- emergencies

Содержание
- 2. Lets start with a case Male brought in as a John Doe found wandering in the
- 3. So this is what we get Utox + ETOH, Na: 140 K+: 3.1 Mg: 2.0 Creat:1.0
- 4. Dx: Tx Acute alcohol intoxication Given Lfts, CBC results appears to be a chronic ETOHic Either-
- 5. Several hours pass, pt indicated he wants to get clean and was beginning to sober up
- 6. Things that come to mind Acute ETOH WD If acute DT- initiate BZ Delirium due to
- 7. Through your excellent care the patient is stabilized but what if…
- 8. The results are as follows: Utox + cocaine Na: 140 K+: 3.9 Mg: 2.2 Creat:1.0 BUN:
- 9. Acute cocaine intoxication Check EKG to make sure not having an MI! Tx with nothing, BZ,
- 10. Could also be an exacerbation of a primary psychotic illness such as schizophrenia Tx with antipsychotics
- 11. So our patient story evolves When the nurse attempts to get the ECG the patient jumps
- 12. Emergency Dept. (ED) Presentations An equal number of men and women attend the ED with a
- 13. ED Presentations Emergency presentations may include: People with suicidal ideation People experiencing psychosis People in situational
- 14. Recognition of distress Situations which may cause distress: Relationship issues Conflict Trauma Bereavement Loss of friends,
- 15. People react differently to stressors and may present as Anxious Depressed Suicidal Angry Tearful Agitated Aggressive
- 16. Respond appropriately Always assess the risk to yourself and others If able to do so ask
- 17. Assessment The most important question is: Is this presentation due to a primary or secondary psychiatric
- 18. Physical Examination Vital Signs Finger-prick blood glucose level Dipstick urinalysis Urine drug screen Look for any
- 19. Mental State Exam Appearance Behaviour Conversation / speech Affect / mood Perception Cognition Insight / Judgement
- 20. Risk Assessment Risk of harm to self Risk of harm to others Level of problem with
- 21. Risk of harm to self What are the static factors Previous suicide attempt Previous high lethality
- 22. Risk of harm to self What are the dynamic factors Intent / plan / thoughts Current
- 23. Risk of harm to others What are the static factors Under 25 years of age History
- 24. Risk of Vulnerability/Exploitation/Self Neglect At risk of being sexually abused by others At risk of domestic/family
- 25. Violence and Aggression Aggression: Hostile or destructive behaviour or actions Violence: Physical force exerted for the
- 26. Biological Amygdala, hypothalamus, prefrontal cortex, limbic system Cortical dysfunction e.g. abnormal EEG in antisocial personality disorder
- 27. Developmental Factors Associated with Adult Violence Abuse by parents Truancy, school failure, lower IQ Delinquency as
- 28. Risk Factors for Aggression or Violence young, male developmental factors less education lack of sustained employment
- 29. Risk Factors for Aggression and Violence (continued) chronic anger towards others recent sense of being unfairly
- 30. Predictors of Impending Violence Include: Refusal to cooperate Intense staring Motor restlessness, akathysia Purposeless movements Labile
- 31. Management Establish differential diagnosis Attempt where possible to initiate treatment with medication to treat underlying illness
- 32. Choice of Medication Consider: speed of onset oral vs IM duration of action side effects past
- 33. Pharmacologic Support: Benzodiazepines Lorazepam - inthe first 24 hours agitation is as effectively addressed with lorazepam
- 34. sedative hypnotic effect which can be additive with other such agents (ex. Alcohol) resulting in excessive
- 35. Benzodiazepines Elderly patients with respiratory disease acute intoxication with alcohol severe impairment of hepatic or renal
- 36. Midazolam Midazolam 2 – 10 mg (IM/IV) for agitated, aggressive patients Risk of respiratory depression –
- 37. Clonazepam Clonazepam (0.5 – 2 mg) is a longer acting IM alternative to midazolam – but
- 38. Lorazepam Lorazepam (0.5 – 2.5 mg) -shorter half life Onset of action 5 – 15 minutes
- 39. Diazepam Diazepam (2.5 – 10 mg) is well absorbed orally IM absorption is erratic IV excellent
- 40. Pharmacologic support: Antipsychotics effective in reducing agitation There are options in the following forms: PO, IM,
- 41. IM Antipsychotics Ziprasidone (Geodon) 20mg IM q 4 hours or 10mg q 2 hours not to
- 42. Haloperidol (oral / IM) Time of Onset of action depends on route of administration IV –
