- Disorders of metabolism. (Subject 9)

Содержание
- 2. ABB regulation Acidosis pH Alkalosis pH > 7.45
- 3. Blood buffer systems Bicarbonate buffer system the most mobile (can be regulated by lungs and kidneys)
- 4. Physiological mechanisms of ABB regulation Respiratory system regulation of the PCO2 and, hence, H2CO3 of the
- 5. Respiratory acidosis Reason: hypoventilation of lungs (obturation of respiratory tract, pulmonary edema, ? of respiratory center
- 6. The effects of high pCO2 spasm of peripheral arterioles, ? of BP ? urine formation. brain
- 7. Metabolic acidosis Reasons: failure of the kidneys to excrete the metabolic acids (uremia) loss of bases
- 8. Metabolic acidosis Formation of excess of metabolic acids in the body: Ketoacidosis: accumulation of keton bodies
- 9. Acidosis clinical manifestation depression of the central nervous system (from disorientation to coma). ? blood vessels
- 10. Respiratory alkalosis Reason - hyperventilation: excitation of respiratory center (brain inflammation or edema) reflex stimulation of
- 11. Metabolic alkalosis Reasons: Diuretic drugs – reabsorption of Na; loss of H+ and K+ Excessive use
- 12. Clinical manifestation of alkalosis ? pCO2 – spasm of brain vessels and dilation of peripheral vessels
- 13. Water (Fluid) Balance Disorders Hypohydration symptoms (2-15% of body weight) ? of blood circulating volume weight
- 14. Water (Fluid) Balance Disorders Hypohydration symptoms Nervous system disorders: headache, dizziness, disorders of consciousness, inability to
- 15. Hypohydration causes concentration of electrolytes in blood plasma (osmotic pressure) low normal high
- 16. Hyperhydration causes concentration of electrolytes in blood plasma (osmotic pressure) low normal high
- 17. Hyperhydration symptoms ? blood circulating volume and ABP heart overload general edema (cardiac failure and hypoproteinemia)
- 18. Edema Accumulation of excess fluid: in intercellular space body cavities (hydrothorax, hydropericardium and hydroperitoneum (ascites)) generalized
- 19. Edema mechanisms ? capillary hydrostatic pressure (high venous BP – local, systemic) Alterations in oncotic pressure
- 20. Starvation Forms of starvation: Total (absolute) – deprivation of food and water Complete – deprivation only
- 21. Starvation Exogenous: voluntary starvation involuntary (social and economical problems) eating disorders (Anorexia nervosa) Endogenous: malabsorption syndrome
- 22. Stage 1. Early starvation blood glucose ??glucagon ? glycogenolysis Glycogen stores are depleted in 12 to
- 23. Stage 2 Prolonged starvation protein catabolism high lipolysis + muscle oxidation of ketone bodies
- 24. Stage 3 Terminal phase Lipid stores of body are completely depleted (97-100%), loss of 40-50% body
