- Lecture pulp and periapical disease

Содержание
- 2. PULPITIS Pulpitis is the most common cause of pain and loss of teeth in younger persons.
- 3. CAUSES OF PULP DISEASE The causes of pulp disease are Physical, Chemical and Bacterial. Physical Mechanical
- 4. 2. Chemical -Phosphoric acid, acrylic monomer, etc. -Erosion (acids) 3. Bacterial -Toxin associated with caries -Direct
- 5. I. According to pathological condition: - Focal or acute reversible pulpitis (Pulp hyperaemia) Irreversible pulpitis II.
- 6. According to extension of inflammation in pulp tissue: - Partial pulpitis Complete / total pulpitis According
- 7. Pulp state
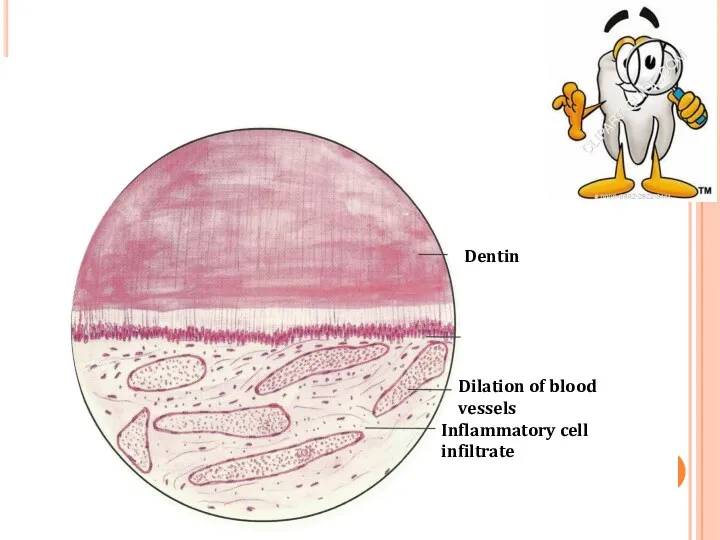
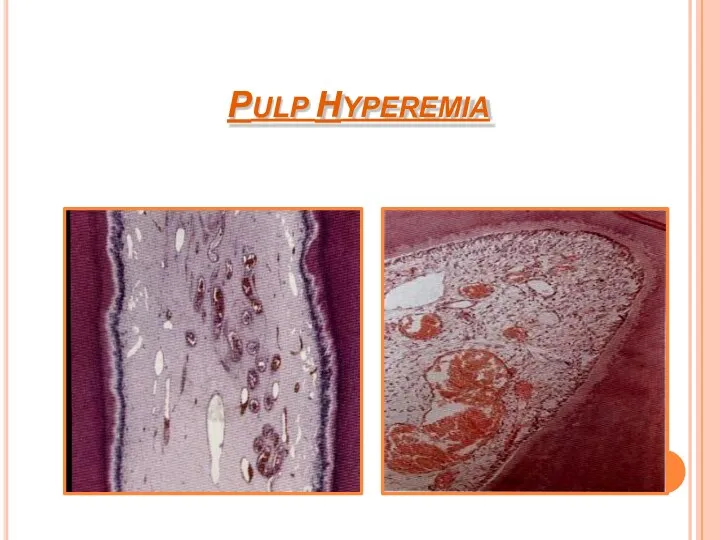
- 8. FOCAL REVERSIBLE PULPITIS (PULP HYPEREMIA) Mild, transient, localized inflammatory response. It is a reversible condition .
- 9. HISTOLOGICAL FEATURES: Dilation of pulp blood vessels. Edema fluid collection due to damage of vessel wall
- 10. Dilation of blood vessels Inflammatory cell infiltrate Dentin
- 11. PULP HYPEREMIA
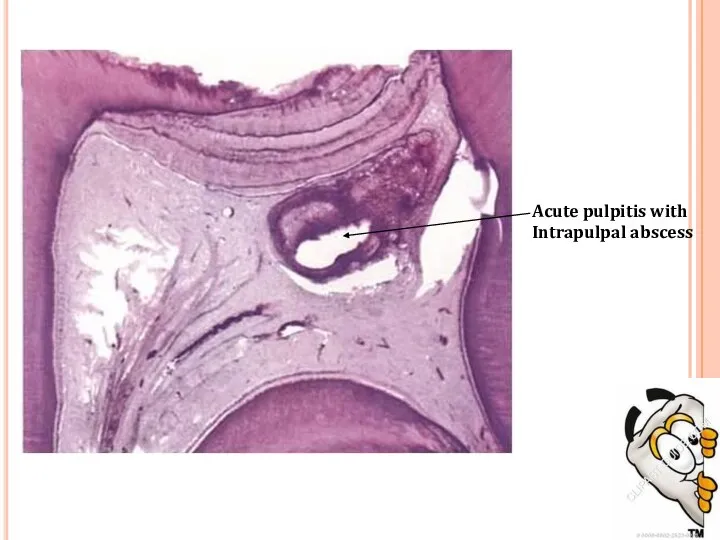
- 12. ACUTE PULPITIS Irreversible condition characterized by acute, intense inflammatory response in pulp. It is a frequent
- 13. Acute pulpitis with Intrapulpal abscess
- 14. Pulp vitality test indicates increased sensitivity at low level of current. Pulpal pain is due to:
- 15. HISTOLOGIC FEATURES: Edema in pulp with vasodilation. Infiltration of polymorphonuclear leukocytes along vascular channels & migrate
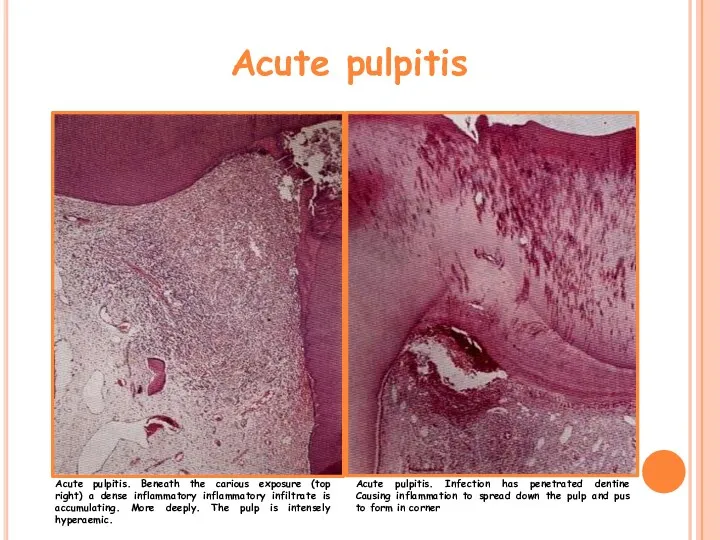
- 16. Acute pulpitis Acute pulpitis. Beneath the carious exposure (top right) a dense inflammatory inflammatory infiltrate is
- 17. Acute pulpitis stage. The entire pulp has been destroyed and replaced by inflammatory cells and dilated
- 18. Acute PULPITIS
- 19. Pulp abscess
- 20. Pulp abscess
- 21. TREATMENT & PROGNOSIS: Options for management: ◊ Extraction ◊ Pulpectomy and root canal treatment—with the following
- 22. Chronic Pulpitis Persistent inflammatory reaction in pulp with little or non symptoms. It can arise from
- 23. HISTOLOGIC FEATURES: Infiltration of mononuclear cells, lymphocytes & plasma cells, with vigorous connective tissue reaction. Capillaries
- 24. Chronic Pulpitis
- 25. TREATMENT & PROGNOSIS: Root canal therapy Extraction of tooth.
