- Plastic Surgery. Survival Guide

Содержание
- 2. Outline of Topics General overview of service Expectations Plastic surgery “Emergencies” Hand Face Soft tissue injuries
- 3. General Overview Plastic surgery at the VA and Elmhurst is a relatively small service staffed soley
- 4. VA is a light service and most ED consults are facial lacerations or hand injuries Elmhurst
- 5. Expectations You are not expected to know everything about plastic surgery YOU SHOULD: be competent in
- 6. Plastic Surgery “Emergencies” Hand/Extremity: amputation, near amputation, vascular compromise compartment syndrome Uncontrolled bleeding Face: Entrapment of
- 7. Hand Includes soft tissue distal to the elbow and bones on wrist and distal Radius/Ulnar fractures
- 8. “Hand History” Specifics about “hand history” Mechanism of injury (crush, laceration, fall) Right-handed or left-handed Occupation
- 10. Amputations This is an emergency - the clock is ticking… Call the plastic surgery resident Also,
- 11. Fractures 95% of time will simply advise to place in splint Splint options: Phalanx, metacarpal, carpals-
- 12. Thumb spica Basic Splinting Position of “safety”
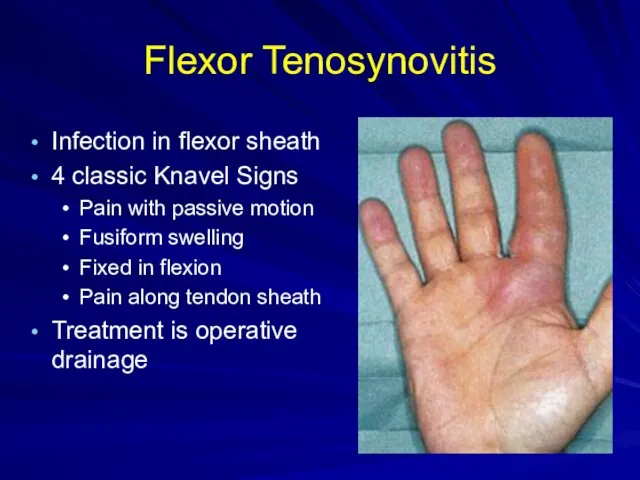
- 13. Flexor Tenosynovitis Infection in flexor sheath 4 classic Knavel Signs Pain with passive motion Fusiform swelling
- 14. Tendon Injuries You are not expected to know how to repair these You must be able
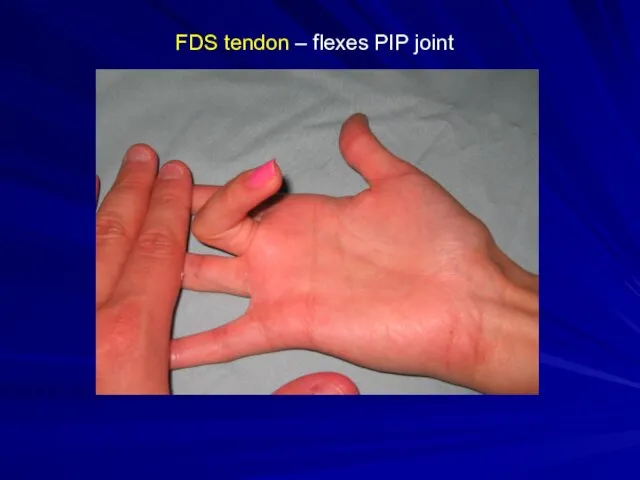
- 15. FDS tendon – flexes PIP joint
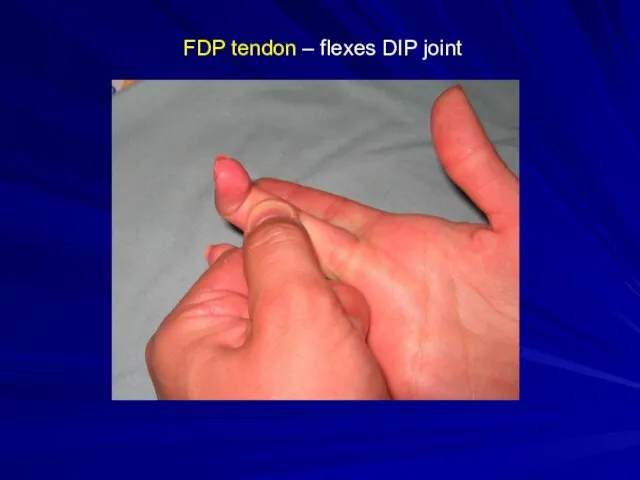
- 16. FDP tendon – flexes DIP joint
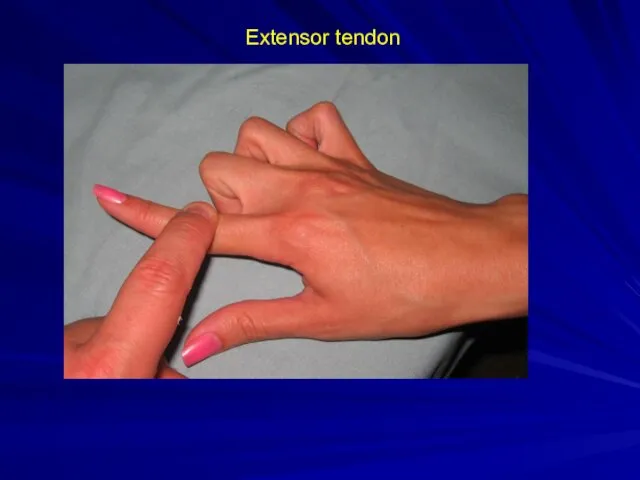
- 17. Extensor tendon
- 18. Nerve Injury Must have high degree of suspicion given location of laceration Most of the time,
