- Lung cancer

Содержание
- 2. Lung cancer is the second most common malignancy Most lung carcinomas are diagnosed at an advanced
- 3. EPIDEMIOLOGY Incidence Lung cancer incidence is increased in urban areas The highest incidence in male is
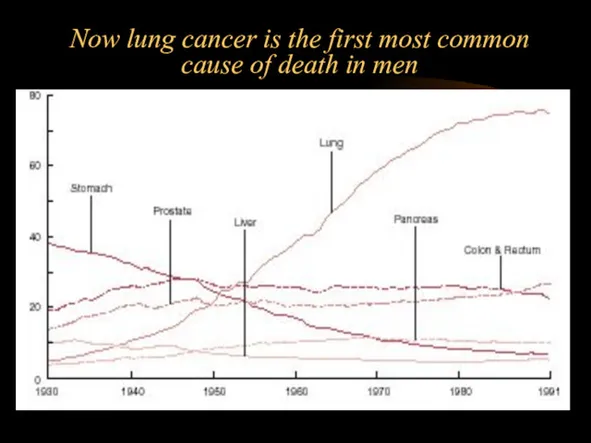
- 4. Now lung cancer is the first most common cause of death in men
- 5. EPIDEMIOLOGY Death rate The highest death rate in male is in Scotland (105,2), Belgium (104,1), and
- 6. EPIDEMIOLOGY Sex Lung cancer is more common in men than in women. The incidence of lung
- 7. EPIDEMIOLOGY Age The probabilities of developing lung cancer among males: from birth to 39 years, 0.04%;
- 8. EPIDEMIOLOGY Race Among men, the incidence of lung cancer ranges from 14 per 100,000 Americans, 42-53
- 9. There are two more common different morphological and clinical forms of lung cancer: 1) Non-Small-Cellular Lang
- 10. Small Cellular Lung Cancer (SCLC) Features: SCLC exhibits aggressive behavior, rapid growth, early spread to distant
- 11. Non–small cell lung cancer (NSCLC) Features: accounts for approximately 75-80% of all lung cancers. non–small cell
- 12. ETIOLOGY 1. Smoking The cause of lung cancer (LC) is tobacco smoking in as many as
- 13. ETIOLOGY 2. History of interstitial lung disease Concomitant chronic obstructive bronchitis, tuberculosis, pneumosclerosis and pneumoconiosis are
- 14. ETIOLOGY 4. Radon Approximately 2-3% of lung cancers annually are estimated to be caused by radon
- 15. ETIOLOGY 6. Other environmental agents Aromatic polycyclic hydrocarbons, chromium, and diesel exhaust all have been implicated
