- Current Treatment Strategies in Colorectal Cancer

Содержание
- 2. Epidemiology 3-d most common cancer in men 3-d most common cancer in women Worldwide: >1 million
- 3. Colorectal Cancer Some facts 15% to 25% have metastases at diagnosis Up to 50% will develop
- 4. Epidemiology CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages 11-30, 17 JAN 2013
- 5. Epidemiologic Data in Israel Every year ~3200 new cases of colon cancer patients in Israel 25%
- 6. Prevalence estimates in unscreened population Individuals aged 50-y or older: 0.5 % chance for invasive CRC
- 7. Risk factors for colorectal Cancer Hereditary colon cancer syndromes Inflammatory bowel disease Personal history of CRC
- 8. Staging of CRC is used to monitor the course of disease and to assess the most
- 9. Treatment options for CRC Surgery Medical Chemotherapy Targeted therapies Radiotherapy
- 10. Surgery For invasive Carcinoma of the colon stage I,II,III, surgery is the only curative treatment Surgical
- 11. STAGE III colon carcinoma ( T1-4N1-2) 5-y Overall Survival benefit ~ 10% (oxaliplatin+5FU/Capecitabine) STAGE II colon
- 12. Oncotype DX® Colon Cancer Assay The Challenge with the Stage II Colon Cancer Patient Implications for
- 13. The challenge: Which stage II colon cancer patients should receive adjuvant chemotherapy? It is unclear which
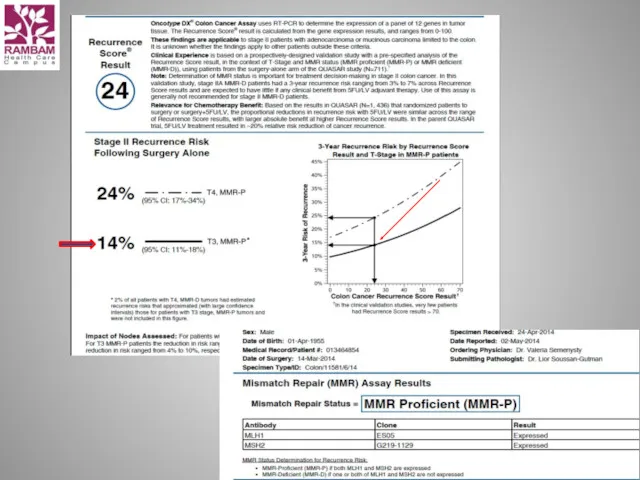
- 14. Integrating the Quantitative Recurrence Score® into Recurrence Risk Assessment and Treatment Planning for Stage II Colon
- 16. Metastatic disease Liver metastases Abdominal cavity metastases Abdominal lymph nodes metastases Pulmonary metastases Bone metastases Brain
- 17. Metastatic disease: Chemotherapy Active chemotherapy drugs 5- Fluorouracil/LCV Oxaliplatin Irinotecan ( CPT-11 ) Combination chemotherapy: 5FU/LCV
- 18. Irinotecan ( CPT-11, Campto ) Camptotheca Acuminata Topoizomerase 1 inhibitor
- 19. Irinotecan Major Adverse Effect: Diarrhea Early onset Caused by cholinergic effect of Irinotecan During or immediately
- 20. Oxaliplatin is classified as an "alkylating agent." Peripheral neuropathy Nausea and vomiting Diarrhea Mouth sores Low
- 22. Overall survival: Toxicity profile: XELODA better than 5-FLUOROURACIL = 5-FLUOROURACIL = XELODA
- 23. Xeloda (capecitabine) - side effects Abdominal or stomach pain diarrhea nausea numbness, pain, tingling, or other
- 25. Cont 5-FU 44h+LCV = De Gramont De Gramont/ Irinotecan(cpt-11) = FOLFIRI De Gramont / Oxaliplatin =
- 26. The Angiogenic Switch Is Necessary for Tumor Growth and Metastasis Somatic mutation Small avascular tumor Tumor
- 27. Avastin(Bevacizumab) inhibits vascularization —Avastin is an antibody that binds to VEGF and blocks its stimulation of
- 28. Bevacizumab precisely targets VEGF to inhibit angiogenesis1,2 Bevacizumab prevents binding of VEGF to receptors1,2 Bevacizumab has
- 29. Bevacizumab: one target, multiple effects1–20 1. Baluk, et al. Curr Opin Genet Dev 2005; 2. Willett,
- 30. June 2004: First Bevacizumab data from Phase III trial published in NEJM
- 31. Early separation of survival curves with bevacizumab – anti-VEGF AB
- 32. ML18147 study design (phase III) CT switch: Oxaliplatin → Irinotecan Irinotecan → Oxaliplatin Study conducted in
- 33. OS: ITT population Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p=0.0062 (log-rank test) Stratifiedb HR: 0.83 (95%
- 34. Primary endpoint – PFS Secondary endpoints – ORR, OS Loupakis, et al. NEJM 2014 TRIBE Study
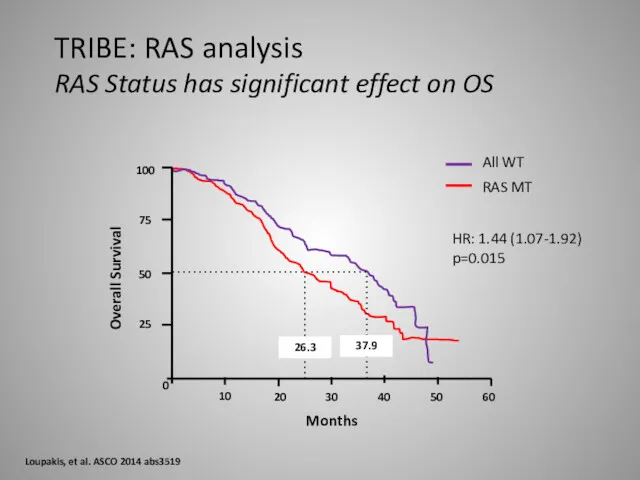
- 35. 100 75 50 25 0 10 20 30 40 50 60 37.9 26.3 All WT RAS
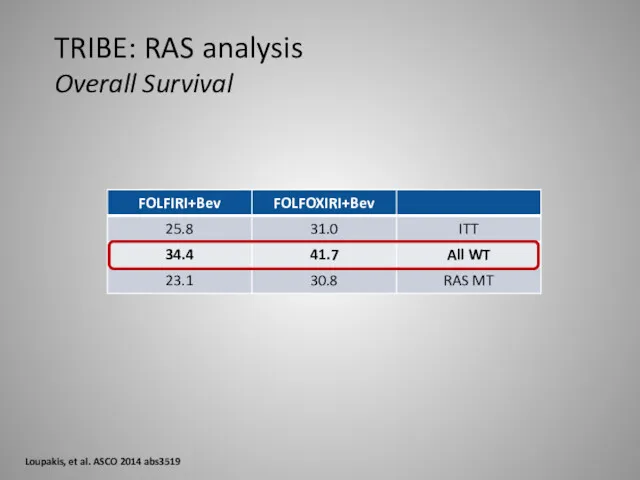
- 36. TRIBE: RAS analysis Overall Survival Loupakis, et al. ASCO 2014 abs3519
- 37. Conclusion anti-VEGF Therapy Duration of VEGF-inhibition matters Treatment to progression Maintenance strategies Treatment beyond progression Clinical
- 38. What are the side effects seen most often? High blood pressure Too much protein in the
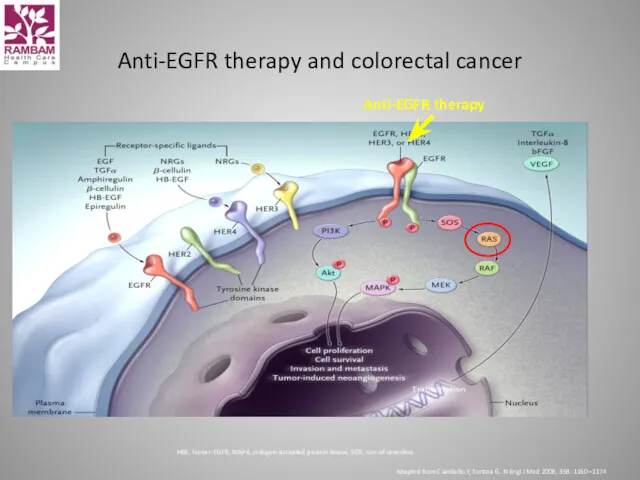
- 39. Anti-EGFR therapy and colorectal cancer HER, human EGFR; MAPK, mitogen-activated protein kinase; SOS, son-of-sevenless Adapted from
- 40. Primary endpoint Progression-free survival Secondary endpoints Overall survival Response Safety CRYSTAL: Erbitux + FOLFIRI vs FOLFIRI
- 41. Overall patient population Time (months) 54 42 48 Erbitux + FOLFIRI (n=599) FOLFIRI (n=599) 0.0 0.2
- 42. Key cancer biomarkers in patient care 1. Committee on Developing Biomarker-Based Tools for Cancer Screening Diagnosis
- 43. Biomarker-guided treatment has the potential to improve clinical outcomes Conley BA, Taube SE. Dis Markers 2004;
- 44. Examples of predictive biomarkers in oncology 1-9: European Public Assessment Reports, available at www.ema.europa.eu for: 1.