- 19. Lacerations Close in 1 layer with 4.0 nylon sutures Not too tight – it will swell
- 20. Digital Block 1% lidocaine – NO EPINEPHERINE 2 nerves – must block both for each finger
- 21. Individual Nerves – inject in each web space Trans-thecal – inject in tendon sheath at A1
- 22. Nailbed injury Typical injury is “crushed finger in door” Remove nail-plate Assess nail-bed injury (below plate)
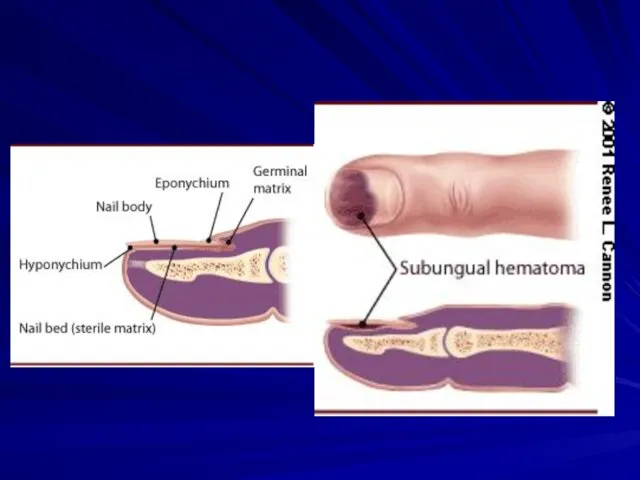
- 24. Sub-Ungal hematoma Hematoma under nail plate Should be drained if > 50% nail surface Drain by
- 26. Facial lacerations Rule out other injuries based on location Lacrimal duct Parotid duct Facial nerve Vascular
- 27. Facial Fractures CT scan – axial and coronal with fine cuts through orbits (3mm) Protect airway
- 28. Orbit Fracture Opthamology must see the patient Assess gross vision Assess occular muscles Entrapment is emergency
- 29. Nasal Fracture Look for septal hematoma Must be drained if present to prevent septal necrosis Is
- 30. Septal Hematoma
- 31. Complex Soft Tissue Injuries Assess wound Irrigate copiously Xray to rule out fractures or foreign bodies
- 32. Decubitus Ulcers Only “emergent” if source of sepsis If wound is open and draining, very unlikely
- 33. V.A.C. system Know how to troubleshoot system if called because it is “beeping” Usually it is
- 35. Clinic Schedule Elmhurst Plastic surgery – Tues 1 PM, Friday 9 AM Hand – Friday 1
- 37. Скачать презентацию
Outline of Topics
General overview of service
Expectations
Plastic surgery “Emergencies”
Hand
Face
Soft tissue injuries
Decubitus ulcers
V.A.C.
Outline of Topics
General overview of service
Expectations
Plastic surgery “Emergencies”
Hand
Face
Soft tissue injuries
Decubitus ulcers
V.A.C.
