- General course of syphilis. Primary syphilis secondary syphslis

Содержание
- 2. Theoretical part Etiology of syphilis. Diagnostic laboratory tests for Treponema pallidum The basic method in the
- 3. Classification of syphilis Primary, seronegative syphilis – syphilis I seronegativa. Primary, seropositive syphilis – syphilis I
- 4. Classification of syphilis Latent syphilis – syphilis latens: Early latent syphilis – syphilis latens praecox; Late
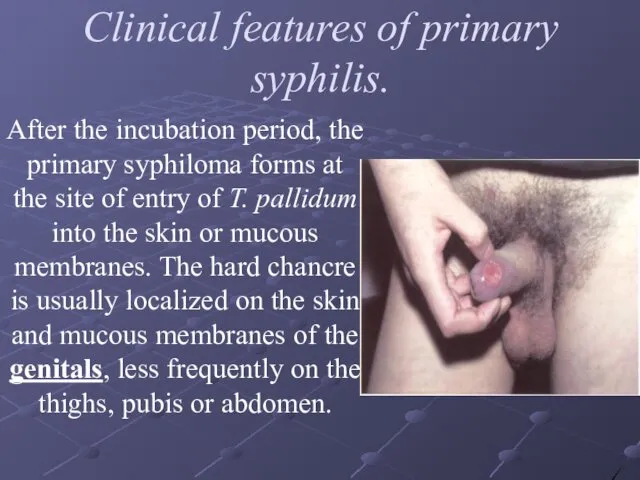
- 5. Clinical features of primary syphilis. After the incubation period, the primary syphiloma forms at the site
- 6. Clinical features of primary syphilis. The extragenital chancre, which is a less frequent occurrence, forms on
- 7. Clinical features of primary syphilis. Regional scleradenitis is the second most important symptom of primary syphilis.
- 8. Atypical Chancres Chancre-amygdalitis is characterized by enlargement and hardening of one tonsil with no erosion or
- 9. Atypical Chancres Indurative swelling as a manifestation of the primary period of syphilis is found in
- 10. Complications of hard chancre Balanitis is the commonest complication. It develops as a result of attendant
- 11. Complications of hard chancre Balanoposthitis may lead to constriction of the prepuce so that the foreskin
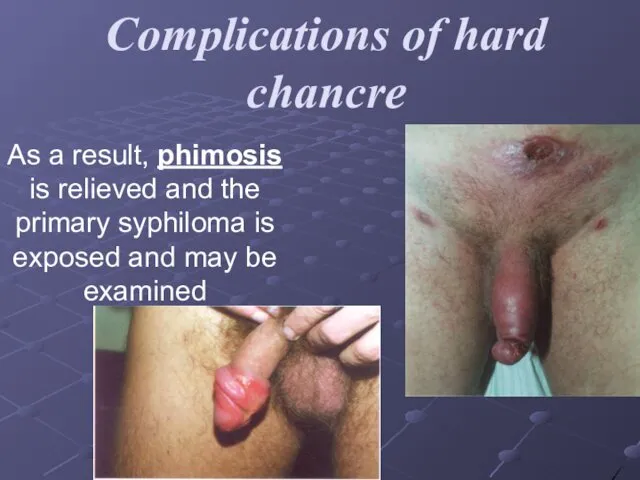
- 12. Complications of hard chancre As a result, phimosis is relieved and the primary syphiloma is exposed
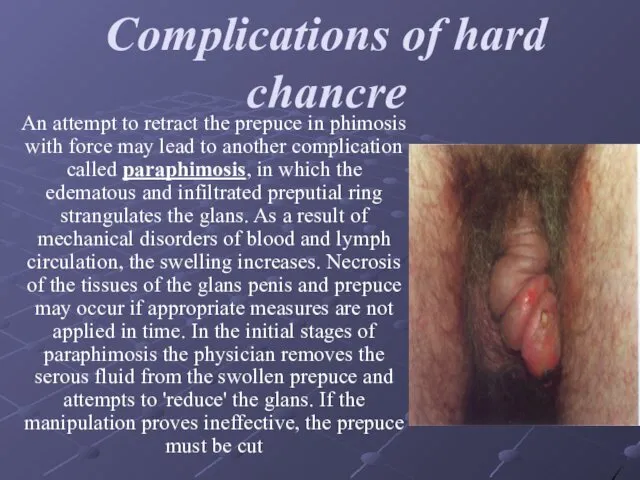
- 13. Complications of hard chancre An attempt to retract the prepuce in phimosis with force may lead
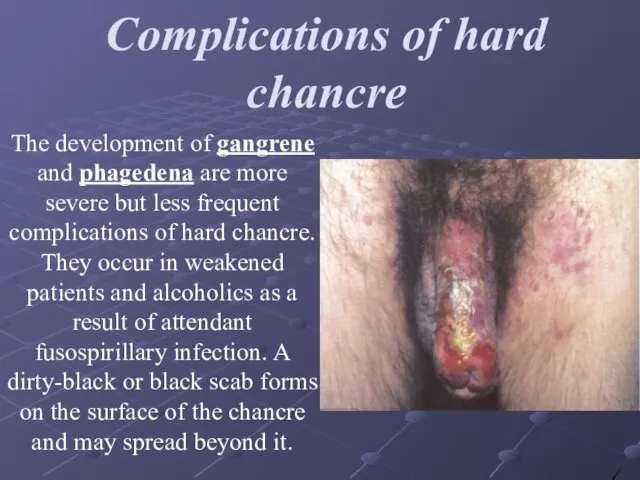