- 45. Personalized treatment is a better approach than “one treatment fits all” KRAS wt population Time (months)
- 46. Distribution of mutations in mCRC: A new definition
- 47. CALGB/SWOG 80405 data
- 48. CALGB/SWOG 80405: Randomized, open-label, multicenter (North America), Phase III IST1* 1. Venook AP, et al. J
- 49. CALGB/SWOG 80405: Efficacy comparison of KRAS exon 2 wt and RAS wt groups *733 KRAS codon
- 50. m a b : 4 0 m g m i . v . 1 2 0
- 51. FIRE-3 PFS 0.75 1.0 0.50 0.25 Probability of survival Events n/N (%) Median (months) 10.0 95%
- 52. FIRE-3 Overall survival Events n/N (%) Median (months) 28.7 95% CI ― FOLFIRI + Cetuximab 158/297
- 53. Greater selection of patients results in further improvement in OS Heinemann V, et al. ASCO 2013
- 54. Panitumumab Panitumumab – a fully human anti-EGFR mAb inhibits ligand binding and EGFR dimerisation Fully human,
- 55. PRIME study FOLFOX4 ± panitumumab in 1st-line treatment of metastatic CRC www.amgentrials.com; protocol ID: 20050203; ClinicalTrials.gov
- 56. PRIME study RAS analysis OS (primary analysis) Douillard JY, et al. N Engl J Med 2013;
- 57. What are the side effects seen most often? Cetuximab and Panitumumab
- 58. Regorafenib (Stivarga)
- 59. CLINICAL TRIALS
- 60. Optimized Treatment Strategy mCRC, palliative setting, PS 0-1 Unresectable Liver and Retroperitoneal LN Metastases Molecular testing
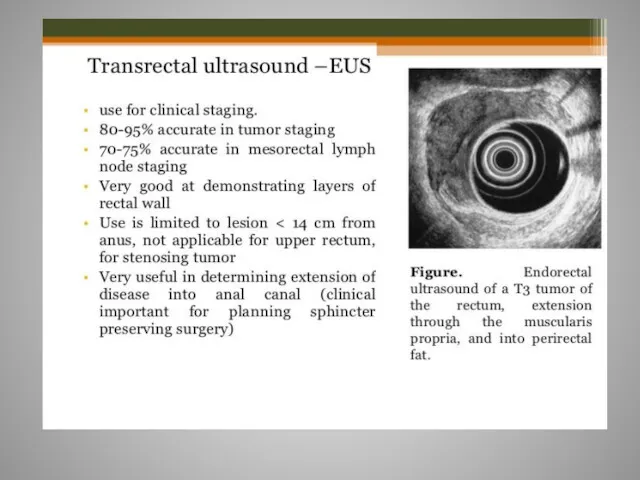
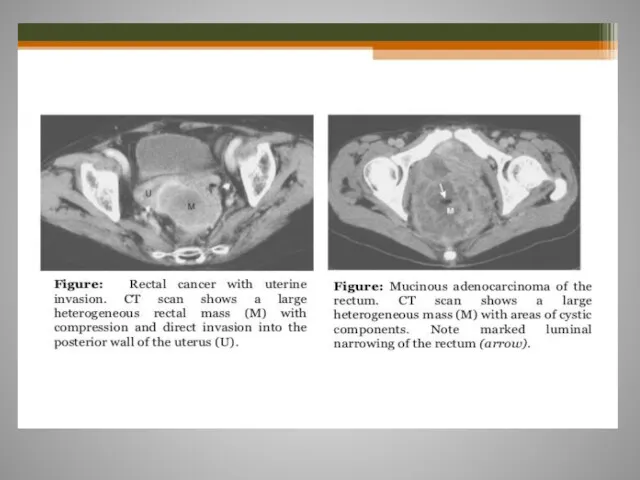
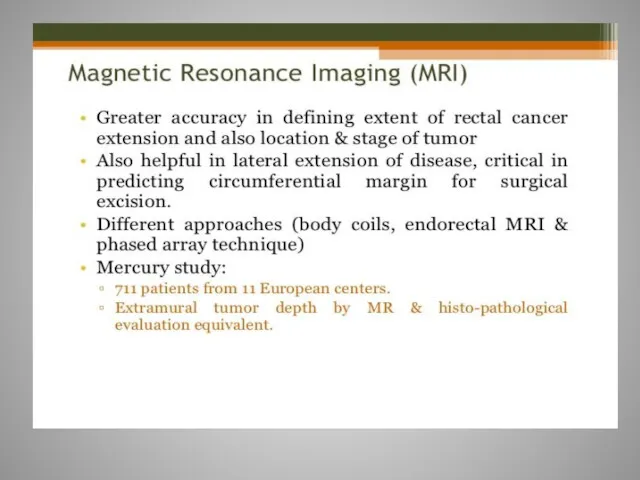
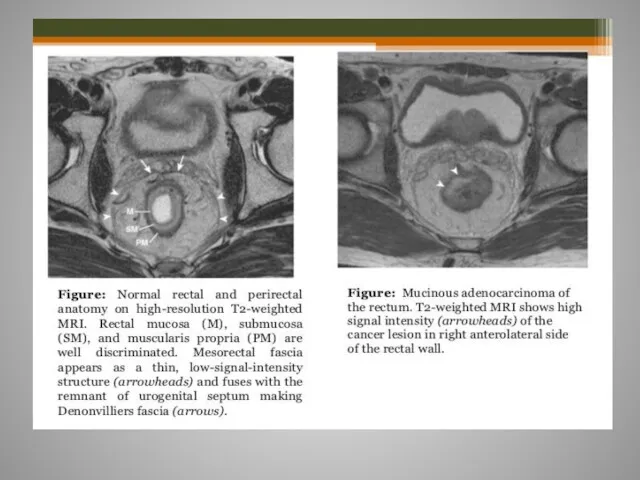
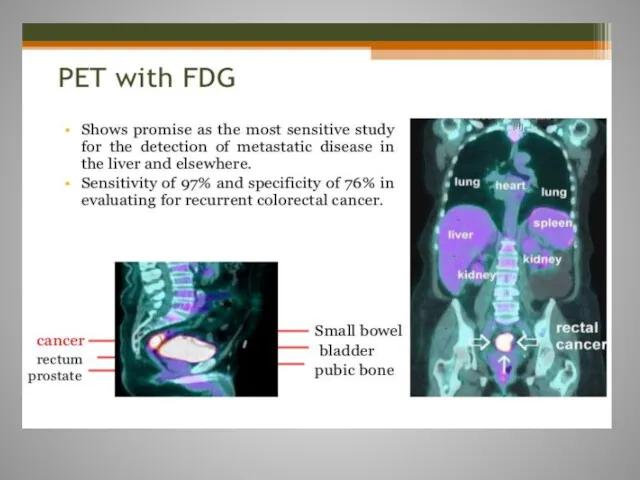
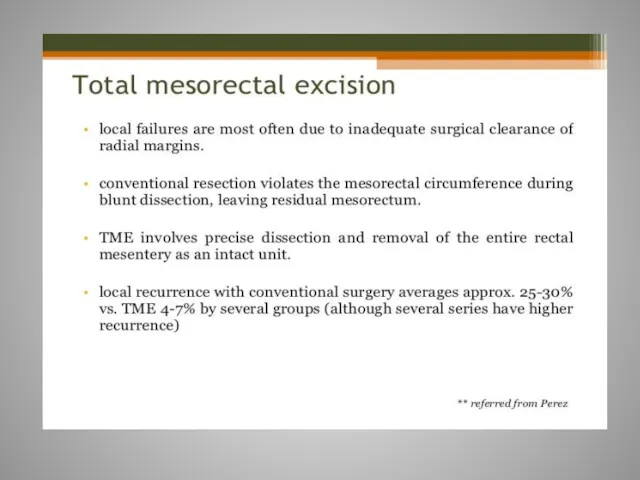
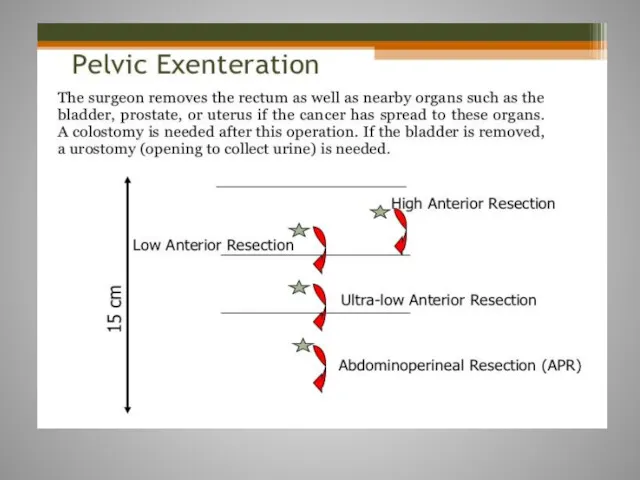
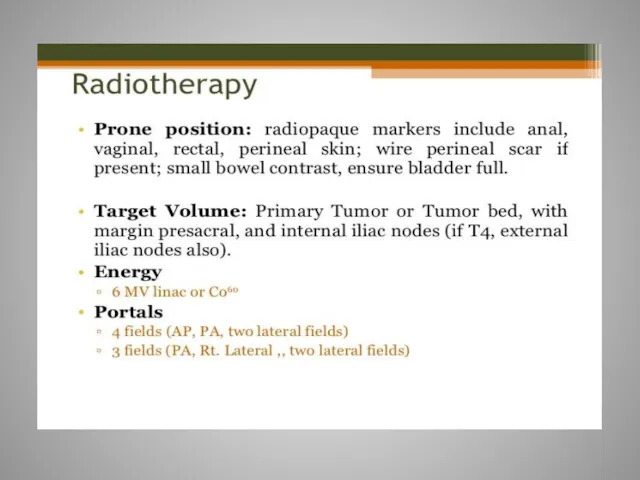
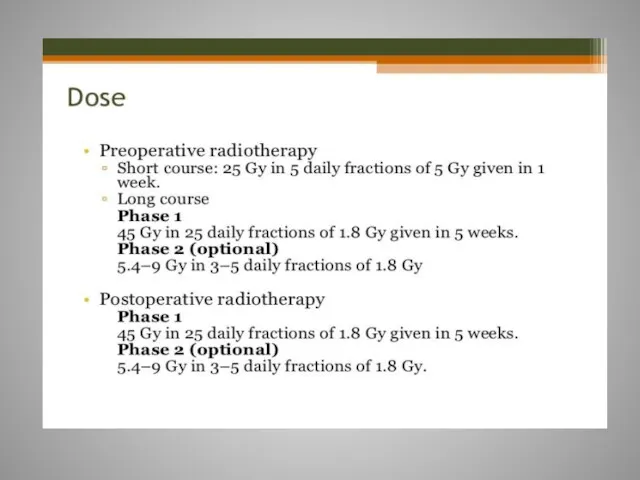
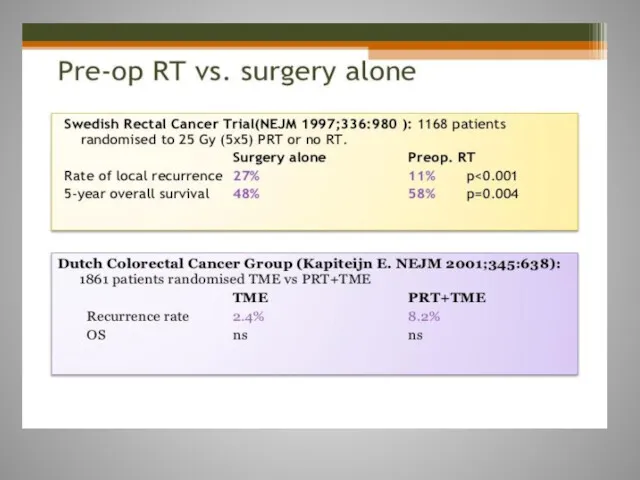
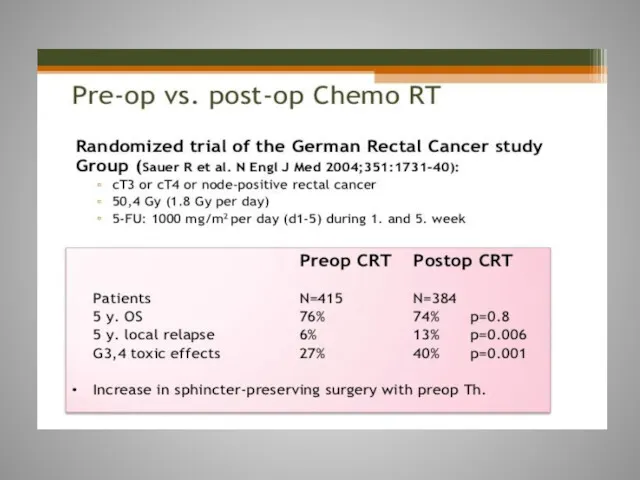