General Overview
Plastic surgery at the VA and Elmhurst is a relatively
General Overview
Plastic surgery at the VA and Elmhurst is a relatively
VA is a light service and most ED consults are facial
VA is a light service and most ED consults are facial
Expectations
You are not expected to know everything about plastic surgery
YOU SHOULD:
be
Expectations
You are not expected to know everything about plastic surgery
YOU SHOULD:
be
Plastic Surgery “Emergencies”
Hand/Extremity:
amputation, near amputation, vascular compromise
compartment syndrome
Uncontrolled bleeding
Face:
Entrapment of ocular
Plastic Surgery “Emergencies”
Hand/Extremity:
amputation, near amputation, vascular compromise
compartment syndrome
Uncontrolled bleeding
Face:
Entrapment of ocular
Hand
Includes soft tissue distal to the elbow and bones on wrist
Hand
Includes soft tissue distal to the elbow and bones on wrist
“Hand History”
Specifics about “hand history”
Mechanism of injury (crush, laceration, fall)
Right-handed or
“Hand History”
Specifics about “hand history”
Mechanism of injury (crush, laceration, fall)
Right-handed or
Amputations
This is an emergency - the clock is ticking…
Call the plastic
Amputations
This is an emergency - the clock is ticking…
Call the plastic
Fractures
95% of time will simply advise to place in splint
Splint options:
Phalanx,
Fractures
95% of time will simply advise to place in splint
Splint options:
Phalanx,

Thumb spica
Basic Splinting
Position of “safety”
Thumb spica
Basic Splinting
Position of “safety”
Flexor Tenosynovitis
Infection in flexor sheath
4 classic Knavel Signs
Pain with passive motion
Fusiform
Flexor Tenosynovitis
Infection in flexor sheath
4 classic Knavel Signs
Pain with passive motion
Fusiform
Tendon Injuries
You are not expected to know how to repair these
You
Tendon Injuries
You are not expected to know how to repair these
You
FDS tendon – flexes PIP joint
FDS tendon – flexes PIP joint
FDP tendon – flexes DIP joint
FDP tendon – flexes DIP joint
Extensor tendon
Extensor tendon
Nerve Injury
Must have high degree of suspicion given location of laceration
Most
Nerve Injury
Must have high degree of suspicion given location of laceration
Most
Lacerations
Close in 1 layer with 4.0 nylon sutures
Not too tight –
Lacerations
Close in 1 layer with 4.0 nylon sutures
Not too tight –
Digital Block
1% lidocaine – NO EPINEPHERINE
2 nerves – must block both
Digital Block
1% lidocaine – NO EPINEPHERINE
2 nerves – must block both
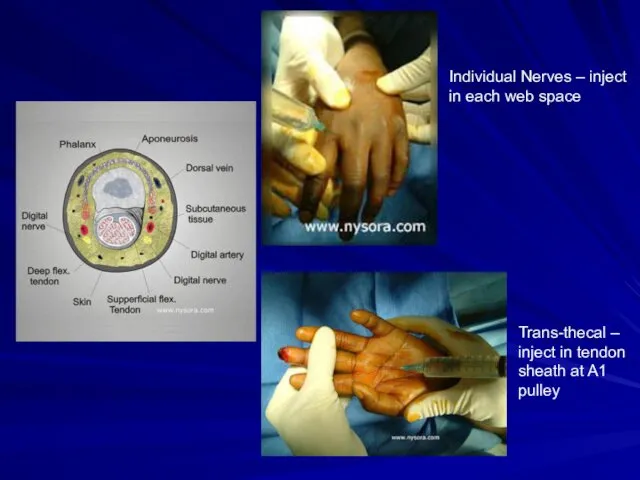
Individual Nerves – inject in each web space
Trans-thecal – inject in
Individual Nerves – inject in each web space
Trans-thecal – inject in
Nailbed injury
Typical injury is “crushed finger in door”
Remove nail-plate
Assess nail-bed injury
Nailbed injury
Typical injury is “crushed finger in door”
Remove nail-plate
Assess nail-bed injury

Sub-Ungal hematoma
Hematoma under nail plate
Should be drained if > 50% nail
Sub-Ungal hematoma
Hematoma under nail plate
Should be drained if > 50% nail
Facial lacerations
Rule out other injuries based on location
Lacrimal duct
Parotid duct
Facial nerve
Vascular
Facial lacerations
Rule out other injuries based on location
Lacrimal duct
Parotid duct
Facial nerve
Vascular
Facial Fractures
CT scan – axial and coronal with fine cuts through
Facial Fractures
CT scan – axial and coronal with fine cuts through
Orbit Fracture
Opthamology must see the patient
Assess gross vision
Assess occular muscles
Entrapment is
Orbit Fracture