- 16. PATHOPHYSIOLOGY The base of pathogenesis of central lung cancer is the metaplasia of bronchial epithelium due
- 17. Tumors arise from a common mucosal, pleuripotential stem cell.
- 18. HISTOPATHOLOGY
- 19. HISTOPATHOLOGY SCLC classified into 3 subcategories: 1) oat cell carcinoma, 2) intermediate cell type, and 3)
- 20. Stage grouping for lung cancer Stage TNM ———————————————— IA T1N0M0 IB T2N0M0 IIA T1N1M0 IIB T2N1M0
- 21. CLINICAL MANIFESTATION Symptoms include the following: 1. Constitutional symptoms: fatigue, anorexia, weight loss. 2. Symptoms due
- 22. The symptoms and sighs depend on its location: (1) central form (2) peripheral (3) Pancoast cancer
- 23. 1. Central tumors diagnosed in 70-85% of all LC. Symptoms: cough, dyspnea, atelectasis, postobstructive pneumonia, wheezing,
- 24. 3. A Pancoast tumor is a rare form 1% that arises in the superior sulcus of
- 25. CLINICAL MANIFESTATION Symptoms due to intrathoracic spread: superior vena cava obstruction, hoarseness (ie, palsy of the
- 26. CLINICAL MANIFESTATION Symptoms due to distant spread: neurological dysfunction (ie, brain metastasis, spinal cord compression), bone
- 27. 4) Paraneoplastic syndromes by ectopic hormone production Squamous cell carcinomas are more likely to be associated
- 28. DIAGNOSTICS Diagnostic strategy: In the presence of a long history of smoking or other risk factors
- 29. DIAGNOSTICS Chest X-Ray (CXR) A chest radiograph is usually the first test ordered in patients. On