- 43. Zuclopenthixol Zuclopenthixol HCl (Clopixol) 10, 25mg tablets Onset of action 10-30 minutes Peak plasma levels in
- 44. Acuphase (Zuclopenthixol acetate) Acuphase (Zuclopenthixol acetate) – short acting depot used when IM medication is required,
- 45. Second Generation Antipsychotics (SGAs) Risperidone (tablets, depot) Paliperidone (tablets, depot) Olanzapine (tablets, short-acting IM) Amisulpride (tablets)
- 46. Second Generation Antipsychotics For tranquilization and to reduce hostility in agitated patients In mania and depression
- 47. Medication for agitated, psychotic patients Oral atypical antipsychotic Oral benzodiazepine in the first instance Generally involves
- 48. Parenteral Medication If patient more agitated or unwilling to accept oral medication: IM olanzapine or IM
- 49. Extrapyramidal symptoms Haldol is the most likely to cause extrapyramidal symptoms (eps) followed by risperidone with
- 50. EPS treatment Be ready to give O2 if breathing problems develop PO or IM Dekinet 5
- 51. Our patient story evolves On interview pt stated he took “a bunch of meds because I’m
- 52. First things first Make sure he is safe in the current setting i.e. is he still
- 53. Suicidality and suicide Suicide- the act of self- murder Suicidality- thoughts, preoccupations, drives and preparations
- 54. Epidemiology 1 completed suicede: 25 attempts Males are X4 successful than females, use mor lethal means
- 55. Self harm X38 risk after any previous attempt Mainly ½ year after 1% of the attempters
- 56. Risk factors M 45y A letter Previous attempts lonely In conflict Any psychiatric diagnosis Chronic pain
- 57. Psychiatric factors At least 1 ps. diagnosis 22% in the first year after receiving the DX
- 62. Protective factors Faith Parenthood, family Responsibility Optimism Fear Social embarassement Morality Support Plans for future
- 63. Suicide assessment Ideation- acute vs. chronic, passive vs. active- if active is there a plan, If
- 64. Suicide assessment cont. Clinical factors: Personal history of suicide attempt, substance use, chronic medical illness, agitation,
- 65. Is it possible to predict suicide? Impossible! Possible to access the immediate risk factors Impossible to
- 66. Managing the suicidal patient Ensure safety Anamnesys and collateral hystory Don’t afraid to directly ask Past
- 67. Acute management Treatment plan Remove the means Address the crisis Treat intoxication Relieve pain If suicidal
- 68. Serotonin syndrome Rapid onset of symptoms 60% present within 6 hours after initial use of medication,
- 69. Drug interactions associated with severe serotonin syndrome Phenelzine and meperidine Tranylcypromine and imipramine Phenelzine and SSRI
- 70. Diagnosis : Classic triad Mental status changes: confusion, restlessness, agitation, anxiety, decreased level of consciousness Neuromuscular
- 71. Spectrum of Clinical Findings. Edward W. Boyer, M.D The serotonin syndrome .N Engl J Med 2005
- 72. Treatment Discontinuation of all serotonergic agents Supportive care, many do not require tx Consult with a
- 73. Sexual abuse- PREVALENCE Sexual assault is one of the most under reported crimes, with 60% still
- 74. Victims of sexual assault are: 3 times more likely to suffer from depression. 6 times more
- 75. Rape is NEVER the victim’s fault! Rape is an act of violence and aggression and is
- 76. UNIQUENESS OF SEXUAL VIOLENCE AS A CRIMINAL VIOLATION The violation of “self” that causes trauma in
- 77. TWO MOST COMMON RESPONSES IMMEDIALEY FOLLOWING RAPE Expressed demonstrating anger, fear, and anxiety through restlessness, crying
- 78. Symptoms of Survivors (both female and male) Nightmares / sleep disturbances Substance Abuse Panic Attacks Irritability/Anger
- 79. Disassociation (zoning out) Anorexia / Bulimia / Overeating (Eating disorders) “Cutting” / Self-mutilation Anger: distance =
- 80. guilt – confusion – sexual identity issues Extreme independence/isolation Triggers / Sights, sounds, smells, feelings: Re-experiencing
- 81. Is alcohol a date rape drug? Any drug that can affect judgment and behavior can put
- 82. ROHYPNOL a.k.a. “roofies” Rohypnol (roh-HIP-nol). Rohypnol is the trade name for flunitrazepam (FLOO-neye-TRAZ-uh-pam). Abuse of two
- 83. GHB - GAMMA HYDROXY BUTYRATE GHB is a central nervous system depressant that is illegally manufactured
- 84. ECSTASY While not classified as a “date rape drug”, many survivors were raped while using ecstasy.
