- Erysipelas

Содержание
- 2. Definition of the Disease Erysipelas – human infectious disease of streptococcal etiology, with acute and chronic
- 3. Etiologic Peculiarities 1. In primary and recurring erysipelas with exogenic route of transmission the cause of
- 4. Etiologic Peculiarities (continued) 2. In relapsing and particularly frequently relapsing erysipelas the etiological cause are the
- 5. Laboratory diagnosis 1. Detection of antigenemia: = А-polysaccaride (А-PSC) = protein-ribosomal antigens (PR-Аg) = L-form antigens
- 6. Epidemiological peculiarities 1. In primary, recurrent, rarely relapsing erysipelas the source of infection are patients with
- 7. Epidemiological peculiarities (continued) 2. In frequently relapsing erysipelas - only endogenous mechanism of infection – reversion
- 8. Epidemiological peculiarities (continued) 3. Vulnerability depends on basic immune status condition and the virulence of the
- 9. Pathogenesis 1. Permeation of the streptococcus into the skin. 2. Reproduction of bacteria in the lymphatic
- 10. Pathogenic features of frequently relapsing erysipelas: 1. Forming of the resistant locus of streptococcal infection in
- 11. Predisposing factors 1. Concomitant diseases – plantar mycosis, diabetes mellitus, obesity, chronic venous insufficiency, lymphostasis, trophic
- 12. There are two main components in the pathogenesis of erysipelas: 1. Infectious-toxic (toxins, transient bacteriemia, secretion
- 13. Clinical classification of erysipelas 1. By frequency: = Primary = Recurrent = Relapsing 2. By the
- 14. Clinical classification of erysipelas (continued) 3. By severity: = mild = moderate = severe 4. By
- 15. Examples of the clinical diagnosis 1. Primary erysipelas of the left shank erythematous form moderate severity.
- 16. Evolution of the erysipelas clinical features 1. More older people (60 year old and older) –
- 17. Clinical features of erysipelas 1. Acute onset of the disease. 2. Intoxication syndrome is usually ahead
- 18. Clinical features of erysipelas (continued) 3. Early signs of the disease before the local changes can
- 19. Clinical features of erysipelas (continued) 3. Local process is characterised by sharply circumscribed hyperemia with the
- 20. Clinical features of erysipelas (continued) 4. Local process is associated with lymphatic edema of various degree
- 21. Erysipelas of the face (EB form)
- 22. Erysipelas of the face (Erythem. form) After recovery (peeling)
- 23. Erythematous-bullous form Pigmentation and peeling (recovery)
- 24. Elephantiasis (outcome)
- 25. Diagnosis Main method – clinical and anamnesis. Differential diagnosis: With infectious diseases (skin form of anthrax,
- 26. Ethiotropic therapy 1. In primary and recurrent erysipelas penicillin is the antibiotic of choice – 5-6
- 27. Pathogenetic therapy 1. Detoxication therapy – oral (enterodez, regidron etc.); parenteral – crystalloids (polyionic solutions: trisol,
- 28. Pathogenetic therapy (continued) 4. Immunocorrection with the control of the immune status (immunoglobulines IV and IM,
- 29. Local treatment 1. Do not touch (!) erythematous forms. 2. Vishnevsky ointment and ichtiolic ointment are
- 30. Ambulatory monitoring 1. Finishing treatment 2. Sanation of the chronic focuses of infection 3. Relapse prophylaxis:
- 32. Скачать презентацию
Definition of the Disease
Erysipelas – human infectious disease of streptococcal etiology,
Definition of the Disease
Erysipelas – human infectious disease of streptococcal etiology,
Etiologic Peculiarities
1. In primary and recurring erysipelas with exogenic route of
Etiologic Peculiarities
1. In primary and recurring erysipelas with exogenic route of
Etiologic Peculiarities (continued)
2. In relapsing and particularly frequently relapsing erysipelas the
Etiologic Peculiarities (continued)
2. In relapsing and particularly frequently relapsing erysipelas the
Laboratory diagnosis
1. Detection of antigenemia:
= А-polysaccaride (А-PSC)
= protein-ribosomal antigens
Laboratory diagnosis
1. Detection of antigenemia:
= А-polysaccaride (А-PSC)
= protein-ribosomal antigens
Epidemiological peculiarities
1. In primary, recurrent, rarely relapsing erysipelas the source of
Epidemiological peculiarities
1. In primary, recurrent, rarely relapsing erysipelas the source of
Epidemiological peculiarities (continued)
2. In frequently relapsing erysipelas - only endogenous mechanism
Epidemiological peculiarities (continued)
2. In frequently relapsing erysipelas - only endogenous mechanism
Epidemiological peculiarities (continued)
3. Vulnerability depends on basic immune status condition and
Epidemiological peculiarities (continued)