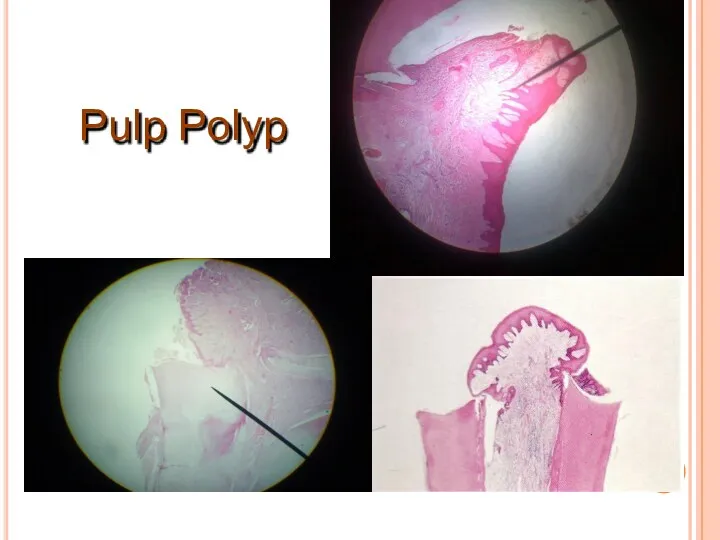
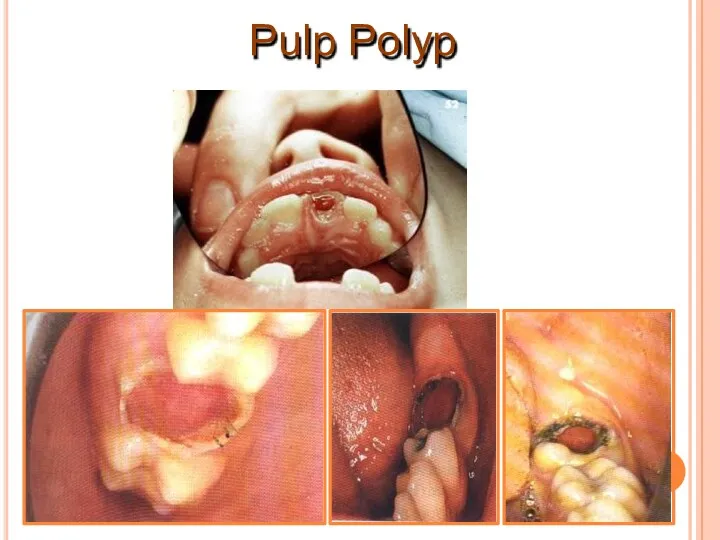
- 26. Chronic Hyperplastic Pulpitis (pulp polyp) It is a form of a chronic pulp disease. Overgrowth of
- 27. Lesion bleeds profusely upon provocation. Due to excellent blood supply high tissue resistance & reactivity in
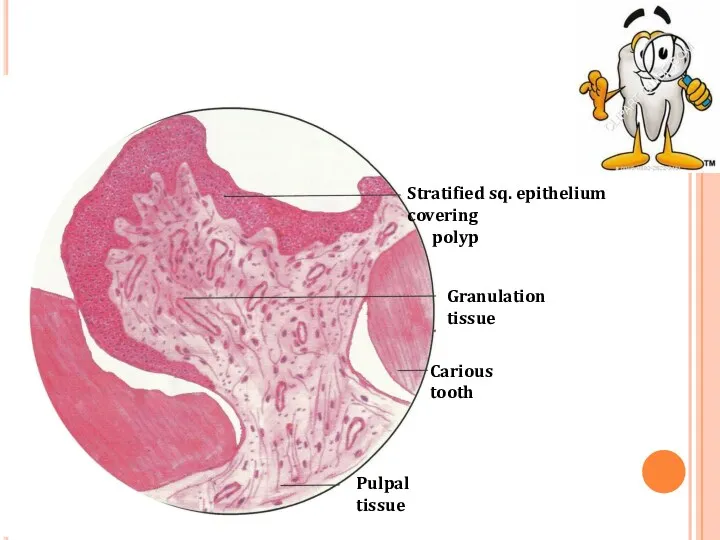
- 28. Pulpal tissue Stratified sq. epithelium covering polyp Granulation tissue Carious tooth
- 29. Stratified squamous type epithelial lining resembles oral mucosa with well formed rete pegs. Grafted epithelial cells
- 30. Pulp Polyp
- 31. Pulp Polyp
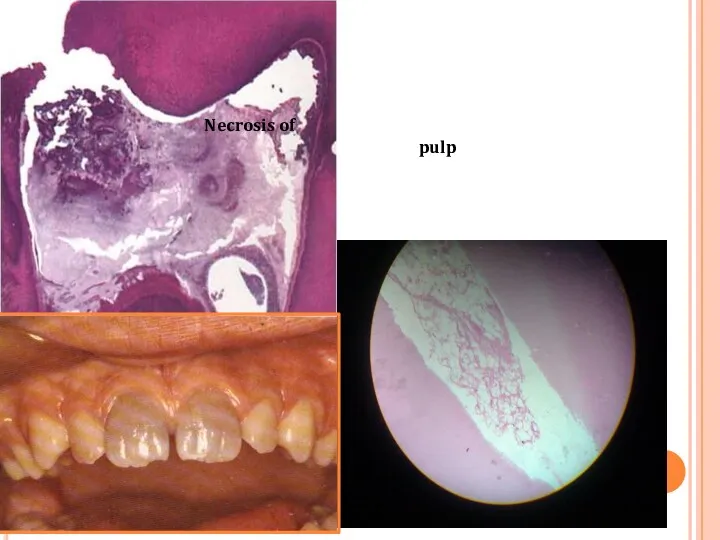
- 32. Untreated pulpitis results complete necrosis of pulp. As this is associated with bacterial infection – pulp
- 33. Necrosis of pulp
- 34. REVERSIBLE PULPITIS condition. Nature of pain is mild & diffuse. Brief duration & can be produce
- 35. DISEASES OF PERIAPICAL TISSUES
- 36. Inflammation of PDL around apical portion of root. Cause:1. spread of infection following pulp necrosis,2. occlusal
- 37. Pulpitis Acute chronic Apical peiodontitis Acute chronic Periapical abscess Acute chronic Periapical granuloma Periodontal cyst Periosteitis
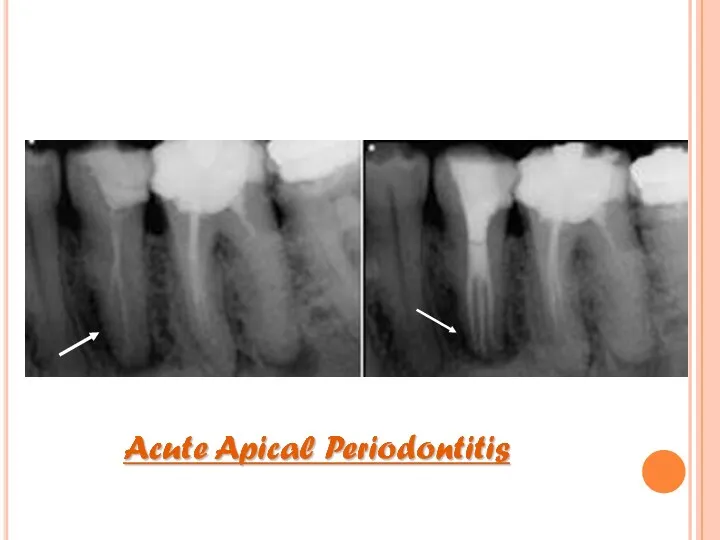
- 38. CLINICAL FEATURES: Thermal changes does not induce pain. Slight extrusion of tooth from socket. Cause tenderness
- 40. HISTOLOGIC FEATURES: PDL shows signs of inflammation -vascular dilation -infiltration of PMNs Inflammation is transient, if