- 14. Complications of hard chancre The development of gangrene and phagedena are more severe but less frequent
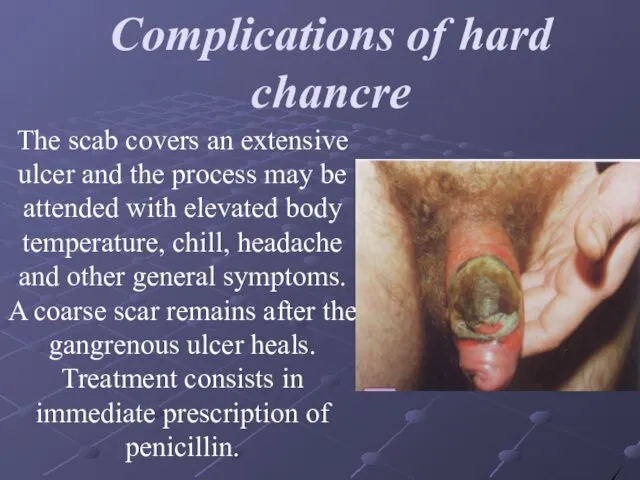
- 15. Complications of hard chancre The scab covers an extensive ulcer and the process may be attended
- 16. Secondary syphilis Secondary syphilis develops 2.5-3, rarely 4 months later after infection. Without treatment relapses can
- 17. Secondary Siphilis Characteristic signs of secondary syphilis Focal situation of the lesions. Round form and sharp
- 18. Secondary syphilis Macular syphilis, or syphilitic roseola. Clinical and morphological characteristics of syphilitic roseolaThe following clinical
- 19. Diagnosis of macular syphilid (roseola) is based on its characteristic features: vascular macula, which disappears by
- 20. Papular syphilid is often a sign of secondary, usually relapsing syphilis. The papule is situated in
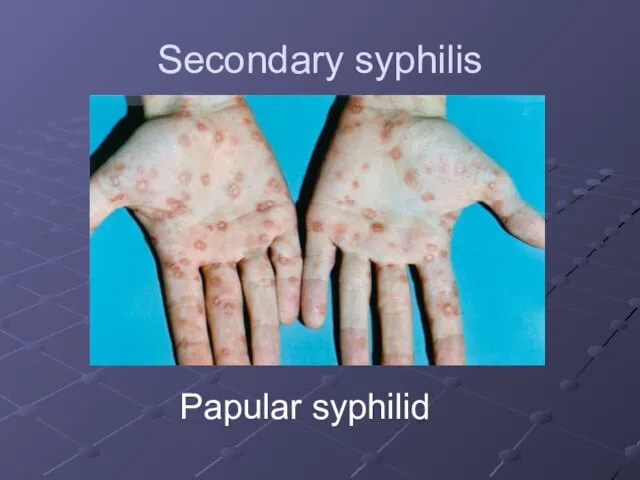
- 21. Secondary syphilis Papular syphilid
- 22. The following clinical varieties of papular lesions are differentiated: a) miliary B) lenticular C) coin-shaped D)
- 23. Secondary syphilis - Papular syphilid
- 24. Pustular syphilid. Pustular syphilid occurs rarely and develops in weak patients and in alcoholics. The following
- 25. Syphilitic alopecia or calvities Alopecia areata: diffuse and mixed forms are differentiated. Syphilitic alopecia can be
- 27. Скачать презентацию
Theoretical part
Etiology of syphilis. Diagnostic laboratory tests for Treponema pallidum
The
Theoretical part
Etiology of syphilis. Diagnostic laboratory tests for Treponema pallidum
The
Classification of syphilis
Primary, seronegative syphilis – syphilis I seronegativa.