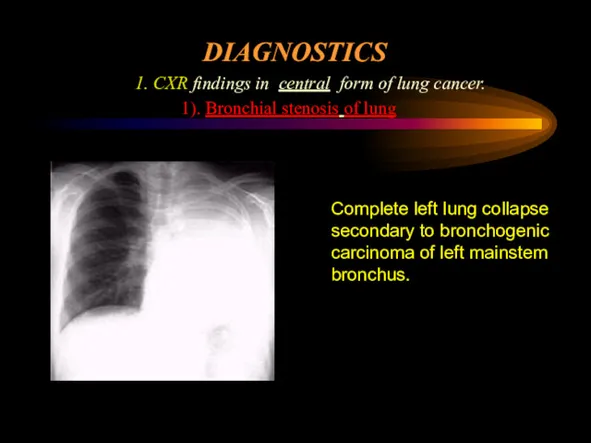
- 30. DIAGNOSTICS 1. CXR findings in central form of lung cancer. 1). Bronchial stenosis of lung Complete
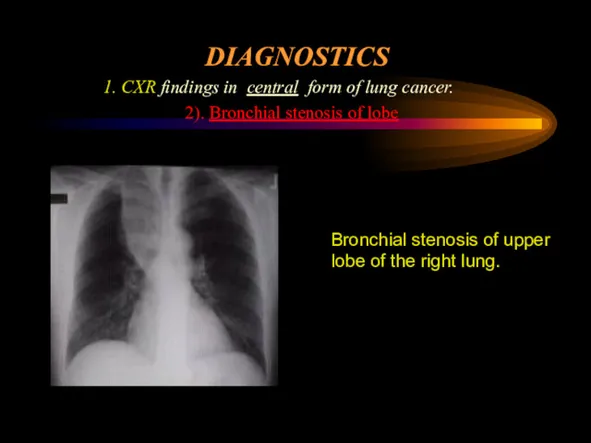
- 31. DIAGNOSTICS 1. CXR findings in central form of lung cancer. 2). Bronchial stenosis of lobe Bronchial
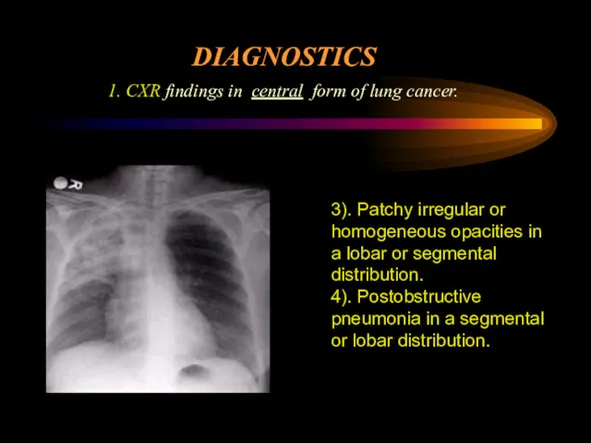
- 32. DIAGNOSTICS 1. CXR findings in central form of lung cancer. 3). Patchy irregular or homogeneous opacities
- 33. DIAGNOSTICS 1. CXR findings in central form of lung cancer. 5). Regional hyperlucency. Partial stenosis of
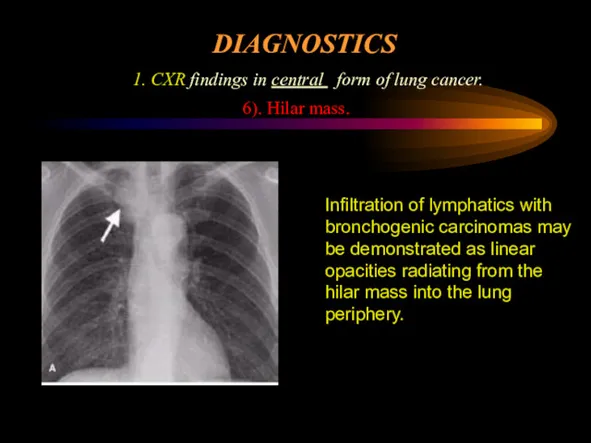
- 34. DIAGNOSTICS 1. CXR findings in central form of lung cancer. 6). Hilar mass. Infiltration of lymphatics
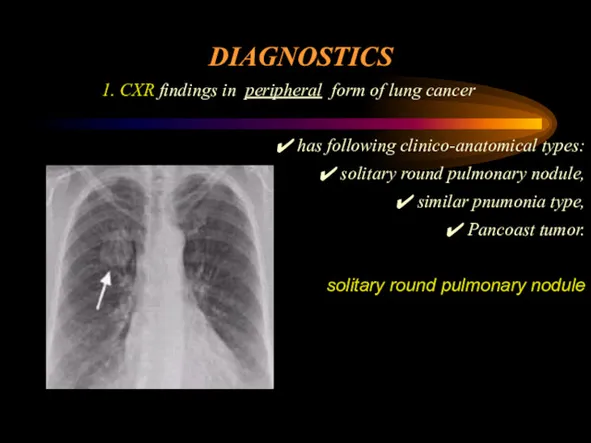
- 35. DIAGNOSTICS 1. CXR findings in peripheral form of lung cancer has following clinico-anatomical types: solitary round
- 36. DIAGNOSTICS 1. The CXR sings of nonresolving pneumonia may be occure both in central and peripheral
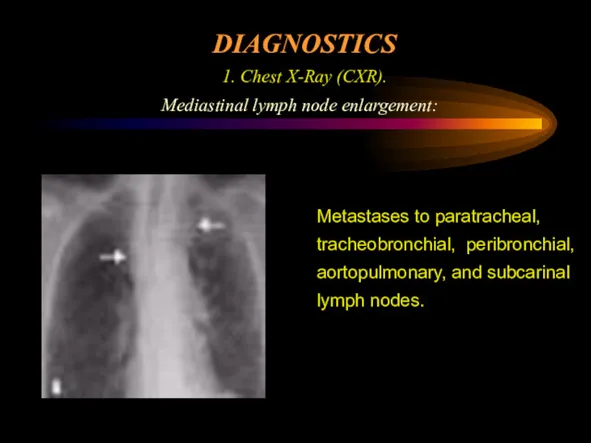
- 37. DIAGNOSTICS 1. Chest X-Ray (CXR). Mediastinal lymph node enlargement: Metastases to paratracheal, tracheobronchial, peribronchial, aortopulmonary, and
- 38. DIAGNOSTICS 2. Sputum cytologic studies. Sputum cytology can be a quick and inexpensive diagnostic test. Sputum
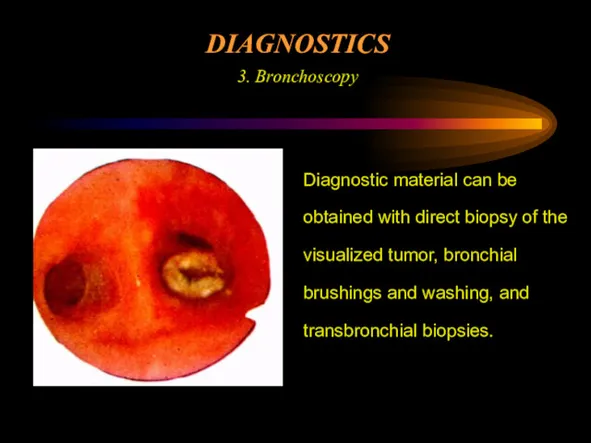
- 39. DIAGNOSTICS 3. Bronchoscopy Diagnostic material can be obtained with direct biopsy of the visualized tumor, bronchial
- 40. DIAGNOSTICS 4. Biopsy. is preferred for tumors located in the periphery of the lungs.