- 41. Chronic Apical Periodontitis (Periapical Granuloma) Most common sequelae of pulpitis or apical periodontitis. If acute (exudative)
- 42. Mild pain on chewing on solid food. Tooth may be slightly elongated in socket. Sensitivity is
- 43. Periapical Granuloma
- 44. Thin radiopaque line or zone of sclerotic bone sometimes seen outlining lesion. Long standing lesion may
- 45. Periapical Granuloma
- 46. Cholesterol clefts
- 47. Collection of cholesterol clefts, with multinuclear gaint cells. Epithelial rests of Malassez may proliferate in response
- 48. Root Apex Granulation Tissue Periapical Granuloma
- 49. The granuloma may continue to enlarge and be associated with resorption of the bone and root
- 50. pulp necrosis, Cause due to – pulp infection, traumatic injury irritation of periapical tissues ( endo
- 51. Periapical abscess
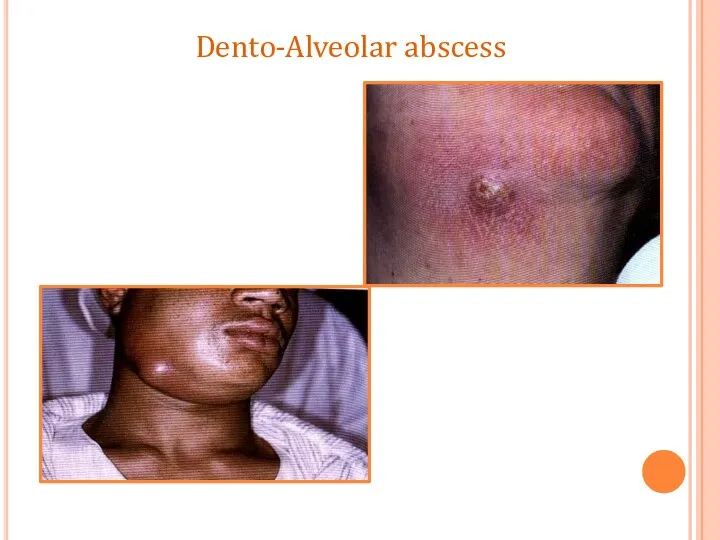
- 53. The pus tends to track through the cancellous bone and eventually perforates the cortex, it becomes
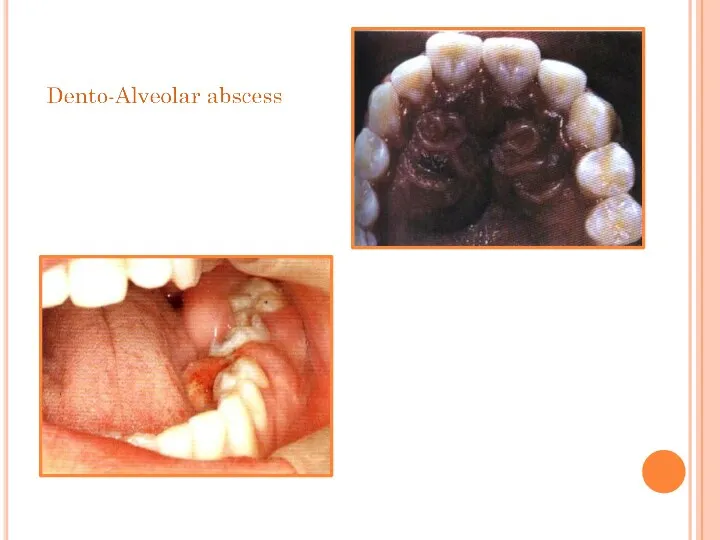
- 54. Dento-Alveolar abscess
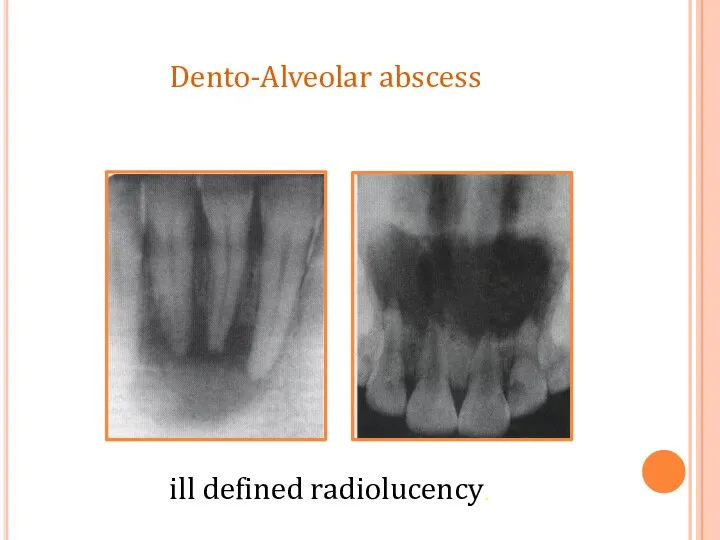
- 55. ill defined radiolucency. Dento-Alveolar abscess
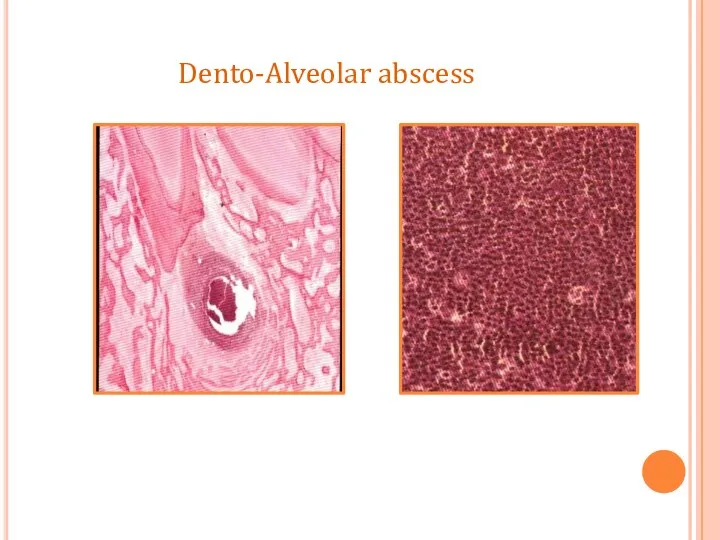
- 56. Dento-Alveolar abscess
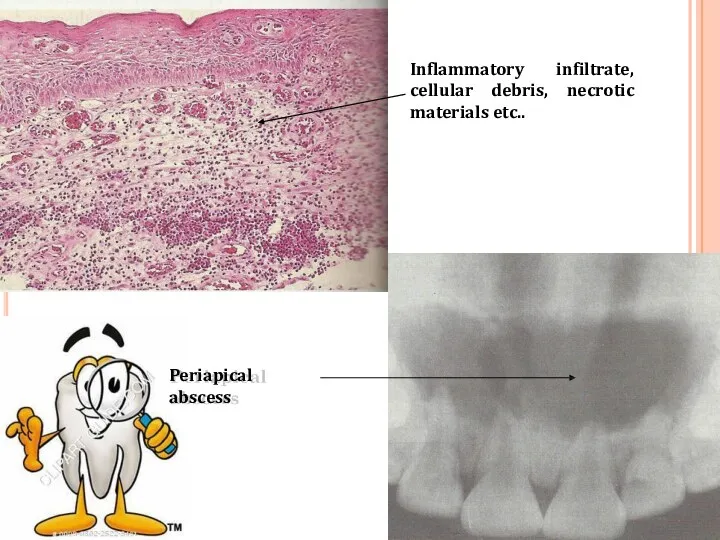
- 57. Periapical abscess Inflammatory infiltrate, cellular debris, necrotic materials etc..
