- Schistosomiasis

Содержание
- 2. Topics Definition The Pathogen Epidemiology Etiology and Life Cycle Pathobiology Clinical manifestations Diagnosis Treatment
- 3. Schistosomiasis is an acute and chronic disease caused by parasitic worms. People are infected during routine
- 4. Schistosomiasis control focuses on reducing disease through periodic, large-scale population treatment with praziquantel; a more comprehensive
- 5. History Schistosomiasis is known as bilharzia or bilharziosis in many countries, after German physician Theodor Bilharz,
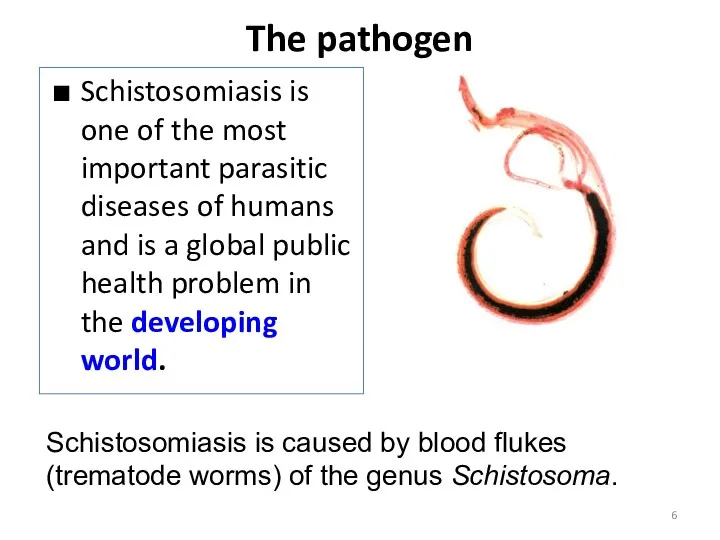
- 6. The pathogen Schistosomiasis is one of the most important parasitic diseases of humans and is a
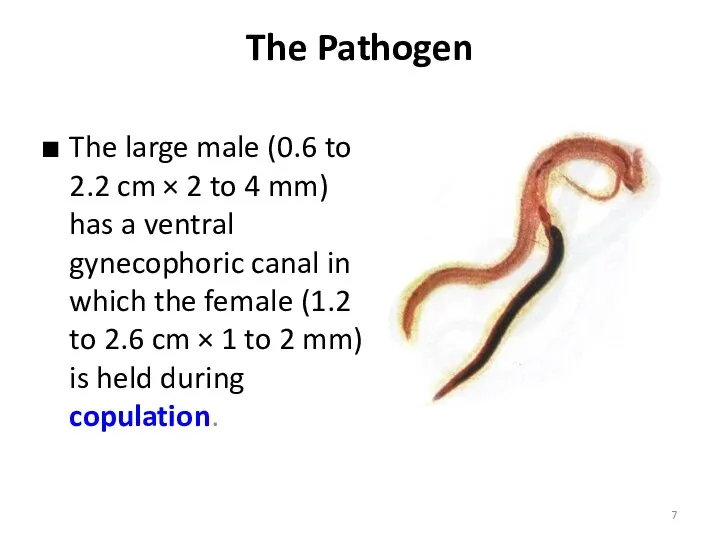
- 7. The Pathogen The large male (0.6 to 2.2 cm × 2 to 4 mm) has a
- 8. The pathogen
- 9. Distribution
- 10. EPIDEMIOLOGY Infection sources Mode of transmission Susceptible population
- 11. Infection sources Patients reservoir host – animal reservoirs cows, pigs(S. japonicum) Rodents, monkeys, and baboons have
- 12. The freshwater snail intermediate hosts are Biomphalaria spp in Africa and Biomphalaria glabrata (Australorbis) and Tropicarbis
- 13. Transmission People become infected when larval forms of the parasite – released by freshwater snails –
- 14. Schistosoma life cycle 4 to 7 weeks 72 hours 6 weeks
- 17. PATHOPHYSIOLOGY Adult worms release eggs in the venules of the mesentery, and the eggs enter the
- 18. Because the habitat of S. mansoni, S. japonicum, S. mekongi, and S. intercalatum worms is the
- 19. CLINICAL MANIFESTATIONS Clinical manifestations of schistosomiasis are divided into -schistosome dermatitis -acute schistosomiasis -chronic schistosomiasis
- 20. CLINICAL MANIFESTATIONS A pruritic papular rash occurs within 24 hours after the penetration of cercariae and
- 21. CLINICAL MANIFESTATIONS ( Acute schistosomiasis ) Acute schistosomiasis occurs usually 20 to 50 days after primary
- 22. CLINICAL MANIFESTATIONS (Acute schistosomiasis ) Malaise, diarrhea, weight loss, cough, dyspnea, chest pain, restrictive respiratory insufficiency
