- Introduction to the Practice of Medicine - II

Содержание
- 2. Examination of the Abdomen Session Objectives: Describe relevant anatomy and physiology as it pertains to the
- 3. Examination of the Abdomen Introduction: The Medical History is an account of the events in the
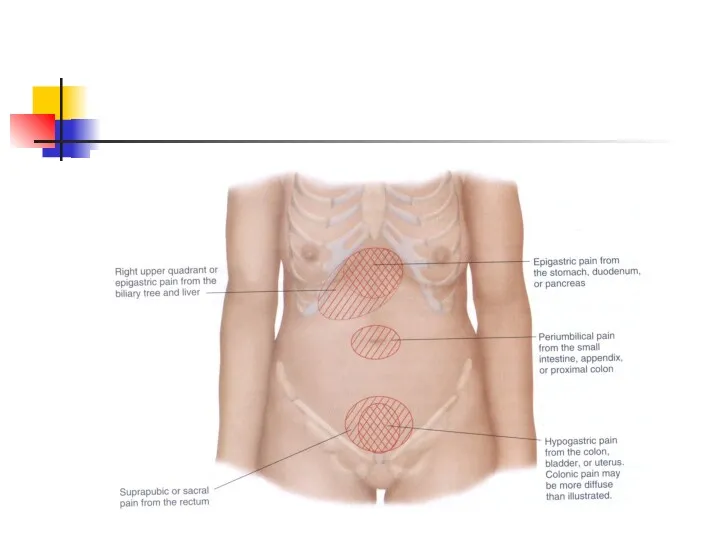
- 4. Examination of the Abdomen Pain is a common symptom of diseases of the abdomen It is
- 5. Examination of the Abdomen Important aspects of abdominal pain: Location and radiation of pain Character of