3. Vulnerability depends on basic immune status condition and
Pathogenesis
1. Permeation of the streptococcus into the skin.
2. Reproduction of bacteria
Pathogenesis
1. Permeation of the streptococcus into the skin.
2. Reproduction of bacteria
Pathogenic features of frequently relapsing erysipelas:
1. Forming of the resistant locus
Pathogenic features of frequently relapsing erysipelas:
1. Forming of the resistant locus
Predisposing factors
1. Concomitant diseases – plantar mycosis, diabetes mellitus, obesity, chronic
Predisposing factors
1. Concomitant diseases – plantar mycosis, diabetes mellitus, obesity, chronic
There are two main components in the pathogenesis of erysipelas:
1. Infectious-toxic
There are two main components in the pathogenesis of erysipelas:
1. Infectious-toxic
Clinical classification of erysipelas
1. By frequency:
= Primary
= Recurrent
=
Clinical classification of erysipelas
1. By frequency:
= Primary
= Recurrent
=
Clinical classification of erysipelas (continued)
3. By severity:
= mild
= moderate
Clinical classification of erysipelas (continued)
3. By severity:
= mild
= moderate
Examples of the clinical diagnosis
1. Primary erysipelas of the left shank
Examples of the clinical diagnosis
1. Primary erysipelas of the left shank
Evolution of the erysipelas clinical features
1. More older people (60 year
Evolution of the erysipelas clinical features
1. More older people (60 year
Clinical features of erysipelas
1. Acute onset of the disease.
2. Intoxication syndrome
Clinical features of erysipelas
1. Acute onset of the disease.
2. Intoxication syndrome
Clinical features of erysipelas (continued)
3. Early signs of the disease before
Clinical features of erysipelas (continued)
3. Early signs of the disease before
Clinical features of erysipelas (continued)
3. Local process is characterised by sharply
Clinical features of erysipelas (continued)
3. Local process is characterised by sharply
Clinical features of erysipelas (continued)
4. Local process is associated with lymphatic
Clinical features of erysipelas (continued)
4. Local process is associated with lymphatic
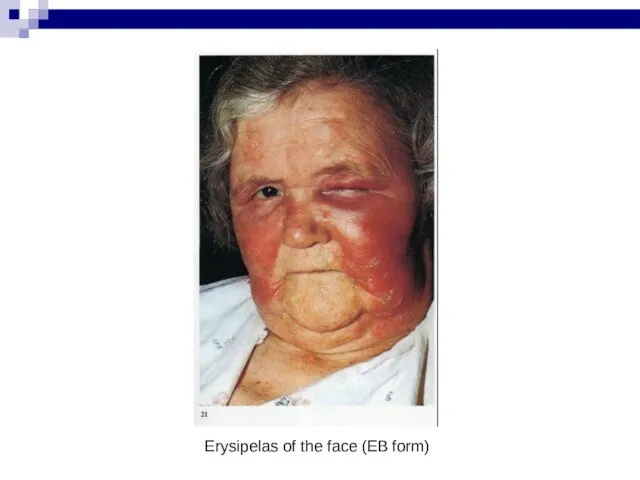
Erysipelas of the face (EB form)
Erysipelas of the face (EB form)
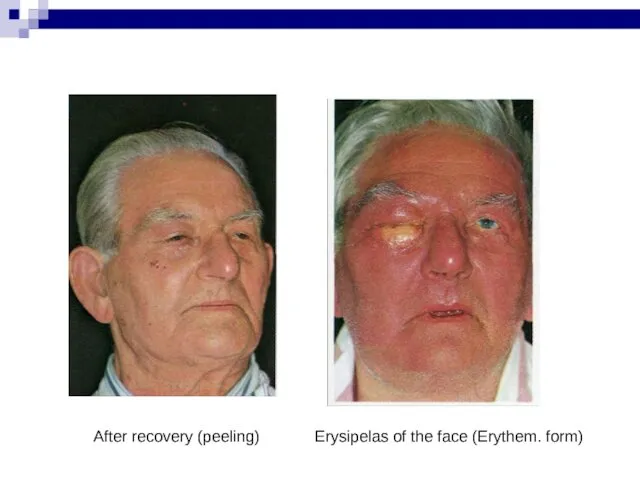
Erysipelas of the face (Erythem. form)
After recovery (peeling)
Erysipelas of the face (Erythem. form)
After recovery (peeling)

Erythematous-bullous form
Pigmentation and peeling (recovery)
Erythematous-bullous form
Pigmentation and peeling (recovery)

Elephantiasis (outcome)
