.Normal
Bifascicular Block
RBBB with LAH
RBBB – QRS > 0.12 sec and
Bifascicular Block
RBBB with LAH
RBBB – QRS > 0.12 sec and
Preexcitation
Wolff-Parkinson-White (WPW) Syndrome
1. PR interval < 0.12 sec
2. Wide QRS complexes
3.
Preexcitation
Wolff-Parkinson-White (WPW) Syndrome
1. PR interval < 0.12 sec
2. Wide QRS complexes
3.
Preexcitation
WPW
LGL
Preexcitation
WPW
LGL
Supraventricular Arrhythmias
PSVT- regular; P waves retrograde if visible; rate 150-250 bpm;
Supraventricular Arrhythmias
PSVT- regular; P waves retrograde if visible; rate 150-250 bpm;
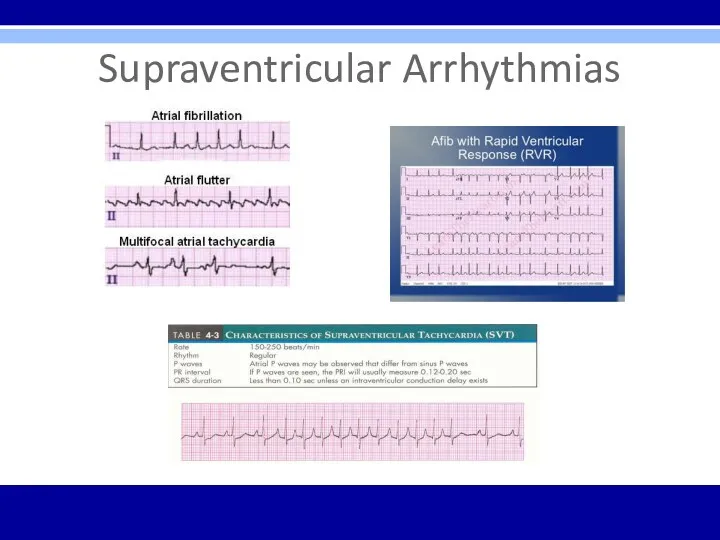
Supraventricular Arrhythmias
Supraventricular Arrhythmias
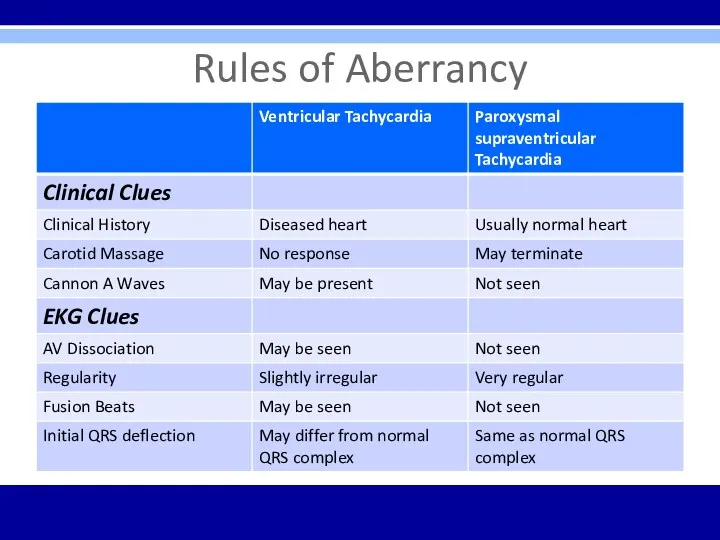
Rules of Aberrancy
Rules of Aberrancy
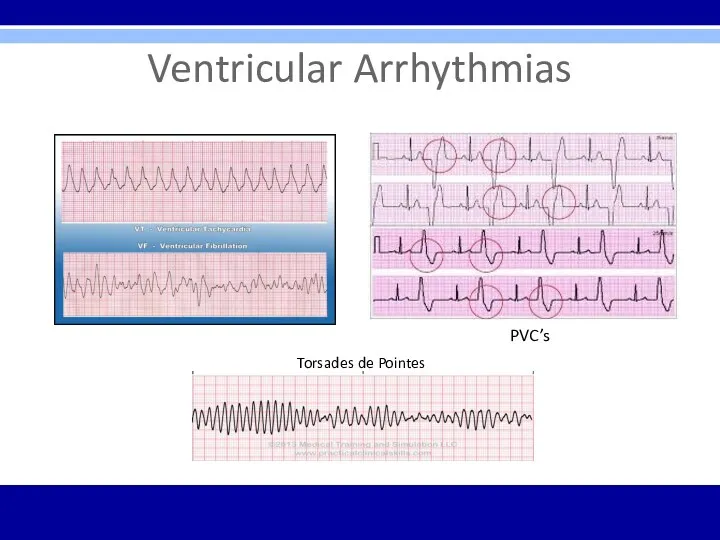
Ventricular Arrhythmias
Torsades de Pointes
PVC’s
Ventricular Arrhythmias
Torsades de Pointes
PVC’s
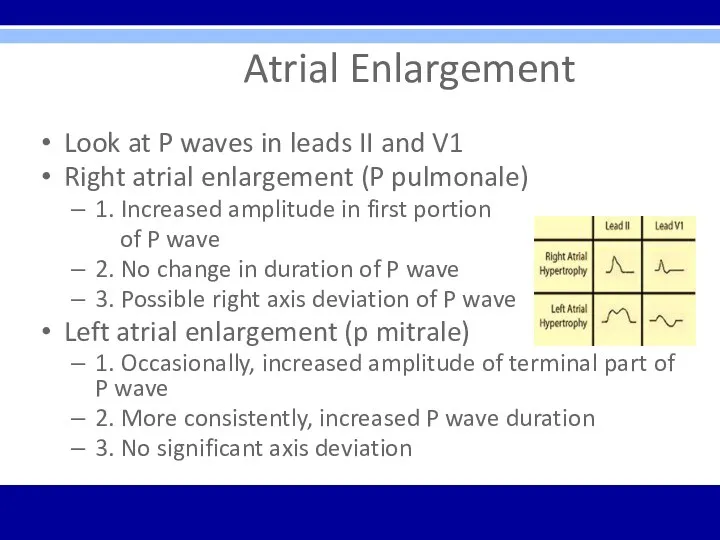
Atrial Enlargement
Look at P waves in leads II and V1
Right
Atrial Enlargement
Look at P waves in leads II and V1
Right
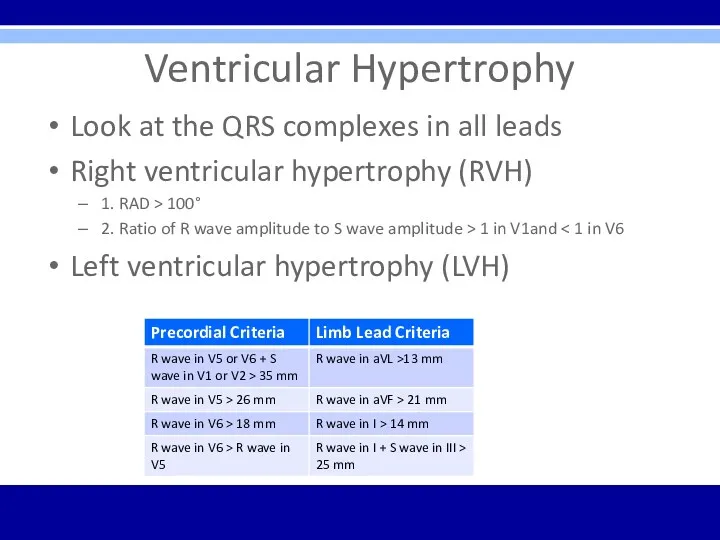
Ventricular Hypertrophy
Look at the QRS complexes in all leads