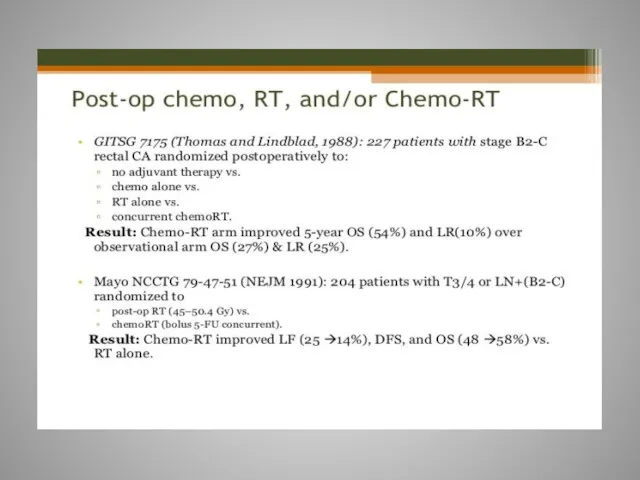
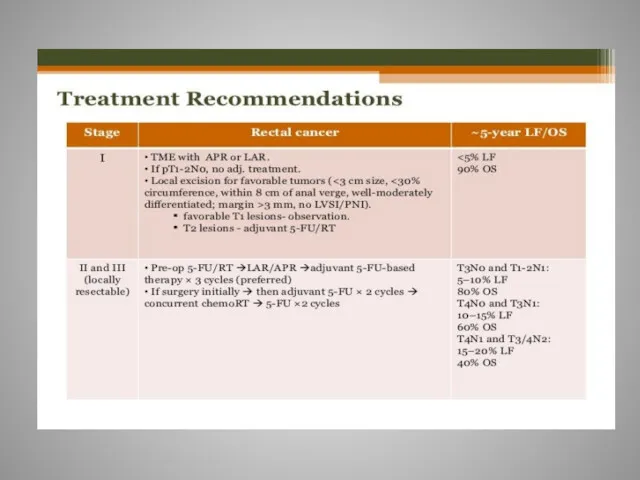
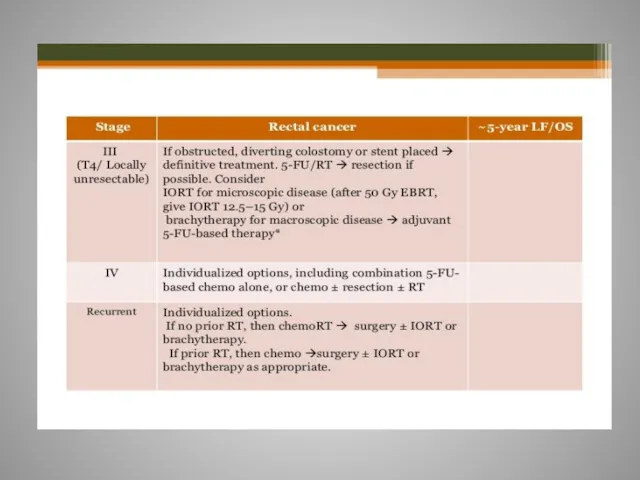
- 61. Rectal cancer
- 97. Скачать презентацию
Epidemiology
3-d most common cancer in men
3-d most common cancer in
Epidemiology
3-d most common cancer in men
3-d most common cancer in
Colorectal Cancer
Some facts
15% to 25% have metastases at diagnosis
Up to 50%
Colorectal Cancer
Some facts
15% to 25% have metastases at diagnosis
Up to 50%
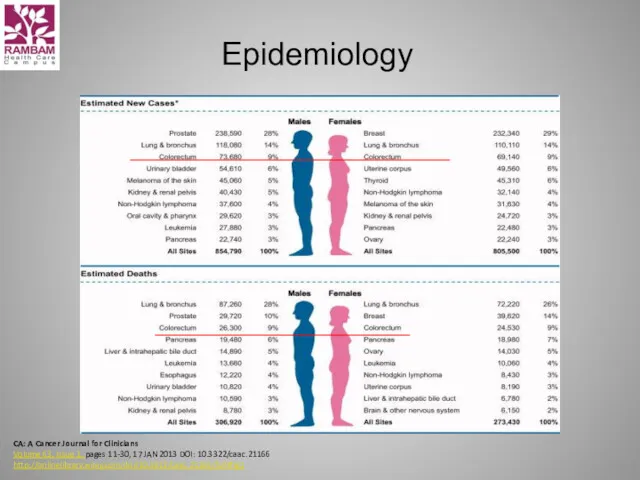
Epidemiology
CA: A Cancer Journal for Clinicians
Volume 63, Issue 1, pages
Epidemiology
CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages
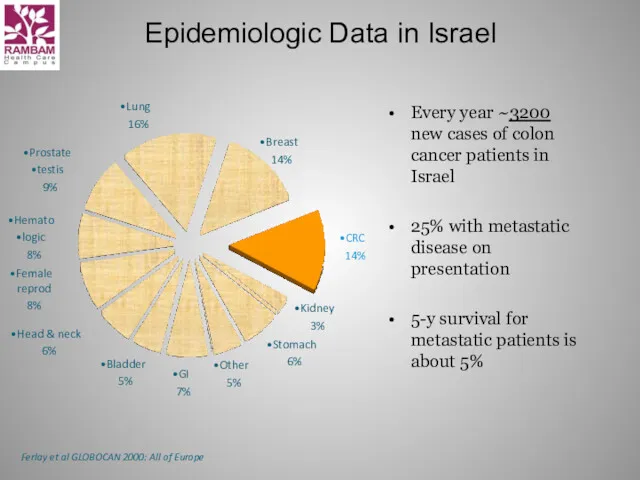
Epidemiologic Data in Israel
Every year ~3200 new cases of colon cancer
Epidemiologic Data in Israel
Every year ~3200 new cases of colon cancer
Prevalence estimates
in unscreened population
Individuals aged 50-y or older:
0.5 %
Prevalence estimates
in unscreened population
Individuals aged 50-y or older:
0.5 %
Risk factors for colorectal Cancer
Hereditary colon cancer syndromes
Inflammatory bowel disease
Personal history
Risk factors for colorectal Cancer
Hereditary colon cancer syndromes
Inflammatory bowel disease
Personal history
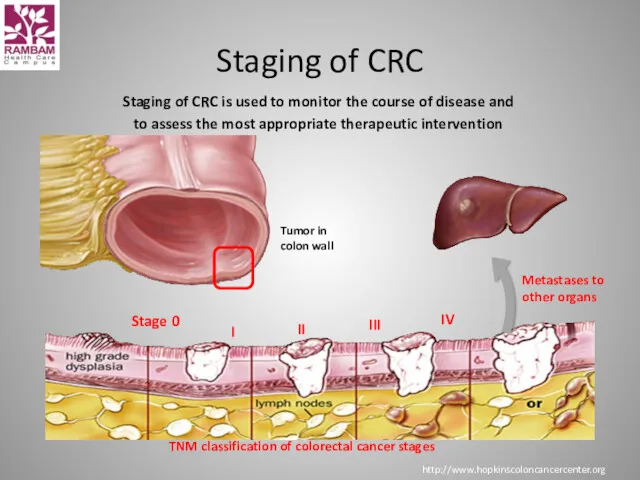
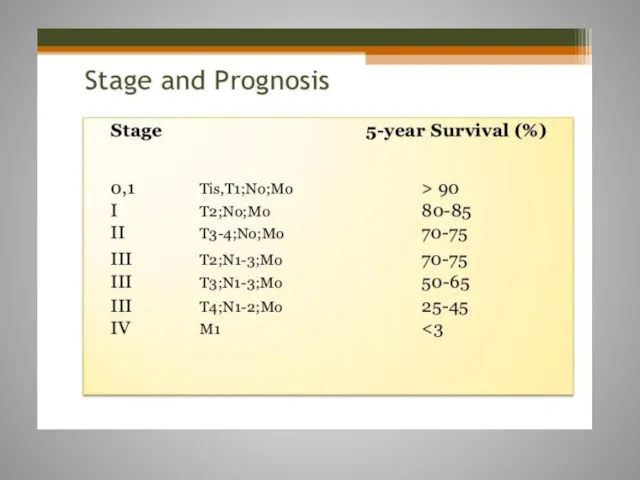
Staging of CRC is used to monitor the course of disease
Staging of CRC is used to monitor the course of disease
Treatment options for CRC
Surgery
Medical
Chemotherapy
Targeted therapies
Radiotherapy
Treatment options for CRC
Surgery
Medical
Chemotherapy
Targeted therapies
Radiotherapy
Surgery
For invasive Carcinoma of the colon stage I,II,III, surgery is
Surgery
For invasive Carcinoma of the colon stage I,II,III, surgery is
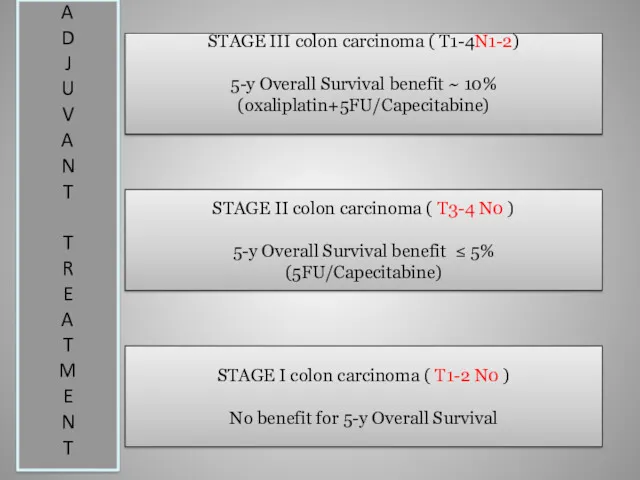
STAGE III colon carcinoma ( T1-4N1-2)
5-y Overall Survival benefit ~ 10%