- 25. Obesity Excessive accumulation and storage of fat in the body. Body mass index (BMI) - weight/height
- 26. Obesity classification General and local obesity. Local obesity - central or peripheral. Central obesity (upper body
- 27. Obesity classification Hyperplastic obesity - ⭡ number of fat cells. massive obesity & early age of
- 28. Obesity classification Primary obesity - leptin deficiency or decreased function. 20% obese patients - absolute leptin
- 29. Obesity pathogenesis Neural mechanisms: Central (psychogenic) mechanism: food addiction. Hypothalamic mechanism: ⭡synthesis of neuropeptide Y Endocrine
- 30. Obesity Consequences Insulin Resistance and Type 2 Diabetes Mellitus weight gain ? insulin resistance ?type 2
- 31. Obesity Consequences Pulmonary Disease obesity hypoventilation syndrome ↓ oxygen and ⭡ carbon dioxide during sleep =
- 33. Скачать презентацию
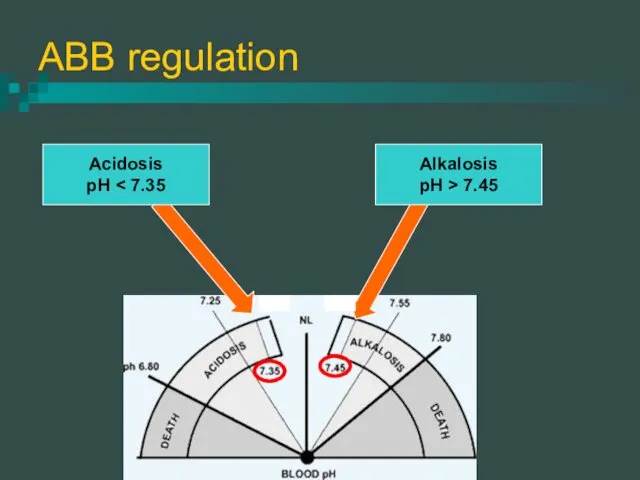
ABB regulation
Acidosis
pH < 7.35
Alkalosis
pH > 7.45
ABB regulation
Acidosis
pH < 7.35
Alkalosis
pH > 7.45
Blood buffer systems
Bicarbonate buffer system
the most mobile (can be
Blood buffer systems
Bicarbonate buffer system
the most mobile (can be
Physiological mechanisms of ABB regulation
Respiratory system
regulation of the PCO2 and,
Physiological mechanisms of ABB regulation
Respiratory system
regulation of the PCO2 and,
Respiratory acidosis
Reason: hypoventilation of lungs (obturation of respiratory tract, pulmonary
Respiratory acidosis
Reason: hypoventilation of lungs (obturation of respiratory tract, pulmonary
The effects of high pCO2
spasm of peripheral arterioles, ? of BP
The effects of high pCO2
spasm of peripheral arterioles, ? of BP
Metabolic acidosis
Reasons:
failure of the kidneys to excrete the metabolic acids (uremia)
loss
Metabolic acidosis
Reasons:
failure of the kidneys to excrete the metabolic acids (uremia)
loss
Metabolic acidosis
Formation of excess of metabolic acids in the body:
Ketoacidosis: accumulation
Metabolic acidosis
Formation of excess of metabolic acids in the body:
Ketoacidosis: accumulation
Acidosis clinical manifestation
depression of the central nervous system (from disorientation to
Acidosis clinical manifestation
depression of the central nervous system (from disorientation to
Respiratory alkalosis
Reason - hyperventilation:
excitation of respiratory center (brain inflammation or edema)
reflex
Respiratory alkalosis
Reason - hyperventilation:
excitation of respiratory center (brain inflammation or edema)
reflex
Metabolic alkalosis
Reasons:
Diuretic drugs – reabsorption of Na; loss of H+ and
Metabolic alkalosis
Reasons:
Diuretic drugs – reabsorption of Na; loss of H+ and
