Chronic middle suppurative otitis. Nonsuppurative pathology of the chronic ear: sensoneural deafness презентация
- Chronic middle suppurative otitis. Nonsuppurative pathology of the chronic ear: sensoneural deafness

Содержание
- 2. The actuality of the theme. Chronic purulent middle otitis is the most frequent disease of the
- 3. Chronic suppurative otitis media is a common disease. Chronic suppurative otitis media is characterized by persistent
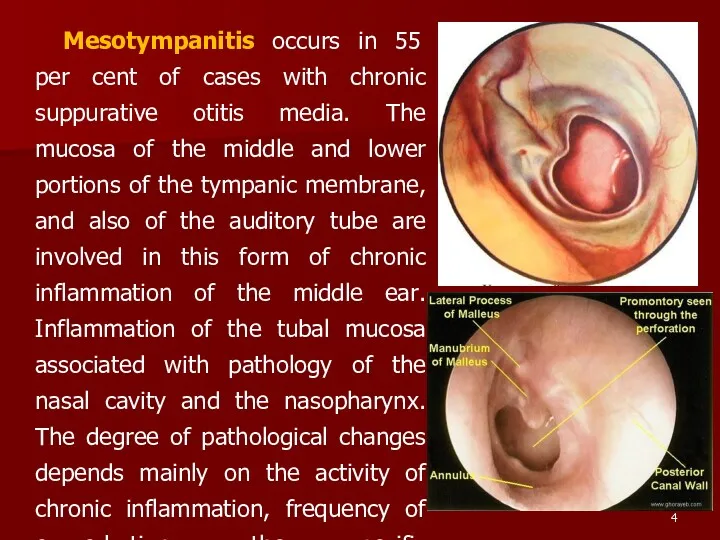
- 4. Mesotympanitis occurs in 55 per cent of cases with chronic suppurative otitis media. The mucosa of
- 5. Otoscopy in mesotympanitis reveals intact flaccid part of the tympanic membrane and the presence of a
- 6. The discharge from the ear can persist for years without causing any serious complications. Otopyorrhoea can
- 7. Prognosis is usually favourable, provided a systematic and rational general and local treatment is given. But
- 8. If the patient feels the taste of the medicine in the mouth, it indicates that the
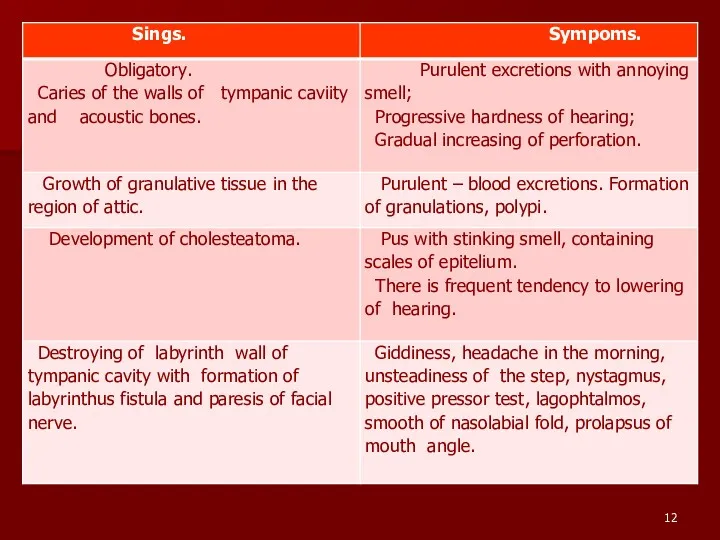
- 9. Epitympanitis (atticitis). The inflammation is mainly localized in the epitympanum, the attic of the tympanum. A
- 10. A sample of cholesteatoma or pus can be extracted from the attic on the tip of
- 11. The hearing function often decreases only slightly. If the neurotic component joins, hearing can be impaired
- 13. Treatment of chronic suppurative epitympanitis is more difficult than of chronic suppurative mesotympanitis. Conservative treatment is