- 58. The abscess cavity is surrounded by acute inflammatory cell and few chronic inflammatory cells. Dilation of
- 59. Abscess may spread along path of least resistance through medullary spaces resulting in Osteomyelitis. Can also
- 60. COMPLICATIONS Facial Cellulitis Ludwig's angina Osteomyelitis Septicaemia Menengitis, brain abscess, cavernous sinus thrombosis
- 61. It is a rapidly spreading inflammation of the soft tissues characterized by diffuse pus formation, usually
- 62. Two especially dangerous forms of cellulitis are:- cellulitis associated with mandibular teeth into submandibular and cervical
- 63. LUDWIG’S ANGINA Cellulitis of submandibular region involving sublingual, submandibular and submental spaces. In 70% cases develops
- 64. CLINICAL FEATURES It produces a broad –like swelling of the floor of the mouth . Involvement
- 65. Lateral pharyngeal space involvement may cause respiratory obstruction due to laryngeal edema(suffocation). In sever cases –
- 66. CAVERNOUS SINUS THROMBOSIS The infection from the posterior maxillary teeth reach the orbit via the maxillary
- 67. CLINICAL FEATURES Periorbital edema including lateral border of nose, protrusion and fixation of eyeball. Pupil dilatation,
- 68. Treatment High dose of penicillin. Extraction and drainage(if fluctuant). Corticosteroid and anticoagulant to prevent thrombosis and
- 70. Скачать презентацию
PULPITIS
Pulpitis is the most common cause of pain and loss of
PULPITIS
Pulpitis is the most common cause of pain and loss of
CAUSES OF PULP DISEASE
The causes of pulp disease are Physical, Chemical
CAUSES OF PULP DISEASE
The causes of pulp disease are Physical, Chemical
2. Chemical
-Phosphoric acid, acrylic monomer, etc.
-Erosion (acids)
3. Bacterial
-Toxin associated with caries
-Direct
2. Chemical
-Phosphoric acid, acrylic monomer, etc.
-Erosion (acids)
3. Bacterial
-Toxin associated with caries
-Direct
I. According to pathological condition: -
Focal or acute reversible pulpitis (Pulp hyperaemia)
Irreversible pulpitis
II.
I. According to pathological condition: -
Focal or acute reversible pulpitis (Pulp hyperaemia)
Irreversible pulpitis
II.
According to extension of inflammation in pulp tissue: -
Partial pulpitis
Complete /
According to extension of inflammation in pulp tissue: -
Partial pulpitis
Complete /
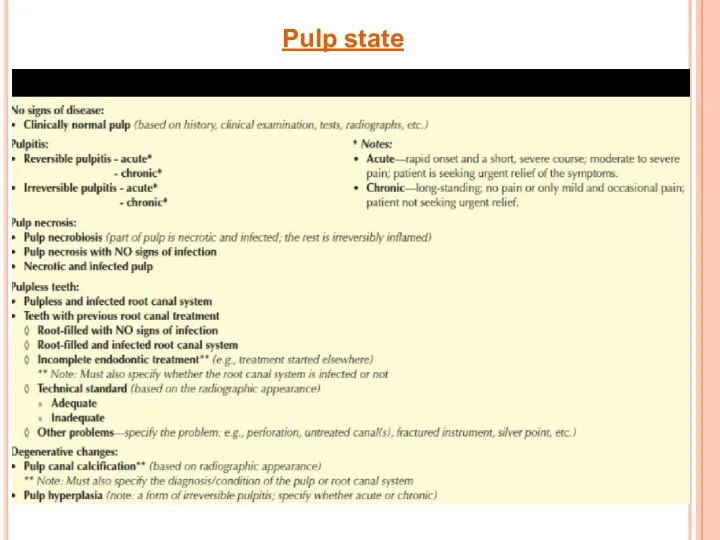
Pulp state
Pulp state
FOCAL REVERSIBLE PULPITIS (PULP HYPEREMIA)
Mild, transient, localized inflammatory response.
It is a
FOCAL REVERSIBLE PULPITIS (PULP HYPEREMIA)
Mild, transient, localized inflammatory response.
It is a
HISTOLOGICAL FEATURES:
Dilation of pulp blood vessels.
Edema fluid collection due to damage
HISTOLOGICAL FEATURES:
Dilation of pulp blood vessels.
Edema fluid collection due to damage
Dilation of blood vessels
Inflammatory cell
infiltrate
Dentin
Dilation of blood vessels
Inflammatory cell
infiltrate
Dentin
PULP HYPEREMIA
PULP HYPEREMIA
ACUTE PULPITIS
Irreversible condition characterized by acute, intense
inflammatory response in pulp.
It is
ACUTE PULPITIS
Irreversible condition characterized by acute, intense
inflammatory response in pulp.
It is
Acute pulpitis with Intrapulpal abscess
Acute pulpitis with Intrapulpal abscess
Pulp vitality test indicates increased sensitivity at low level of current.
Pulpal
Pulp vitality test indicates increased sensitivity at low level of current.
Pulpal
HISTOLOGIC FEATURES:
Edema in pulp with vasodilation.
Infiltration of polymorphonuclear leukocytes along vascular
HISTOLOGIC FEATURES:
Edema in pulp with vasodilation.