Primary, seropositive syphilis
Classification of syphilis
Primary, seronegative syphilis – syphilis I seronegativa.
Primary, seropositive syphilis
Classification of syphilis
Latent syphilis – syphilis latens:
Early latent syphilis – syphilis
Classification of syphilis
Latent syphilis – syphilis latens:
Early latent syphilis – syphilis
Clinical features of primary syphilis.
After the incubation period, the primary
Clinical features of primary syphilis.
After the incubation period, the primary
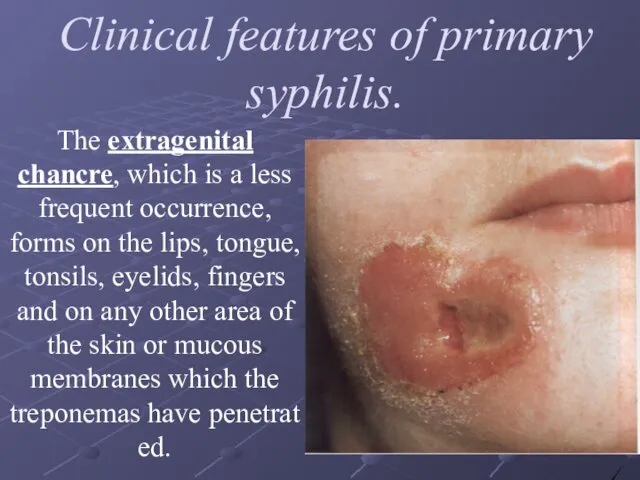
Clinical features of primary syphilis.
The extragenital chancre, which is a less
Clinical features of primary syphilis.
The extragenital chancre, which is a less
Clinical features of primary syphilis.
Regional scleradenitis is the second most important
Clinical features of primary syphilis.