- 14. The operation begins with opening the antrum, as in mastoidectomy; next follows the removal of the
- 15. The operation is rounded off with a plastic repair in order that the walls of the
- 16. Tympanoplasty is the surgical reconstruction and building of new sound conduction apparatus. It is an operation
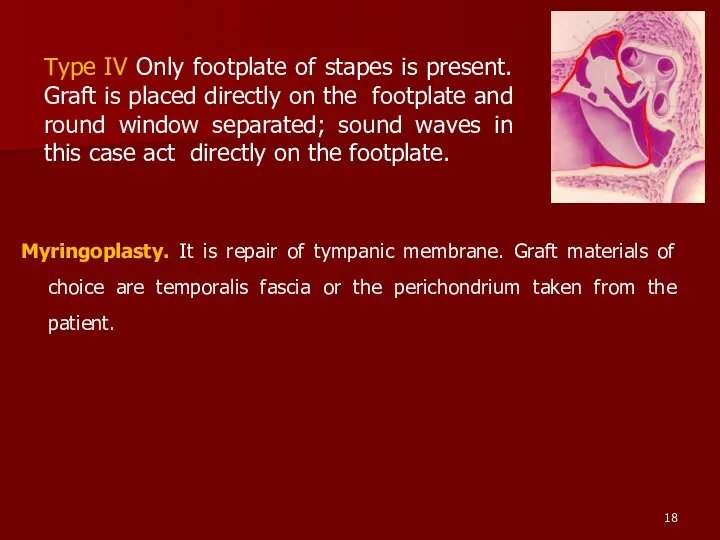
- 17. Types of tympanoplasty. Wullstein classified tympanoplasty into five types. Type I Defect is perforation of tympanic
- 18. Myringoplasty. It is repair of tympanic membrane. Graft materials of choice are temporalis fascia or the
- 19. VESTIBULOCOCHLEAR (COCHLEAR) NEURITIS. Neuritis of the vestibulocochlear (auditory) nerve is a collective term implying affection of
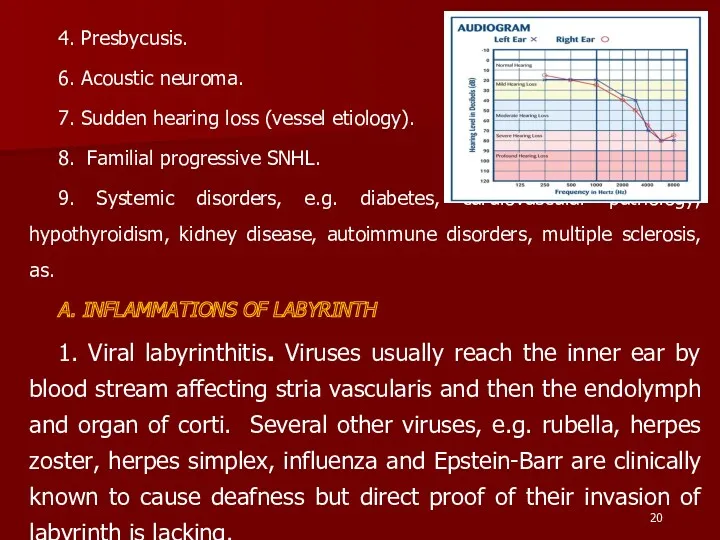
- 20. 4. Presbycusis. 6. Acoustic neuroma. 7. Sudden hearing loss (vessel etiology). 8. Familial progressive SNHL. 9.
- 21. 2. Bacterial. Bacterial infections reach labyrinth through the middle ear (tympanogenic) or through CSF (meningogenic). Sensorineural
- 22. They cause selective destruction of outer hair cells, starting at the basal coil and progressing onto
- 23. Hearing loss due to salicylates is reversible after the drug is discontinued. 4. Quinine. Ototoxic symptoms
- 24. D. NOISE TRAUMA. Hearing loss associated with exposure to noise has been well-known in boiler makers,
- 25. F. PRESBYCUSIS. Sensorineural hearing loss associated with physiological aging process in the ear is called presbycusis.
- 26. Less frequently the patients complain of permanent or transient buzzing (ringing) noise in the ears (tinnitus).