Right ventricular
Ventricular Hypertrophy
Look at the QRS complexes in all leads
Right ventricular
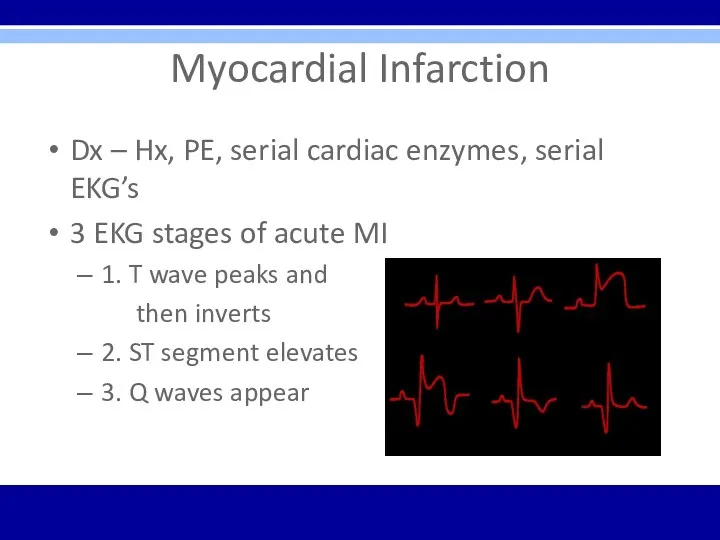
Myocardial Infarction
Dx – Hx, PE, serial cardiac enzymes, serial EKG’s
3 EKG
Myocardial Infarction
Dx – Hx, PE, serial cardiac enzymes, serial EKG’s
3 EKG
Q Waves
Criteria for significant Q waves
Q wave > 0.04 seconds in
Q Waves
Criteria for significant Q waves
Q wave > 0.04 seconds in
Localizing MI on EKG
Inferior infarction – leads II, III, aVF
Often caused
Localizing MI on EKG
Inferior infarction – leads II, III, aVF
Often caused
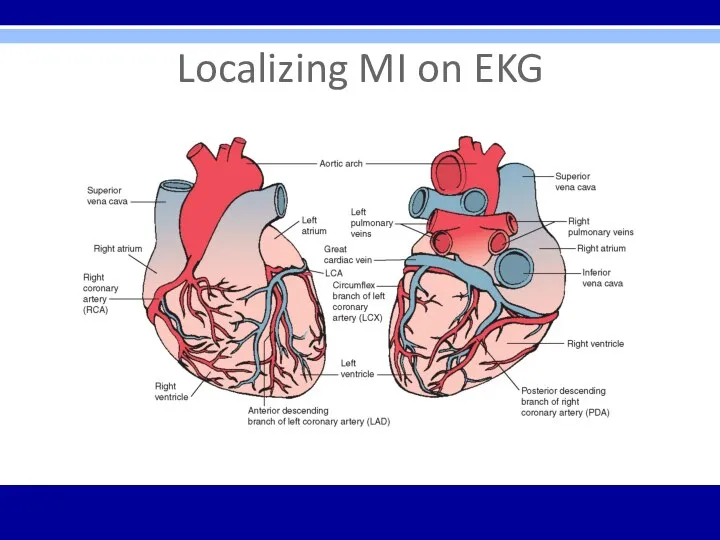
Localizing MI on EKG
Localizing MI on EKG
ST segment
Elevation
Seen with evolving infarction, Prinzmetal’s angina
Other causes – J
ST segment
Elevation
Seen with evolving infarction, Prinzmetal’s angina
Other causes – J
Electrolyte Abnormalities on EKG
Hyperkalemia – peaked T waves, prolonged PR, flattened
Electrolyte Abnormalities on EKG
Hyperkalemia – peaked T waves, prolonged PR, flattened
Drugs
Digitalis
Therapeutic levels – ST segment and T wave changes in
Drugs
Digitalis
Therapeutic levels – ST segment and T wave changes in