Infiltration of polymorphonuclear leukocytes along vascular
Acute pulpitis
Acute pulpitis. Beneath the carious exposure (top right) a dense
Acute pulpitis
Acute pulpitis. Beneath the carious exposure (top right) a dense
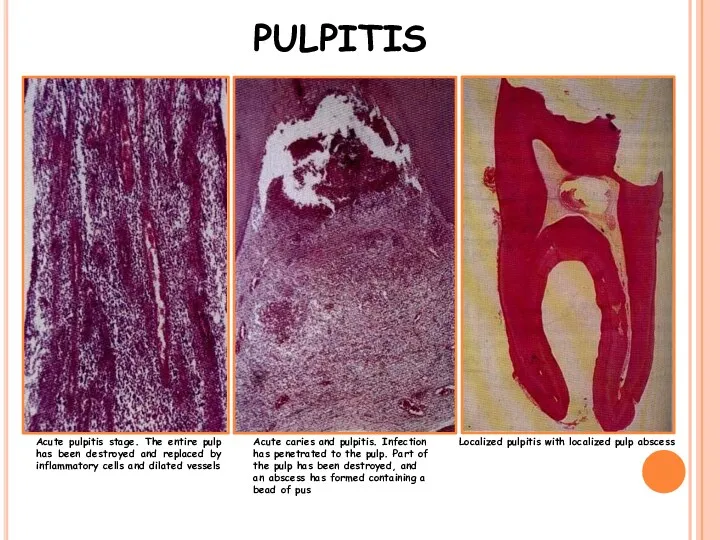
Acute pulpitis stage. The entire pulp has been destroyed and replaced
Acute pulpitis stage. The entire pulp has been destroyed and replaced
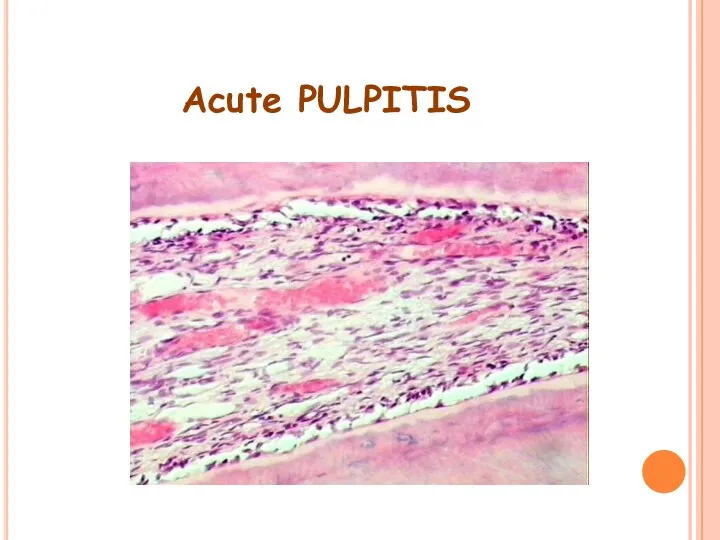
Acute PULPITIS
Acute PULPITIS
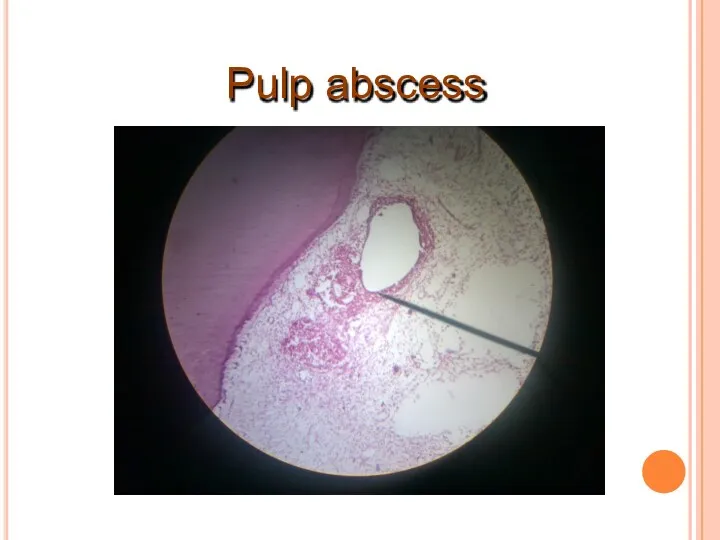
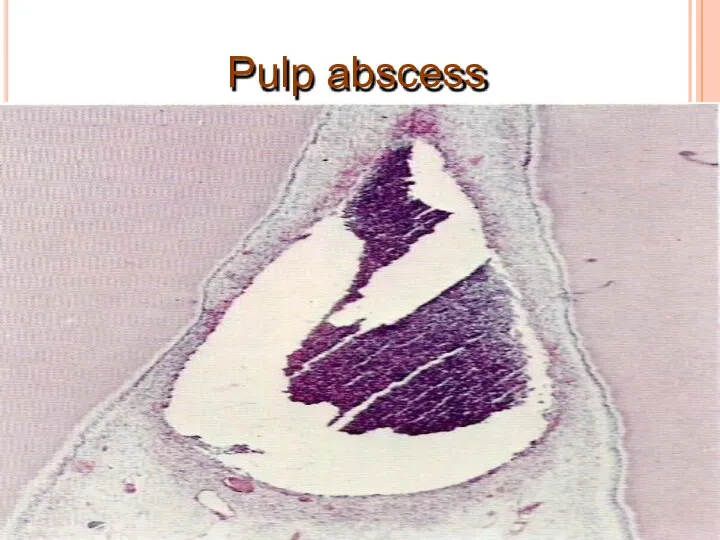
Pulp abscess
Pulp abscess
Pulp abscess
Pulp abscess
TREATMENT & PROGNOSIS:
Options for management:
◊ Extraction
◊ Pulpectomy and root canal treatment—with
TREATMENT & PROGNOSIS:
Options for management:
◊ Extraction
◊ Pulpectomy and root canal treatment—with
Chronic Pulpitis
Persistent inflammatory reaction in pulp with little or non symptoms.
It
Chronic Pulpitis
Persistent inflammatory reaction in pulp with little or non symptoms.
It
HISTOLOGIC FEATURES:
Infiltration of mononuclear cells, lymphocytes & plasma cells, with vigorous
HISTOLOGIC FEATURES:
Infiltration of mononuclear cells, lymphocytes & plasma cells, with vigorous
Chronic Pulpitis
Chronic Pulpitis
TREATMENT & PROGNOSIS:
Root canal therapy
Extraction of tooth.
TREATMENT & PROGNOSIS:
Root canal therapy
Extraction of tooth.
Chronic Hyperplastic Pulpitis (pulp polyp)
It is a form of a chronic pulp
Chronic Hyperplastic Pulpitis (pulp polyp)
It is a form of a chronic pulp
Lesion bleeds profusely upon provocation.
Due to excellent blood supply high tissue
Lesion bleeds profusely upon provocation.
Due to excellent blood supply high tissue
Pulpal tissue
Stratified sq. epithelium covering
polyp
Granulation tissue
Carious tooth
Pulpal tissue
Stratified sq. epithelium covering
polyp
Granulation tissue
Carious tooth
Stratified squamous type epithelial lining resembles oral mucosa with well formed
Stratified squamous type epithelial lining resembles oral mucosa with well formed
Pulp Polyp
Pulp Polyp
Pulp Polyp
Pulp Polyp
Untreated pulpitis results complete necrosis of pulp.