- 27. Characteristics of sensorinural hearing loss are : 1. A positive Rinne test, i.e. air conduction better
- 28. A doctor prescribes to these patients a confinement to bed, a limit of salt and a
- 29. Treatment of toxic neuritis first of all includes prevention of further ingress of toxins into the
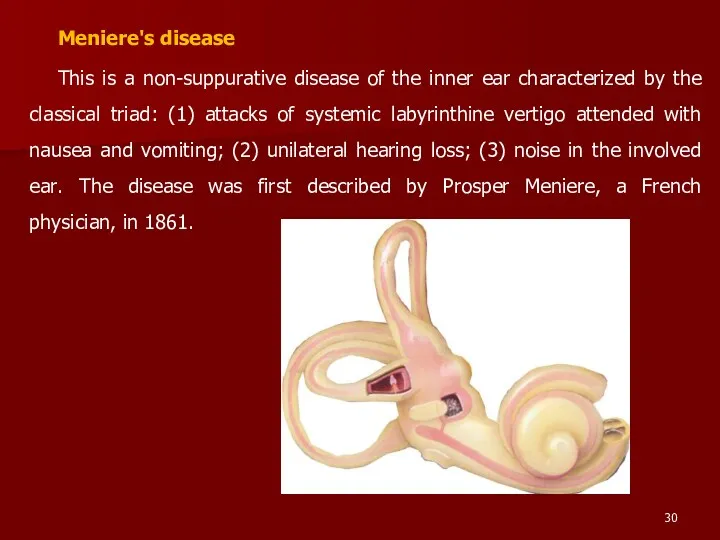
- 30. Meniere's disease This is a non-suppurative disease of the inner ear characterized by the classical triad:
- 31. Fluctuation of hearing is a leading diagnostic sign of the auditory disorder: the hearing can improve
- 32. Treatment. The polyaetiological origin of the disease accounts for the multitude of methods of treating it.
- 33. Treatment in the period between attack 1. I/v. driply pour 4 % a solution of a
- 34. Surgical treatment It is used only when medical treatment fails. Conservative procedures. They are used in
- 35. OTOSCLEROSIS Otosclerosis is a frequent cause of deafness (it occurs in more than 0.5 per cent
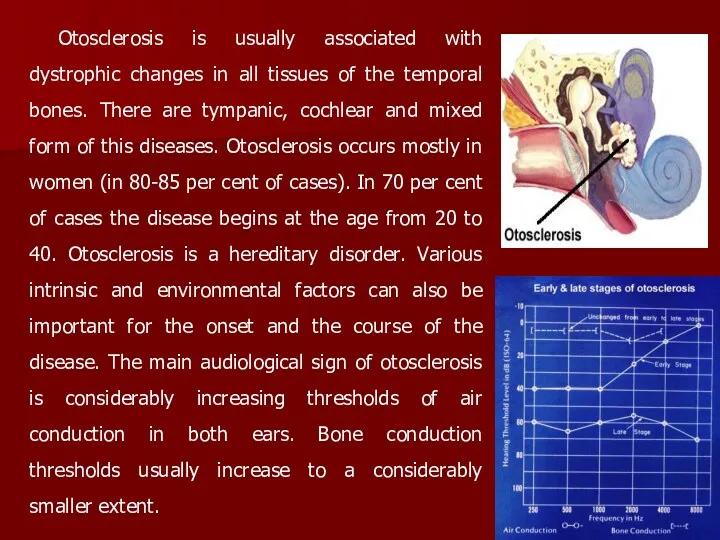
- 36. Otosclerosis is usually associated with dystrophic changes in all tissues of the temporal bones. There are
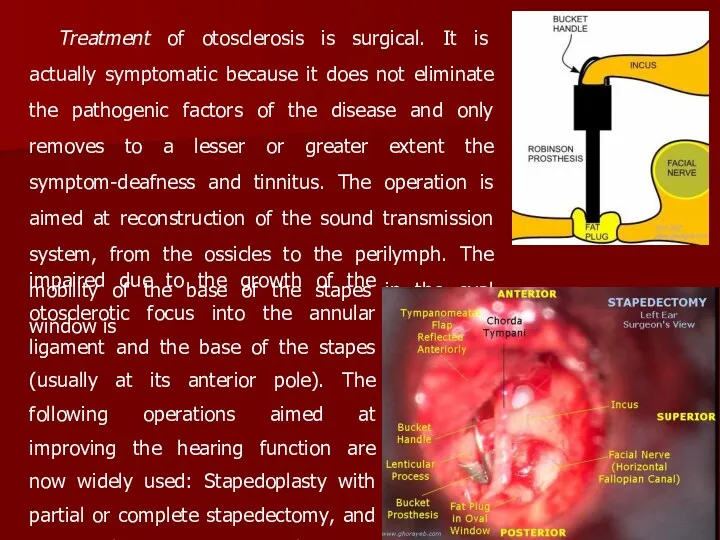
- 37. Treatment of otosclerosis is surgical. It is actually symptomatic because it does not eliminate the pathogenic
- 39. Скачать презентацию
The actuality of the theme.