Clinical manifestation of alkalosis
? pCO2 – spasm of brain vessels and
Clinical manifestation of alkalosis
? pCO2 – spasm of brain vessels and
Water (Fluid) Balance Disorders
Hypohydration symptoms (2-15% of body weight)
? of blood
Water (Fluid) Balance Disorders
Hypohydration symptoms (2-15% of body weight)
? of blood
Water (Fluid) Balance Disorders
Hypohydration symptoms
Nervous system disorders:
headache, dizziness,
disorders of consciousness, inability
Water (Fluid) Balance Disorders
Hypohydration symptoms
Nervous system disorders:
headache, dizziness,
disorders of consciousness, inability
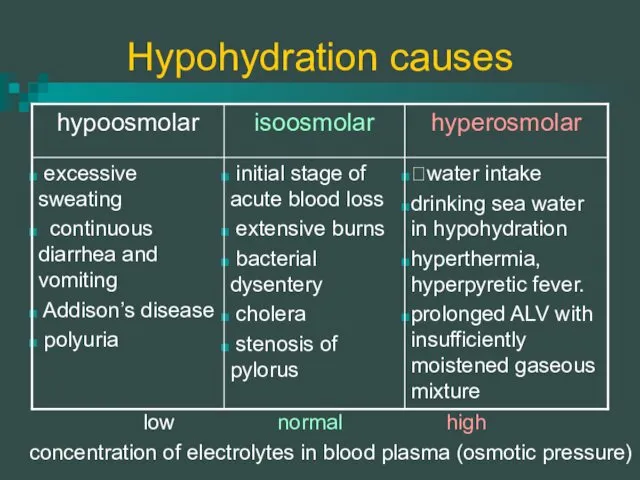
Hypohydration causes
concentration of electrolytes in blood plasma (osmotic pressure)
low
normal
high
Hypohydration causes
concentration of electrolytes in blood plasma (osmotic pressure)
low
normal
high
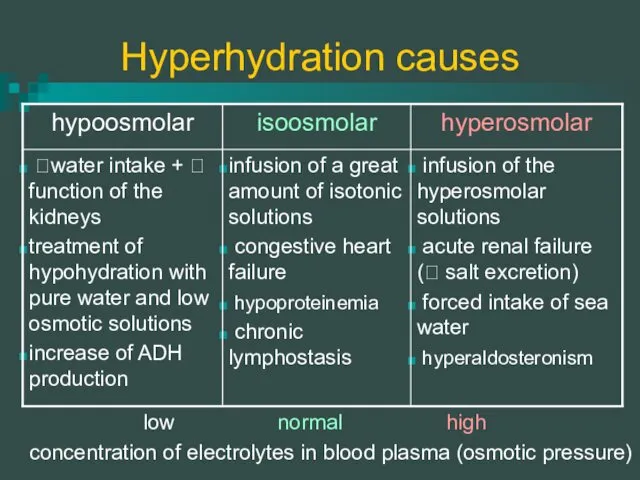
Hyperhydration causes
concentration of electrolytes in blood plasma (osmotic pressure)
low
normal
high
Hyperhydration causes
concentration of electrolytes in blood plasma (osmotic pressure)
low
normal
high
Hyperhydration symptoms
? blood circulating volume and ABP
heart overload
general edema
Hyperhydration symptoms
? blood circulating volume and ABP
heart overload
general edema
Edema
Accumulation of excess fluid:
in intercellular space
body cavities (hydrothorax, hydropericardium and
Edema
Accumulation of excess fluid:
in intercellular space
body cavities (hydrothorax, hydropericardium and
Edema mechanisms
? capillary hydrostatic pressure (high venous BP – local, systemic)
Alterations
Edema mechanisms
? capillary hydrostatic pressure (high venous BP – local, systemic)
Alterations
Starvation
Forms of starvation:
Total (absolute) – deprivation of food and water
Complete –
Starvation
Forms of starvation:
Total (absolute) – deprivation of food and water
Complete –
Starvation
Exogenous:
voluntary starvation
involuntary (social and economical problems)
eating disorders (Anorexia nervosa)
Starvation
Exogenous:
voluntary starvation
involuntary (social and economical problems)
eating disorders (Anorexia nervosa)
Stage 1. Early starvation
blood glucose ??glucagon ? glycogenolysis
Glycogen stores are depleted
Stage 1. Early starvation
blood glucose ??glucagon ? glycogenolysis
Glycogen stores are depleted
Stage 2 Prolonged starvation
protein catabolism
high lipolysis +
Stage 2 Prolonged starvation
protein catabolism
high lipolysis +
Stage 3 Terminal phase
Lipid stores of body are completely depleted (97-100%),
Stage 3 Terminal phase
Lipid stores of body are completely depleted (97-100%),
Obesity
Excessive accumulation and storage of fat in the body.
Body
Obesity
Excessive accumulation and storage of fat in the body.