- 6. Examination of the Abdomen Important related symptoms/signs in patients with abdominal pain: Fever/rigors/sweats Nausea/vomiting Weight loss
- 7. Examination of the Abdomen Physical Examination: The PE of the abdomen must be performed in an
- 8. Examination of the Abdomen Physical Examinationof the Abdomen is conducted in four parts Inspection/observation Auscultation Percussion
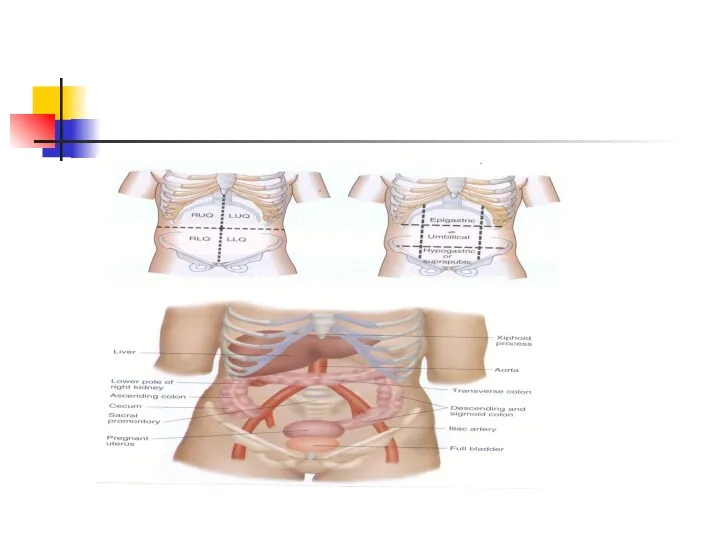
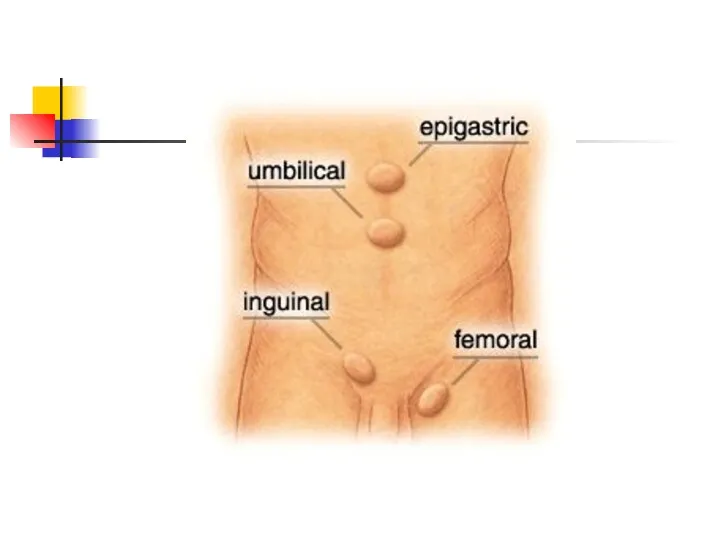
- 11. Examination of the Abdomen For descriptive purposes, the abdomen is divided into four quadrants RUQ,LUQ,RLQ,LLQ Epigastric,umbilical,