- 85. SUBSTANCE ABUSING SURVIVORS 75% of men and 55% of women involved in acquaintance rapes reported using
- 86. Substance Abuse Two to three times more common among those with psychiatric illness than in general
- 87. Common Substances of Abuse Alcohol Cocaine Amphetamine Methamphetamine MDMA (3,4 methylene dioxymethamphetamine), (ecstasy) Ketamine Cannabis Opiates
- 88. The Drug Abusing Patient Patient may present with intoxication or withdrawal symptom Stimulant intoxication may induce
- 89. Amphetamine – Methamphetamine Abuse Clinical Presentation: Acute anxiety Paranoid ideation Loud, demanding behaviour Motor agitation, aggression
- 91. Скачать презентацию
Lets start with a case
Male brought in as a John
Lets start with a case
Male brought in as a John
So this is what we get
Utox + ETOH,
Na: 140 K+:
So this is what we get
Utox + ETOH,
Na: 140 K+:
Dx: Tx
Acute alcohol intoxication
Given Lfts, CBC results appears to be a
Dx: Tx
Acute alcohol intoxication
Given Lfts, CBC results appears to be a
Several hours pass, pt indicated he wants to get clean and
Several hours pass, pt indicated he wants to get clean and
Things that come to mind
Acute ETOH WD
If acute DT- initiate BZ
Delirium
Things that come to mind
Acute ETOH WD
If acute DT- initiate BZ
Delirium
Through your excellent care the patient is stabilized but what if…
Through your excellent care the patient is stabilized but what if…
The results are as follows:
Utox + cocaine
Na: 140 K+: 3.9 Mg:
The results are as follows:
Utox + cocaine
Na: 140 K+: 3.9 Mg:
Acute cocaine intoxication
Check EKG to make sure not having an MI!
Acute cocaine intoxication
Check EKG to make sure not having an MI!
Could also be an exacerbation of a primary psychotic illness such
Could also be an exacerbation of a primary psychotic illness such
So our patient story evolves
When the nurse attempts to get
So our patient story evolves
When the nurse attempts to get
Emergency Dept. (ED) Presentations
An equal number of men and women attend
Emergency Dept. (ED) Presentations
An equal number of men and women attend
ED Presentations
Emergency presentations may include:
People with suicidal ideation
People experiencing psychosis
People in
ED Presentations
Emergency presentations may include:
People with suicidal ideation
People experiencing psychosis
People in
Recognition of distress
Situations which may cause distress:
Relationship issues
Conflict
Trauma
Bereavement
Loss of friends, job,
Recognition of distress
Situations which may cause distress:
Relationship issues
Conflict
Trauma
Bereavement
Loss of friends, job,

People react differently to stressors and may present as
Anxious
Depressed
Suicidal
Angry
Tearful
Agitated
Aggressive
Confused
People react differently to stressors and may present as
Anxious
Depressed
Suicidal
Angry
Tearful
Agitated
Aggressive
Confused
Respond appropriately
Always assess the risk to yourself and others
If able to
Respond appropriately
Always assess the risk to yourself and others
If able to
Assessment
The most important question is:
Is this presentation due to a primary
Assessment
The most important question is:
Is this presentation due to a primary
Physical Examination
Vital Signs
Finger-prick blood glucose level
Dipstick urinalysis
Urine drug screen
Look for any
Physical Examination
Vital Signs
Finger-prick blood glucose level
Dipstick urinalysis
Urine drug screen
Look for any
Mental State Exam
Appearance
Behaviour
Conversation / speech
Affect / mood
Perception
Cognition
Insight / Judgement
Rapport
Mental State Exam
Appearance
Behaviour
Conversation / speech
Affect / mood
Perception
Cognition
Insight / Judgement
Rapport
Risk Assessment
Risk of harm to self
Risk of harm to others
Level of
Risk Assessment