Chronic purulent middle otitis is the
The actuality of the theme.
Chronic purulent middle otitis is the
Chronic suppurative otitis media is a common disease. Chronic suppurative otitis
Chronic suppurative otitis media is a common disease. Chronic suppurative otitis
Mesotympanitis occurs in 55 per cent of cases with chronic suppurative
Mesotympanitis occurs in 55 per cent of cases with chronic suppurative
Otoscopy in mesotympanitis reveals intact flaccid part of the tympanic membrane
Otoscopy in mesotympanitis reveals intact flaccid part of the tympanic membrane
The discharge from the ear can persist for years without
The discharge from the ear can persist for years without
Prognosis is usually favourable, provided a systematic and rational general and
Prognosis is usually favourable, provided a systematic and rational general and
If the patient feels the taste of the medicine in the
If the patient feels the taste of the medicine in the
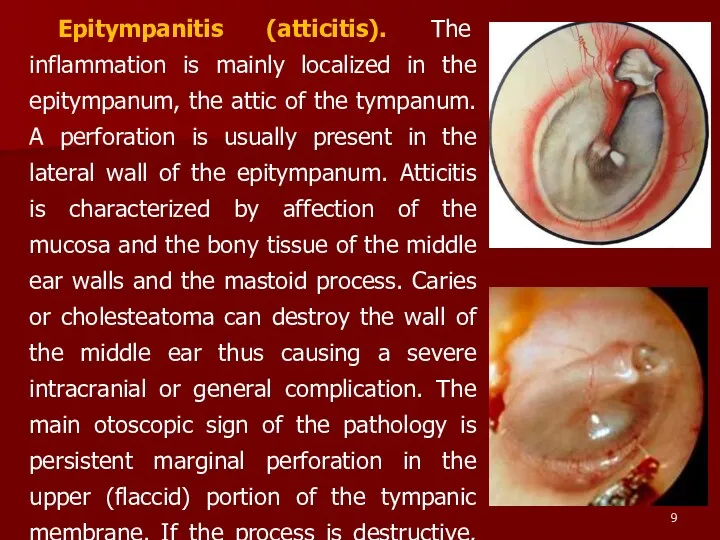
Epitympanitis (atticitis). The inflammation is mainly localized in the epitympanum, the
Epitympanitis (atticitis). The inflammation is mainly localized in the epitympanum, the
A sample of cholesteatoma or pus can be extracted from
A sample of cholesteatoma or pus can be extracted from
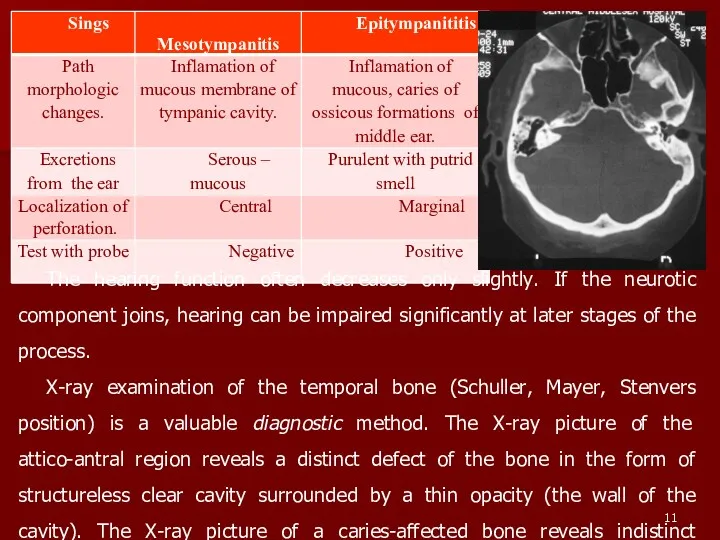
The hearing function often decreases only slightly. If the neurotic component
The hearing function often decreases only slightly. If the neurotic component
Treatment of chronic suppurative epitympanitis is more difficult than of chronic
Treatment of chronic suppurative epitympanitis is more difficult than of chronic
