- Gynecological infections and abnormalities

Содержание
- 2. Dysmenorrhea Most common cause of pelvic pain in females. Definition - menstrual pain Etiology - Obstruction
- 3. Dysmenorrhea Management. NSAIDS (nonsteroidal anti inflammatory drugs). Oral contraceptive. Adequate rest and sleep and regular exercise
- 4. Premenstrual syndrome (PMS) premenstrual tension Definition--is a distinct clinical entity characterized by a cluster of physical
- 5. Premenstrual syndrome (PMS) premenstrual tension Known precipitating factors include an increase in antidiuretic hormone and aldosterone
- 6. Premenstrual syndrome (PMS) premenstrual tension PMS increases with age and body weight. Uncommon in women in
- 7. Premenstrual syndrome (PMS) premenstrual tension Symptoms. Physical. Painful and swollen breast. Bloating. Abdominal pain. Headache and
- 8. Premenstrual syndrome (PMS) premenstrual tension Psychologically. Depression. Anxiety. Irritability. Behavioral changes.
- 9. Premenstrual syndrome (PMS) premenstrual tension Treatment. Past treatment has been symptomatic. Diuretics to reduce fluid retention.
- 10. Premenstrual syndrome (PMS) premenstrual tension Treatment. Decrease salt intake to relieve bloating and edema. Drug therapy
- 11. Pelvic Inflammatory Disease Definition--Pelvic Inflammatory Disease (PID) is any acute, subacute, recurrent, or chronic infection of
- 12. Pelvic Inflammatory Disease Sites - it includes inflammation of the cervix (cervicitis) uterus (endometritis) fallopian tubes
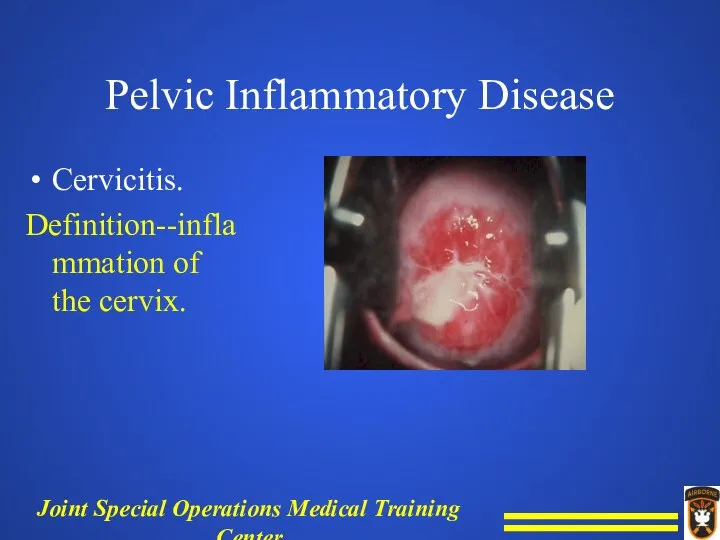
- 13. Pelvic Inflammatory Disease Cervicitis. Definition--inflammation of the cervix.
- 14. Pelvic Inflammatory Disease Causative organisms - gonococcus, streptococcus, staphylococcus, aerobic and anaerobic organisms, herpes virus, and
- 15. Pelvic Inflammatory Disease Forms of cervicitis-- Acute and Chronic.
- 16. Pelvic Inflammatory Disease Acute cervicitis. Symptoms. Purulent, foul smelling vaginal discharge. Itching and/or burning sensation. Red,
- 17. Pelvic Inflammatory Disease Acute cervicitis. Assessment. Physical examination. Cultures for N. gonorrhea are positive greater than
- 18. Pelvic Inflammatory Disease Chronic cervicitis. Symptoms. Cervical dystocia--difficult labor. Lacerations or eversion of the cervix. Ulceration
- 19. Pelvic Inflammatory Disease Assessment. Physical examination. Chronic cervicitis, causative organisms are usually staphylococcus or streptococcus.
- 20. Pelvic Inflammatory Disease Management - manage by cauterization, cryotherapy, conization (excision of a cone of tissue).