Elephantiasis (outcome)
Diagnosis
Main method – clinical and anamnesis.
Differential diagnosis:
With infectious diseases (skin form
Diagnosis
Main method – clinical and anamnesis.
Differential diagnosis:
With infectious diseases (skin form
Ethiotropic therapy
1. In primary and recurrent erysipelas penicillin is the antibiotic
Ethiotropic therapy
1. In primary and recurrent erysipelas penicillin is the antibiotic
Pathogenetic therapy
1. Detoxication therapy – oral (enterodez, regidron etc.); parenteral –
Pathogenetic therapy
1. Detoxication therapy – oral (enterodez, regidron etc.); parenteral –
Pathogenetic therapy (continued)
4. Immunocorrection with the control of the immune status
Pathogenetic therapy (continued)
4. Immunocorrection with the control of the immune status
Local treatment
1. Do not touch (!) erythematous forms.
2. Vishnevsky ointment and
Local treatment
1. Do not touch (!) erythematous forms.
2. Vishnevsky ointment and
Ambulatory monitoring
1. Finishing treatment
2. Sanation of the chronic focuses of infection
3.
Ambulatory monitoring
1. Finishing treatment
2. Sanation of the chronic focuses of infection
3.
 Australian block. Test
Australian block. Test Learning to write letters
Learning to write letters Цвета. Словарь
Цвета. Словарь Party animals
Party animals Английский язык – нисходящая интонация
Английский язык – нисходящая интонация Modal Verbs
Modal Verbs Муж - husband. Unit 3
Муж - husband. Unit 3 Sharks
Sharks Regular verbs
Regular verbs Go Getter 2
Go Getter 2 Body
Body Mobile phones in schools
Mobile phones in schools Profession is a logistician
Profession is a logistician British tea
British tea Adverb. The role of an adverb
Adverb. The role of an adverb Английский язык и его значимость в мире
Английский язык и его значимость в мире Определение перевода. Предмет и объект теории перевода
Определение перевода. Предмет и объект теории перевода Global problems of today
Global problems of today Spotlight C14-16
Spotlight C14-16 Past continuous. Прошедшее продолженное время
Past continuous. Прошедшее продолженное время Motorola mobility
Motorola mobility Basketball
Basketball Sweden national dish. Meat boals
Sweden national dish. Meat boals My family and I. Lesson 1
My family and I. Lesson 1 Условные предложения в английском языке. Conditionals
Условные предложения в английском языке. Conditionals Компетентісно-орієнтоване навчання англійської мови
Компетентісно-орієнтоване навчання англійської мови Why is English so popular
Why is English so popular Letter
Letter