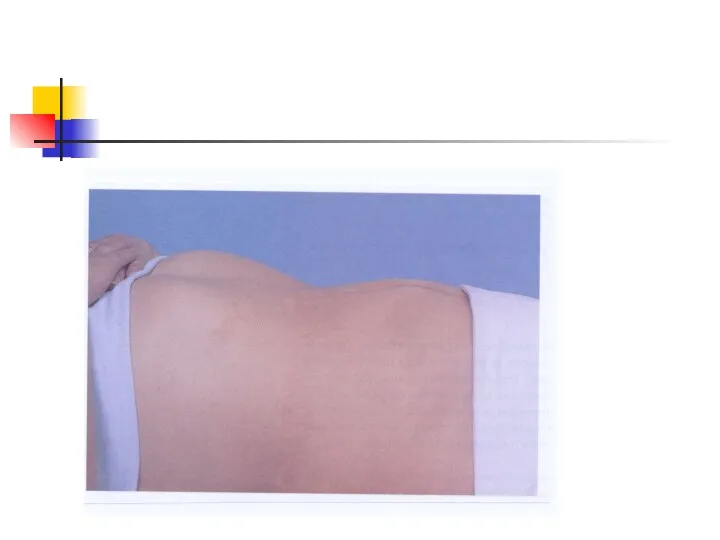
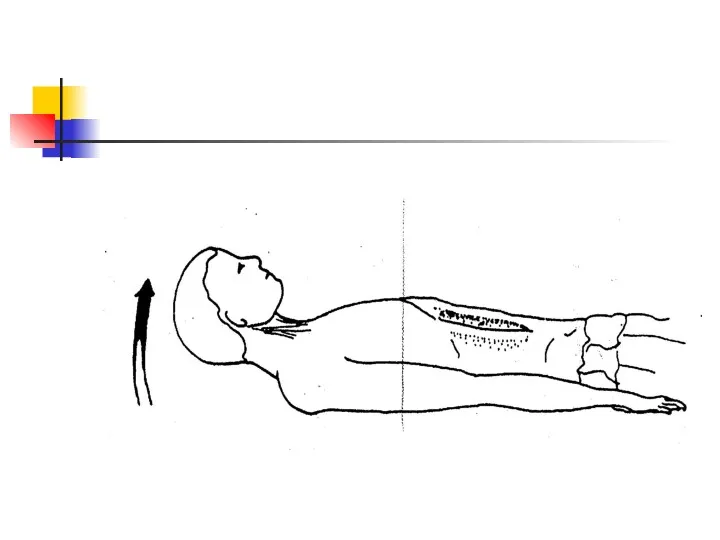
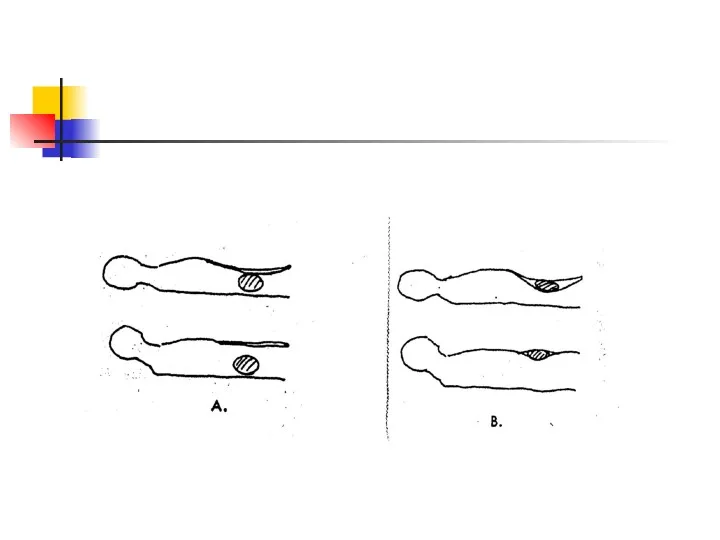
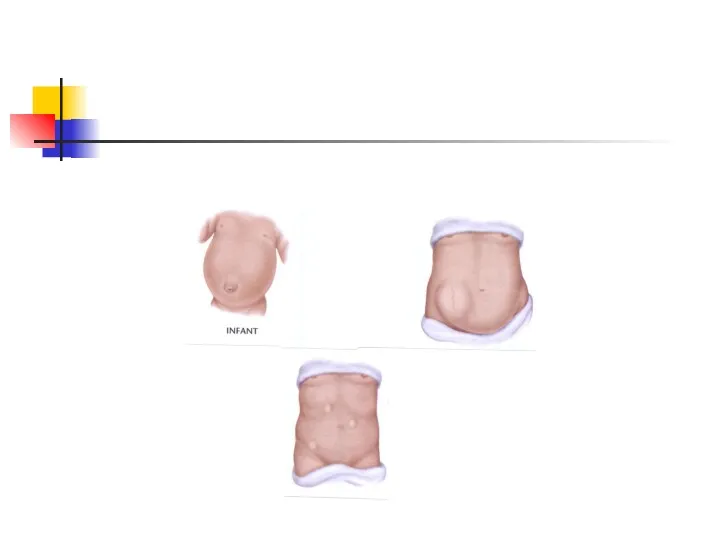
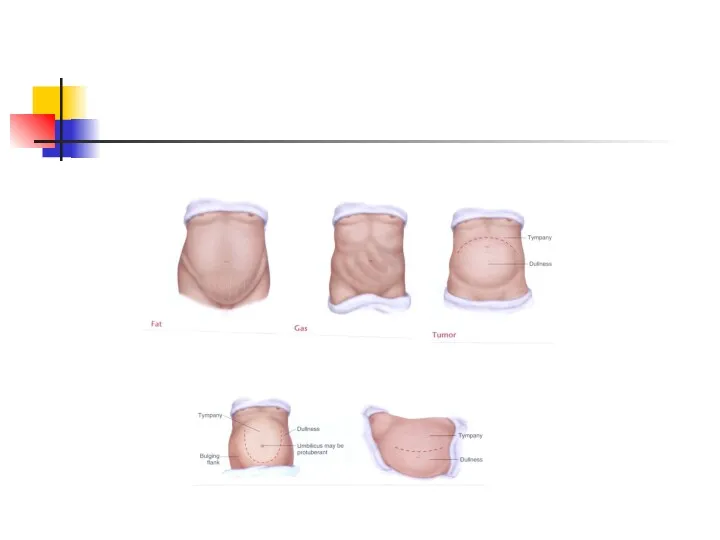
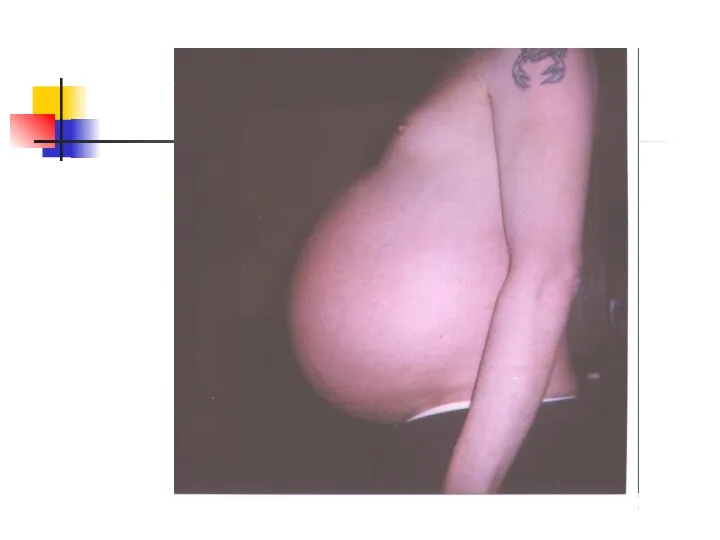
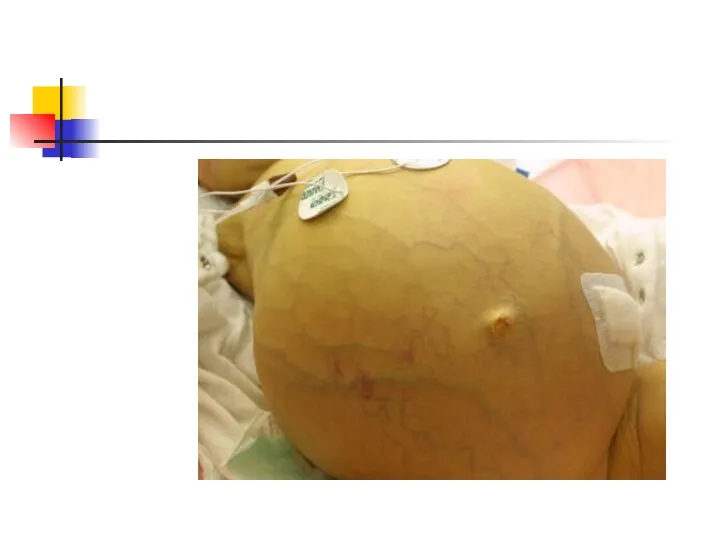
- 14. Examination of the Abdomen Inspection/Observation (#40) Inspect the contour of the abdomen. It may be flat,
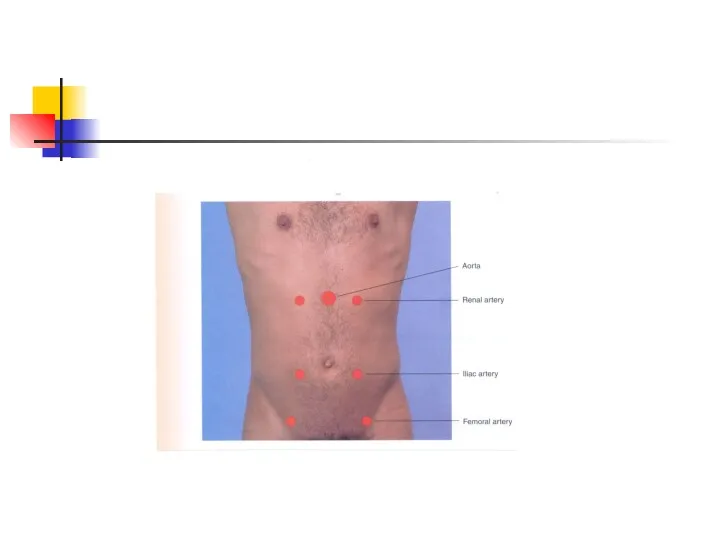
- 16. Examination of the Abdomen Auscultation (#41) Useful in assessing bowel motility and vascular bruits Note frequency/character