- 21. Pelvic Inflammatory Disease Endometritis. Definition - inflammation of the endometrium. Etiology - produced by bacterial infection
- 22. Pelvic Inflammatory Disease Endometritis. Etiology - produced by bacterial infection most commonly staphylococci, colon bacilli, or
- 23. NOTE Endometriosis - ectopic endometrium located in various sites throughout the pelvis or on the abdominal
- 25. Pelvic Inflammatory Disease Endometriosis Symptoms. Low back and low abdominal pain. Dysmenorrhea. Menorrhagia. Pain on defecation,
- 26. Pelvic Inflammatory Disease Endometriosis Assessment. Physical examination. Vaginal cultures. Management - based upon culture results.
- 27. Pelvic Inflammatory Disease Salpingitis and Oophoritis. Definition - infection of the fallopian tubes and ovaries. History
- 28. Pelvic Inflammatory Disease Salpingitis and Oophoritis. Signs and symptoms. Lower abdominal pain sometimes with signs and
- 29. Pelvic Inflammatory Disease Salpingitis and Oophoritis. Signs and symptoms (cont.) Purulent cervical discharge. Leukocytosis.
- 30. Pelvic Inflammatory Disease Salpingitis and Oophoritis. Assessment. Physical examination. Gonorrhea culture. Test for chlamydia.
- 31. Pelvic Inflammatory Disease Salpingitis and Oophoritis Complications. Tubal abscess. Infertility--common.
- 32. Pelvic Inflammatory Disease Salpingitis and Oophoritis Management. IV fluids to correct dehydration. NG suction in the
- 33. OTHER GYN ASSOCIATED ABNORMALITIES.
- 34. Ovarian Cyst
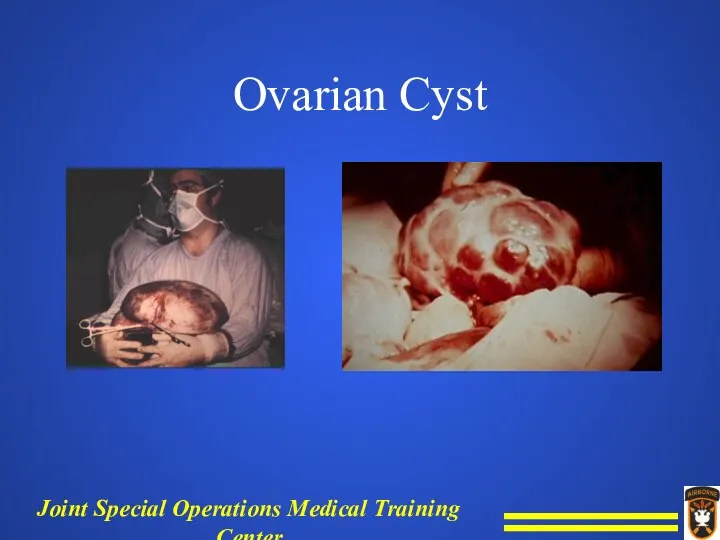
- 35. Ovarian Cyst Ovarian cysts are usually nonneoplastic sacs on an ovary that contain fluid or semisolid
- 36. Ovarian Cyst Sudden or sharp pain may indicate rupture, hemorrhage, or torsion of cyst. Fever, leukocytosis
- 37. OTHER GYN ASSOCIATED ABNORMALITIES Leukorrhea - white/yellowish mucoid discharge from cervical canal or vagina.