- 23. CLINICAL MANIFESTATIONS ( Acute schistosomiasis ) Acute disease is not observed in individuals living in endemic
- 24. CLINICAL MANIFESTATIONS (chronic schistosomiasis) Abdominal pain, irregular bowel movements and blood in the stool are the
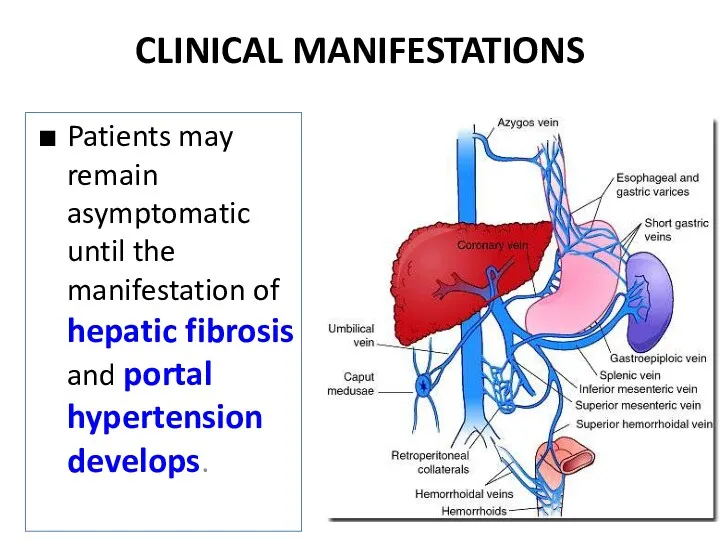
- 25. CLINICAL MANIFESTATIONS Patients may remain asymptomatic until the manifestation of hepatic fibrosis and portal hypertension develops.
- 26. CLINICAL MANIFESTATIONS Hepatic fibrosis is caused by a granulomatous reaction to Schistosoma eggs that have been
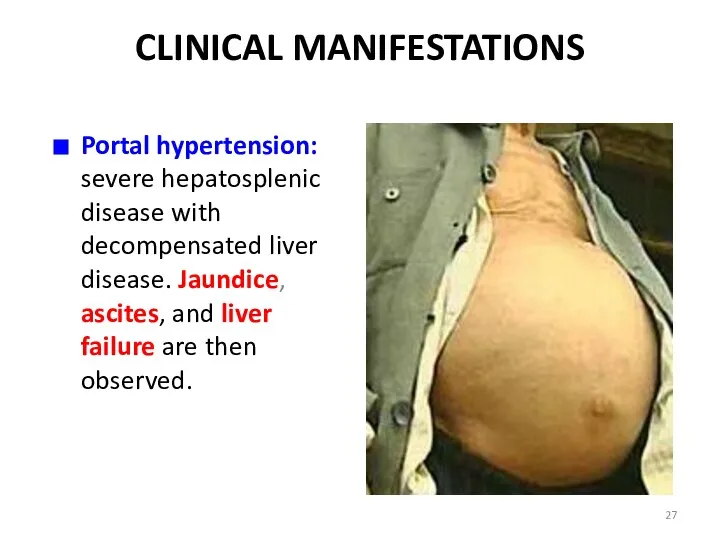
- 27. CLINICAL MANIFESTATIONS Portal hypertension: severe hepatosplenic disease with decompensated liver disease. Jaundice, ascites, and liver failure
- 28. CLINICAL MANIFESTATIONS In hospitalized adult patients with S. japonicum infection, cerebral schistosomiasis occurs in 1.7 to
- 29. CLINICAL MANIFESTATIONS In S. haematobium infection, the main organ system involved is the urinary tract. The
- 30. CLINICAL MANIFESTATIONS In chronic disease, usually in older patients, granulomas at the lower end of the
- 31. CLINICAL MANIFESTATIONS An increased incidence of squamous cell carcinoma of the bladder has been reported in
- 32. Basis for DIAGNOSIS History of epidemiology: infested water contanct Clinical manifestation Laboratory tests Differentiation diagnosis
- 33. DIAGNOSIS Blood routine examination Liver function test Liver ultrasonic CT Antibodies detection: Several serologic tests for
- 34. Schistosomiasis is diagnosed through the detection of parasite eggs in stool or urine specimens. Antibodies and/or
- 35. For urogenital schistosomiasis, a filtration technique using nylon, paper or polycarbonate filters is the standard diagnostic
- 36. TREATMENT Three compounds are in use metrifonate, oxamniquine, and praziquantel, and all three are included in
- 37. Praziquantel A pyrazinoisoquinoline derivative, is the drug of choice for the treatment of schistosomiasis for four
- 38. TREATMENT The standard recommended treatment consists of a single dose of praziquantel, 40 mg/kg, for S.