EKG ∆’s in other Cardiac Conditions
Pericarditis – Diffuse ST segment elevations
EKG ∆’s in other Cardiac Conditions
Pericarditis – Diffuse ST segment elevations
EKG ∆’s in Pulmonary Disorders
COPD – low voltage, right axis
EKG ∆’s in Pulmonary Disorders
COPD – low voltage, right axis
EKG ∆’s in Other Conditions
Hypothermia – Osborn waves, prolonged intervals, sinus
EKG ∆’s in Other Conditions
Hypothermia – Osborn waves, prolonged intervals, sinus
Utter Confusion
Verify lead placement
Repeat EKG
Repeat standardized process of EKG analysis- starting
Utter Confusion
Verify lead placement
Repeat EKG
Repeat standardized process of EKG analysis- starting
Arrhythmia Indications to Consult Cardiology
Diagnostic or management uncertainty
Medications not controlling symptoms
Patient
Arrhythmia Indications to Consult Cardiology
Diagnostic or management uncertainty
Medications not controlling symptoms
Patient
Care Considerations Prior to
Cardiology Consult
Thorough Hx and PE
Basic labs
EKG and
Care Considerations Prior to
Cardiology Consult
Thorough Hx and PE
Basic labs
EKG and
Pacemaker Considerations
Third-degree (complete) AV block