Risk of harm to self
Risk of harm to others
Level of
Risk of harm to self
What are the static factors
Previous suicide attempt
Previous
Risk of harm to self
What are the static factors
Previous suicide attempt
Previous
Risk of harm to self
What are the dynamic factors
Intent / plan
Risk of harm to self
What are the dynamic factors
Intent / plan
Risk of harm to others
What are the static factors
Under 25 years
Risk of harm to others
What are the static factors
Under 25 years
Risk of Vulnerability/Exploitation/Self Neglect
At risk of being sexually abused by others
At
Risk of Vulnerability/Exploitation/Self Neglect
At risk of being sexually abused by others
At
Violence and Aggression
Aggression: Hostile or destructive behaviour or actions
Violence: Physical
Violence and Aggression
Aggression: Hostile or destructive behaviour or actions
Violence: Physical
Biological
Amygdala, hypothalamus, prefrontal cortex, limbic system
Cortical dysfunction e.g. abnormal EEG
Biological
Amygdala, hypothalamus, prefrontal cortex, limbic system
Cortical dysfunction e.g. abnormal EEG
Developmental Factors Associated with Adult Violence
Abuse by parents
Truancy, school failure,
Developmental Factors Associated with Adult Violence
Abuse by parents
Truancy, school failure,
Risk Factors for Aggression or Violence
young, male
developmental factors
less education
lack of
Risk Factors for Aggression or Violence
young, male
developmental factors
less education
lack of
Risk Factors for Aggression and Violence (continued)
chronic anger towards others
recent sense
Risk Factors for Aggression and Violence (continued)
chronic anger towards others
recent sense
Predictors of Impending Violence Include:
Refusal to cooperate
Intense staring
Motor restlessness, akathysia
Purposeless movements
Labile
Predictors of Impending Violence Include:
Refusal to cooperate
Intense staring
Motor restlessness, akathysia
Purposeless movements
Labile
Management
Establish differential diagnosis
Attempt where possible to initiate treatment with medication
Management
Establish differential diagnosis
Attempt where possible to initiate treatment with medication
Choice of Medication
Consider:
speed of onset
oral vs IM
duration of action
side effects
past response
patient
Choice of Medication
Consider:
speed of onset
oral vs IM
duration of action
side effects
past response
patient
Pharmacologic Support: Benzodiazepines
Lorazepam - inthe first 24 hours agitation is as
Pharmacologic Support: Benzodiazepines
Lorazepam - inthe first 24 hours agitation is as
sedative hypnotic effect which can be additive with other such agents
sedative hypnotic effect which can be additive with other such agents
Benzodiazepines
Elderly
patients with respiratory disease
acute intoxication with alcohol
severe impairment of
Benzodiazepines
Elderly
patients with respiratory disease
acute intoxication with alcohol
severe impairment of
Midazolam
Midazolam 2 – 10 mg (IM/IV) for agitated, aggressive patients
Risk of
Midazolam
Midazolam 2 – 10 mg (IM/IV) for agitated, aggressive patients
Risk of
Clonazepam
Clonazepam (0.5 – 2 mg) is a longer acting IM alternative
Clonazepam
Clonazepam (0.5 – 2 mg) is a longer acting IM alternative
Lorazepam
Lorazepam (0.5 – 2.5 mg) -shorter half life
Onset of action 5
Lorazepam
Lorazepam (0.5 – 2.5 mg) -shorter half life
Onset of action 5
Diazepam
Diazepam (2.5 – 10 mg) is well absorbed orally
IM absorption is
Diazepam
Diazepam (2.5 – 10 mg) is well absorbed orally
IM absorption is
Pharmacologic support: Antipsychotics
effective in reducing agitation
There are options in the following
Pharmacologic support: Antipsychotics
effective in reducing agitation
There are options in the following
IM Antipsychotics