- 41. DIAGNOSTICS Staging workup 1. Ultrasaund or CT scan of the upper abdomen, including liver and adrenals
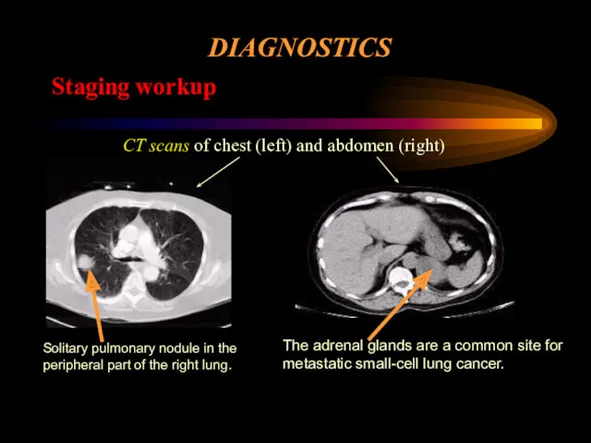
- 42. DIAGNOSTICS Staging workup CT scans of chest (left) and abdomen (right) Solitary pulmonary nodule in the
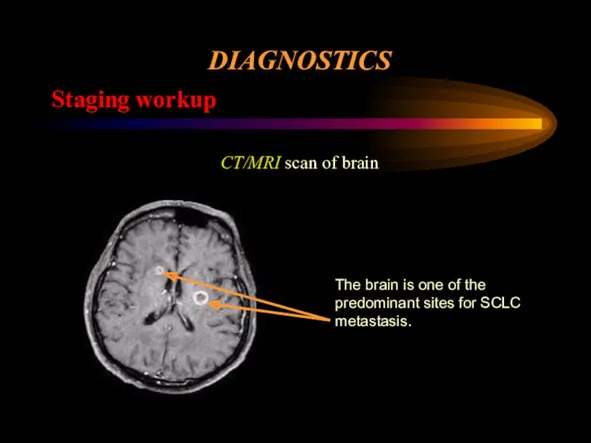
- 43. DIAGNOSTICS Staging workup CT/MRI scan of brain The brain is one of the predominant sites for
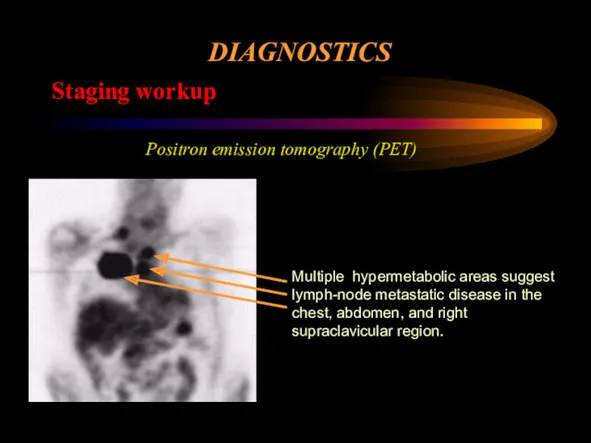
- 44. DIAGNOSTICS Staging workup Positron emission tomography (PET) Multiple hypermetabolic areas suggest lymph-node metastatic disease in the
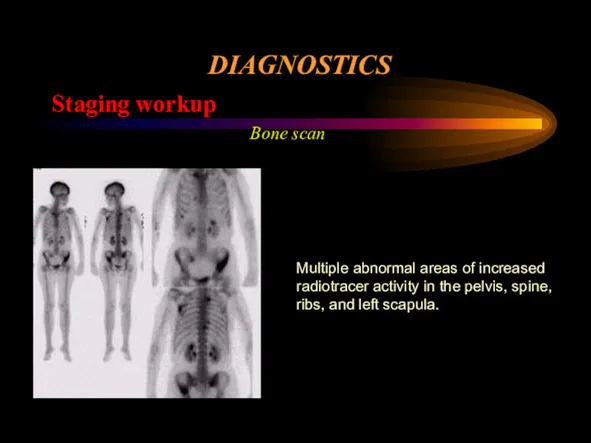
- 45. DIAGNOSTICS Staging workup Bone scan Multiple abnormal areas of increased radiotracer activity in the pelvis, spine,
- 46. DIAGNOSTICS Staging workup Thoracentesis. Pleural effusions should be aspirated and examined for malignant cells Bone marrow
- 47. DIFFERENTIAL DIAGNOSES Bronchogenic cyst Neurogenic tumors Teratodermoid tumor Thymoma Vascular aneurysm Esophageal lesions Lymphadenopathy from other
- 48. SURGICAL CARE Surgical resection provides the best chance of long-term disease-free survival and possibility of a
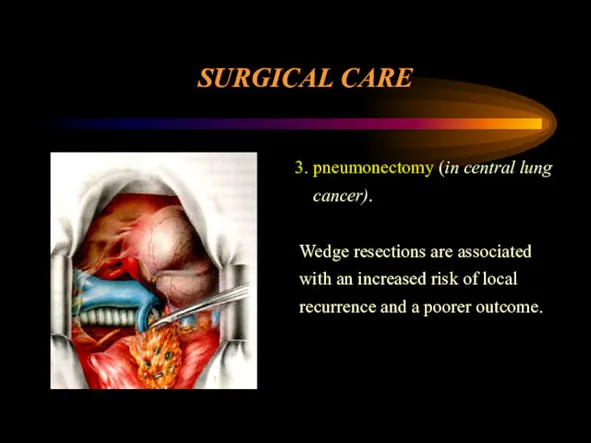
- 49. PRINCIPLES OF TREATMENT SURGICAL CARE 3. pneumonectomy (in central lung cancer). Wedge resections are associated with
- 50. CHEMOTHERAPY Alone has no role in potentially curative therapy. Is used alone in the palliative treatment
- 51. RADIATION THERAPY Reduces local failures in completely resected stages (II and IIIA) NSCLC But has not
- 52. PROGNOSIS Estimated 5-year survival rates are as follows: Stage IA - 75%; Stage IB - 55%;
- 54. Скачать презентацию
Lung cancer is the second most common malignancy
Most lung carcinomas
Lung cancer is the second most common malignancy
Most lung carcinomas
EPIDEMIOLOGY
Incidence
Lung cancer incidence is increased in urban areas
The highest
EPIDEMIOLOGY
Incidence
Lung cancer incidence is increased in urban areas