Body
Obesity classification
General and local obesity.
Local obesity - central or peripheral.
Central
Obesity classification
General and local obesity.
Local obesity - central or peripheral.
Central
Obesity classification
Hyperplastic obesity - ⭡ number of fat cells.
massive obesity &
Obesity classification
Hyperplastic obesity - ⭡ number of fat cells.
massive obesity &
Obesity classification
Primary obesity - leptin deficiency or decreased function.
20% obese patients
Obesity classification
Primary obesity - leptin deficiency or decreased function.
20% obese patients
Obesity pathogenesis
Neural mechanisms:
Central (psychogenic) mechanism:
food addiction.
Hypothalamic mechanism:
⭡synthesis of neuropeptide Y
Obesity pathogenesis
Neural mechanisms:
Central (psychogenic) mechanism:
food addiction.
Hypothalamic mechanism:
⭡synthesis of neuropeptide Y
Obesity Consequences
Insulin Resistance and Type 2 Diabetes Mellitus
weight gain ?
Obesity Consequences
Insulin Resistance and Type 2 Diabetes Mellitus
weight gain ?
Obesity Consequences
Pulmonary Disease
obesity hypoventilation syndrome
↓ oxygen and ⭡ carbon
Obesity Consequences
Pulmonary Disease
obesity hypoventilation syndrome
↓ oxygen and ⭡ carbon
 Биоэквивалентность лекарственных средств
Биоэквивалентность лекарственных средств Острый мастит
Острый мастит Метод лактационной аменорреи
Метод лактационной аменорреи Оба қоздырғышы
Оба қоздырғышы Дитячі інфекційні захворювання. Лекція 19
Дитячі інфекційні захворювання. Лекція 19 Диагностика и удаление инородных тел глотки
Диагностика и удаление инородных тел глотки Врожденные расщелины верхней губы
Врожденные расщелины верхней губы Физиология спинного мозга. (Лекция 7)
Физиология спинного мозга. (Лекция 7) Травматизм и профессиональные заболевания в отрасли
Травматизм и профессиональные заболевания в отрасли Профилактические прививки. Реакции и осложнения
Профилактические прививки. Реакции и осложнения Рак печени
Рак печени Сәулемен қатаятын композитті пломбалық материалдар
Сәулемен қатаятын композитті пломбалық материалдар Дентальная имплантация в стоматологии. (Лекция 3)
Дентальная имплантация в стоматологии. (Лекция 3) Жүктіліктің УД зерттеу әдісі
Жүктіліктің УД зерттеу әдісі Переломы. Классификация переломов
Переломы. Классификация переломов Пероральные сахароснижающие ЛС
Пероральные сахароснижающие ЛС Виды бега и их влияние на здоровье человека
Виды бега и их влияние на здоровье человека Парапроктит (параректальный абсцесс)
Парапроктит (параректальный абсцесс) Rheumatic endocarditis
Rheumatic endocarditis Жарықтар. Іш жарығы (кіндік және ақ сызық)
Жарықтар. Іш жарығы (кіндік және ақ сызық) Гипотиреоз
Гипотиреоз Профилактика внутрисосудистых тромботических осложнений при травмах
Профилактика внутрисосудистых тромботических осложнений при травмах Неотложные состояния в урологии и андрологии
Неотложные состояния в урологии и андрологии Аутоимунный гепатит
Аутоимунный гепатит Діагностика та лікування дифтерії у дітей
Діагностика та лікування дифтерії у дітей Предмет і завдання дефектології. Поняття норма і відхилення в розвитку дитини. Лекція 1-2
Предмет і завдання дефектології. Поняття норма і відхилення в розвитку дитини. Лекція 1-2 Клиническая анатомия тройничного и лицевого нерва. Особенности анестезии в стоматологии
Клиническая анатомия тройничного и лицевого нерва. Особенности анестезии в стоматологии Асептика. Антисептика
Асептика. Антисептика