- 39. TREATMENT With these dosages of praziquantel, recorded cure rates are: 75 to 85% for S.haematobium, 63
- 40. TREATMENT The most common side effects observed with praziquantel or oxamniquine are related to the gastrointestinal
- 41. TREATMENT These symptoms can be observed in up to 50% of patients but are usually well
- 42. TREATMENT Although a reduction in the intensity of infection and morbidity has been documented after mass
- 43. TREATMENT The mortality rate is 0.05% for severe S. mansoni infection and 1.8% for severe S.japonicum
- 44. Summary of schistosomiasis (1) Schistosomiasis occurs mainly in rural agricultural and periurban areas in the developing
- 46. Скачать презентацию
Topics
Definition
The Pathogen
Epidemiology
Etiology and Life Cycle
Pathobiology
Clinical manifestations
Diagnosis
Treatment
Topics
Definition
The Pathogen
Epidemiology
Etiology and Life Cycle
Pathobiology
Clinical manifestations
Diagnosis
Treatment
Schistosomiasis is an acute and chronic disease caused by parasitic
Schistosomiasis is an acute and chronic disease caused by parasitic
Schistosomiasis control focuses on reducing disease through periodic, large-scale population
Schistosomiasis control focuses on reducing disease through periodic, large-scale population
History
Schistosomiasis is known as bilharzia or bilharziosis in many countries, after
History
Schistosomiasis is known as bilharzia or bilharziosis in many countries, after
The pathogen
Schistosomiasis is one of the most important parasitic diseases of
The pathogen
Schistosomiasis is one of the most important parasitic diseases of
The Pathogen
The large male (0.6 to 2.2 cm × 2 to
The Pathogen
The large male (0.6 to 2.2 cm × 2 to
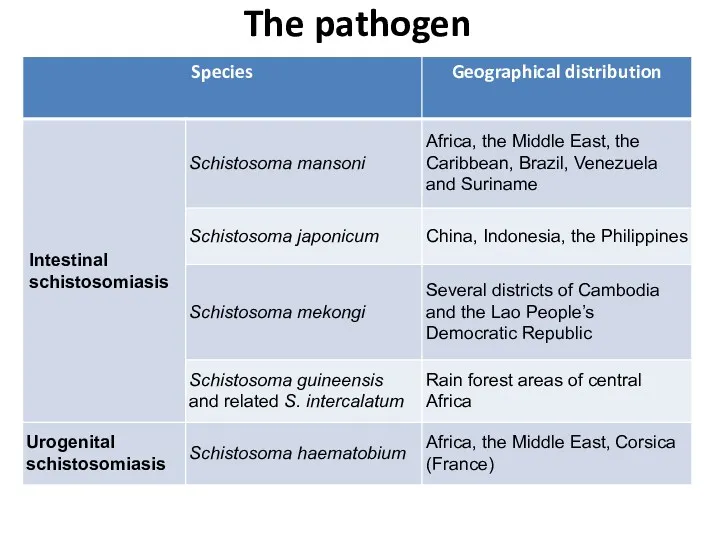
The pathogen
The pathogen
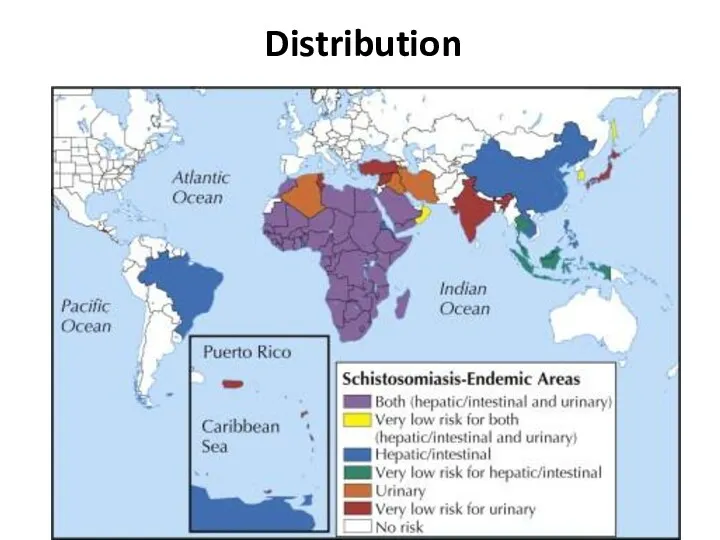
Distribution
Distribution
EPIDEMIOLOGY
Infection sources
Mode of transmission
Susceptible population
EPIDEMIOLOGY
Infection sources
Mode of transmission
Susceptible population
Infection sources
Patients
reservoir host – animal reservoirs
cows, pigs(S. japonicum)
Rodents, monkeys,