(oxaliplatin+5FU/Capecitabine)
STAGE
STAGE III colon carcinoma ( T1-4N1-2)
5-y Overall Survival benefit ~ 10%
(oxaliplatin+5FU/Capecitabine)
STAGE
Oncotype DX® Colon Cancer Assay
The Challenge with the Stage II Colon
Oncotype DX® Colon Cancer Assay
The Challenge with the Stage II Colon
The challenge: Which stage II colon cancer patients should receive adjuvant
The challenge: Which stage II colon cancer patients should receive adjuvant
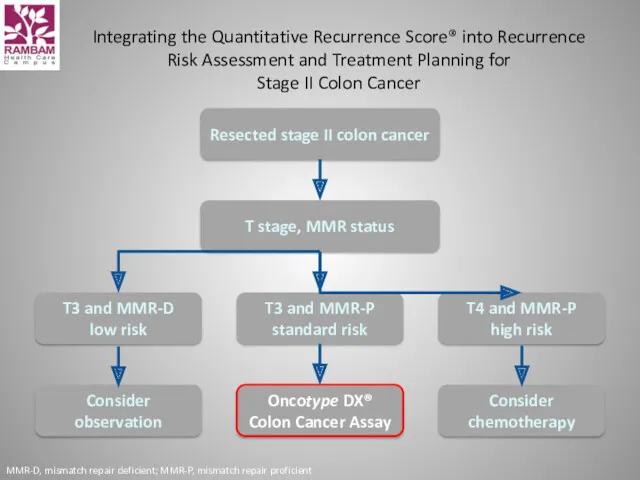
Integrating the Quantitative Recurrence Score® into Recurrence Risk Assessment and Treatment
Integrating the Quantitative Recurrence Score® into Recurrence Risk Assessment and Treatment
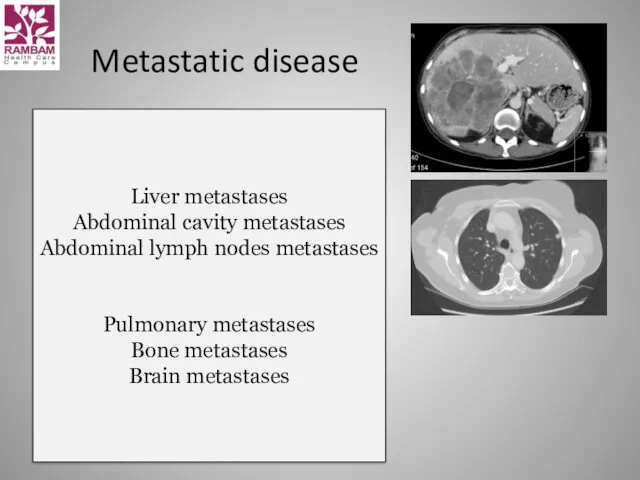
Metastatic disease
Liver metastases
Abdominal cavity metastases
Abdominal lymph nodes metastases
Pulmonary metastases
Bone metastases
Brain metastases
Metastatic disease
Liver metastases
Abdominal cavity metastases
Abdominal lymph nodes metastases
Pulmonary metastases
Bone metastases
Brain metastases
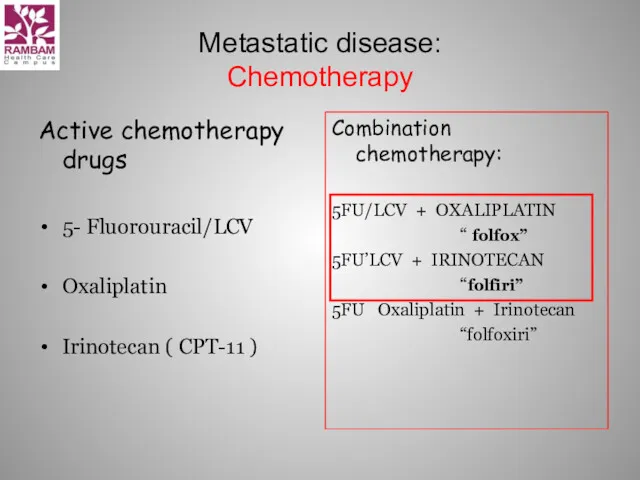
Metastatic disease:
Chemotherapy
Active chemotherapy drugs
5- Fluorouracil/LCV
Oxaliplatin
Irinotecan ( CPT-11 )
Combination chemotherapy:
5FU/LCV +
Metastatic disease:
Chemotherapy
Active chemotherapy drugs
5- Fluorouracil/LCV
Oxaliplatin
Irinotecan ( CPT-11 )
Combination chemotherapy:
5FU/LCV +
Irinotecan ( CPT-11, Campto )
Camptotheca Acuminata
Topoizomerase 1 inhibitor
Irinotecan ( CPT-11, Campto )
Camptotheca Acuminata
Topoizomerase 1 inhibitor
Irinotecan Major Adverse Effect:
Diarrhea
Early onset
Caused by cholinergic effect of
Irinotecan Major Adverse Effect:
Diarrhea
Early onset
Caused by cholinergic effect of
Oxaliplatin
is classified as an "alkylating agent."
Peripheral neuropathy
Nausea and vomiting
Diarrhea
Oxaliplatin
is classified as an "alkylating agent."