- 38. Leukorrhea Probably most frequently encountered gynecological symptom. Generally associated with simple infection of the cervix and
- 39. OTHER GYN ASSOCIATED ABNORMALITIES Candidiasis Trichomonas Gardnerella Bartholin’s abscess VAGINITIS - Inflammation of the vagina
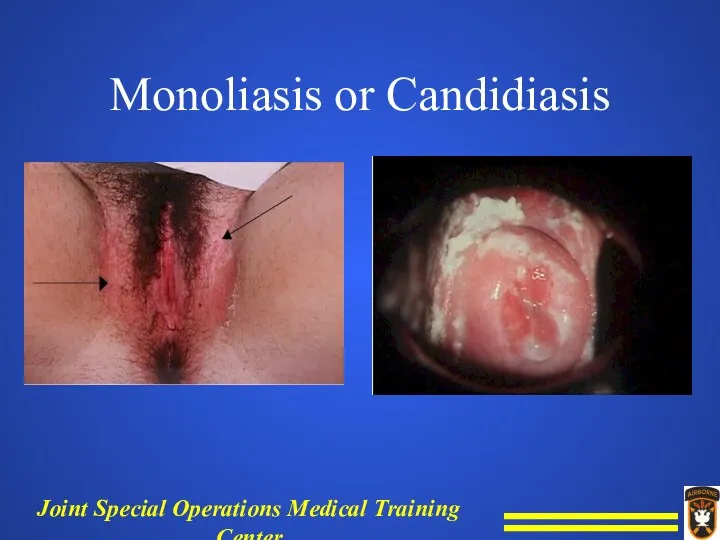
- 40. Monoliasis or Candidiasis
- 41. Monoliasis or Candidiasis Signs and symptoms. Marked leukorrhea, marked redness of vulva, extreme pruritus. White, creamy,
- 42. Monoliasis or Candidiasis Assessment - lab KOH wet mount NS KOH 10% 20% look for (branching
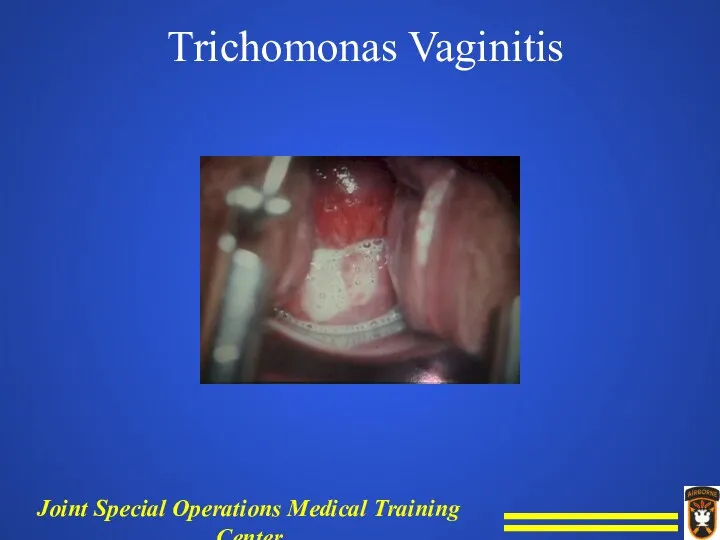
- 43. Trichomonas Vaginitis
- 44. Trichomonas Vaginitis Signs and symptoms. Leukorrhea, vaginal soreness, burning, pruritus, dyspareunia (pain during intercourse). Bubbly, yellowish
- 45. Trichomonas Vaginitis Assessment - lab wet prep, microscopic exam reveals pear shaped parasite with long flagella
- 46. Bacterial Vaginitis (Gardnerella vaginitis) Signs and symptoms. Leukorrhea, pruritus, dyspareunia. Turbid, chalky, white/gray or yellowish discharge;
- 47. Bacterial Vaginitis (Gardnerella vaginitis) Assessment. Gram-positive nonmotile coccobacillus that normally inhabits the vagina. Wet smears of
- 48. Bacterial Vaginitis (Gardnerella vaginitis) Management. Metronidazole (Flagyl) 250 mg TID to 500 mg BID orally for
- 49. Perineal pain - Bartholin’s abscess Definition and etiology - acute or chronic infection of the Bartholin's
- 50. Perineal pain - Bartholin’s abscess Signs and symptoms. Mass in perineum that is hot, tender, and
- 52. Perineal pain - Bartholin’s abscess Management. I & D. Sitz bath. Broad-spectrum antibiotics which cover gram-positive
- 53. BREAST ABNORMALITIES.
- 54. Acute Mastitis Definition - bacterial infection of breast. Time - confined generally to the first 2
- 55. Acute Mastitis Signs and symptoms. Pain in the breast. Withdraw from palpation. Erythema. Induration. Hot.
- 56. Acute Mastitis Management. Prevention by good hygiene. Preabscess--antibiotics. Abscess I & D.