Ziprasidone (Geodon) 20mg IM q 4 hours or 10mg q
IM Antipsychotics
Ziprasidone (Geodon) 20mg IM q 4 hours or 10mg q
Haloperidol (oral / IM)
Time of Onset of action depends on route
Haloperidol (oral / IM)
Time of Onset of action depends on route
Zuclopenthixol
Zuclopenthixol HCl (Clopixol) 10, 25mg tablets
Onset of action 10-30 minutes
Peak plasma
Zuclopenthixol
Zuclopenthixol HCl (Clopixol) 10, 25mg tablets
Onset of action 10-30 minutes
Peak plasma
Acuphase (Zuclopenthixol acetate)
Acuphase (Zuclopenthixol acetate) – short acting depot used when
Acuphase (Zuclopenthixol acetate)
Acuphase (Zuclopenthixol acetate) – short acting depot used when
Second Generation Antipsychotics (SGAs)
Risperidone (tablets, depot)
Paliperidone (tablets, depot)
Olanzapine (tablets, short-acting IM)
Amisulpride
Second Generation Antipsychotics (SGAs)
Risperidone (tablets, depot)
Paliperidone (tablets, depot)
Olanzapine (tablets, short-acting IM)
Amisulpride
Second Generation Antipsychotics
For tranquilization and to reduce hostility in agitated patients
In
Second Generation Antipsychotics
For tranquilization and to reduce hostility in agitated patients
In
Medication for agitated, psychotic patients
Oral atypical antipsychotic
Oral benzodiazepine in the first
Medication for agitated, psychotic patients
Oral atypical antipsychotic
Oral benzodiazepine in the first
Parenteral Medication
If patient more agitated or unwilling to accept oral
Parenteral Medication
If patient more agitated or unwilling to accept oral
Extrapyramidal symptoms
Haldol is the most likely to cause extrapyramidal symptoms (eps)
Extrapyramidal symptoms
Haldol is the most likely to cause extrapyramidal symptoms (eps)
EPS treatment
Be ready to give O2 if breathing problems develop
PO or
EPS treatment
Be ready to give O2 if breathing problems develop
PO or
Our patient story evolves
On interview pt stated he took “a
Our patient story evolves
On interview pt stated he took “a
First things first
Make sure he is safe in the current
First things first
Make sure he is safe in the current
Suicidality and suicide
Suicide- the act of self- murder
Suicidality- thoughts, preoccupations, drives
Suicidality and suicide
Suicide- the act of self- murder
Suicidality- thoughts, preoccupations, drives
Epidemiology
1 completed suicede: 25 attempts
Males are X4 successful than females, use
Epidemiology
1 completed suicede: 25 attempts
Males are X4 successful than females, use
Self harm
X38 risk after any previous attempt
Mainly ½ year after
1% of
Self harm
X38 risk after any previous attempt
Mainly ½ year after
1% of
Risk factors
M
45y<
A letter
Previous attempts
lonely
In conflict
Any psychiatric diagnosis
Chronic pain and disability
Cancer, epilepsy,
Risk factors
M
45y<
A letter
Previous attempts
lonely
In conflict
Any psychiatric diagnosis
Chronic pain and disability
Cancer, epilepsy,
Psychiatric factors
At least 1 ps. diagnosis
22% in the first year after
Psychiatric factors
At least 1 ps. diagnosis
22% in the first year after


Protective factors
Faith
Parenthood, family
Responsibility
Optimism
Fear
Social embarassement
Morality
Support
Plans for future
Protective factors
Faith
Parenthood, family
Responsibility
Optimism
Fear
Social embarassement
Morality
Support
Plans for future
Suicide assessment
Ideation- acute vs. chronic, passive vs. active- if active
Suicide assessment
Ideation- acute vs. chronic, passive vs. active- if active
Suicide assessment cont.
Clinical factors: Personal history of suicide attempt, substance use,
Suicide assessment cont.
Clinical factors: Personal history of suicide attempt, substance use,
Is it possible to predict suicide?
Impossible!
Possible to access the immediate risk
Is it possible to predict suicide?
Impossible!
