- Митральды стенозы бар науқастарда кораксан мен карведилолдың физикалық әсерін

Содержание
- 2. Митральды стеноз - сол жақ жүрекше мен қарынша арасындағы атриовентрикулярлы тесіктің тарылуымен сипатталады. Барлық жүре пайда
- 3. Карведилол – альфа және бетта блокатор болып табылады.Тамыр кеңейткіш әсері бар,жүрекке күш түсуді азайтады.Қандағы ренин мөлшерін
- 4. Мақсаты Митральды стенозы бар науқастарда Кораксан мен Карведилолдың физикалық жүктемені көтеруге әсерін салыстыру
- 5. Сұрақ: 45-70 жас аралығындағы митральды стенозы бар науқастарда Кораксан 5 мг күніне 2 рет 6 апта
- 6. PICO P- 45-70 жас аралығындағы митральды стенозы бар наукастар I- Кораксан 5 мг күніне 2 рет
- 7. Тапсырма Зерттеуге жүрек жеткіліксіздігі бар 45-70 жас аралығындағы науқастарды алу Екі топқа бөлу: бақылау тобы карведилол
- 8. Дизайн: - екі жақты жасырын РБЗ Таңдау : қарапайым кездейсоқ таңдау Енгізу критерийі: 19-45 жас аралығындағы
- 9. Этикалық аспекті Этикалық комитетпен рұқсат етілді. Зерттеу жүргізуге жазбаша түрде ақпараттық келісім алынды. Пациенттер кез келген
- 10. Effect of Combining Сoraxane and β-Blockers: Focus on the Use of Carvedilol in the SHIFT Population.
- 11. Сұрақ: 55-70 жас аралығындағы Созылмалы жүрек жеткіліксіздігі бар науқастарда Кораксанды 5 мг күніне 2 рет қолдану
- 12. PICO P- 55-70 жас аралығындағы созылмалы жүрек жеткіліксіздігі бар науқастар I- Кораксанды 5 мг күніне 2
- 13. Зерттеу жобасы: Дизайн: описание серии случаев Таңдау : типтік таңдау Енгізу критерийі: 65-80 жас аралығындағы Созылмалы
- 14. Пайдаланған әдебиеттер: https://pubchem.ncbi.nlm.nih.gov/compound/132999#section=Top https://health.mail.ru/drug/koraksan_1/ Беленков Ю.Н Хроническая сердечная недостаточность. ГЭОТАР-Медиа,2006г Дземешкевич С.Л :Дисфункций миокарда и сердечная
- 16. Скачать презентацию
Митральды стеноз - сол жақ жүрекше мен қарынша арасындағы атриовентрикулярлы тесіктің
Митральды стеноз - сол жақ жүрекше мен қарынша арасындағы атриовентрикулярлы тесіктің
Карведилол – альфа және бетта блокатор болып табылады.Тамыр кеңейткіш әсері бар,жүрекке
Карведилол – альфа және бетта блокатор болып табылады.Тамыр кеңейткіш әсері бар,жүрекке
Мақсаты
Митральды стенозы бар науқастарда Кораксан мен Карведилолдың физикалық жүктемені көтеруге әсерін
Мақсаты
Митральды стенозы бар науқастарда Кораксан мен Карведилолдың физикалық жүктемені көтеруге әсерін
Сұрақ:
45-70 жас аралығындағы митральды стенозы бар науқастарда Кораксан 5 мг күніне
Сұрақ:
45-70 жас аралығындағы митральды стенозы бар науқастарда Кораксан 5 мг күніне
PICO
P- 45-70 жас аралығындағы митральды стенозы бар наукастар
I- Кораксан 5 мг
PICO
P- 45-70 жас аралығындағы митральды стенозы бар наукастар
I- Кораксан 5 мг
Тапсырма
Зерттеуге жүрек жеткіліксіздігі бар 45-70 жас аралығындағы науқастарды алу
Екі топқа бөлу:
Тапсырма
Зерттеуге жүрек жеткіліксіздігі бар 45-70 жас аралығындағы науқастарды алу
Екі топқа бөлу:
Дизайн:
- екі жақты жасырын РБЗ
Таңдау : қарапайым кездейсоқ таңдау
Енгізу критерийі:
19-45
Дизайн:
- екі жақты жасырын РБЗ
Таңдау : қарапайым кездейсоқ таңдау
Енгізу критерийі:
19-45
Этикалық аспекті
Этикалық комитетпен рұқсат етілді.
Зерттеу жүргізуге жазбаша түрде ақпараттық келісім алынды.
Пациенттер
Этикалық аспекті
Этикалық комитетпен рұқсат етілді.