- 57. Chronic Cystic Mastitis Benign pathology - fibrocystic syndrome. Age - begins in twenties and increases with
- 58. Chronic Cystic Mastitis Significance - increased incidence of breast cancer 3-5 times. Management. Rule out cancer.
- 59. Malignant Breast Lesions Primary Malignancy Origin--primarily the ducts. Incidence. Major cancer killer of females. 1 out
- 60. Malignant Breast Lesions Risk factors. Age, over 40. Sex F:M = 100:1. Family history of breast
- 61. Malignant Breast Lesions Signs and symptoms Persistent lump or thickening, hard irregular mass. Fixation--tumor invades surrounding
- 62. Malignant Breast Lesions Signs and symptoms. Invade skin--ulcer, satellite. Peau d'orange--invasion of lymphatics causes edema. Hard,
- 63. Malignant Breast Lesions Signs and symptoms. Bloody nipple discharge. Metastasis--bone pain, fracture, lung, liver. Pain or
- 64. Malignant Breast Lesions Assessment. Physical exam suspicion. Self breast exam suspicion. Mammogram X ray exam of
- 65. Malignant Breast Lesions Survival - increases with early diagnosis because size of lesion is smaller and
- 66. Breast Abnormalities Metastic malignancy of the breast - systemic involvement; breast changes during pregnancy with some
- 67. BREAST CHANGES DURING PREGNANCY
- 68. Breasts in Pregnancy Physical Findings - Tenderness. Increase in size and veins. Nipples increase in size
- 69. Breasts in Pregnancy Lactation. Milk letdown in response to suckling or crying. Requires adequate fluids. Production
- 70. Breasts in Pregnancy Lactation. Most drugs ingested are secreted. Engorgement--manage with binder, ice, codeine. Suppression--ice, binder,
- 71. Lactation Agalactia - complete lack of milk, very rare. Polygalactia - excess milk.
- 72. SUMMARY Evaluation and management of gynecologic infections and abnormalities require the ability to recognize normal structures
- 73. SUMMARY From that point, one must be able to categorize the problem into an anatomical, traumatic
- 74. SUMMARY Knowing the key signs and symptoms for each of these categories will ensure your ability
- 75. QUESTIONS???
- 77. Скачать презентацию
Dysmenorrhea
Most common cause of pelvic pain in females.
Definition - menstrual pain
Etiology
Dysmenorrhea
Most common cause of pelvic pain in females.
Definition - menstrual pain
Etiology
Dysmenorrhea
Management.
NSAIDS (nonsteroidal anti inflammatory drugs).
Oral contraceptive.
Adequate rest and sleep and regular
Dysmenorrhea
Management.
NSAIDS (nonsteroidal anti inflammatory drugs).
Oral contraceptive.
Adequate rest and sleep and regular
Premenstrual syndrome (PMS) premenstrual tension
Definition--is a distinct clinical entity characterized by
Premenstrual syndrome (PMS) premenstrual tension
Definition--is a distinct clinical entity characterized by
Premenstrual syndrome (PMS) premenstrual tension
Known precipitating factors include an increase in
Premenstrual syndrome (PMS) premenstrual tension
Known precipitating factors include an increase in
Premenstrual syndrome (PMS) premenstrual tension
PMS increases with age and body weight.
Uncommon
Premenstrual syndrome (PMS) premenstrual tension
PMS increases with age and body weight.
Uncommon
Premenstrual syndrome (PMS) premenstrual tension
Symptoms.
Physical.
Painful and swollen breast.
Bloating.
Abdominal pain.
Headache and back
Premenstrual syndrome (PMS) premenstrual tension
Symptoms.
Physical.
Painful and swollen breast.
Bloating.
Abdominal pain.
Headache and back
Premenstrual syndrome (PMS) premenstrual tension
Psychologically.
Depression.
Anxiety.
Irritability.
Behavioral changes.
Premenstrual syndrome (PMS) premenstrual tension
Psychologically.
Depression.
Anxiety.
Irritability.
Behavioral changes.
Premenstrual syndrome (PMS) premenstrual tension
Treatment.
Past treatment has been symptomatic.