Infection sources
Patients
reservoir host – animal reservoirs
cows, pigs(S. japonicum)
Rodents, monkeys,

The freshwater snail intermediate hosts are Biomphalaria spp in Africa and
The freshwater snail intermediate hosts are Biomphalaria spp in Africa and
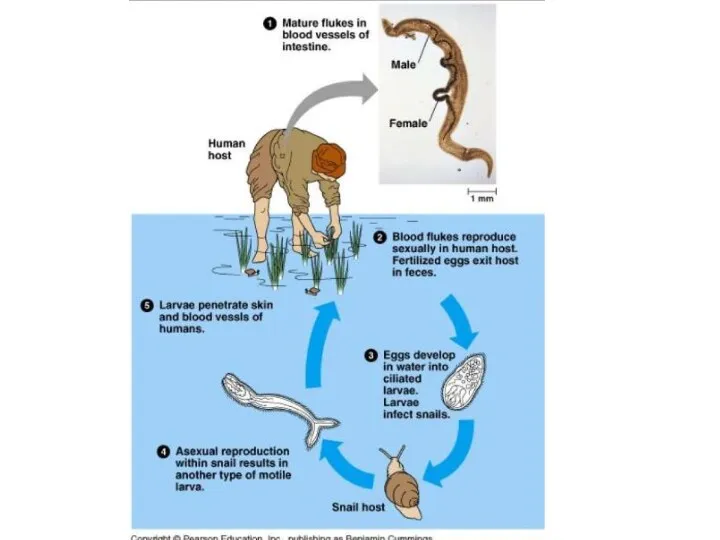
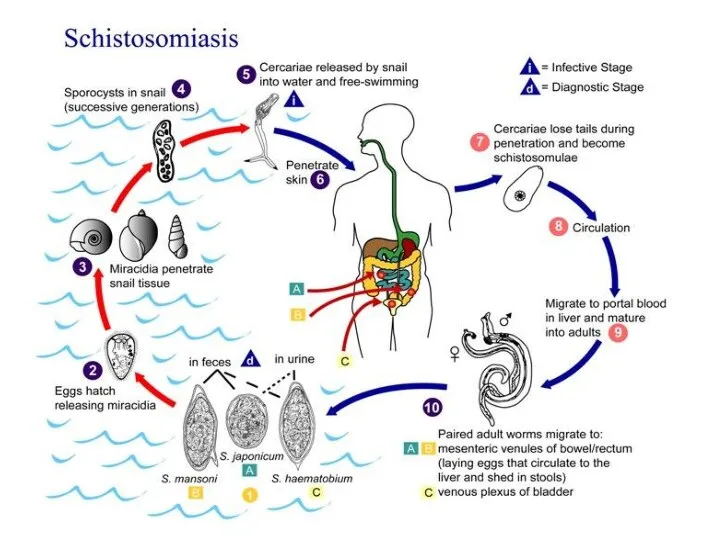
Transmission
People become infected when larval forms of the parasite – released
Transmission
People become infected when larval forms of the parasite – released
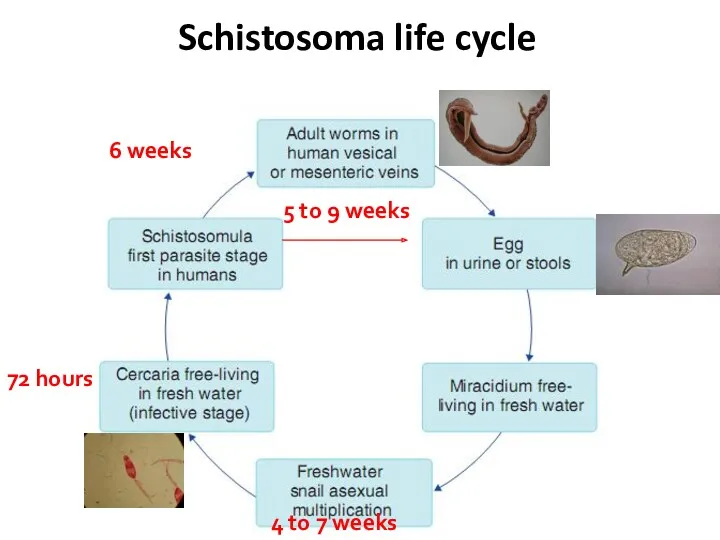
Schistosoma life cycle
4 to 7 weeks
72 hours
6 weeks
Schistosoma life cycle
4 to 7 weeks
72 hours
6 weeks
PATHOPHYSIOLOGY
Adult worms release eggs in the venules of the mesentery, and
PATHOPHYSIOLOGY
Adult worms release eggs in the venules of the mesentery, and
Because the habitat of S. mansoni, S. japonicum, S. mekongi, and
Because the habitat of S. mansoni, S. japonicum, S. mekongi, and
CLINICAL MANIFESTATIONS
Clinical manifestations of schistosomiasis are divided into
-schistosome dermatitis
CLINICAL MANIFESTATIONS
Clinical manifestations of schistosomiasis are divided into
-schistosome dermatitis
CLINICAL MANIFESTATIONS
A pruritic papular rash occurs within 24 hours after the
CLINICAL MANIFESTATIONS
A pruritic papular rash occurs within 24 hours after the
CLINICAL MANIFESTATIONS
( Acute schistosomiasis )
Acute schistosomiasis occurs usually 20 to 50
CLINICAL MANIFESTATIONS
( Acute schistosomiasis )
Acute schistosomiasis occurs usually 20 to 50
CLINICAL MANIFESTATIONS
(Acute schistosomiasis )
Malaise, diarrhea, weight loss, cough, dyspnea, chest
CLINICAL MANIFESTATIONS
(Acute schistosomiasis )
Malaise, diarrhea, weight loss, cough, dyspnea, chest
CLINICAL MANIFESTATIONS
( Acute schistosomiasis )
Acute disease is not observed in
CLINICAL MANIFESTATIONS
( Acute schistosomiasis )
Acute disease is not observed in
CLINICAL MANIFESTATIONS
(chronic schistosomiasis)
Abdominal pain, irregular bowel movements and blood in the
CLINICAL MANIFESTATIONS
(chronic schistosomiasis)
Abdominal pain, irregular bowel movements and blood in the
CLINICAL MANIFESTATIONS