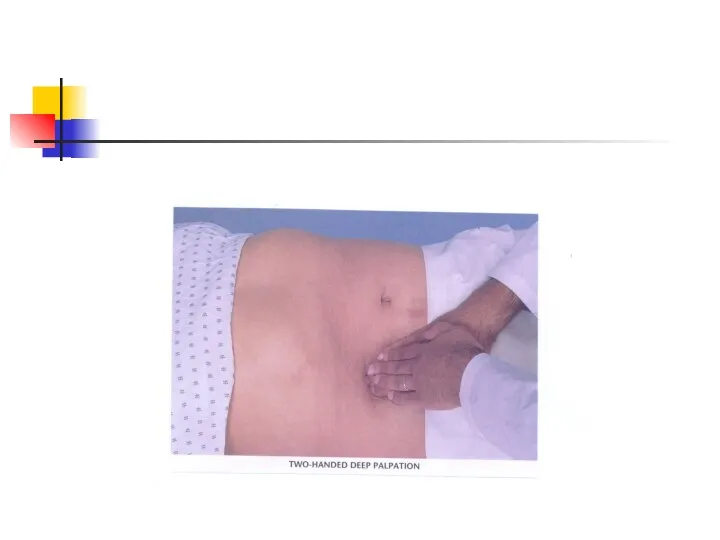
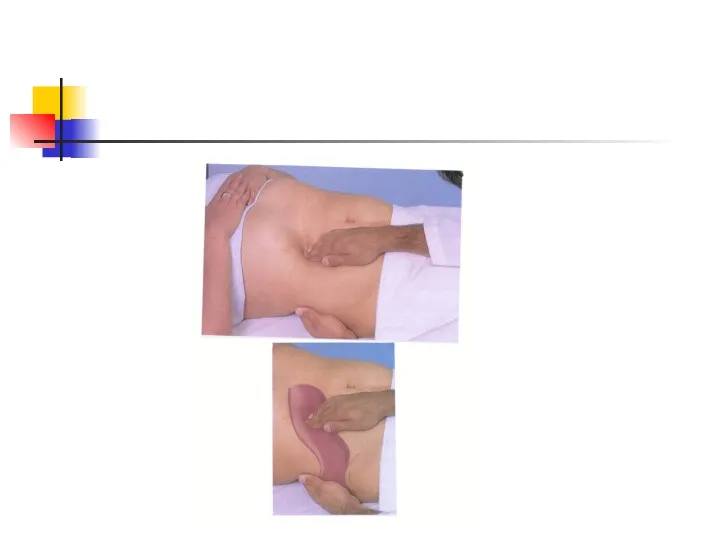
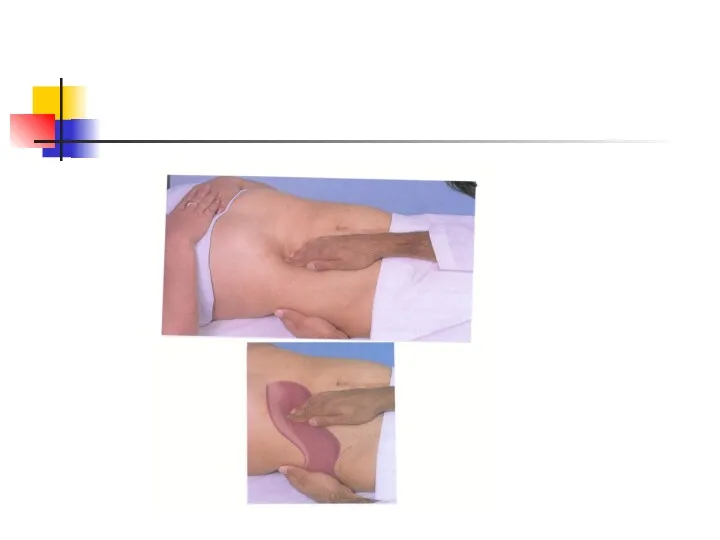
- 18. Examination of the Abdomen Palpation (#43-#50) Palpate lightly then deeply in all four quadrants Differentiate between
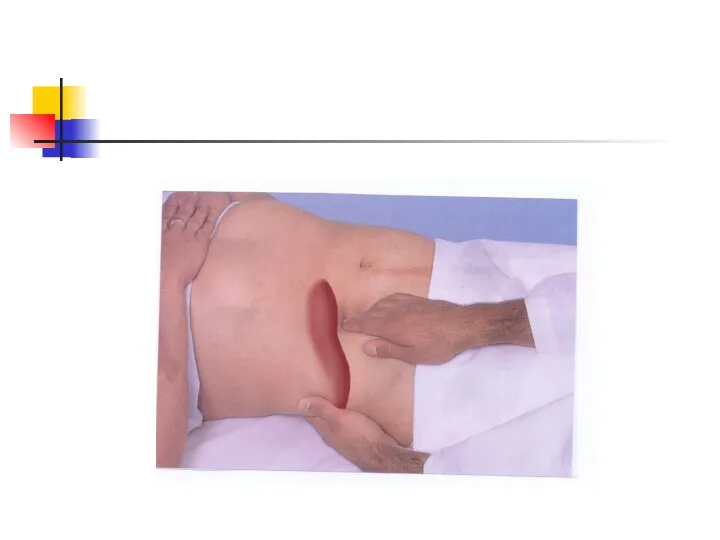
- 21. Examination of the Abdomen Palpation (#43-#50) cont’d Assess peritoneal irritation and rebound tenderness Palpate liver, spleen,
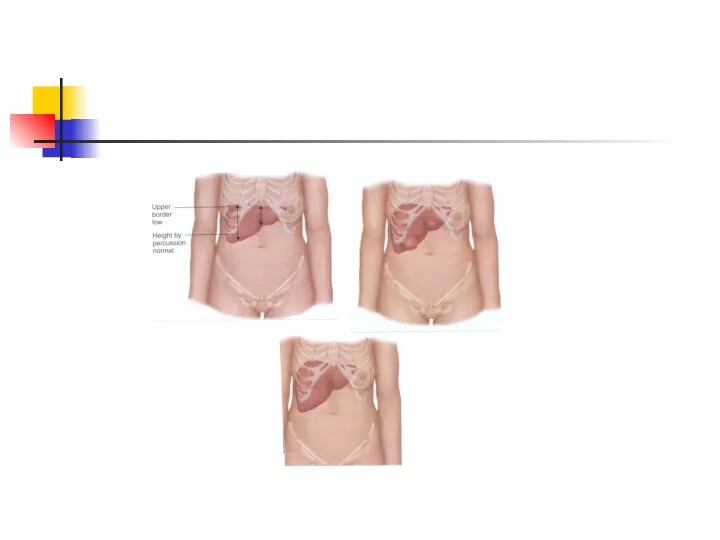
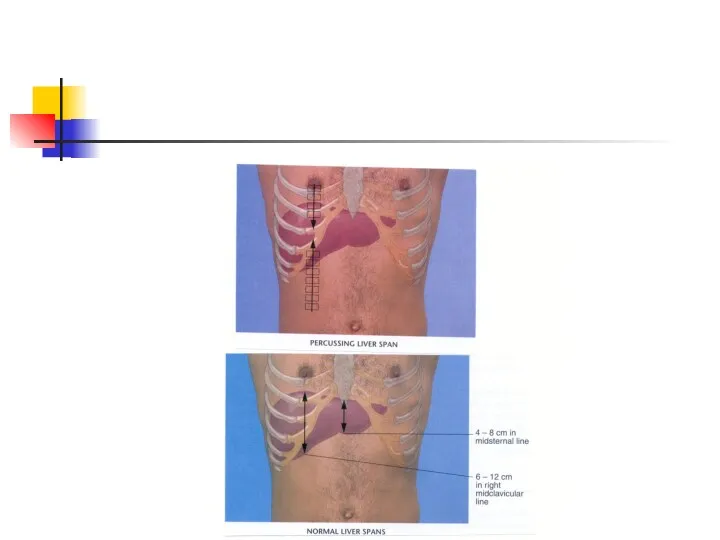