Diuretics to reduce
Premenstrual syndrome (PMS) premenstrual tension
Treatment.
Past treatment has been symptomatic.
Diuretics to reduce
Premenstrual syndrome (PMS) premenstrual tension
Treatment.
Decrease salt intake to relieve bloating and
Premenstrual syndrome (PMS) premenstrual tension
Treatment.
Decrease salt intake to relieve bloating and
Pelvic Inflammatory Disease
Definition--Pelvic Inflammatory Disease (PID) is any acute, subacute, recurrent,
Pelvic Inflammatory Disease
Definition--Pelvic Inflammatory Disease (PID) is any acute, subacute, recurrent,
Pelvic Inflammatory Disease
Sites - it includes inflammation of the cervix (cervicitis)
Pelvic Inflammatory Disease
Sites - it includes inflammation of the cervix (cervicitis)
Pelvic Inflammatory Disease
Cervicitis.
Definition--inflammation of the cervix.
Pelvic Inflammatory Disease
Cervicitis.
Definition--inflammation of the cervix.
Pelvic Inflammatory Disease
Causative organisms - gonococcus, streptococcus, staphylococcus, aerobic and anaerobic
Pelvic Inflammatory Disease
Causative organisms - gonococcus, streptococcus, staphylococcus, aerobic and anaerobic
Pelvic Inflammatory Disease
Forms of cervicitis--
Acute and Chronic.
Pelvic Inflammatory Disease
Forms of cervicitis--
Acute and Chronic.
Pelvic Inflammatory Disease
Acute cervicitis.
Symptoms.
Purulent, foul smelling vaginal discharge.
Itching and/or burning sensation.
Red,
Pelvic Inflammatory Disease
Acute cervicitis.
Symptoms.
Purulent, foul smelling vaginal discharge.
Itching and/or burning sensation.
Red,
Pelvic Inflammatory Disease
Acute cervicitis.
Assessment.
Physical examination.
Cultures for N. gonorrhea are positive greater
Pelvic Inflammatory Disease
Acute cervicitis.
Assessment.
Physical examination.
Cultures for N. gonorrhea are positive greater
Pelvic Inflammatory Disease
Chronic cervicitis.
Symptoms.
Cervical dystocia--difficult labor.
Lacerations or eversion of the cervix.
Ulceration
Pelvic Inflammatory Disease
Chronic cervicitis.
Symptoms.
Cervical dystocia--difficult labor.
Lacerations or eversion of the cervix.
Ulceration
Pelvic Inflammatory Disease
Assessment.
Physical examination.
Chronic cervicitis, causative organisms are usually staphylococcus or
Pelvic Inflammatory Disease
Assessment.
Physical examination.
Chronic cervicitis, causative organisms are usually staphylococcus or
Pelvic Inflammatory Disease
Management - manage by cauterization, cryotherapy, conization (excision of
Pelvic Inflammatory Disease
Management - manage by cauterization, cryotherapy, conization (excision of
Pelvic Inflammatory Disease
Endometritis.
Definition - inflammation of the endometrium.
Etiology - produced by
Pelvic Inflammatory Disease
Endometritis.
Definition - inflammation of the endometrium.
Etiology - produced by
Pelvic Inflammatory Disease
Endometritis.
Etiology - produced by bacterial infection most commonly staphylococci,
Pelvic Inflammatory Disease
Endometritis.
Etiology - produced by bacterial infection most commonly staphylococci,
NOTE
Endometriosis - ectopic endometrium located in various sites throughout the pelvis
NOTE
Endometriosis - ectopic endometrium located in various sites throughout the pelvis

Pelvic Inflammatory Disease
Endometriosis
Symptoms.
Low back and low abdominal pain.
Dysmenorrhea.
Menorrhagia.
Pain on defecation, constipation.
Sterility.
Pelvic Inflammatory Disease
Endometriosis
Symptoms.
Low back and low abdominal pain.
Dysmenorrhea.
Menorrhagia.
Pain on defecation, constipation.
Sterility.
Pelvic Inflammatory Disease
Endometriosis
Assessment.
Physical examination.
Vaginal cultures.
Management - based upon culture results.
Pelvic Inflammatory Disease
Endometriosis
Assessment.