Peripheral neuropathy
Nausea and vomiting
Diarrhea

Overall survival:
Toxicity profile:
XELODA better than 5-FLUOROURACIL
=
5-FLUOROURACIL = XELODA
Overall survival:
Toxicity profile:
XELODA better than 5-FLUOROURACIL
=
5-FLUOROURACIL = XELODA
Xeloda (capecitabine) -
side effects
Abdominal or stomach pain
diarrhea
nausea
numbness, pain, tingling, or
Xeloda (capecitabine) -
side effects
Abdominal or stomach pain
diarrhea
nausea
numbness, pain, tingling, or
Cont 5-FU 44h+LCV = De Gramont
De Gramont/ Irinotecan(cpt-11) = FOLFIRI
De Gramont
Cont 5-FU 44h+LCV = De Gramont
De Gramont/ Irinotecan(cpt-11) = FOLFIRI
De Gramont
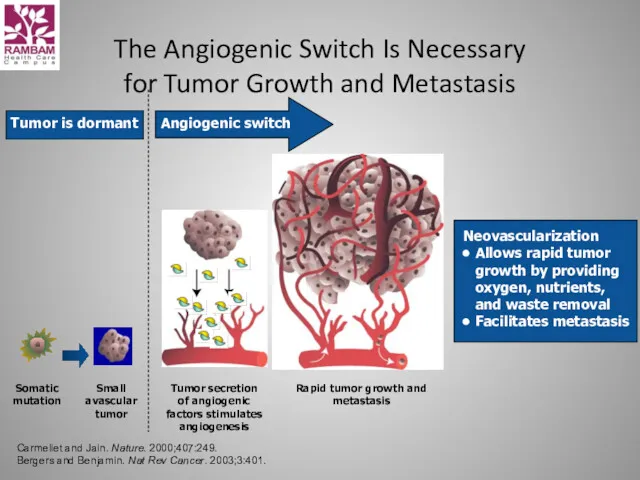
The Angiogenic Switch Is Necessary
for Tumor Growth and Metastasis
Somatic
mutation
Small
avascular
tumor
Tumor
The Angiogenic Switch Is Necessary
for Tumor Growth and Metastasis
Somatic
mutation
Small
avascular
tumor
Tumor
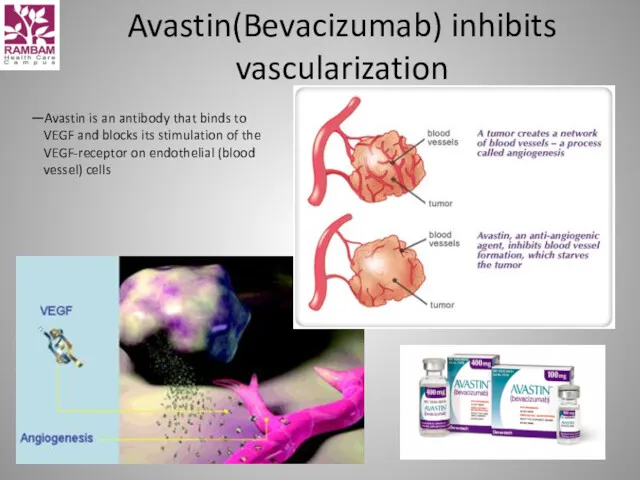
Avastin(Bevacizumab) inhibits vascularization
—Avastin is an antibody that binds to VEGF and
Avastin(Bevacizumab) inhibits vascularization
—Avastin is an antibody that binds to VEGF and
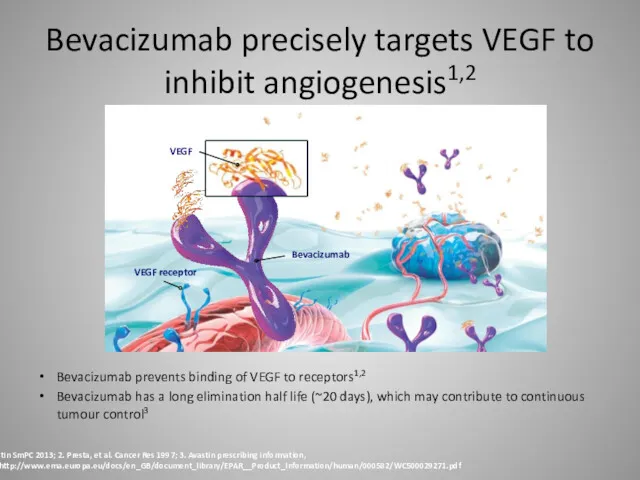
Bevacizumab precisely targets VEGF to inhibit angiogenesis1,2
Bevacizumab prevents binding of VEGF
Bevacizumab precisely targets VEGF to inhibit angiogenesis1,2
Bevacizumab prevents binding of VEGF
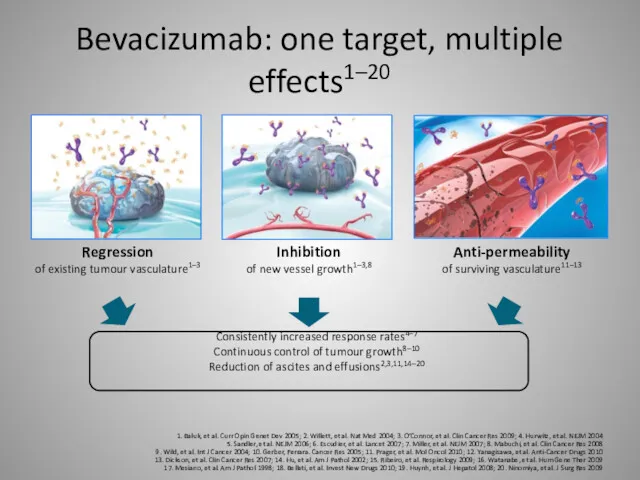
Bevacizumab: one target, multiple effects1–20
1. Baluk, et al. Curr Opin Genet
Bevacizumab: one target, multiple effects1–20
1. Baluk, et al. Curr Opin Genet
June 2004: First Bevacizumab data from Phase III trial published in
June 2004: First Bevacizumab data from Phase III trial published in
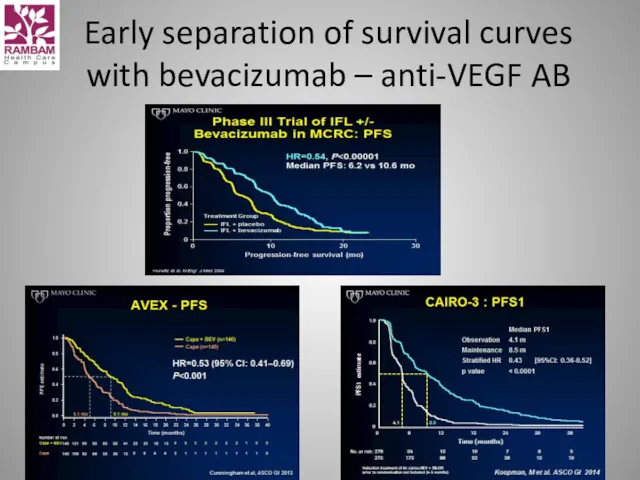
Early separation of survival curves with bevacizumab – anti-VEGF AB
Early separation of survival curves with bevacizumab – anti-VEGF AB
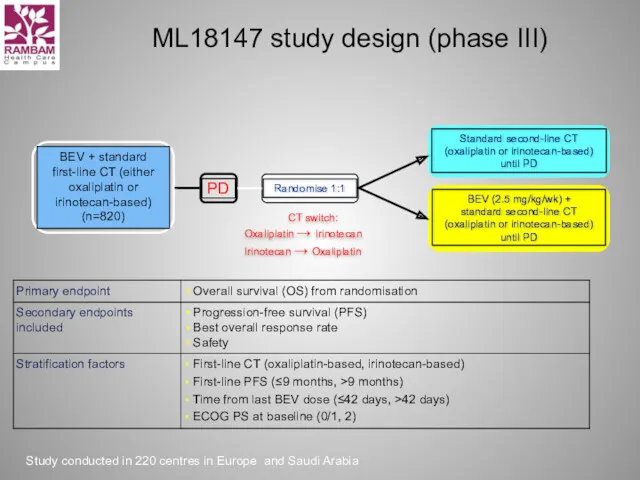
ML18147 study design (phase III)
CT switch:
Oxaliplatin → Irinotecan
Irinotecan → Oxaliplatin
Study conducted
ML18147 study design (phase III)
CT switch:
Oxaliplatin → Irinotecan
Irinotecan → Oxaliplatin
Study conducted
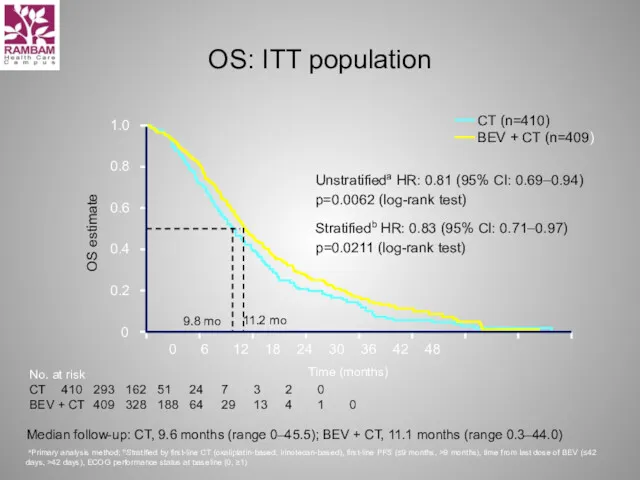
OS: ITT population
Unstratifieda HR: 0.81 (95% CI: 0.69–0.94)
p=0.0062 (log-rank test)
Stratifiedb HR:
OS: ITT population
Unstratifieda HR: 0.81 (95% CI: 0.69–0.94)
p=0.0062 (log-rank test)
Stratifiedb HR:
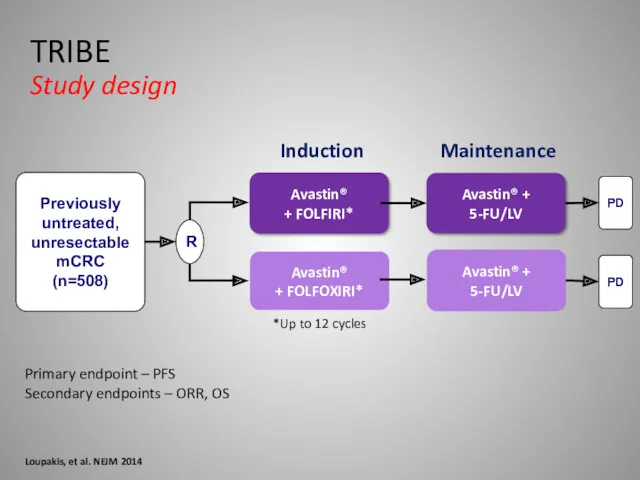
Primary endpoint – PFS
Secondary endpoints – ORR, OS
Loupakis, et al. NEJM
Primary endpoint – PFS
Secondary endpoints – ORR, OS
Loupakis, et al. NEJM
100
75
50
25
0
10
20
30
40
50
60
37.9
26.3
All WT
RAS MT
Overall Survival
Months
HR: 1.44 (1.07-1.92)
p=0.015
TRIBE: RAS analysis
RAS Status has
100
75
50
25
0
10
20
30
40
50
60
37.9
26.3
All WT
RAS MT
Overall Survival
Months
HR: 1.44 (1.07-1.92)
p=0.015
TRIBE: RAS analysis RAS Status has
TRIBE: RAS analysis
Overall Survival
Loupakis, et al. ASCO 2014 abs3519
TRIBE: RAS analysis
Overall Survival
Loupakis, et al. ASCO 2014 abs3519
Conclusion anti-VEGF Therapy
Duration of VEGF-inhibition matters
Treatment to progression
Maintenance strategies
Treatment beyond progression
Clinical
Conclusion anti-VEGF Therapy
Duration of VEGF-inhibition matters
Treatment to progression
Maintenance strategies
Treatment beyond progression
Clinical
What are the side effects seen most often?