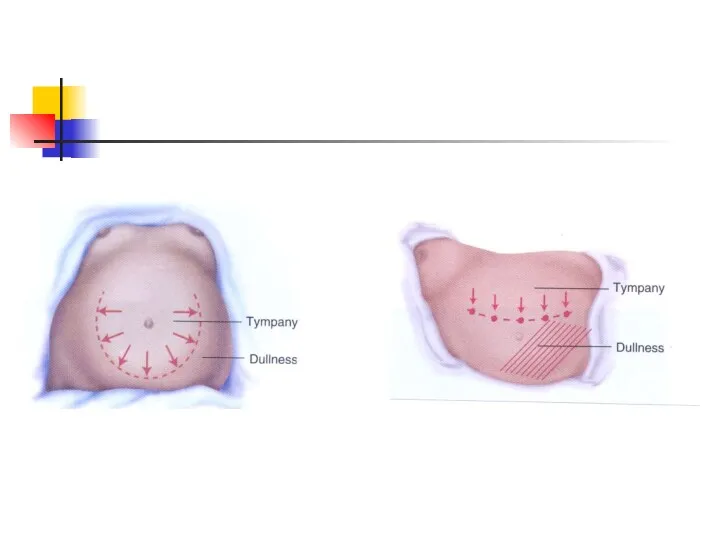
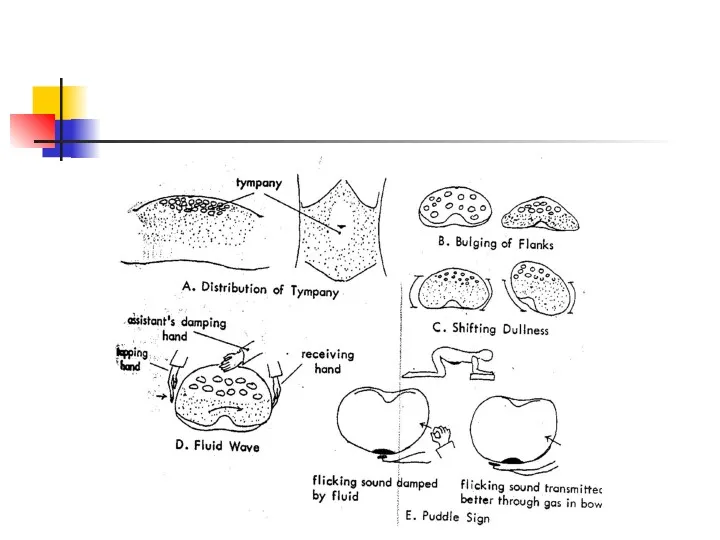
- 26. Examination of the Abdomen Percussion (#48) Percuss the liver in mid-clavicular line. Assess size by percussing
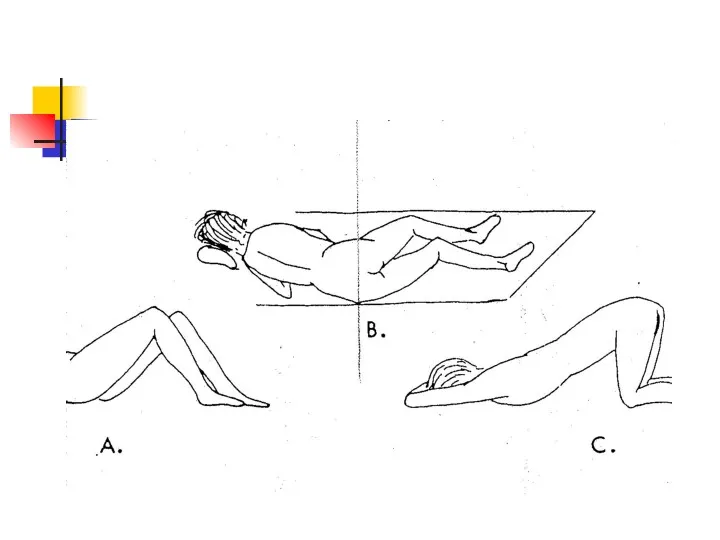
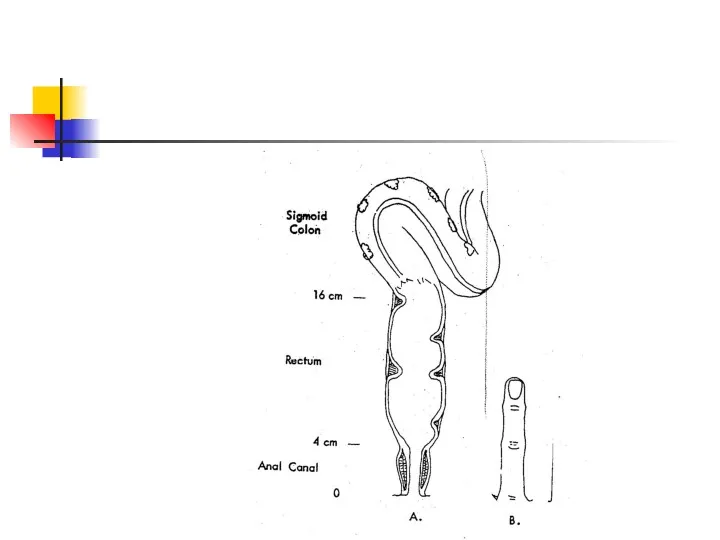
- 28. Examination of the Abdomen Rectal examination and stool specimen for FOBT Last step of the physical
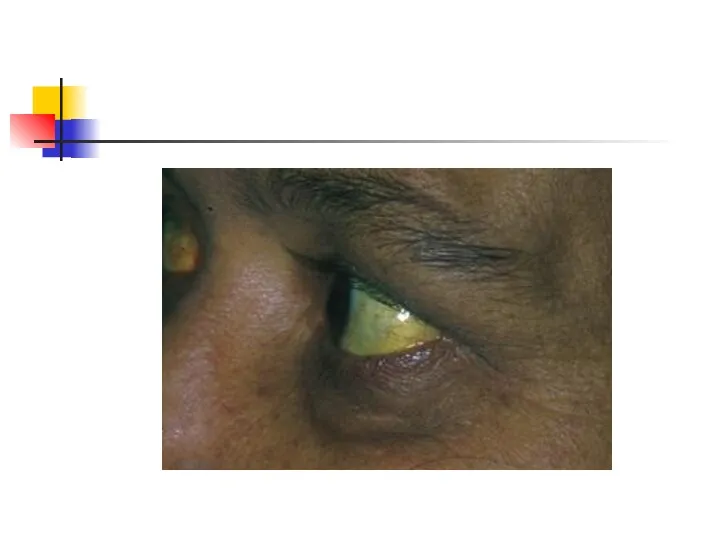
- 39. Jaundice and Scleral Icterus
- 41. Gynaecomastia or enlargement of breast tissue in men may occur either bilaterally or unilaterally.
- 42. Palmar Erythema is charactarized by a prominent rim of colour beginning on the hypothenar border of
- 43. Dupuytren's Contractures arise as a result of fibrous change in the palmar fascia which inserts into
- 44. Parotid Hypertrophy contributes to the rounded appearance of the face; the submandibular glands may also be
- 45. Spider Naevi are found only in the distribution of the superior vena cava, most commonly on
- 52. Thrombosed external hemorrhoids (long arrow) and perianal tags from "old" disease (short arrow).