Physical examination.
Vaginal cultures.
Management - based upon culture results.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Definition - infection of the fallopian tubes
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Definition - infection of the fallopian tubes
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Signs and symptoms.
Lower abdominal pain sometimes with
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Signs and symptoms.
Lower abdominal pain sometimes with
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Signs and symptoms (cont.)
Purulent cervical discharge.
Leukocytosis.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Signs and symptoms (cont.)
Purulent cervical discharge.
Leukocytosis.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Assessment.
Physical examination.
Gonorrhea culture.
Test for chlamydia.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis.
Assessment.
Physical examination.
Gonorrhea culture.
Test for chlamydia.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis
Complications.
Tubal abscess.
Infertility--common.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis
Complications.
Tubal abscess.
Infertility--common.
Pelvic Inflammatory Disease
Salpingitis and Oophoritis
Management.
IV fluids to correct dehydration.
NG suction in
Pelvic Inflammatory Disease
Salpingitis and Oophoritis
Management.
IV fluids to correct dehydration.
NG suction in
OTHER GYN ASSOCIATED ABNORMALITIES.
OTHER GYN ASSOCIATED ABNORMALITIES.
Ovarian Cyst
Ovarian Cyst
Ovarian Cyst
Ovarian cysts are usually nonneoplastic sacs on an ovary that
Ovarian Cyst
Ovarian cysts are usually nonneoplastic sacs on an ovary that
Ovarian Cyst
Sudden or sharp pain may indicate rupture, hemorrhage, or torsion
Ovarian Cyst
Sudden or sharp pain may indicate rupture, hemorrhage, or torsion
OTHER GYN ASSOCIATED ABNORMALITIES
Leukorrhea - white/yellowish mucoid discharge from cervical canal
OTHER GYN ASSOCIATED ABNORMALITIES
Leukorrhea - white/yellowish mucoid discharge from cervical canal
Leukorrhea
Probably most frequently encountered gynecological symptom.
Generally associated with simple infection of
Leukorrhea
Probably most frequently encountered gynecological symptom.
Generally associated with simple infection of
OTHER GYN ASSOCIATED ABNORMALITIES
Candidiasis
Trichomonas
Gardnerella
Bartholin’s abscess
VAGINITIS - Inflammation of the vagina
OTHER GYN ASSOCIATED ABNORMALITIES
Candidiasis
Trichomonas
Gardnerella
Bartholin’s abscess
VAGINITIS - Inflammation of the vagina
Monoliasis or Candidiasis
Monoliasis or Candidiasis
Monoliasis or Candidiasis
Signs and symptoms.
Marked leukorrhea, marked redness of vulva, extreme
Monoliasis or Candidiasis
Signs and symptoms.
Marked leukorrhea, marked redness of vulva, extreme
Monoliasis or Candidiasis
Assessment - lab KOH wet mount NS KOH 10%
Monoliasis or Candidiasis
Assessment - lab KOH wet mount NS KOH 10%
Trichomonas Vaginitis
Trichomonas Vaginitis
Trichomonas Vaginitis
Signs and symptoms.
Leukorrhea, vaginal soreness, burning, pruritus, dyspareunia (pain during
Trichomonas Vaginitis
Signs and symptoms.
Leukorrhea, vaginal soreness, burning, pruritus, dyspareunia (pain during
Trichomonas Vaginitis
Assessment - lab wet prep, microscopic exam reveals pear shaped
Trichomonas Vaginitis
Assessment - lab wet prep, microscopic exam reveals pear shaped
Bacterial Vaginitis
(Gardnerella vaginitis)
Signs and symptoms.
Leukorrhea, pruritus, dyspareunia.
Turbid, chalky, white/gray or
Bacterial Vaginitis
(Gardnerella vaginitis)
Signs and symptoms.
Leukorrhea, pruritus, dyspareunia.
Turbid, chalky, white/gray or
Bacterial Vaginitis
(Gardnerella vaginitis)
Assessment.
Gram-positive nonmotile coccobacillus that normally inhabits the vagina.
Wet
Bacterial Vaginitis
(Gardnerella vaginitis)
Assessment.