As this is associated with bacterial
Untreated pulpitis results complete necrosis of pulp.
As this is associated with bacterial
Necrosis of
pulp
Necrosis of
pulp
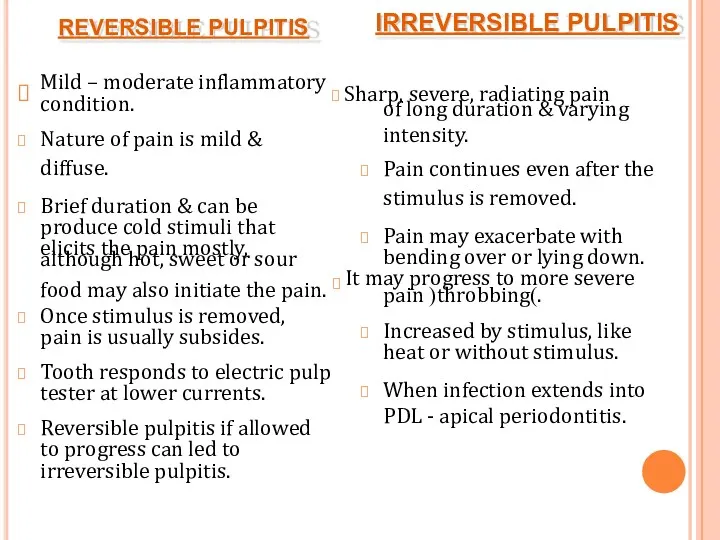
REVERSIBLE PULPITIS
condition.
Nature of pain is mild &
diffuse.
Brief duration & can be
REVERSIBLE PULPITIS
condition.
Nature of pain is mild &
diffuse.
Brief duration & can be
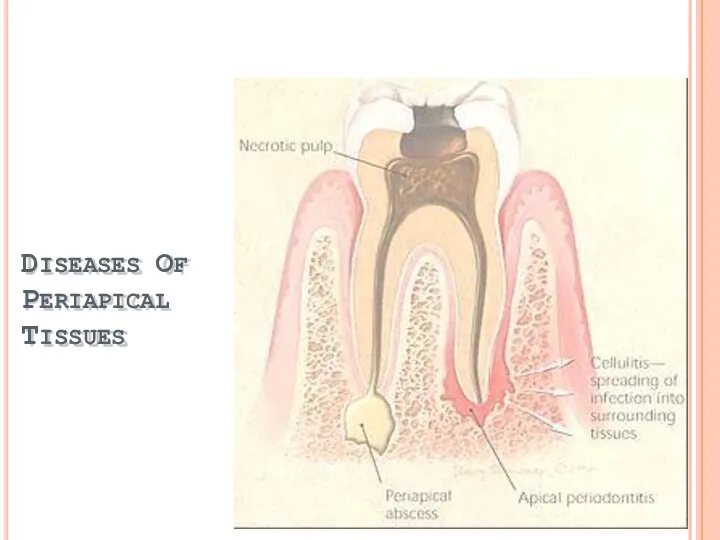
DISEASES OF PERIAPICAL TISSUES
DISEASES OF PERIAPICAL TISSUES
Inflammation of PDL around apical portion of root.
Cause:1. spread of infection
Inflammation of PDL around apical portion of root.
Cause:1. spread of infection
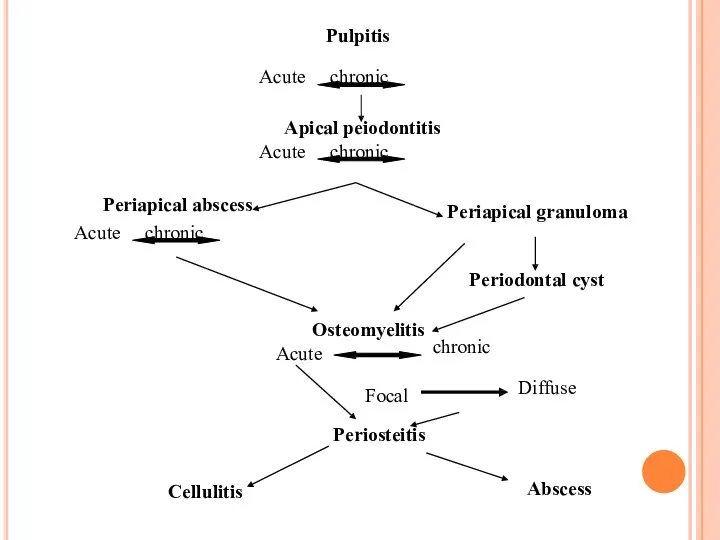
Pulpitis
Acute chronic
Apical peiodontitis
Acute chronic
Periapical abscess
Acute chronic
Periapical granuloma
Periodontal cyst
Periosteitis
Cellulitis
Abscess
chronic
Osteomyelitis
Acute
Focal
Diffuse
Pulpitis
Acute chronic
Apical peiodontitis
Acute chronic
Periapical abscess
Acute chronic
Periapical granuloma
Periodontal cyst
Periosteitis
Cellulitis
Abscess
chronic
Osteomyelitis
Acute
Focal
Diffuse
CLINICAL FEATURES:
Thermal changes does not induce pain.
Slight extrusion of tooth from
CLINICAL FEATURES:
Thermal changes does not induce pain.
Slight extrusion of tooth from
HISTOLOGIC FEATURES:
PDL shows signs of inflammation -vascular dilation
-infiltration of PMNs
Inflammation is
HISTOLOGIC FEATURES:
PDL shows signs of inflammation -vascular dilation
-infiltration of PMNs
Inflammation is
Chronic Apical Periodontitis
(Periapical Granuloma)
Most common sequelae of pulpitis or apical periodontitis.
If
Chronic Apical Periodontitis
(Periapical Granuloma)
Most common sequelae of pulpitis or apical periodontitis.
If
Mild pain on chewing on solid food.
Tooth may be slightly elongated
Mild pain on chewing on solid food.