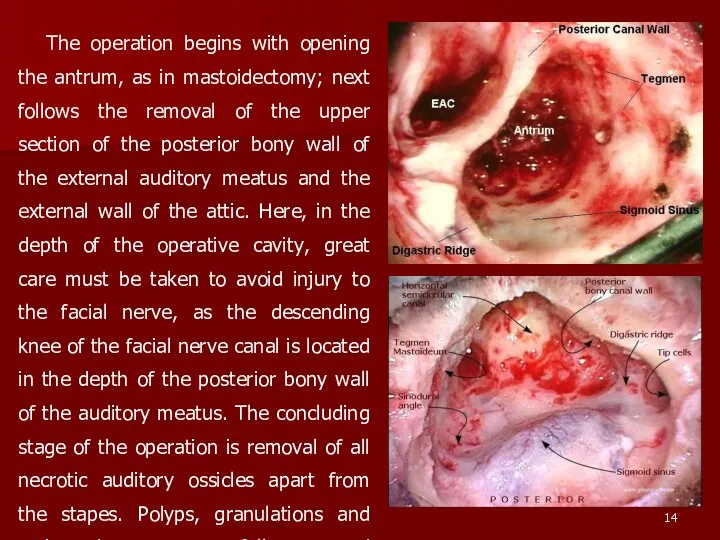
The operation begins with opening the antrum, as in mastoidectomy; next
The operation begins with opening the antrum, as in mastoidectomy; next
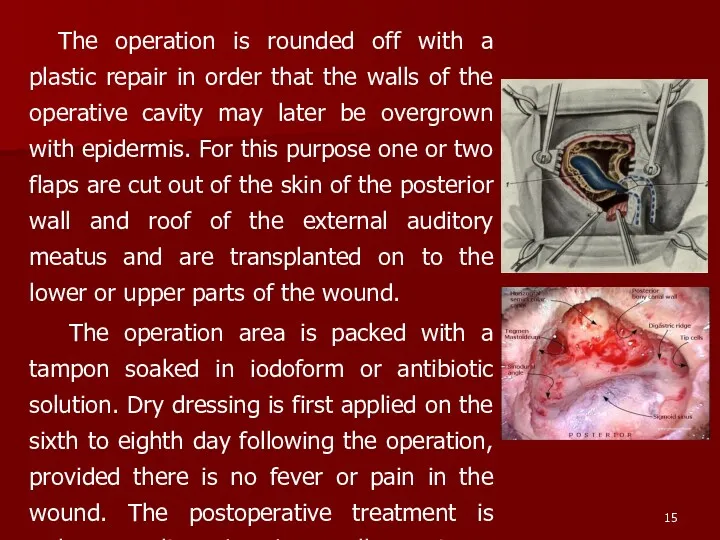
The operation is rounded off with a plastic repair in order
The operation is rounded off with a plastic repair in order
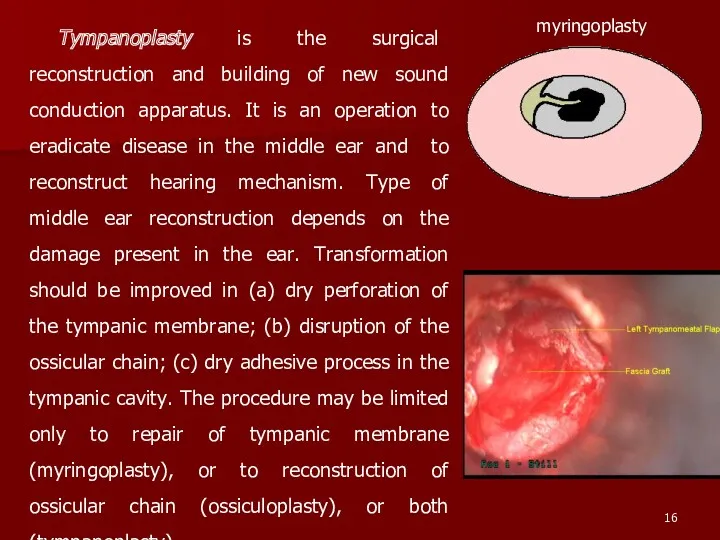
Tympanoplasty is the surgical reconstruction and building of new sound conduction
Tympanoplasty is the surgical reconstruction and building of new sound conduction
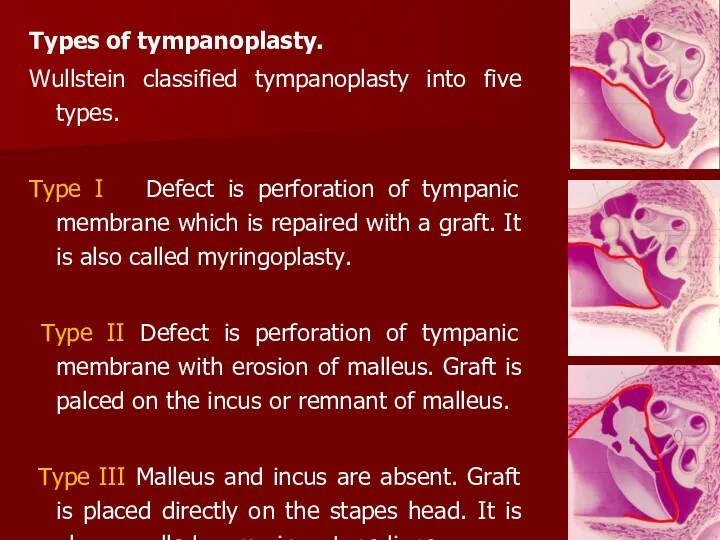
Types of tympanoplasty.
Wullstein classified tympanoplasty into five types.
Type I
Types of tympanoplasty.
Wullstein classified tympanoplasty into five types.
Type I
Myringoplasty. It is repair of tympanic membrane. Graft materials of choice
VESTIBULOCOCHLEAR (COCHLEAR) NEURITIS. Neuritis of the vestibulocochlear (auditory) nerve is a
VESTIBULOCOCHLEAR (COCHLEAR) NEURITIS. Neuritis of the vestibulocochlear (auditory) nerve is a
4. Presbycusis.
6. Acoustic neuroma.
7. Sudden hearing loss (vessel etiology).
8. Familial
4. Presbycusis.
6. Acoustic neuroma.
7. Sudden hearing loss (vessel etiology).
8. Familial
2. Bacterial. Bacterial infections reach labyrinth through the middle ear (tympanogenic)
2. Bacterial. Bacterial infections reach labyrinth through the middle ear (tympanogenic)
They cause selective destruction of outer hair cells, starting at the
They cause selective destruction of outer hair cells, starting at the
Hearing loss due to salicylates is reversible after the drug is