Gram-positive nonmotile coccobacillus that normally inhabits the vagina.
Wet
Bacterial Vaginitis
(Gardnerella vaginitis)
Management.
Metronidazole (Flagyl) 250 mg TID to 500 mg
Bacterial Vaginitis
(Gardnerella vaginitis)
Management.
Metronidazole (Flagyl) 250 mg TID to 500 mg
Perineal pain -
Bartholin’s abscess
Definition and etiology - acute or chronic infection
Perineal pain -
Bartholin’s abscess
Definition and etiology - acute or chronic infection
Perineal pain -
Bartholin’s abscess
Signs and symptoms.
Mass in perineum that is hot,
Perineal pain -
Bartholin’s abscess
Signs and symptoms.
Mass in perineum that is hot,

Perineal pain -
Bartholin’s abscess
Management.
I & D.
Sitz bath.
Broad-spectrum antibiotics which cover gram-positive
Perineal pain -
Bartholin’s abscess
Management.
I & D.
Sitz bath.
Broad-spectrum antibiotics which cover gram-positive
BREAST ABNORMALITIES.
BREAST ABNORMALITIES.
Acute Mastitis
Definition - bacterial infection of breast.
Time - confined generally to
Acute Mastitis
Definition - bacterial infection of breast.
Time - confined generally to
Acute Mastitis
Signs and symptoms.
Pain in the breast.
Withdraw from palpation.
Erythema.
Induration.
Hot.
Acute Mastitis
Signs and symptoms.
Pain in the breast.
Withdraw from palpation.
Erythema.
Induration.
Hot.
Acute Mastitis
Management.
Prevention by good hygiene.
Preabscess--antibiotics.
Abscess I & D.
Acute Mastitis
Management.
Prevention by good hygiene.
Preabscess--antibiotics.
Abscess I & D.
Chronic Cystic Mastitis
Benign pathology - fibrocystic syndrome.
Age - begins in twenties
Chronic Cystic Mastitis
Benign pathology - fibrocystic syndrome.
Age - begins in twenties
Chronic Cystic Mastitis
Significance - increased incidence of breast cancer 3-5 times.
Management.
Rule
Chronic Cystic Mastitis
Significance - increased incidence of breast cancer 3-5 times.
Management.
Rule
Malignant Breast Lesions
Primary Malignancy
Origin--primarily the ducts.
Incidence.
Major cancer killer of females.
1
Malignant Breast Lesions
Primary Malignancy
Origin--primarily the ducts.
Incidence.
Major cancer killer of females.
1
Malignant Breast Lesions
Risk factors.
Age, over 40.
Sex F:M = 100:1.
Family history of
Malignant Breast Lesions
Risk factors.
Age, over 40.
Sex F:M = 100:1.
Family history of
Malignant Breast Lesions
Signs and symptoms
Persistent lump or thickening, hard irregular mass.
Fixation--tumor
Malignant Breast Lesions
Signs and symptoms
Persistent lump or thickening, hard irregular mass.
Fixation--tumor
Malignant Breast Lesions
Signs and symptoms.
Invade skin--ulcer, satellite.
Peau d'orange--invasion of lymphatics causes
Malignant Breast Lesions
Signs and symptoms.
Invade skin--ulcer, satellite.
Peau d'orange--invasion of lymphatics causes
Malignant Breast Lesions
Signs and symptoms.
Bloody nipple discharge.
Metastasis--bone pain, fracture, lung, liver.
Pain
Malignant Breast Lesions
Signs and symptoms.
Bloody nipple discharge.
Metastasis--bone pain, fracture, lung, liver.
Pain
Malignant Breast Lesions
Assessment.
Physical exam suspicion.
Self breast exam suspicion.
Mammogram X ray exam
Malignant Breast Lesions
Assessment.
Physical exam suspicion.
Self breast exam suspicion.
Mammogram X ray exam
Malignant Breast Lesions
Survival - increases with early diagnosis because size of
Malignant Breast Lesions
Survival - increases with early diagnosis because size of
Breast Abnormalities
Metastic malignancy of the breast - systemic involvement; breast changes
Breast Abnormalities
Metastic malignancy of the breast - systemic involvement; breast changes
BREAST CHANGES DURING PREGNANCY
BREAST CHANGES DURING PREGNANCY
Breasts in Pregnancy
Physical Findings -
Tenderness.