Tooth may be slightly elongated
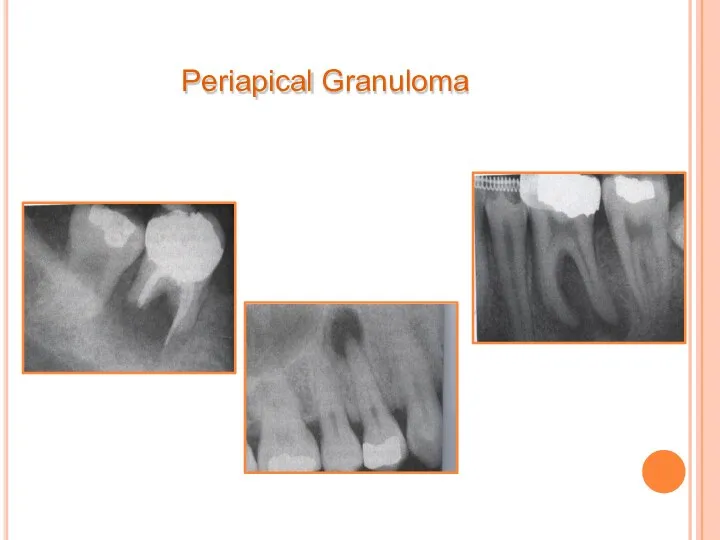
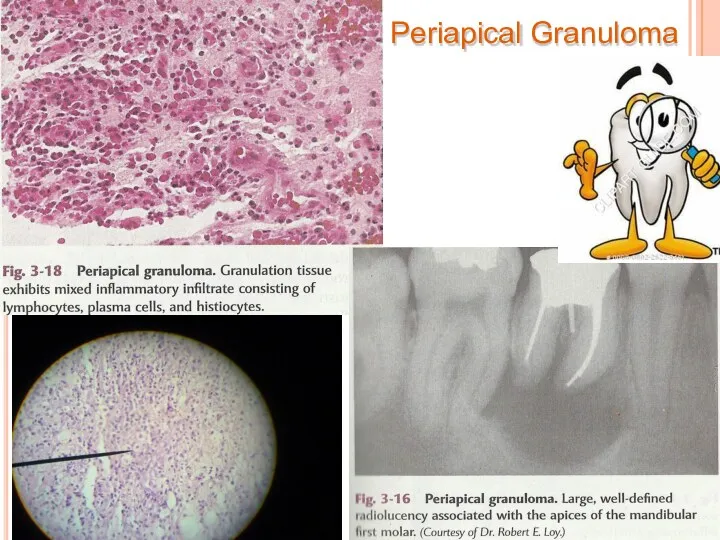
Periapical Granuloma
Periapical Granuloma
Thin radiopaque line or zone of sclerotic bone sometimes seen outlining
Thin radiopaque line or zone of sclerotic bone sometimes seen outlining
Periapical Granuloma
Periapical Granuloma
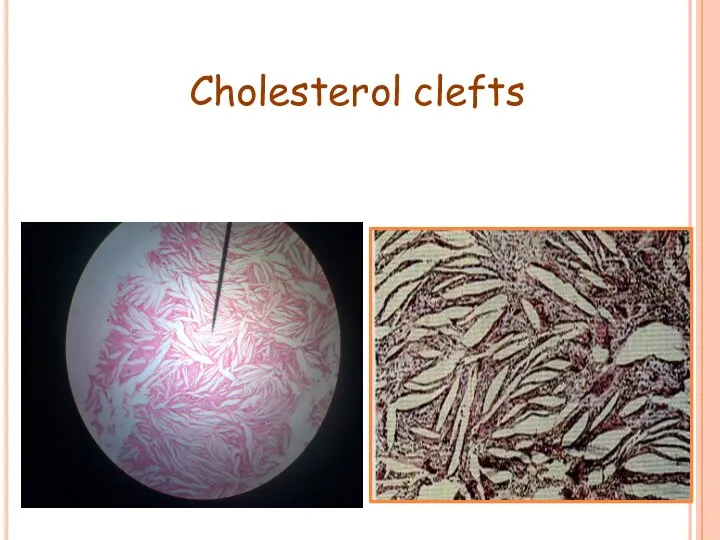
Cholesterol clefts
Cholesterol clefts
Collection of cholesterol clefts, with multinuclear gaint cells.
Epithelial rests of Malassez
Collection of cholesterol clefts, with multinuclear gaint cells.
Epithelial rests of Malassez
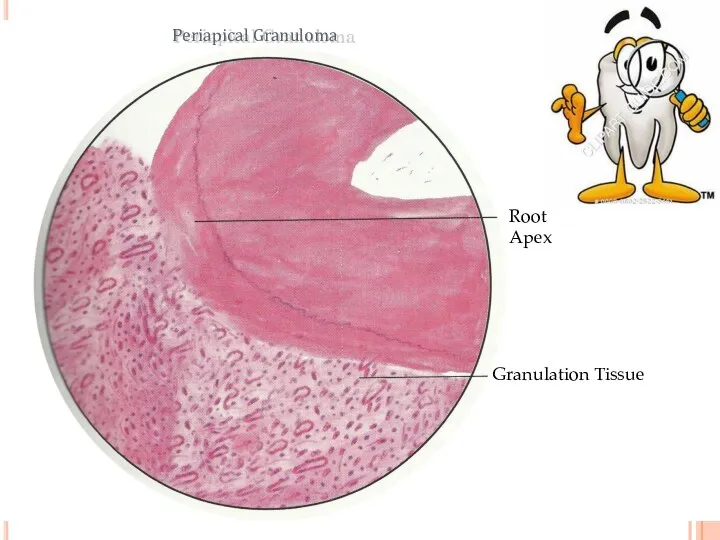
Root Apex
Granulation Tissue
Periapical Granuloma
Root Apex
Granulation Tissue
Periapical Granuloma
The granuloma may continue to enlarge and be associated with resorption
The granuloma may continue to enlarge and be associated with resorption
pulp necrosis,
Cause due to – pulp infection, traumatic injury irritation of
pulp necrosis,
Cause due to – pulp infection, traumatic injury irritation of
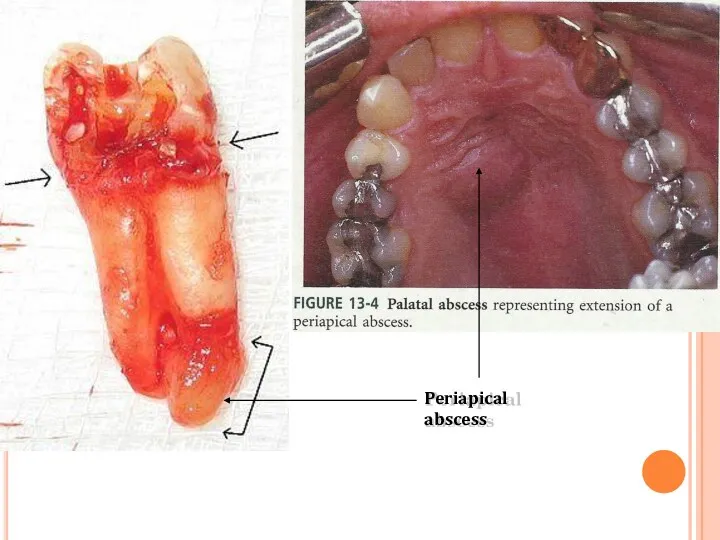
Periapical abscess
Periapical abscess
The pus tends to track through the cancellous bone and eventually
The pus tends to track through the cancellous bone and eventually
Dento-Alveolar abscess
Dento-Alveolar abscess
ill defined radiolucency.
Dento-Alveolar abscess
ill defined radiolucency.
Dento-Alveolar abscess
Dento-Alveolar abscess
Dento-Alveolar abscess
Periapical abscess
Inflammatory infiltrate, cellular debris, necrotic materials etc..
Periapical abscess
Inflammatory infiltrate, cellular debris, necrotic materials etc..