The highest
Now lung cancer is the first most common cause of death
Now lung cancer is the first most common cause of death
EPIDEMIOLOGY
Death rate
The highest death rate in male is in Scotland
EPIDEMIOLOGY
Death rate
The highest death rate in male is in Scotland
EPIDEMIOLOGY
Sex
Lung cancer is more common in men than
EPIDEMIOLOGY
Sex
Lung cancer is more common in men than
EPIDEMIOLOGY
Age
The probabilities of developing lung cancer
among males: from
EPIDEMIOLOGY
Age
The probabilities of developing lung cancer
among males: from
EPIDEMIOLOGY
Race
Among men, the incidence of lung cancer ranges from
EPIDEMIOLOGY
Race
Among men, the incidence of lung cancer ranges from
There are two more common different morphological and clinical forms of
Small Cellular Lung Cancer (SCLC)
Features:
SCLC exhibits aggressive behavior,
rapid growth,
early
Small Cellular Lung Cancer (SCLC)
Features:
SCLC exhibits aggressive behavior,
rapid growth,
early
Non–small cell lung cancer (NSCLC)
Features:
accounts for approximately 75-80% of
Features:
accounts for approximately 75-80% of
ETIOLOGY
1. Smoking
The cause of lung cancer (LC) is
ETIOLOGY
1. Smoking
The cause of lung cancer (LC) is
ETIOLOGY
2. History of interstitial lung disease
Concomitant chronic obstructive
ETIOLOGY
2. History of interstitial lung disease
Concomitant chronic obstructive
ETIOLOGY
4. Radon
Approximately 2-3% of lung cancers annually are
ETIOLOGY
4. Radon
Approximately 2-3% of lung cancers annually are
ETIOLOGY
6. Other environmental agents
Aromatic polycyclic hydrocarbons, chromium, and diesel exhaust
ETIOLOGY
6. Other environmental agents
Aromatic polycyclic hydrocarbons, chromium, and diesel exhaust
PATHOPHYSIOLOGY
The base of pathogenesis of central lung cancer is the
PATHOPHYSIOLOGY
The base of pathogenesis of central lung cancer is the
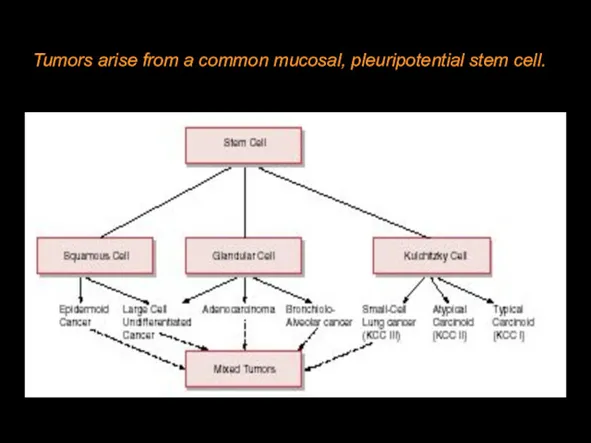
Tumors arise from a common mucosal, pleuripotential stem cell.