Symptomatic lesser degree AV block or bradycardia
Sudden
Pacemaker Considerations
Third-degree (complete) AV block
Symptomatic lesser degree AV block or bradycardia
Sudden
Osteopathic Considerations
Treatments –
Lymphatics – thoracic inlet, abdominal diaphragm, rib raising, lymphatic
Osteopathic Considerations
Treatments –
Lymphatics – thoracic inlet, abdominal diaphragm, rib raising, lymphatic
Clinical Cases/EKG’s
Clinical Cases/EKG’s
Case 1
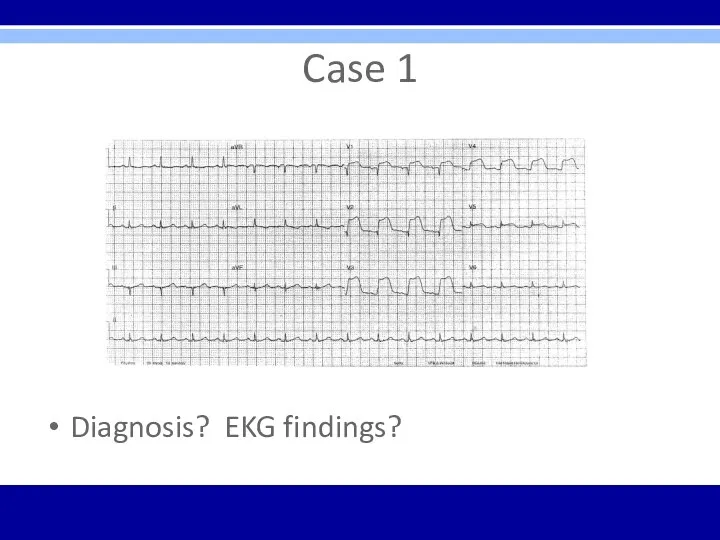
53 year old caucasian female with 4 day hx of
Case 1
53 year old caucasian female with 4 day hx of
Case 1
Diagnosis? EKG findings?
Case 1
Diagnosis? EKG findings?
Case 1
Acute anterior ST-elevation MI with “tombstone” or “fireman’s hat” in
Case 1
Acute anterior ST-elevation MI with “tombstone” or “fireman’s hat” in
Case 1
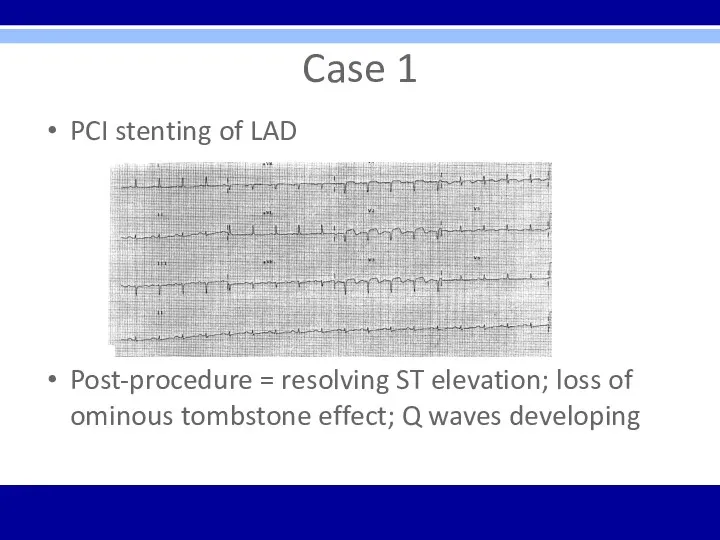
PCI stenting of LAD
Post-procedure = resolving ST elevation; loss of
Case 1
PCI stenting of LAD
Post-procedure = resolving ST elevation; loss of
Case 2
45 yo male presents with acute SOB s/p long vacation
Case 2
45 yo male presents with acute SOB s/p long vacation
Case 2
Diagnosis? EKG findings?