Opthamology must see the patient
Assess gross vision
Assess occular muscles
Entrapment is
Nasal Fracture
Look for septal hematoma
Must be drained if present to prevent
Nasal Fracture
Look for septal hematoma
Must be drained if present to prevent
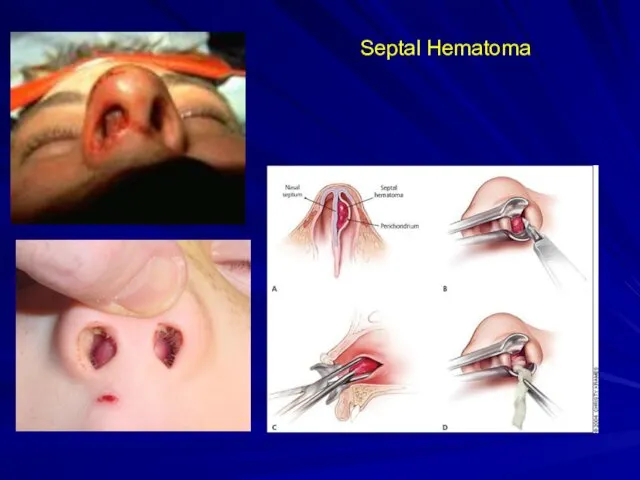
Septal Hematoma
Septal Hematoma
Complex Soft Tissue Injuries
Assess wound
Irrigate copiously
Xray to rule out fractures or
Complex Soft Tissue Injuries
Assess wound
Irrigate copiously
Xray to rule out fractures or
Decubitus Ulcers
Only “emergent” if source of sepsis
If wound is open and
Decubitus Ulcers
Only “emergent” if source of sepsis
If wound is open and
V.A.C. system
Know how to troubleshoot system if called because it is
V.A.C. system
Know how to troubleshoot system if called because it is
Clinic Schedule
Elmhurst
Plastic surgery – Tues 1 PM, Friday 9 AM
Hand –
Clinic Schedule
Elmhurst
Plastic surgery – Tues 1 PM, Friday 9 AM
Hand –
 Постепенная потеря зрения
Постепенная потеря зрения Лечение огнестрельных ранений живота
Лечение огнестрельных ранений живота Офтальмология. Заболевание иридоциклит
Офтальмология. Заболевание иридоциклит Синдром Внезапной Смерти Младенцев
Синдром Внезапной Смерти Младенцев Заболевания толстой кишки
Заболевания толстой кишки Общественное здоровье. Лекция 3. Планирование в здравоохранении
Общественное здоровье. Лекция 3. Планирование в здравоохранении Острая почечная недостаточность (ОПН)
Острая почечная недостаточность (ОПН) Санаторно-курортное обслуживание населения в СССР
Санаторно-курортное обслуживание населения в СССР Инструментальные методы диагностики в гастроэнтерологии. Фиброгастродуоденоскопия
Инструментальные методы диагностики в гастроэнтерологии. Фиброгастродуоденоскопия Жатыр мойнының қатерлі ісігі жүктілік кезінде
Жатыр мойнының қатерлі ісігі жүктілік кезінде Консервированные корма для кошек и собак
Консервированные корма для кошек и собак Роль ультразвукового исследования в дифференциальной диагностики синдрома острой мошонки у детей
Роль ультразвукового исследования в дифференциальной диагностики синдрома острой мошонки у детей Жүректің ишемиялық аурулары кезіндегі ультрадыбыстық зерттеулер
Жүректің ишемиялық аурулары кезіндегі ультрадыбыстық зерттеулер Организация медицинской помощи взрослым пациентам с гемофилией
Организация медицинской помощи взрослым пациентам с гемофилией Ботулизм
Ботулизм Логопедия. Дизартрия
Логопедия. Дизартрия Регенерация тканей и органов (стволовые клетки)
Регенерация тканей и органов (стволовые клетки) Роль акушерки в профилактике геморрагического шока в послеродовом периоде
Роль акушерки в профилактике геморрагического шока в послеродовом периоде Restauration d'une dent pulpée
Restauration d'une dent pulpée Ювенильді идиопатиялық артрит емінде адам иммуноглобулинін тағайындау
Ювенильді идиопатиялық артрит емінде адам иммуноглобулинін тағайындау Строение кожи
Строение кожи Регенерация костной ткани
Регенерация костной ткани Медикалық-генетикалық кеңес. Пренатальдық диогностика әдістері
Медикалық-генетикалық кеңес. Пренатальдық диогностика әдістері Острая сердечная недостаточность (ОСН)
Острая сердечная недостаточность (ОСН) Вспомогательные вещества. Значение в фармацевтической технологии
Вспомогательные вещества. Значение в фармацевтической технологии Рентгенография. Показания к рентгенографии
Рентгенография. Показания к рентгенографии Инфекции дыхательных путей
Инфекции дыхательных путей Тики (тикозные гиперкинезы)
Тики (тикозные гиперкинезы)