Hearing loss due to salicylates is reversible after the drug is
D. NOISE TRAUMA. Hearing loss associated with exposure to noise has
D. NOISE TRAUMA. Hearing loss associated with exposure to noise has
F. PRESBYCUSIS. Sensorineural hearing loss associated with physiological aging process in
F. PRESBYCUSIS. Sensorineural hearing loss associated with physiological aging process in
Less frequently the patients complain of permanent or transient buzzing (ringing)
Less frequently the patients complain of permanent or transient buzzing (ringing)
Characteristics of sensorinural hearing loss are :
1. A positive Rinne test,
Characteristics of sensorinural hearing loss are :
1. A positive Rinne test,
A doctor prescribes to these patients a confinement to bed, a
A doctor prescribes to these patients a confinement to bed, a
Treatment of toxic neuritis first of all includes prevention of further
Treatment of toxic neuritis first of all includes prevention of further
Meniere's disease
This is a non-suppurative disease of the inner ear characterized
Meniere's disease
This is a non-suppurative disease of the inner ear characterized
Fluctuation of hearing is a leading diagnostic sign of the auditory
Fluctuation of hearing is a leading diagnostic sign of the auditory
Treatment. The polyaetiological origin of the disease accounts for the multitude
Treatment. The polyaetiological origin of the disease accounts for the multitude
Treatment in the period between attack
1. I/v. driply pour 4 %
Treatment in the period between attack
1. I/v. driply pour 4 %
Surgical treatment
It is used only when medical treatment fails.