- 53. Prolapsed internal hemorrhoids, grade IV (long black arrow). The dentate line (short black arrow) is indicated,
- 55. Acute posterior fissure (arrow). Anterior and posterior fissures are most common. Fissures can often be identified
- 56. Anal tag (arrow). Anal tags should be removed or a biopsy should be obtained to confirm
- 57. Anal cancer (arrow). This anal cancer had been treated for three months with steroid suppositories although
- 58. External site of perianal fistula. This patient presented with "just a little blood when I wipe."
- 60. Скачать презентацию
Examination of the Abdomen
Session Objectives:
Describe relevant anatomy and physiology as it
Examination of the Abdomen
Session Objectives:
Describe relevant anatomy and physiology as it
Examination of the Abdomen
Introduction:
The Medical History is an account of the
Examination of the Abdomen
Introduction:
The Medical History is an account of the
Examination of the Abdomen
Pain is a common symptom of diseases of
Examination of the Abdomen
Pain is a common symptom of diseases of
Examination of the Abdomen
Important aspects of abdominal pain:
Location and radiation of
Examination of the Abdomen
Important aspects of abdominal pain:
Location and radiation of
Examination of the Abdomen
Important related symptoms/signs in patients with abdominal pain:
Fever/rigors/sweats
Nausea/vomiting
Weight
Examination of the Abdomen
Important related symptoms/signs in patients with abdominal pain:
Fever/rigors/sweats
Nausea/vomiting
Weight
Examination of the Abdomen
Physical Examination:
The PE of the abdomen must be
Examination of the Abdomen
Physical Examination:
The PE of the abdomen must be
Examination of the Abdomen
Physical Examinationof the Abdomen is conducted in four
Examination of the Abdomen
Physical Examinationof the Abdomen is conducted in four
Examination of the Abdomen
For descriptive purposes, the abdomen is divided into
Examination of the Abdomen
For descriptive purposes, the abdomen is divided into