HISTOPATHOLOGY
HISTOPATHOLOGY
HISTOPATHOLOGY
SCLC classified into 3 subcategories: 1) oat cell carcinoma, 2) intermediate
HISTOPATHOLOGY
SCLC classified into 3 subcategories: 1) oat cell carcinoma, 2) intermediate
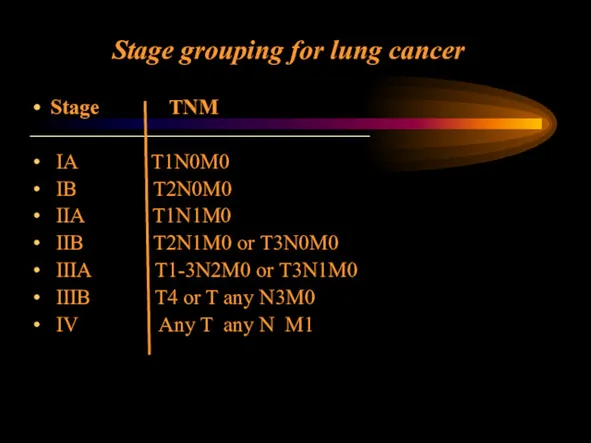
Stage grouping for lung cancer
Stage TNM
————————————————
IA T1N0M0
IB T2N0M0
IIA
Stage grouping for lung cancer
Stage TNM
————————————————
IA T1N0M0
IB T2N0M0
IIA
CLINICAL MANIFESTATION
Symptoms include the following:
1. Constitutional symptoms: fatigue, anorexia,
CLINICAL MANIFESTATION
Symptoms include the following:
1. Constitutional symptoms: fatigue, anorexia,
The symptoms and sighs
depend on its location:
(1) central form
(2)
The symptoms and sighs
depend on its location:
(1) central form
(2)
1. Central tumors diagnosed in 70-85% of all LC.
Symptoms:
1. Central tumors diagnosed in 70-85% of all LC.
Symptoms:
3. A Pancoast tumor is a rare form 1% that arises
3. A Pancoast tumor is a rare form 1% that arises
CLINICAL MANIFESTATION
Symptoms due to intrathoracic spread:
superior vena cava
Symptoms due to intrathoracic spread:
superior vena cava
CLINICAL MANIFESTATION
Symptoms due to distant spread:
neurological dysfunction (ie,
CLINICAL MANIFESTATION
Symptoms due to distant spread:
neurological dysfunction (ie,
4) Paraneoplastic syndromes by ectopic hormone production
Squamous cell carcinomas
4) Paraneoplastic syndromes by ectopic hormone production
Squamous cell carcinomas
DIAGNOSTICS
Diagnostic strategy:
In the presence of a long history of
DIAGNOSTICS
Diagnostic strategy:
In the presence of a long history of
DIAGNOSTICS
Chest X-Ray (CXR)
A chest radiograph is usually the first test
DIAGNOSTICS
Chest X-Ray (CXR)
A chest radiograph is usually the first test
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
2).
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
2).
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
3).
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
3).
DIAGNOSTICS
1. CXR findings in central form of lung
DIAGNOSTICS
1. CXR findings in central form of lung
DIAGNOSTICS
1. CXR findings in central form of lung cancer.
1. CXR findings in central form of lung cancer.
DIAGNOSTICS
1. CXR findings in peripheral form of lung cancer
1. CXR findings in peripheral form of lung cancer
DIAGNOSTICS
1. The CXR sings of nonresolving pneumonia may be occure
DIAGNOSTICS
1. The CXR sings of nonresolving pneumonia may be occure
DIAGNOSTICS
1. Chest X-Ray (CXR).
Mediastinal lymph node enlargement:
Metastases to
1. Chest X-Ray (CXR).
Mediastinal lymph node enlargement:
Metastases to
DIAGNOSTICS
2. Sputum cytologic studies.
Sputum cytology can be a quick
2. Sputum cytologic studies.
Sputum cytology can be a quick
DIAGNOSTICS
3. Bronchoscopy
Diagnostic material can be
obtained with direct biopsy of
3. Bronchoscopy
Diagnostic material can be
obtained with direct biopsy of
DIAGNOSTICS
4. Biopsy.
is preferred for tumors located in the periphery
4. Biopsy.
is preferred for tumors located in the periphery
DIAGNOSTICS
Staging workup
1. Ultrasaund or CT scan of the
Staging workup
1. Ultrasaund or CT scan of the
DIAGNOSTICS
Staging workup
CT scans of chest (left) and abdomen
DIAGNOSTICS
Staging workup
CT scans of chest (left) and abdomen
DIAGNOSTICS
Staging workup
CT/MRI scan of brain
The brain is one of
DIAGNOSTICS
Staging workup
CT/MRI scan of brain
The brain is one of
DIAGNOSTICS
Staging workup
Positron emission tomography (PET)
Multiple hypermetabolic areas suggest
DIAGNOSTICS
Staging workup
Positron emission tomography (PET)
Multiple hypermetabolic areas suggest
DIAGNOSTICS
Staging workup
Bone scan
Multiple abnormal areas of increased radiotracer
DIAGNOSTICS
Staging workup
Bone scan
Multiple abnormal areas of increased radiotracer
DIAGNOSTICS
Staging workup
Thoracentesis. Pleural effusions should be aspirated and examined
DIAGNOSTICS
Staging workup
Thoracentesis. Pleural effusions should be aspirated and examined
DIFFERENTIAL DIAGNOSES
Bronchogenic cyst
Neurogenic tumors
Teratodermoid tumor
DIFFERENTIAL DIAGNOSES
Bronchogenic cyst
Neurogenic tumors
Teratodermoid tumor
SURGICAL CARE
Surgical resection provides the best chance of long-term
Surgical resection provides the best chance of long-term
PRINCIPLES OF TREATMENT
SURGICAL CARE
3. pneumonectomy (in central lung
SURGICAL CARE
3. pneumonectomy (in central lung
CHEMOTHERAPY
Alone has no role in potentially curative therapy.
Is used
Alone has no role in potentially curative therapy.
Is used
RADIATION THERAPY
Reduces local failures in completely
resected stages (II
Reduces local failures in completely
resected stages (II
PROGNOSIS
Estimated 5-year survival rates are as follows:
Stage IA -
Estimated 5-year survival rates are as follows:
Stage IA -
 Проблема вкусовой привлекательности рациона при ХБП и способы ее повышения
Проблема вкусовой привлекательности рациона при ХБП и способы ее повышения БМСК жағдайында көмек көрсету қағидалары
БМСК жағдайында көмек көрсету қағидалары Становление теоретической и клинической медицины Нового времени. Научные революции в медицине. Лекция 7
Становление теоретической и клинической медицины Нового времени. Научные революции в медицине. Лекция 7 Атопический дерматит
Атопический дерматит Лабораторные методы исследования системы крови
Лабораторные методы исследования системы крови Осторожно: грипп и орви
Осторожно: грипп и орви Вакцина против полиомиелита
Вакцина против полиомиелита Әйелдердегі маскүнемдік
Әйелдердегі маскүнемдік Медико-соціальна експертиза при захворюваннях органів дихання
Медико-соціальна експертиза при захворюваннях органів дихання Идиопатические заболевания пародонта
Идиопатические заболевания пародонта Семинар по классификации в Бочча
Семинар по классификации в Бочча ВКР: Течение и лечение катаральных (альвеолярных) маститов в ООО РУСЬ
ВКР: Течение и лечение катаральных (альвеолярных) маститов в ООО РУСЬ Тактика медперсонала при выявлении у пациентов факторов риска или клинических симптомов наркологического заболевания
Тактика медперсонала при выявлении у пациентов факторов риска или клинических симптомов наркологического заболевания Созылмалы бүйрек шамасыздығы
Созылмалы бүйрек шамасыздығы Предмет и задачи психиатрии
Предмет и задачи психиатрии Детская городская клиническая больница имени Н.Ф. Филатова
Детская городская клиническая больница имени Н.Ф. Филатова Электрокардиография при нарушениях ритма сердца
Электрокардиография при нарушениях ритма сердца Шап жарығы
Шап жарығы Нагноительные заболевания легких. Заболевания плевры
Нагноительные заболевания легких. Заболевания плевры Деформация зубных рядов. Зубочелюстная аномалия
Деформация зубных рядов. Зубочелюстная аномалия Харчування дітей старше року
Харчування дітей старше року Физиология крови. Лейкоциты
Физиология крови. Лейкоциты Виразково-некротичний гінгівіт
Виразково-некротичний гінгівіт Современная антимикробная терапия
Современная антимикробная терапия Современные подходы к образованию обучающихся с ОВЗ
Современные подходы к образованию обучающихся с ОВЗ Анаэробная инфекция
Анаэробная инфекция Противоопухолевый иммунитет
Противоопухолевый иммунитет Физиолечение флегмоны кисти
Физиолечение флегмоны кисти