Patients may remain asymptomatic until the manifestation of hepatic fibrosis
CLINICAL MANIFESTATIONS
Patients may remain asymptomatic until the manifestation of hepatic fibrosis
CLINICAL MANIFESTATIONS
Hepatic fibrosis is caused by a granulomatous reaction to Schistosoma
CLINICAL MANIFESTATIONS
Hepatic fibrosis is caused by a granulomatous reaction to Schistosoma
CLINICAL MANIFESTATIONS
Portal hypertension: severe hepatosplenic disease with decompensated liver disease. Jaundice,
CLINICAL MANIFESTATIONS
Portal hypertension: severe hepatosplenic disease with decompensated liver disease. Jaundice,
CLINICAL MANIFESTATIONS
In hospitalized adult patients with S. japonicum infection, cerebral schistosomiasis
CLINICAL MANIFESTATIONS
In hospitalized adult patients with S. japonicum infection, cerebral schistosomiasis
CLINICAL MANIFESTATIONS
In S. haematobium infection, the main organ system involved is
CLINICAL MANIFESTATIONS
In S. haematobium infection, the main organ system involved is
CLINICAL MANIFESTATIONS
In chronic disease, usually in older patients, granulomas at the
CLINICAL MANIFESTATIONS
In chronic disease, usually in older patients, granulomas at the
CLINICAL MANIFESTATIONS
An increased incidence of squamous cell carcinoma of the
CLINICAL MANIFESTATIONS
An increased incidence of squamous cell carcinoma of the
Basis for DIAGNOSIS
History of epidemiology: infested water contanct
Clinical manifestation
Laboratory tests
Differentiation
Basis for DIAGNOSIS
History of epidemiology: infested water contanct
Clinical manifestation
Laboratory tests
Differentiation
DIAGNOSIS
Blood routine examination
Liver function test
Liver ultrasonic
CT
Antibodies detection: Several serologic tests for
DIAGNOSIS
Blood routine examination
Liver function test
Liver ultrasonic
CT
Antibodies detection: Several serologic tests for
Schistosomiasis is diagnosed through the detection of parasite eggs in stool
Schistosomiasis is diagnosed through the detection of parasite eggs in stool
For urogenital schistosomiasis, a filtration technique using nylon, paper or polycarbonate