High blood pressure
Too much
What are the side effects seen most often?
High blood pressure
Too much
Anti-EGFR therapy and colorectal cancer
HER, human EGFR; MAPK, mitogen-activated protein kinase;
Anti-EGFR therapy and colorectal cancer
HER, human EGFR; MAPK, mitogen-activated protein kinase;
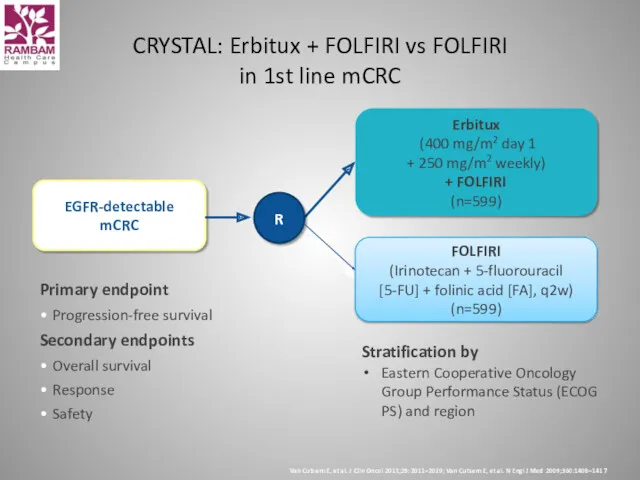
Primary endpoint
Progression-free survival
Secondary endpoints
Overall survival
Response
Safety
CRYSTAL: Erbitux + FOLFIRI vs FOLFIRI
in
Primary endpoint
Progression-free survival
Secondary endpoints
Overall survival
Response
Safety
CRYSTAL: Erbitux + FOLFIRI vs FOLFIRI in
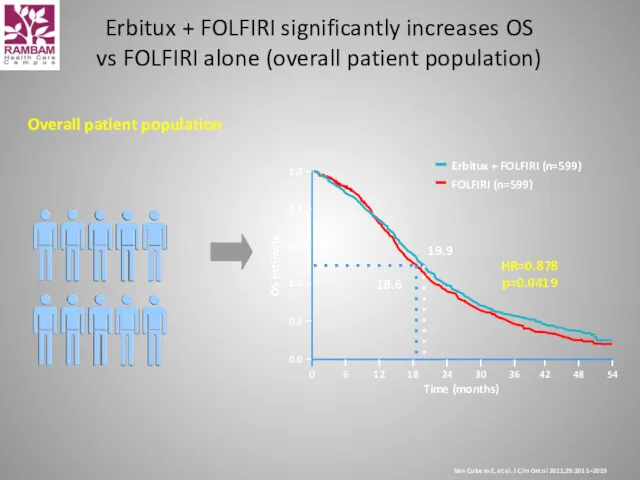
Overall patient population
Time (months)
54
42
48
Erbitux + FOLFIRI (n=599)
FOLFIRI (n=599)
0.0
0.2
0.4
0.6
0.8
1.0
18
0
6
12
24
30
36
OS estimate
HR=0.878
p=0.0419
19.9
18.6
Erbitux + FOLFIRI
Overall patient population
Time (months)
54
42
48
Erbitux + FOLFIRI (n=599)
FOLFIRI (n=599)
0.0
0.2
0.4
0.6
0.8
1.0
18
0
6
12
24
30
36
OS estimate
HR=0.878
p=0.0419
19.9
18.6
Erbitux + FOLFIRI
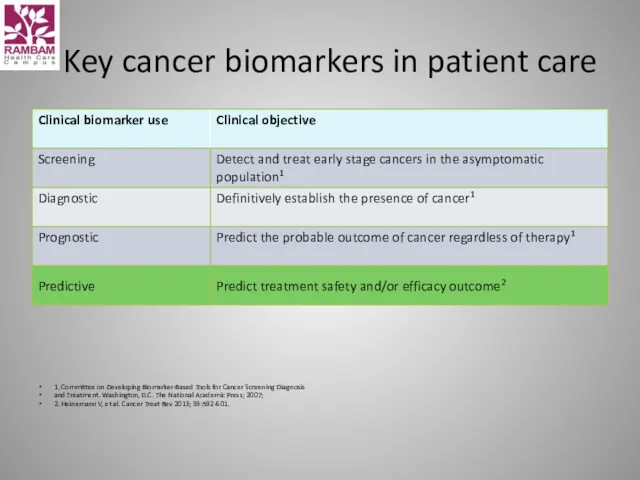
Key cancer biomarkers in patient care
1. Committee on Developing Biomarker-Based Tools
Key cancer biomarkers in patient care
1. Committee on Developing Biomarker-Based Tools
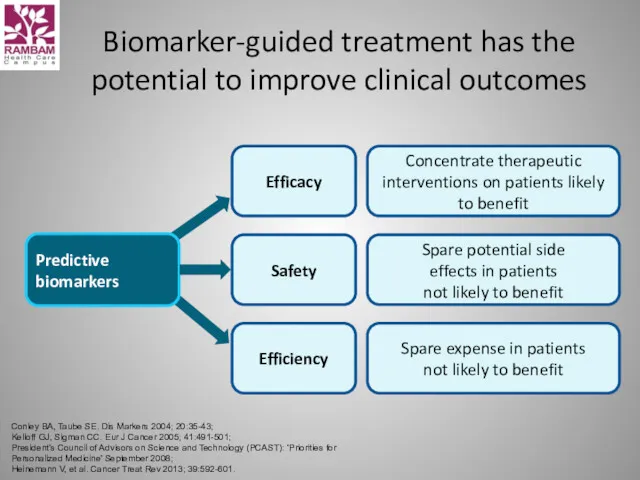
Biomarker-guided treatment has the potential to improve clinical outcomes
Conley BA, Taube
Biomarker-guided treatment has the potential to improve clinical outcomes
Conley BA, Taube
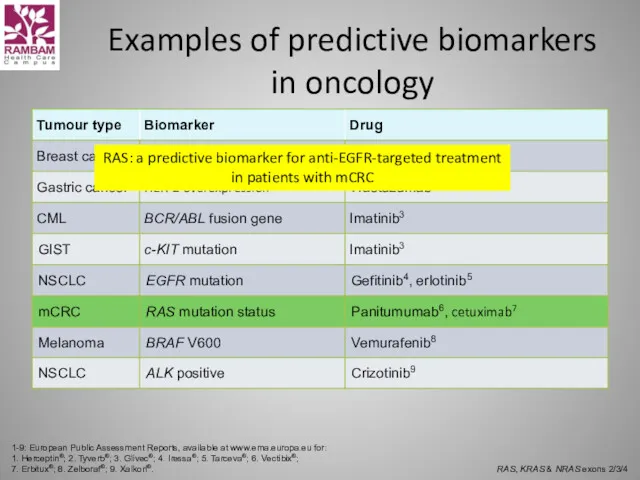
Examples of predictive biomarkers in oncology
1-9: European Public Assessment Reports, available
Examples of predictive biomarkers in oncology
1-9: European Public Assessment Reports, available
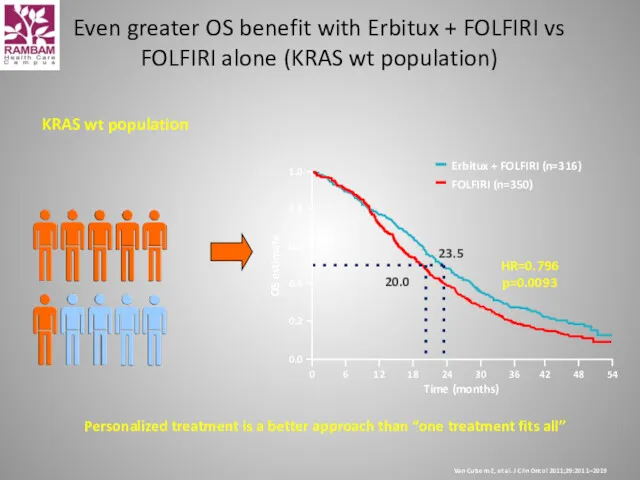
Personalized treatment is a better approach than “one treatment fits all”
KRAS
Personalized treatment is a better approach than “one treatment fits all”
KRAS
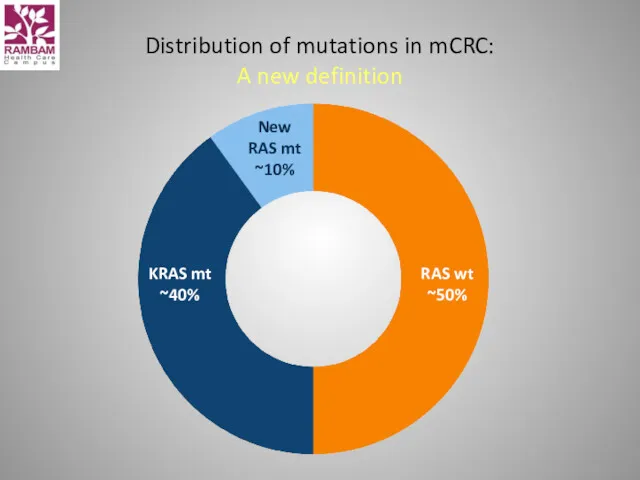
Distribution of mutations in mCRC:
A new definition
Distribution of mutations in mCRC:
A new definition
CALGB/SWOG 80405 data
CALGB/SWOG 80405 data
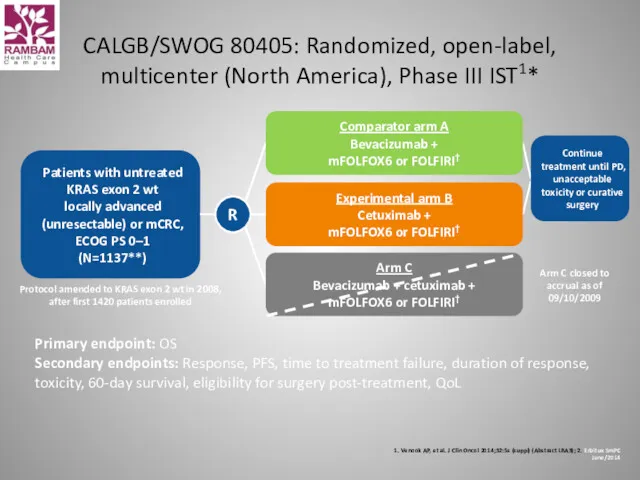
CALGB/SWOG 80405: Randomized, open-label, multicenter (North America), Phase III IST1*
1. Venook
CALGB/SWOG 80405: Randomized, open-label, multicenter (North America), Phase III IST1*
1. Venook
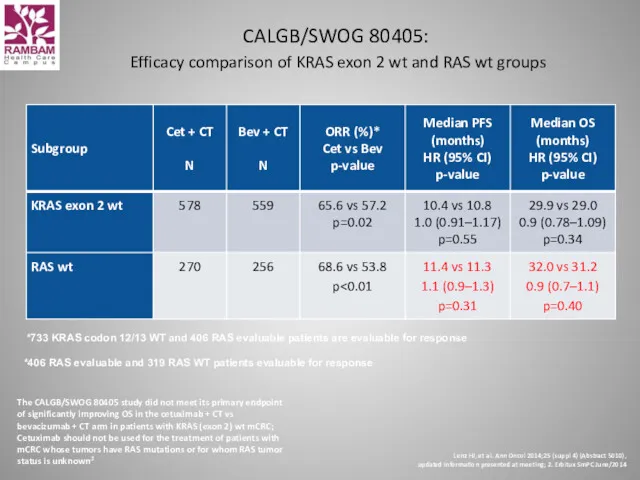
CALGB/SWOG 80405:
Efficacy comparison of KRAS exon 2 wt and RAS
CALGB/SWOG 80405: Efficacy comparison of KRAS exon 2 wt and RAS
m
a
b
:
4
0
m
g
m
i
.