Possible to access the immediate risk
Managing the suicidal patient
Ensure safety
Anamnesys and collateral hystory
Don’t afraid to directly
Managing the suicidal patient
Ensure safety
Anamnesys and collateral hystory
Don’t afraid to directly
Acute management
Treatment plan
Remove the means
Address the crisis
Treat intoxication
Relieve pain
If suicidal but
Acute management
Treatment plan
Remove the means
Address the crisis
Treat intoxication
Relieve pain
If suicidal but
Serotonin syndrome
Rapid onset of symptoms
60% present within 6 hours after initial
Serotonin syndrome
Rapid onset of symptoms
60% present within 6 hours after initial
Drug interactions associated with severe serotonin syndrome
Phenelzine and meperidine
Tranylcypromine and imipramine
Phenelzine
Drug interactions associated with severe serotonin syndrome
Phenelzine and meperidine
Tranylcypromine and imipramine
Phenelzine
Diagnosis : Classic triad
Mental status changes: confusion, restlessness, agitation, anxiety, decreased
Diagnosis : Classic triad
Mental status changes: confusion, restlessness, agitation, anxiety, decreased
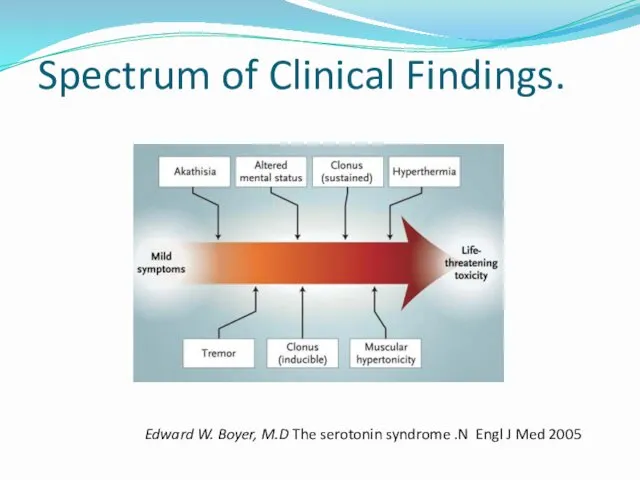
Spectrum of Clinical Findings.
Edward W. Boyer, M.D The serotonin syndrome .N
Spectrum of Clinical Findings.
Edward W. Boyer, M.D The serotonin syndrome .N
Treatment
Discontinuation of all serotonergic agents
Supportive care, many do not require tx
Consult
Treatment
Discontinuation of all serotonergic agents
Supportive care, many do not require tx
Consult
Sexual abuse- PREVALENCE
Sexual assault is one of the most under reported
Sexual abuse- PREVALENCE
Sexual assault is one of the most under reported
Victims of sexual assault are:
3 times more likely to suffer from
Victims of sexual assault are:
3 times more likely to suffer from
Rape is NEVER the victim’s fault!
Rape is an act of violence
Rape is NEVER the victim’s fault!
Rape is an act of violence

UNIQUENESS OF SEXUAL VIOLENCE AS A CRIMINAL VIOLATION
The violation of “self”
UNIQUENESS OF SEXUAL VIOLENCE AS A CRIMINAL VIOLATION
The violation of “self”
TWO MOST COMMON RESPONSES
IMMEDIALEY FOLLOWING RAPE
Expressed
demonstrating anger, fear, and anxiety
TWO MOST COMMON RESPONSES
IMMEDIALEY FOLLOWING RAPE
Expressed
demonstrating anger, fear, and anxiety
Symptoms of Survivors (both female and male)
Nightmares / sleep disturbances
Substance Abuse
Panic
Symptoms of Survivors (both female and male)
Nightmares / sleep disturbances
Substance Abuse
Panic
Disassociation (zoning out)
Anorexia / Bulimia / Overeating (Eating disorders)
“Cutting” /
Anorexia / Bulimia / Overeating (Eating disorders)
“Cutting” /
guilt – confusion – sexual identity issues
Extreme independence/isolation
Triggers / Sights,
guilt – confusion – sexual identity issues
Extreme independence/isolation
Triggers / Sights,
Is alcohol a date rape drug?
Any drug that can affect
Is alcohol a date rape drug?