For urogenital schistosomiasis, a filtration technique using nylon, paper or polycarbonate
TREATMENT
Three compounds are in use metrifonate, oxamniquine, and praziquantel, and all
TREATMENT
Three compounds are in use metrifonate, oxamniquine, and praziquantel, and all
Praziquantel
A pyrazinoisoquinoline derivative, is the drug of choice for the treatment of
Praziquantel
A pyrazinoisoquinoline derivative, is the drug of choice for the treatment of
TREATMENT
The standard recommended treatment consists of a single dose of praziquantel, 40 mg/kg, for S. mansoni, S. haematobium and S. intercalatum infection.
In S.japonicum infection, a total dose of 60 mg/kg is recommended, split into two or three doses in a single day.
S. mekongi may require two treatments at 60 mg/kg body weight.
TREATMENT
The standard recommended treatment consists of a single dose of praziquantel, 40 mg/kg, for S. mansoni, S. haematobium and S. intercalatum infection.
In S.japonicum infection, a total dose of 60 mg/kg is recommended, split into two or three doses in a single day.
S. mekongi may require two treatments at 60 mg/kg body weight.
TREATMENT
With these dosages of praziquantel, recorded cure rates are:
75 to 85% for S.haematobium,
63 to 85% for S. mansoni,
80 to 90% for S. japonicum,
89% for S.intercalatum,
60 to 80% for double infections
with S. mansoni and S. haematobium.
TREATMENT
With these dosages of praziquantel, recorded cure rates are:
75 to 85% for S.haematobium,
63 to 85% for S. mansoni,
80 to 90% for S. japonicum,
89% for S.intercalatum,
60 to 80% for double infections
with S. mansoni and S. haematobium.
TREATMENT
The most common side effects observed with
praziquantel or oxamniquine are related to the gastrointestinal tract: abdominal pain or discomfort, nausea, vomiting, anorexia, and diarrhea.
TREATMENT
The most common side effects observed with
praziquantel or oxamniquine are related to the gastrointestinal tract: abdominal pain or discomfort, nausea, vomiting, anorexia, and diarrhea.
TREATMENT
These symptoms can be observed in up to 50% of patients but are usually well tolerated.