v
.
1
2
0
m
i
n
i
n
i
t
i
a
l
d
o
s
e
2
5
0
m
g
/
m
2
i
.
v
.
6
0
m
in
q
1
w
B
e
v
a
c
i
z
u
m
a
b
:
5
m
g
/
k
g
i
.
v
.
3
0
-
9
0
m
i
n
q
2
w
/
0
i
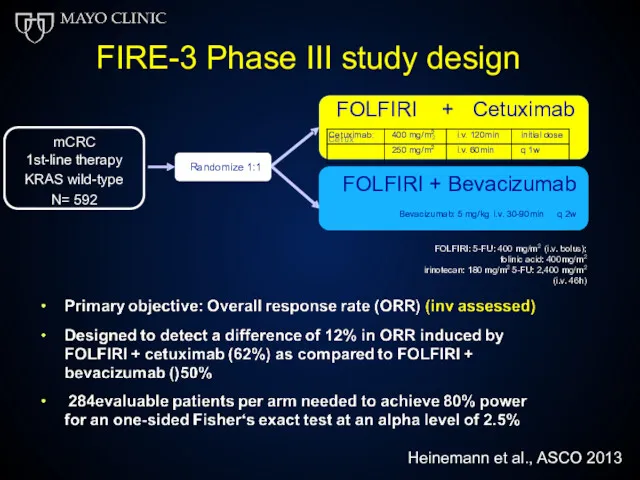
FIRE-3 Phase III study design
C
e
t
u
x
2
FOLFIRI
+ Cetuximab
FOLFIRI + Bevacizumab
Bevacizumab: 5 mg/kg i.v. 30-90min q 2w
mCRC
1st-line
m
a
b
:
4
0
m
g
m
i
.
v
.
1
2
0
m
i
n
i
n
i
t
i
a
l
d
o
s
e
2
5
0
m
g
/
m
2
i
.
v
.
6
0
m
in
q
1
w
B
e
v
a
c
i
z
u
m
a
b
:
5
m
g
/
k
g
i
.
v
.
3
0
-
9
0
m
i
n
q
2
w
/
0
i
FIRE-3 Phase III study design
C
e
t
u
x
2
FOLFIRI
+ Cetuximab
FOLFIRI + Bevacizumab
Bevacizumab: 5 mg/kg i.v. 30-90min q 2w
mCRC
1st-line
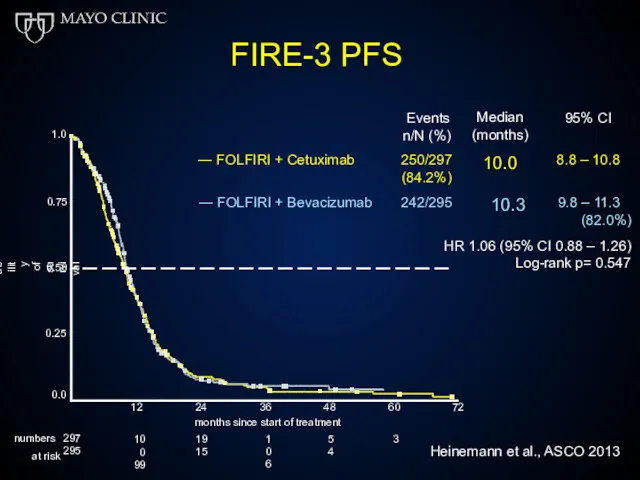
FIRE-3 PFS
0.75
1.0
0.50
0.25
Probability of survival
Events
n/N (%)
Median (months)
10.0
95% CI
― FOLFIRI + Cetuximab
250/297
(84.2%)
8.8 –
FIRE-3 PFS
0.75
1.0
0.50
0.25
Probability of survival
Events
n/N (%)
Median (months)
10.0
95% CI
― FOLFIRI + Cetuximab
250/297
(84.2%)
8.8 –
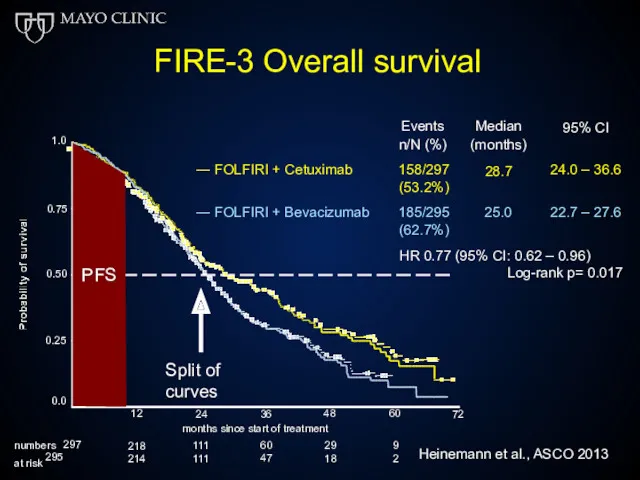
FIRE-3 Overall survival
Events n/N (%)
Median (months)
28.7
95% CI
― FOLFIRI + Cetuximab
158/297
(53.2%)
24.0 –
FIRE-3 Overall survival
Events n/N (%)
Median (months)
28.7
95% CI
― FOLFIRI + Cetuximab
158/297
(53.2%)
24.0 –
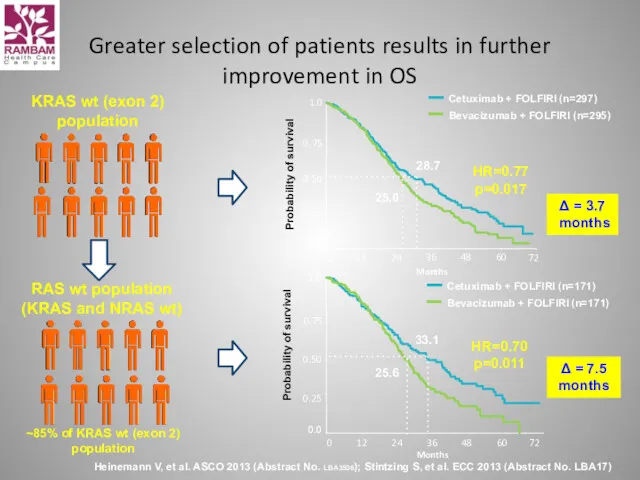
Greater selection of patients results in further improvement in OS
Heinemann V,
Greater selection of patients results in further improvement in OS
Heinemann V,
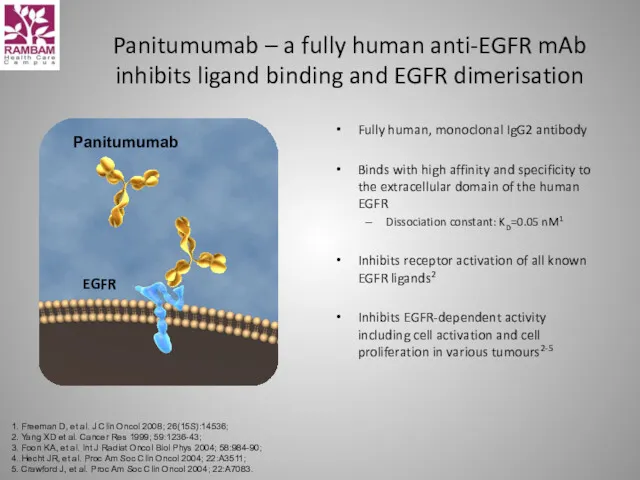
Panitumumab
Panitumumab – a fully human anti-EGFR mAb
inhibits ligand binding and
Panitumumab
Panitumumab – a fully human anti-EGFR mAb inhibits ligand binding and
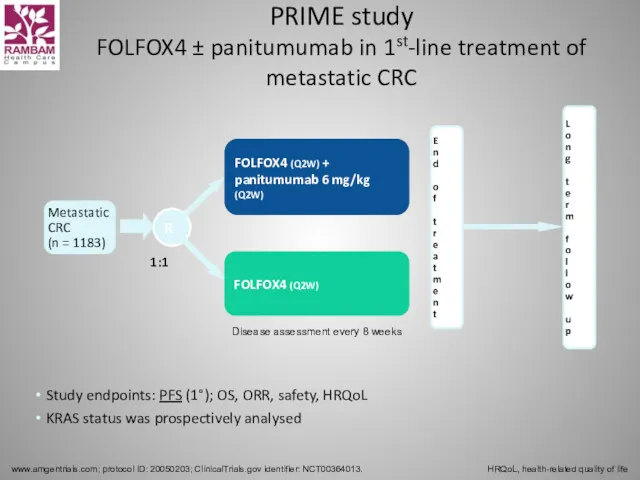
PRIME study
FOLFOX4 ± panitumumab in 1st-line treatment of metastatic CRC
www.amgentrials.com;
PRIME study
FOLFOX4 ± panitumumab in 1st-line treatment of metastatic CRC
www.amgentrials.com;
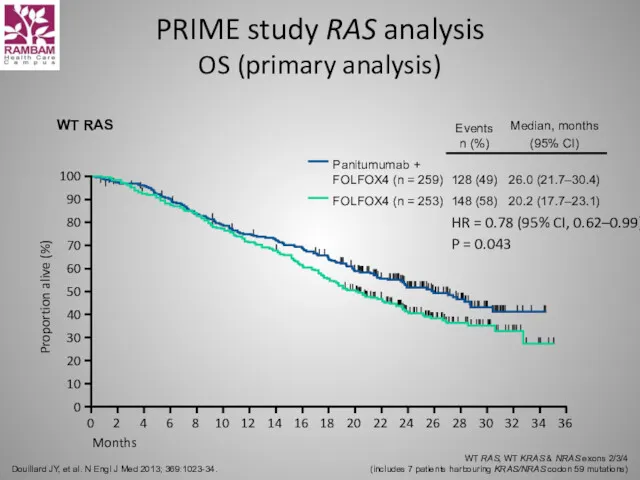
PRIME study RAS analysis
OS (primary analysis)
Douillard JY, et al. N Engl
PRIME study RAS analysis
OS (primary analysis)
Douillard JY, et al. N Engl
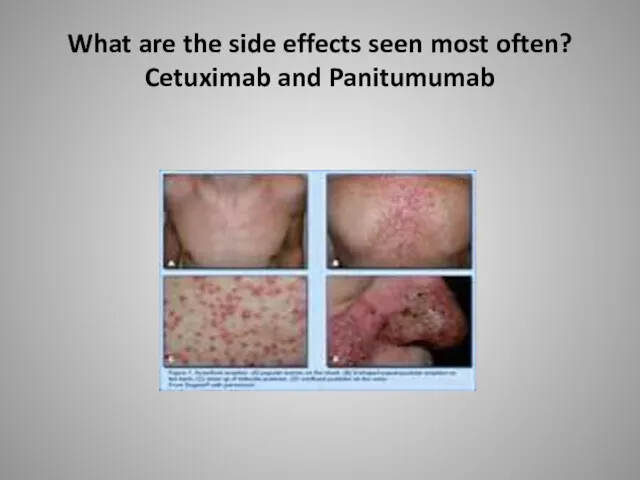
What are the side effects seen most often?
Cetuximab and Panitumumab
What are the side effects seen most often?
Cetuximab and Panitumumab
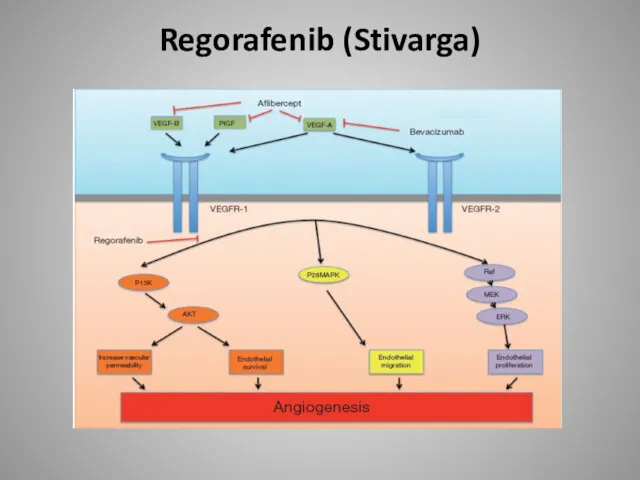
Regorafenib (Stivarga)
Regorafenib (Stivarga)
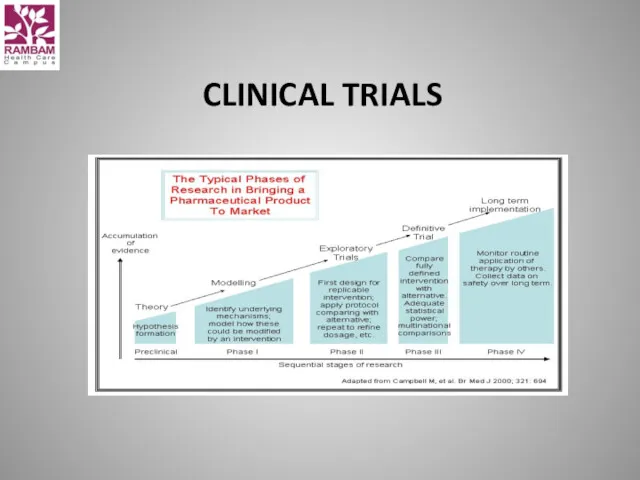
CLINICAL TRIALS
CLINICAL TRIALS
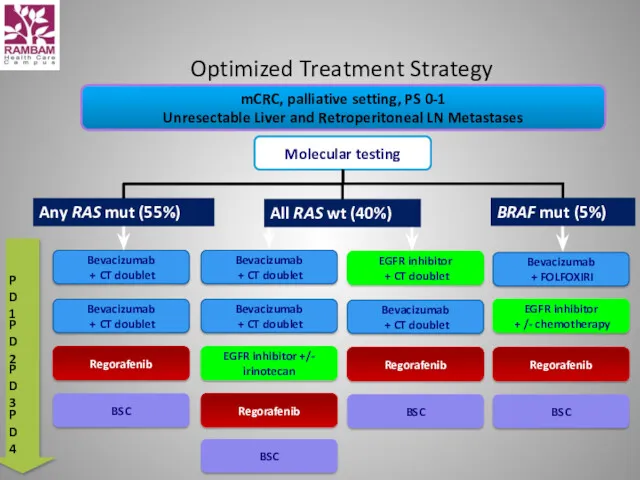
Optimized Treatment Strategy
mCRC, palliative setting, PS 0-1
Unresectable Liver and Retroperitoneal LN
Optimized Treatment Strategy
mCRC, palliative setting, PS 0-1
Unresectable Liver and Retroperitoneal LN
Rectal cancer
Rectal cancer

 Применение в стоматологии светолечения, вибротерапии, ультразвуковой терапии, ионотерапии, аэрозольтерапии