Increase in size and veins.
Nipples increase
Breasts in Pregnancy
Physical Findings -
Tenderness.
Increase in size and veins.
Nipples increase
Breasts in Pregnancy
Lactation.
Milk letdown in response to suckling or crying.
Requires adequate
Breasts in Pregnancy
Lactation.
Milk letdown in response to suckling or crying.
Requires adequate
Breasts in Pregnancy
Lactation.
Most drugs ingested are secreted.
Engorgement--manage with binder, ice, codeine.
Suppression--ice,
Breasts in Pregnancy
Lactation.
Most drugs ingested are secreted.
Engorgement--manage with binder, ice, codeine.
Suppression--ice,
Lactation
Agalactia - complete lack of milk, very rare.
Polygalactia - excess milk.
Lactation
Agalactia - complete lack of milk, very rare.
Polygalactia - excess milk.
SUMMARY
Evaluation and management of gynecologic infections and abnormalities require the ability
SUMMARY
Evaluation and management of gynecologic infections and abnormalities require the ability
SUMMARY
From that point, one must be able to categorize the problem
SUMMARY
From that point, one must be able to categorize the problem
SUMMARY
Knowing the key signs and symptoms for each of these categories
SUMMARY
Knowing the key signs and symptoms for each of these categories
QUESTIONS???
QUESTIONS???
 СПИД. ВИЧ-инфекция
СПИД. ВИЧ-инфекция Несахарный диабет
Несахарный диабет Походная медицина
Походная медицина Неврозы и неврозоподобные состояния
Неврозы и неврозоподобные состояния Детский церебральный паралич
Детский церебральный паралич Переломы костей плеча
Переломы костей плеча Медико-профилактические аспекты близорукости у детей школьного возраста
Медико-профилактические аспекты близорукости у детей школьного возраста Сучасні моделі ендоскопів, інструментарію і допоміжного обладнання
Сучасні моделі ендоскопів, інструментарію і допоміжного обладнання Туберкулез костей и суставов
Туберкулез костей и суставов Hormones. Régulation du métabolisme
Hormones. Régulation du métabolisme Безопасность гемотрансфузии и гемокоррекции в педиатрической практике
Безопасность гемотрансфузии и гемокоррекции в педиатрической практике Лабораторная диагностика (ВОЗ)
Лабораторная диагностика (ВОЗ) Особенности аппаратной чистки лица
Особенности аппаратной чистки лица Общие основы массажа
Общие основы массажа Пульпиты. Классификация
Пульпиты. Классификация Шаншаров-фарм жшс кәсіпорынында сасықшөп тұндырмасы өндіріс үрдісін қарқындату
Шаншаров-фарм жшс кәсіпорынында сасықшөп тұндырмасы өндіріс үрдісін қарқындату Внутриутробное развитие организма. Развитие после рождения
Внутриутробное развитие организма. Развитие после рождения Грипп: этиология, эпидемиология, клиника, лечение
Грипп: этиология, эпидемиология, клиника, лечение Наследственные болезни человека
Наследственные болезни человека Заболевания пищеварительной системы
Заболевания пищеварительной системы Научно – обоснованная медицинская практика. Поиск доказательной информации. Базы данных
Научно – обоснованная медицинская практика. Поиск доказательной информации. Базы данных Неотложная медицинская помощь и лечение при астматическом статусе
Неотложная медицинская помощь и лечение при астматическом статусе Сибирская язва
Сибирская язва Лекарственные растения и сырье, содержащие жиры и жироподобные вещества. (Лекция 6)
Лекарственные растения и сырье, содержащие жиры и жироподобные вещества. (Лекция 6) Период грудного возраста
Период грудного возраста Белый порок сердца
Белый порок сердца Лабораторная диагностика стафилококковой инфекции
Лабораторная диагностика стафилококковой инфекции Понятие стресс. Фазы стресса. Схема развития стресс-реакции
Понятие стресс. Фазы стресса. Схема развития стресс-реакции