Other side effects are related to the central nervous system (e.g., headache, dizziness, drowsiness) and the skin (e.g., pruritus, eruptions) or may be nonspecific (e.g., fever, fatigue).
TREATMENT
These symptoms can be observed in up to 50% of patients but are usually well tolerated.
Other side effects are related to the central nervous system (e.g., headache, dizziness, drowsiness) and the skin (e.g., pruritus, eruptions) or may be nonspecific (e.g., fever, fatigue).
TREATMENT
Although a reduction in the intensity of infection and morbidity has been documented after mass chemotherapy, provision of clean water, use of molluscicides (kill the snail), and adequate
TREATMENT
Although a reduction in the intensity of infection and morbidity has been documented after mass chemotherapy, provision of clean water, use of molluscicides (kill the snail), and adequate
TREATMENT
The mortality rate is 0.05% for severe S. mansoni infection and 1.8% for severe S.japonicum infection.
Bleeding from esophageal varices is the most
serious complication.
Chronic infection can lead to hepatocellular
carcinoma.
TREATMENT
The mortality rate is 0.05% for severe S. mansoni infection and 1.8% for severe S.japonicum infection.
Bleeding from esophageal varices is the most
serious complication.
Chronic infection can lead to hepatocellular
carcinoma.
Summary of schistosomiasis (1)
Schistosomiasis occurs mainly in rural agricultural and periurban
Summary of schistosomiasis (1)
Schistosomiasis occurs mainly in rural agricultural and periurban
 Офтальмология. Патология вспомогательного аппарата глаза
Офтальмология. Патология вспомогательного аппарата глаза Техника транспортной иммобилизации верхней конечности
Техника транспортной иммобилизации верхней конечности Догоспитальный этап экстренной помощи детям при отеке легких, отеке мозга, отравлении
Догоспитальный этап экстренной помощи детям при отеке легких, отеке мозга, отравлении Гормональные нарушения и хроническая венозная недостаточность
Гормональные нарушения и хроническая венозная недостаточность Классификация звуков
Классификация звуков Профессиональная интоксикация пестицидами
Профессиональная интоксикация пестицидами Инфекции, передающиеся половым путем
Инфекции, передающиеся половым путем Деятельность медицинской сестры в организации ухода за пациентами с повреждениями нижних конечностей
Деятельность медицинской сестры в организации ухода за пациентами с повреждениями нижних конечностей Організація надання медичної допомоги населенню в умовах надзвичайних ситуацій
Організація надання медичної допомоги населенню в умовах надзвичайних ситуацій Утопление и погружение в воду
Утопление и погружение в воду Транспортная иммобилизация
Транспортная иммобилизация Вирусные инфекции. Задачи
Вирусные инфекции. Задачи Гигиена труда в металлургической промышленности. Основные профессиональные группы. Основные неблагоприятные факторы
Гигиена труда в металлургической промышленности. Основные профессиональные группы. Основные неблагоприятные факторы Тері физиологиясы
Тері физиологиясы Аллергия. Классификация аллергических процессов
Аллергия. Классификация аллергических процессов Патологические изменения кожи
Патологические изменения кожи Клиническая фармакология психотропных средств Часть 1. Антипсихотики (нейролептики)
Клиническая фармакология психотропных средств Часть 1. Антипсихотики (нейролептики) Почки. Синдромы
Почки. Синдромы Фармацевтическая опека при травматических и инфекционных повреждениях кожи
Фармацевтическая опека при травматических и инфекционных повреждениях кожи Прием у детского гинеколога. Методы исследования
Прием у детского гинеколога. Методы исследования Бинокулярное зрение. Косоглазие
Бинокулярное зрение. Косоглазие Нейросенсорная тугоухость
Нейросенсорная тугоухость Виды и стадии голодания. Изменения обмена веществ и функции организма при голодании
Виды и стадии голодания. Изменения обмена веществ и функции организма при голодании Правила чистки зубов
Правила чистки зубов Иерсинии - псевдотуберкулезный микроб. Микробиология
Иерсинии - псевдотуберкулезный микроб. Микробиология ҰлпАның қабынбалы аурулары
ҰлпАның қабынбалы аурулары Расстройства сознания
Расстройства сознания Питание человека и долголетие
Питание человека и долголетие