Any drug that can affect
ROHYPNOL a.k.a. “roofies”
Rohypnol (roh-HIP-nol). Rohypnol is the trade name for flunitrazepam
ROHYPNOL a.k.a. “roofies”
Rohypnol (roh-HIP-nol). Rohypnol is the trade name for flunitrazepam
GHB - GAMMA HYDROXY BUTYRATE
GHB is a central nervous system depressant
GHB - GAMMA HYDROXY BUTYRATE
GHB is a central nervous system depressant
ECSTASY
While not classified as a “date rape drug”, many
ECSTASY
While not classified as a “date rape drug”, many
SUBSTANCE ABUSING SURVIVORS
75% of men and 55% of women involved in
SUBSTANCE ABUSING SURVIVORS
75% of men and 55% of women involved in
Substance Abuse
Two to three times more common among those with psychiatric
Substance Abuse
Two to three times more common among those with psychiatric
Common Substances of Abuse
Alcohol
Cocaine
Amphetamine
Methamphetamine
MDMA (3,4 methylene dioxymethamphetamine), (ecstasy)
Ketamine
Cannabis
Opiates
A/Professor David Ash
Common Substances of Abuse
Alcohol
Cocaine
Amphetamine
Methamphetamine
MDMA (3,4 methylene dioxymethamphetamine), (ecstasy)
Ketamine
Cannabis
Opiates
A/Professor David Ash
The Drug Abusing Patient
Patient may present with intoxication or withdrawal symptom
Stimulant
The Drug Abusing Patient
Patient may present with intoxication or withdrawal symptom
Stimulant
Amphetamine – Methamphetamine Abuse
Clinical Presentation:
Acute anxiety
Paranoid ideation
Loud, demanding behaviour
Motor agitation, aggression
Stereotypic
Amphetamine – Methamphetamine Abuse
Clinical Presentation:
Acute anxiety
Paranoid ideation
Loud, demanding behaviour
Motor agitation, aggression
Stereotypic
 Шаблоны Школьные
Шаблоны Школьные Числа от 1 до 100. Умножение и деление
Числа от 1 до 100. Умножение и деление ТУРГЕНЕВ ОТЦЫ БАЗАРОВ И РОДИТЕЛИ 2
ТУРГЕНЕВ ОТЦЫ БАЗАРОВ И РОДИТЕЛИ 2 Судовое вспомогательное энергооборудование
Судовое вспомогательное энергооборудование Традиции, обычаи воспитания казаков
Традиции, обычаи воспитания казаков Німеччина (ФРН), утворення ФРН 23 травня 1949
Німеччина (ФРН), утворення ФРН 23 травня 1949 Виды и рода войск Российской федерации
Виды и рода войск Российской федерации Северная Америка
Северная Америка Системы обеспечения безопасности движения
Системы обеспечения безопасности движения Виды условных знаков. Виды карт по содержанию
Виды условных знаков. Виды карт по содержанию Рафаэль Санти
Рафаэль Санти Презентация Христос и Его крест
Презентация Христос и Его крест ) Жизнь на материках
) Жизнь на материках Разработка занятия по технике изонить. Первые шаги - угол.
Разработка занятия по технике изонить. Первые шаги - угол. Анонимные Наркоманы. Служение больницы и учреждения. Исправительные учреждения
Анонимные Наркоманы. Служение больницы и учреждения. Исправительные учреждения урок - кроссворд
урок - кроссворд Организация видов работ при эксплуатации и реконструкции строительных объектов
Организация видов работ при эксплуатации и реконструкции строительных объектов Урок технологии в малокомплектной сельской школе Изготовление домашних оберегов
Урок технологии в малокомплектной сельской школе Изготовление домашних оберегов Қазақтың сүт өнімдері. Сүт өнімдерінің адам ағзасына пайдасы
Қазақтың сүт өнімдері. Сүт өнімдерінің адам ағзасына пайдасы Базовые эмоции
Базовые эмоции Наноспутники в системе космической радиосвязи
Наноспутники в системе космической радиосвязи Балалардағы жүрек ырғағының бұзылысы
Балалардағы жүрек ырғағының бұзылысы ИСПОЛЬЗОВАНИЕ СИСТЕМНОГО ПОДХОДА КЛАССНОГО РУКОВОДИТЕЛЯ К ЗДОРОВЬЕСБЕРЕГАЮЩЕЙ ДЕЯТЕЛЬНОСТИ ЧЕРЕЗ ПРОЕКТ НАШЕ ЗДОРОВЬЕ
ИСПОЛЬЗОВАНИЕ СИСТЕМНОГО ПОДХОДА КЛАССНОГО РУКОВОДИТЕЛЯ К ЗДОРОВЬЕСБЕРЕГАЮЩЕЙ ДЕЯТЕЛЬНОСТИ ЧЕРЕЗ ПРОЕКТ НАШЕ ЗДОРОВЬЕ Лечение болевого синдрома у онкологических пациентов в педиатрии
Лечение болевого синдрома у онкологических пациентов в педиатрии презентация: Здоровые дети - здоровая страна
презентация: Здоровые дети - здоровая страна Николай Николаевич Носов
Николай Николаевич Носов Презентация. Игра на тему Этикет
Презентация. Игра на тему Этикет Библия и Евангелие
Библия и Евангелие