Применение в стоматологии светолечения, вибротерапии, ультразвуковой терапии, ионотерапии, аэрозольтерапии Психотропные средства
Психотропные средства Лечебное применение механических факторов (часть 1. Использование звука в лечебных целях)
Лечебное применение механических факторов (часть 1. Использование звука в лечебных целях) Здоровье человека. Факторы, определяющие здоровье человека. Основные причины болезней. Оценка состояния здоровья человека
Здоровье человека. Факторы, определяющие здоровье человека. Основные причины болезней. Оценка состояния здоровья человека Менструальный цикл. Овогенез. Анатомия мужских половых органов. Сперматогенез
Менструальный цикл. Овогенез. Анатомия мужских половых органов. Сперматогенез Профилактика профессионального заражения ВИЧ
Профилактика профессионального заражения ВИЧ Анатомия спинномозговых нервов
Анатомия спинномозговых нервов Символы медицины
Символы медицины Өкпе туберкулезі
Өкпе туберкулезі Омыртқа жотасының физиологиялық және паталогиялық иілімдері
Омыртқа жотасының физиологиялық және паталогиялық иілімдері Философия мен медицинадағы Болмыс және Сана ұғымдары
Философия мен медицинадағы Болмыс және Сана ұғымдары Нормальная ЭКГ
Нормальная ЭКГ Трансплантология. Тері бұлшықет, жүйке,сүйек тінді қуысты ағзалардың пластикасы. Тіндерді қондырудың биологиялық жағдайлары
Трансплантология. Тері бұлшықет, жүйке,сүйек тінді қуысты ағзалардың пластикасы. Тіндерді қондырудың биологиялық жағдайлары Фармацевтическая опека при головной боли
Фармацевтическая опека при головной боли Порядок оказания медицинской помощи при острых и хронических профессиональных заболеваниях
Порядок оказания медицинской помощи при острых и хронических профессиональных заболеваниях Физическое развитие детей
Физическое развитие детей Лекарственная болезнь
Лекарственная болезнь Сестринский уход при заболеваниях сердечно-сосудистой системы и системы крови у гериатрических пациентов
Сестринский уход при заболеваниях сердечно-сосудистой системы и системы крови у гериатрических пациентов Медицинская демография. Динамика населения. Младенческая смертность. (Лекция 10)
Медицинская демография. Динамика населения. Младенческая смертность. (Лекция 10) Естің бұзылысы
Естің бұзылысы Трезвый образ жизни – забытая норма
Трезвый образ жизни – забытая норма Инфекционные заболевания
Инфекционные заболевания Ес және сана-сезімнің бұзылыстары
Ес және сана-сезімнің бұзылыстары Заттар алмасуының гормональді реттелуі. Гормональді реттелудің бұзылыстары
Заттар алмасуының гормональді реттелуі. Гормональді реттелудің бұзылыстары Эмфизема легких
Эмфизема легких Острый живот в гинекологии
Острый живот в гинекологии Современные представления о миоме матки
Современные представления о миоме матки Хронические заболевания легких у детей
Хронические заболевания легких у детей