Regional scleradenitis is the second most important
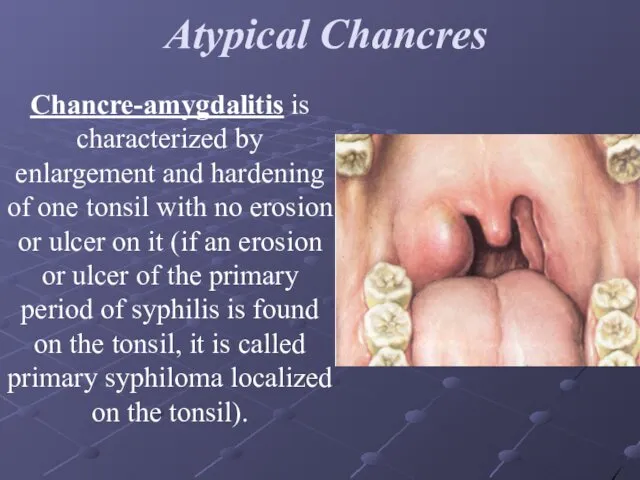
Atypical Chancres
Chancre-amygdalitis is characterized by enlargement and hardening of one
Atypical Chancres
Chancre-amygdalitis is characterized by enlargement and hardening of one
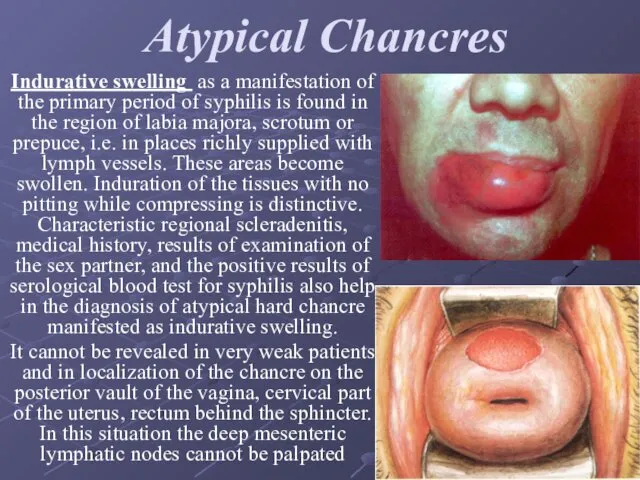
Atypical Chancres
Indurative swelling as a manifestation of the primary period of
Atypical Chancres
Indurative swelling as a manifestation of the primary period of
Complications of hard chancre
Balanitis is the commonest complication. It develops as
Complications of hard chancre
Balanitis is the commonest complication. It develops as
Complications of hard chancre
Balanoposthitis may lead to constriction of the prepuce
Complications of hard chancre
Balanoposthitis may lead to constriction of the prepuce
Complications of hard chancre
As a result, phimosis is relieved and the
Complications of hard chancre
As a result, phimosis is relieved and the
Complications of hard chancre
An attempt to retract the prepuce in phimosis
Complications of hard chancre
An attempt to retract the prepuce in phimosis
Complications of hard chancre
The development of gangrene and phagedena are more
Complications of hard chancre
The development of gangrene and phagedena are more
Complications of hard chancre
The scab covers an extensive ulcer and the
Complications of hard chancre
The scab covers an extensive ulcer and the
Secondary syphilis
Secondary syphilis develops 2.5-3, rarely 4 months later after infection.
Secondary syphilis
Secondary syphilis develops 2.5-3, rarely 4 months later after infection.
Secondary Siphilis
Characteristic signs of secondary syphilis
Focal situation of the lesions.
Round form
Secondary Siphilis
Characteristic signs of secondary syphilis
Focal situation of the lesions.
Round form
Secondary syphilis
Macular syphilis, or syphilitic roseola. Clinical and morphological characteristics of
Secondary syphilis
Macular syphilis, or syphilitic roseola. Clinical and morphological characteristics of
Diagnosis of macular syphilid (roseola) is based on its characteristic features:
Diagnosis of macular syphilid (roseola) is based on its characteristic features:
Papular syphilid
is often a sign of secondary, usually relapsing syphilis.
Papular syphilid
is often a sign of secondary, usually relapsing syphilis.
Secondary syphilis
Papular syphilid
Secondary syphilis
Papular syphilid
The following clinical varieties of papular lesions are differentiated:
a) miliary
B) lenticular
C)
The following clinical varieties of papular lesions are differentiated:
a) miliary
B) lenticular
C)

Secondary syphilis - Papular syphilid
Secondary syphilis - Papular syphilid
Pustular syphilid.
Pustular syphilid occurs rarely and develops in weak patients and
Pustular syphilid.
Pustular syphilid occurs rarely and develops in weak patients and
Syphilitic alopecia or calvities
Alopecia areata: diffuse and mixed forms are differentiated.
Syphilitic alopecia or calvities
Alopecia areata: diffuse and mixed forms are differentiated.