Case 2
Diagnosis? EKG findings?
Case 2
Acute PE with sinus tachycardia, a PVC, and S1Q3T3 pattern
Case 2
Acute PE with sinus tachycardia, a PVC, and S1Q3T3 pattern
Case 3
72 yo male presents to the office for evaluation prior
Case 3
72 yo male presents to the office for evaluation prior
Case 3
Diagnosis? EKG findings?
Case 3
Diagnosis? EKG findings?
Case 3
LVH – QRS voltage criteria in precordial leads and repolarization
Case 3
LVH – QRS voltage criteria in precordial leads and repolarization
Case 4
27 yo female presents to the ED with c/o chest
Case 4
27 yo female presents to the ED with c/o chest
Case 4
Diagnosis? EKG findings?
Case 4
Diagnosis? EKG findings?
Case 4
SVT – regular, narrow-QRS tachycardia, rate of 160 bpm
Case 4
SVT – regular, narrow-QRS tachycardia, rate of 160 bpm
Case 5
46 yo male presents to ED with c/o severe HA
Case 5
46 yo male presents to ED with c/o severe HA
Case 5
Diagnosis? EKG findings?
Case 5
Diagnosis? EKG findings?
Case 5
Normal EKG
Case 5
Normal EKG
Case 6
56 yo female presents to family physician with c/o light-headedness
Case 6
56 yo female presents to family physician with c/o light-headedness
Case 6
Diagnosis? EKG findings?
Case 6
Diagnosis? EKG findings?
Case 6
Second degree AV block – Mobitz Type I – Wenckebach
Case 6
Second degree AV block – Mobitz Type I – Wenckebach
Case 7
28 yo male presents for commercial driver’s license (CDL) evaluation
Case 7
28 yo male presents for commercial driver’s license (CDL) evaluation
Case 7
Diagnosis? EKG findings?
Case 7
Diagnosis? EKG findings?
Case 7
Typical preexcitation (WPW) pattern
Short PR interval and delta waves in
Case 7
Typical preexcitation (WPW) pattern
Short PR interval and delta waves in
Case 8
32 yo male presents to ED with c/o feeling sick
Case 8
32 yo male presents to ED with c/o feeling sick
Case 8
Diagnosis? EKG findings?
Case 8
Diagnosis? EKG findings?
Case 8
Acute pericarditis – diffuse ST elevation with PR segment depression
Case 8
Acute pericarditis – diffuse ST elevation with PR segment depression
Case 9
67 yo male presents to his cardiologist for out-patient 6
Case 9
67 yo male presents to his cardiologist for out-patient 6
Case 9
Diagnosis? EKG findings?
Case 9
Diagnosis? EKG findings?
Case 9
Atrial fibrillation – irregularly irregular without P waves
RBBB –
Case 9
Atrial fibrillation – irregularly irregular without P waves
RBBB –
Case 10
79 yo male brought to ED via EMS with chest
Case 10
79 yo male brought to ED via EMS with chest
Case 10
Diagnosis? EKG findings?
Case 10
Diagnosis? EKG findings?