Зерттеу жүргізуге жазбаша түрде ақпараттық келісім алынды.
Пациенттер
Effect of Combining Сoraxane and β-Blockers: Focus on the Use of Carvedilol
Effect of Combining Сoraxane and β-Blockers: Focus on the Use of Carvedilol
Сұрақ:
55-70 жас аралығындағы Созылмалы жүрек жеткіліксіздігі бар науқастарда Кораксанды 5 мг
Сұрақ:
55-70 жас аралығындағы Созылмалы жүрек жеткіліксіздігі бар науқастарда Кораксанды 5 мг
PICO
P- 55-70 жас аралығындағы созылмалы жүрек жеткіліксіздігі бар науқастар
I- Кораксанды 5
PICO
P- 55-70 жас аралығындағы созылмалы жүрек жеткіліксіздігі бар науқастар
I- Кораксанды 5
Зерттеу жобасы:
Дизайн:
описание серии случаев
Таңдау : типтік таңдау
Енгізу критерийі:
65-80 жас аралығындағы
Зерттеу жобасы:
Дизайн:
описание серии случаев
Таңдау : типтік таңдау
Енгізу критерийі:
65-80 жас аралығындағы
Пайдаланған әдебиеттер:
https://pubchem.ncbi.nlm.nih.gov/compound/132999#section=Top
https://health.mail.ru/drug/koraksan_1/
Беленков Ю.Н Хроническая сердечная недостаточность. ГЭОТАР-Медиа,2006г
Дземешкевич С.Л :Дисфункций миокарда и
Пайдаланған әдебиеттер:
https://pubchem.ncbi.nlm.nih.gov/compound/132999#section=Top
https://health.mail.ru/drug/koraksan_1/
Беленков Ю.Н Хроническая сердечная недостаточность. ГЭОТАР-Медиа,2006г
Дземешкевич С.Л :Дисфункций миокарда и
 Проектная деятельность как составная часть современного образования
Проектная деятельность как составная часть современного образования Источники права
Источники права Современные строительные технологии
Современные строительные технологии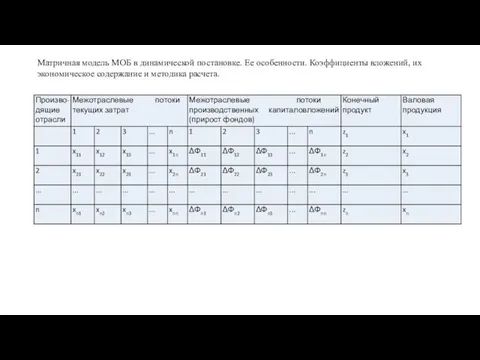 Матричная модель МОБ в динамической постановке
Матричная модель МОБ в динамической постановке Христианство. Основные направления христианства – сравнительная характеристика
Христианство. Основные направления христианства – сравнительная характеристика Любимые игрушки. Лепка из пластилина
Любимые игрушки. Лепка из пластилина Реконструкция электрооборудования многоквартирного жилого дома
Реконструкция электрооборудования многоквартирного жилого дома Системы электронного документооборота
Системы электронного документооборота Наблюдение за состоянием пациентов и интенсивная терапия, во время анестезии
Наблюдение за состоянием пациентов и интенсивная терапия, во время анестезии Оперативная память
Оперативная память Блокада Ленинграда Диск
Блокада Ленинграда Диск Нефтегазоность Севернего Устюрта
Нефтегазоность Севернего Устюрта Формирование комфортной городской среды
Формирование комфортной городской среды Комплексная безопасность информационных систем. Асимметричные алгоритмы шифрования. (Лекция 8)
Комплексная безопасность информационных систем. Асимметричные алгоритмы шифрования. (Лекция 8) Food
Food История дорожного движения
История дорожного движения Презентация балет Щелкунчик П.И.Чайковский
Презентация балет Щелкунчик П.И.Чайковский презентация к занятию В гости к зайке
презентация к занятию В гости к зайке Дягилев
Дягилев Презентация MsPP Дни воинской славы России, часть 2
Презентация MsPP Дни воинской славы России, часть 2 Категорія числа іменників
Категорія числа іменників Космический КВН (презентация)
Космический КВН (презентация) Циркуляция вектора напряженности вихревого электрического поля
Циркуляция вектора напряженности вихревого электрического поля По следам рудознатцев
По следам рудознатцев КЛАССНЫЙ ЧАС
КЛАССНЫЙ ЧАС Zarządzanie procesami
Zarządzanie procesami Рибні консерви і ікра риб
Рибні консерви і ікра риб Австро-Венгрия в XIX - начале XX века
Австро-Венгрия в XIX - начале XX века