 Неотложная радиология в урологии. Почечная колика
Неотложная радиология в урологии. Почечная колика Психикалық және мінез-құлық бұзылыстарының этиологиясы және таралуы
Психикалық және мінез-құлық бұзылыстарының этиологиясы және таралуы Regularities of post-embryonic development
Regularities of post-embryonic development Инфекционная безопасность пациента и персонала
Инфекционная безопасность пациента и персонала Гражданско-правовая ответственность медицинских работников
Гражданско-правовая ответственность медицинских работников Инфекции, связанные с оказанием медицинской помощи. ИСМП
Инфекции, связанные с оказанием медицинской помощи. ИСМП Гиперпластические процессы и рак эндометрия
Гиперпластические процессы и рак эндометрия Босанған әйелдерде қаламаған жүктілікті алдын алу мақсатында жатыр ішілік спираль (жіс) мен гормональды контрацепцияның
Босанған әйелдерде қаламаған жүктілікті алдын алу мақсатында жатыр ішілік спираль (жіс) мен гормональды контрацепцияның Правовое регулирование установления инвалидности
Правовое регулирование установления инвалидности Клинические практические руководства. Принципы разработки и внедрения в практику. Преимущества и недостатки
Клинические практические руководства. Принципы разработки и внедрения в практику. Преимущества и недостатки Асептика және антисептика
Асептика және антисептика Лапароскопия
Лапароскопия Формулярная система: разработка формуляров на различных уровнях системы здравоохранения
Формулярная система: разработка формуляров на различных уровнях системы здравоохранения Превентивные мероприятия в ветеринарной практике
Превентивные мероприятия в ветеринарной практике Баланың физикалық және жүйке-психикалық дамуын бағалау
Баланың физикалық және жүйке-психикалық дамуын бағалау Оказание первой доврачебной помощи пострадавшим
Оказание первой доврачебной помощи пострадавшим Антигены: строение молекул, свойства
Антигены: строение молекул, свойства Гигиена кожи
Гигиена кожи Геморрагическа я лихорадка Эбола
Геморрагическа я лихорадка Эбола Рентгенологические методы исследования заболеваний почек и мочевыводящих путей в педиатрии
Рентгенологические методы исследования заболеваний почек и мочевыводящих путей в педиатрии Гормональна контрацепція
Гормональна контрацепція Хронический панкреатит. Консервативное лечение
Хронический панкреатит. Консервативное лечение Қазақстандағы денсаулық сақтау ұйымы және бағдарламалары
Қазақстандағы денсаулық сақтау ұйымы және бағдарламалары Дисбиоз кишечника. Как поставить диагноз практическому врачу
Дисбиоз кишечника. Как поставить диагноз практическому врачу Су - Джок терапия для детей и взрослых
Су - Джок терапия для детей и взрослых Личная гигиена
Личная гигиена Школы здоровья ИБС и АГ
Школы здоровья ИБС и АГ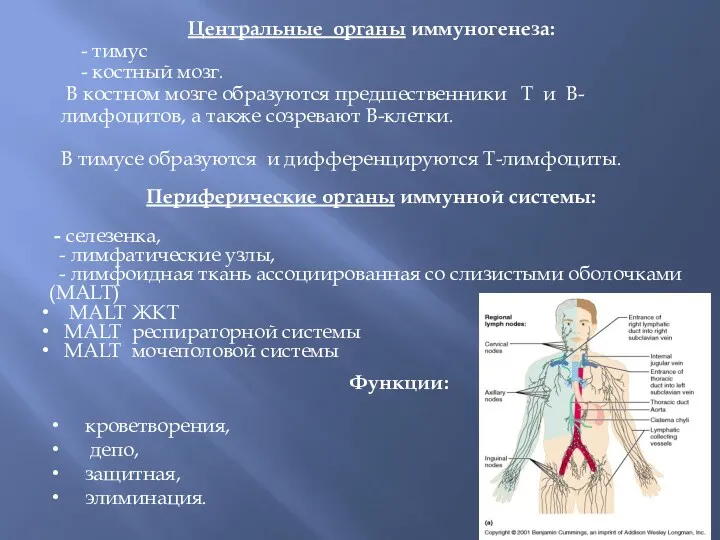 Центральные органы иммуногенеза
Центральные органы иммуногенеза