Case 10
Monomorphic sustained ventricular tachycardia (VT) – could rapidly deteriorate into
Case 10
Monomorphic sustained ventricular tachycardia (VT) – could rapidly deteriorate into
Case 11
82 yo female admitted to acute care hospital secondary to
Case 11
82 yo female admitted to acute care hospital secondary to
Case 11
Diagnosis? EKG findings?
Case 11
Diagnosis? EKG findings?
Case 11
LBBB – wide QRS; broad, notched R wave in V5,
Case 11
LBBB – wide QRS; broad, notched R wave in V5,
Case 12
59 yo male presents to ED diaphoretic and in distress
PMHx
Case 12
59 yo male presents to ED diaphoretic and in distress
PMHx
Case 12
Diagnosis? EKG findings?
Case 12
Diagnosis? EKG findings?
Case 12
Hyperkalemia – tall peaked T waves present throughout; other progressive
Case 12
Hyperkalemia – tall peaked T waves present throughout; other progressive
Bonus Case
18 yo male undergoing military physical exam and evaluation prior
Bonus Case
18 yo male undergoing military physical exam and evaluation prior
Bonus Case
Diagnosis? EKG findings?
Bonus Case
Diagnosis? EKG findings?
Bonus Case
Reversed arm leads – inverted P waves in lead I
Bonus Case
Reversed arm leads – inverted P waves in lead I
Board Exam Points
EKG’s likely to have 1 main finding
Clinical case likely
Board Exam Points
EKG’s likely to have 1 main finding
Clinical case likely
Questions?
Questions?
 Специфическая (антидотная) фармакотерапия острых отравлений
Специфическая (антидотная) фармакотерапия острых отравлений Стоматологическое просвещение. Принципы разработки, внедрения и оценки эффективности программ профилактики
Стоматологическое просвещение. Принципы разработки, внедрения и оценки эффективности программ профилактики Психогенные расстройства
Психогенные расстройства Роль медицинской сестры в подготовке пациента к плановой операции
Роль медицинской сестры в подготовке пациента к плановой операции Первый патронаж новорождённого
Первый патронаж новорождённого Периостит челюстных костей клиника, диагностика и лечение
Периостит челюстных костей клиника, диагностика и лечение Сосудистые заболевания спинного мозга
Сосудистые заболевания спинного мозга Ас қорыту жүйесі. Сүт тістерінің құрылыс ерекшелігі. Тіс алмасу
Ас қорыту жүйесі. Сүт тістерінің құрылыс ерекшелігі. Тіс алмасу Неонатальный скрининг
Неонатальный скрининг Нозологическая диагностика когнитивных нарушений
Нозологическая диагностика когнитивных нарушений Дифференциальная диагностика муковисцидоза. Причины ложноположительных результатов скриннинга на муковисцидоз
Дифференциальная диагностика муковисцидоза. Причины ложноположительных результатов скриннинга на муковисцидоз Влияние компьютера на здоровье человека
Влияние компьютера на здоровье человека Терапия ожирения. Групповой метод
Терапия ожирения. Групповой метод Микроорганизмд ер
Микроорганизмд ер ЛФК и массаж при остеохондрозе
ЛФК и массаж при остеохондрозе Физиотерапия при остеомиелите, альвеолите
Физиотерапия при остеомиелите, альвеолите Митральды стеноз
Митральды стеноз Несахарный диабет
Несахарный диабет Желатинді капсулалардағы дәрілік заттар технологиясы
Желатинді капсулалардағы дәрілік заттар технологиясы Ревматоидный артрит
Ревматоидный артрит Теоретические основы сестринского дела
Теоретические основы сестринского дела Общая фармакология
Общая фармакология Нанотехнологии в хирургии
Нанотехнологии в хирургии Гнатология и функциональная диагностика ВНЧС
Гнатология и функциональная диагностика ВНЧС Кардиогенный шок. Дефиниции: термины и понятия
Кардиогенный шок. Дефиниции: термины и понятия Первая медицинская помощь в походе
Первая медицинская помощь в походе Цитокины
Цитокины Кровотечения во второй половине беременности
Кровотечения во второй половине беременности