The abscess cavity is surrounded by acute inflammatory cell and few
The abscess cavity is surrounded by acute inflammatory cell and few
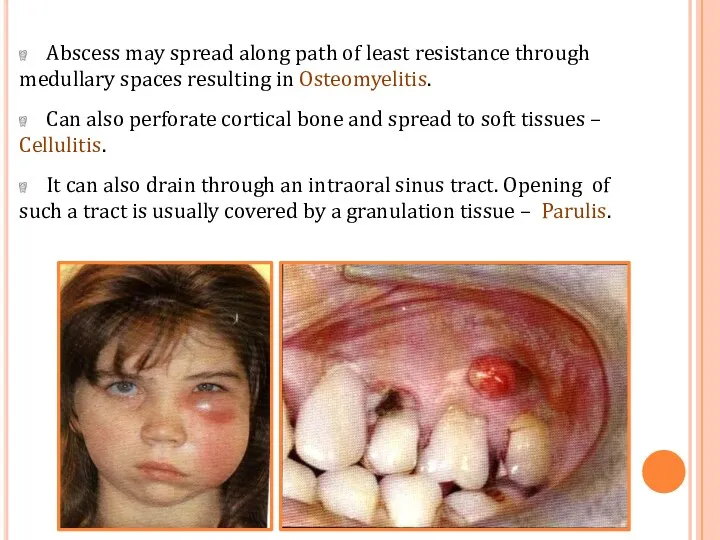
Abscess may spread along path of least resistance through medullary spaces
Abscess may spread along path of least resistance through medullary spaces
COMPLICATIONS
Facial Cellulitis
Ludwig's angina
Osteomyelitis
Septicaemia
Menengitis, brain abscess, cavernous sinus thrombosis
COMPLICATIONS
Facial Cellulitis
Ludwig's angina
Osteomyelitis
Septicaemia
Menengitis, brain abscess, cavernous sinus thrombosis
It is a rapidly spreading inflammation of the soft tissues characterized
It is a rapidly spreading inflammation of the soft tissues characterized
Two especially dangerous forms of cellulitis are:-
cellulitis associated with mandibular teeth
Two especially dangerous forms of cellulitis are:-
cellulitis associated with mandibular teeth
LUDWIG’S ANGINA
Cellulitis of submandibular region involving sublingual, submandibular and submental spaces.
In
LUDWIG’S ANGINA
Cellulitis of submandibular region involving sublingual, submandibular and submental spaces.
In
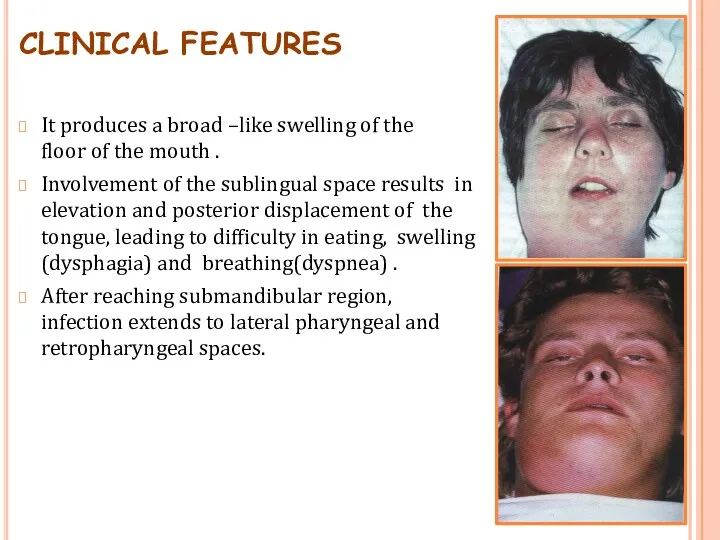
CLINICAL FEATURES
It produces a broad –like swelling of the floor of
CLINICAL FEATURES
It produces a broad –like swelling of the floor of
Lateral pharyngeal space involvement may cause respiratory obstruction due to laryngeal
Lateral pharyngeal space involvement may cause respiratory obstruction due to laryngeal
CAVERNOUS SINUS THROMBOSIS
The infection from the posterior maxillary teeth reach the
CAVERNOUS SINUS THROMBOSIS
The infection from the posterior maxillary teeth reach the
CLINICAL FEATURES
Periorbital edema including lateral border of nose, protrusion and fixation
CLINICAL FEATURES
Periorbital edema including lateral border of nose, protrusion and fixation
Treatment
High dose of penicillin.
Extraction and drainage(if fluctuant).
Corticosteroid and anticoagulant to prevent
Treatment
High dose of penicillin.
Extraction and drainage(if fluctuant).
Corticosteroid and anticoagulant to prevent
 Аппендициттің асқынулары
Аппендициттің асқынулары Здоровье и гигиена. Рекомендательный список литературы для родителей
Здоровье и гигиена. Рекомендательный список литературы для родителей Бронхо-обструктивный синдром у детей
Бронхо-обструктивный синдром у детей Мифы о питании
Мифы о питании Философия и принципы паллиативной помощи Palliative Care
Философия и принципы паллиативной помощи Palliative Care Гастроэзофагеальная рефлюксная болезнь
Гастроэзофагеальная рефлюксная болезнь Таңдама әдісі Кездеймоқ шамалардың негізгі статистикалық сипаттамалары
Таңдама әдісі Кездеймоқ шамалардың негізгі статистикалық сипаттамалары Болевой синдром. Медикаментозное лечение
Болевой синдром. Медикаментозное лечение Особо опасные инфекции. Холера. Чума. Геморрагические лихорадки
Особо опасные инфекции. Холера. Чума. Геморрагические лихорадки 1 грудня - Всесвітній день боротьби зі СНІДом
1 грудня - Всесвітній день боротьби зі СНІДом Фармакологическая регуляция гемостаза
Фармакологическая регуляция гемостаза Профессиональная бронхиальная астма
Профессиональная бронхиальная астма Перикардит
Перикардит Infectious diseases
Infectious diseases Поперечные методы исследования
Поперечные методы исследования Организация работы родильного дома, женской консультации
Организация работы родильного дома, женской консультации Физиологические основы формирования речевой функции
Физиологические основы формирования речевой функции Гемопоэз. Современные представления о кроветворении
Гемопоэз. Современные представления о кроветворении Всасывание лекарств
Всасывание лекарств Лекция Хир. пат. прямой кишки
Лекция Хир. пат. прямой кишки Операции при портальной гипертензии
Операции при портальной гипертензии Тромбоцитопенії, тромбоцитопатії у новонароджених. Діагностика, клініка, лікування
Тромбоцитопенії, тромбоцитопатії у новонароджених. Діагностика, клініка, лікування Определение групп крови
Определение групп крови Тірегі имплант болғанда тіс протездерін қалыптастыру ерекшеліктері
Тірегі имплант болғанда тіс протездерін қалыптастыру ерекшеліктері Листериялар. Морфология, физиология, листериялар антигені. Экологиясы. Әйелдер патологиясындағы маңызы
Листериялар. Морфология, физиология, листериялар антигені. Экологиясы. Әйелдер патологиясындағы маңызы Көмей обыры
Көмей обыры Высотная болезнь
Высотная болезнь Противоаритмические лекарственные средства
Противоаритмические лекарственные средства