Conservative procedures. They
Surgical treatment
It is used only when medical treatment fails.
Conservative procedures. They
OTOSCLEROSIS Otosclerosis is a frequent cause of deafness (it occurs in
OTOSCLEROSIS Otosclerosis is a frequent cause of deafness (it occurs in
Otosclerosis is usually associated with dystrophic changes in all tissues of
Otosclerosis is usually associated with dystrophic changes in all tissues of
Treatment of otosclerosis is surgical. It is actually symptomatic because it
Treatment of otosclerosis is surgical. It is actually symptomatic because it
 Травмы органов и тканей челюстнолицевой области у детей
Травмы органов и тканей челюстнолицевой области у детей Вирус гепатита А (ВГА, HAV)
Вирус гепатита А (ВГА, HAV) Загальна характеристика вірусних гепатитів. Вірусні гепатити з фекально-оральним механізмом зараження
Загальна характеристика вірусних гепатитів. Вірусні гепатити з фекально-оральним механізмом зараження Патофизиология системы внешнего дыхания
Патофизиология системы внешнего дыхания Жүйелі аурулар және зат алмасу ауруларында ауыз қуысы кілегей қабығының зақымдануы. Клиникасы, диагностикасы, емі
Жүйелі аурулар және зат алмасу ауруларында ауыз қуысы кілегей қабығының зақымдануы. Клиникасы, диагностикасы, емі Лучевая анатомия позвоночника
Лучевая анатомия позвоночника Лямблиоз
Лямблиоз Эргономические основы организации рабочего места врача-стоматолога. Работа врача с помощником в четыре руки
Эргономические основы организации рабочего места врача-стоматолога. Работа врача с помощником в четыре руки Антенатальды кезеңдегі инвазивті тексеру
Антенатальды кезеңдегі инвазивті тексеру Национальный институт рака им. Дж. Паскале
Национальный институт рака им. Дж. Паскале Хроническая венозная недостаточность
Хроническая венозная недостаточность Холиномиметические средства (Лекция № 4)
Холиномиметические средства (Лекция № 4) Сarec cистема, Cad/Cem система, свойства, применение
Сarec cистема, Cad/Cem система, свойства, применение Работа в очаге туберкулёзной инфекции
Работа в очаге туберкулёзной инфекции Пиодермии. Этиология. Классификация. Клиника
Пиодермии. Этиология. Классификация. Клиника Физиология эндокринной системы
Физиология эндокринной системы Жинақталған салыстыру. Бонферронидің түзетуімен. Стьюдент белгісі
Жинақталған салыстыру. Бонферронидің түзетуімен. Стьюдент белгісі Образ врача. Нравственные принципы профессии врача
Образ врача. Нравственные принципы профессии врача Дегидрогеназалардың нуклеотидті. Коферменттері. НАД, НАДФ, ФАД нуклеозидті коферменттер
Дегидрогеназалардың нуклеотидті. Коферменттері. НАД, НАДФ, ФАД нуклеозидті коферменттер Кожные проявления аллергии. Клинические аспекты и принципы лечения
Кожные проявления аллергии. Клинические аспекты и принципы лечения Роль медицинской сестры в преодолении деформации личности онкологических больных разных возрастов
Роль медицинской сестры в преодолении деформации личности онкологических больных разных возрастов Комплексна оцінка здоров’я населення. Методика вивчення та оцінка чинників, що впливають на здоров’я населення
Комплексна оцінка здоров’я населення. Методика вивчення та оцінка чинників, що впливають на здоров’я населення Принцип действия лазерного луча. Терапия сосудистых патологий
Принцип действия лазерного луча. Терапия сосудистых патологий Задачи принципы организации диетического питания
Задачи принципы организации диетического питания Развитие медицины в России в 19 веке. Хирургия
Развитие медицины в России в 19 веке. Хирургия Сердце. Основные диагностические алгоритмы
Сердце. Основные диагностические алгоритмы Зәр және жыныстық жүйесінің қатерсіз және қатерлі ісіктері
Зәр және жыныстық жүйесінің қатерсіз және қатерлі ісіктері Всемирный день здоровья
Всемирный день здоровья