Examination of the Abdomen
Inspection/Observation (#40)
Inspect the contour of the abdomen. It
Examination of the Abdomen
Inspection/Observation (#40)
Inspect the contour of the abdomen. It
Examination of the Abdomen
Auscultation (#41)
Useful in assessing bowel motility and vascular
Examination of the Abdomen
Auscultation (#41)
Useful in assessing bowel motility and vascular
Examination of the Abdomen
Palpation (#43-#50)
Palpate lightly then deeply in all four
Examination of the Abdomen
Palpation (#43-#50)
Palpate lightly then deeply in all four

Examination of the Abdomen
Palpation (#43-#50) cont’d
Assess peritoneal irritation and rebound tenderness
Palpate
Examination of the Abdomen
Palpation (#43-#50) cont’d
Assess peritoneal irritation and rebound tenderness
Palpate
Examination of the Abdomen
Percussion (#48)
Percuss the liver in mid-clavicular line. Assess
Examination of the Abdomen
Percussion (#48)
Percuss the liver in mid-clavicular line. Assess
Examination of the Abdomen
Rectal examination and stool specimen for FOBT
Last step
Examination of the Abdomen
Rectal examination and stool specimen for FOBT
Last step
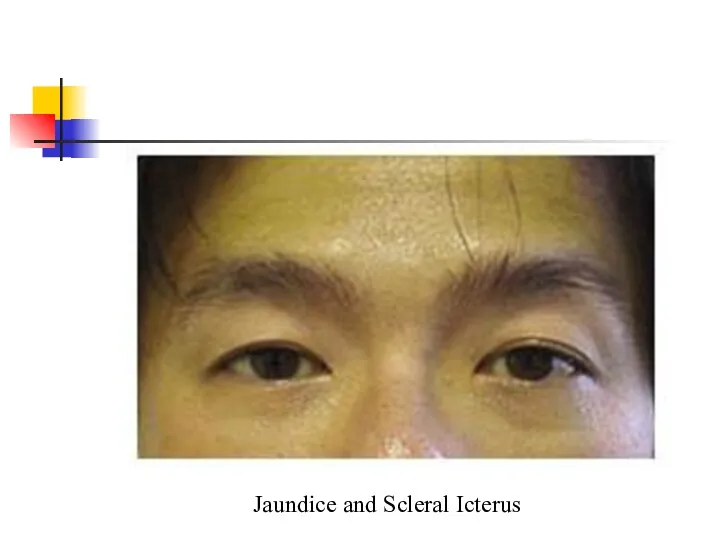
Jaundice and Scleral Icterus
Jaundice and Scleral Icterus
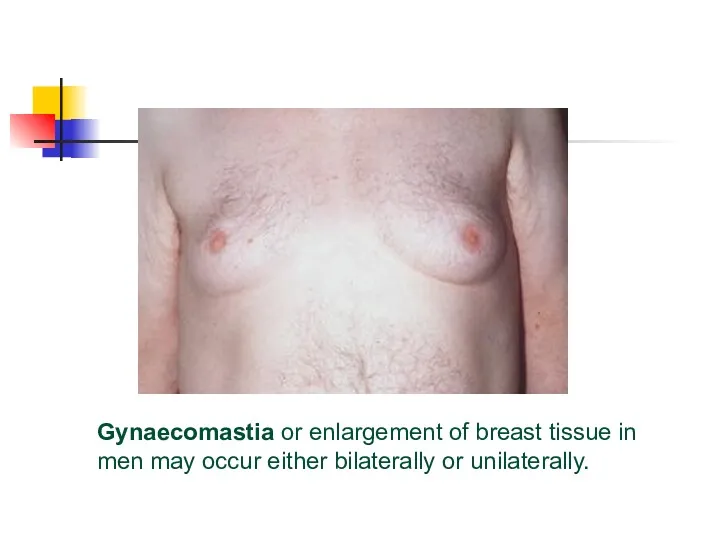
Gynaecomastia or enlargement of breast tissue in men may occur either
Gynaecomastia or enlargement of breast tissue in men may occur either
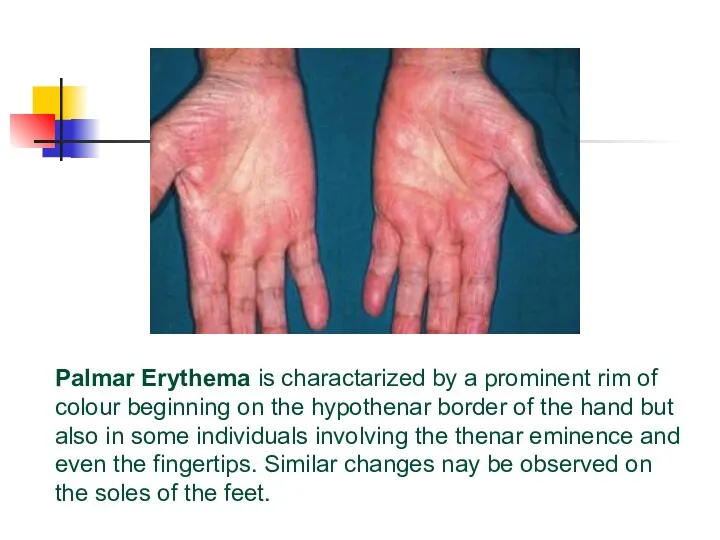
Palmar Erythema is charactarized by a prominent rim of colour beginning
Palmar Erythema is charactarized by a prominent rim of colour beginning
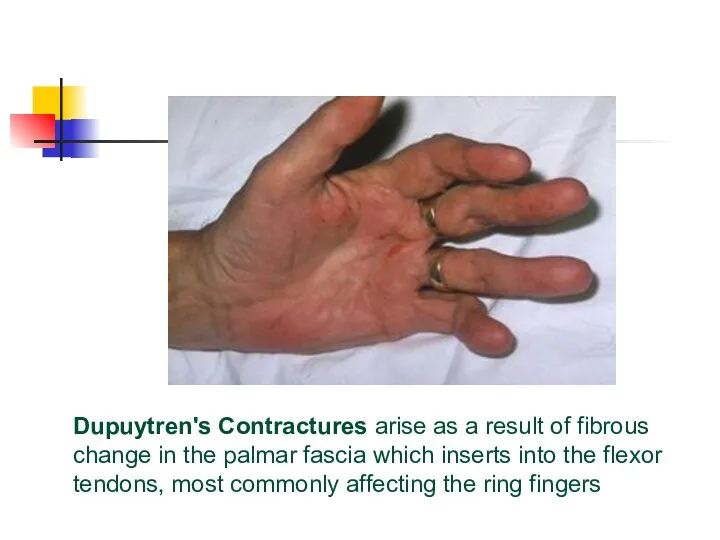
Dupuytren's Contractures arise as a result of fibrous change in the
Dupuytren's Contractures arise as a result of fibrous change in the
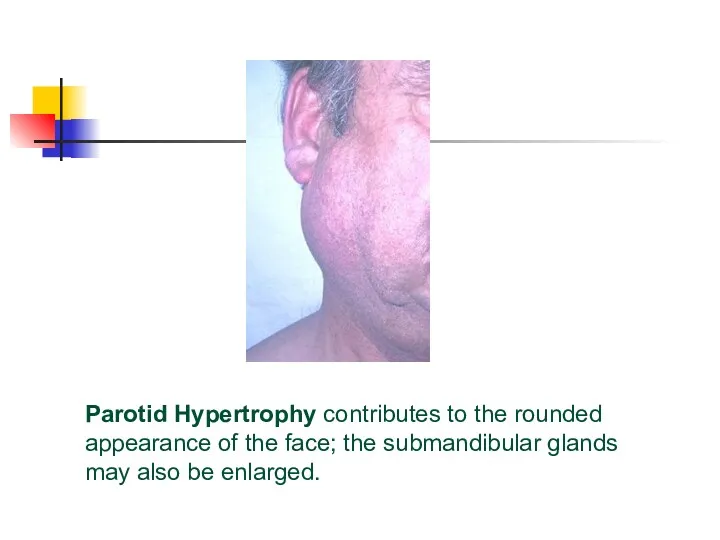
Parotid Hypertrophy contributes to the rounded appearance of the face; the
Parotid Hypertrophy contributes to the rounded appearance of the face; the
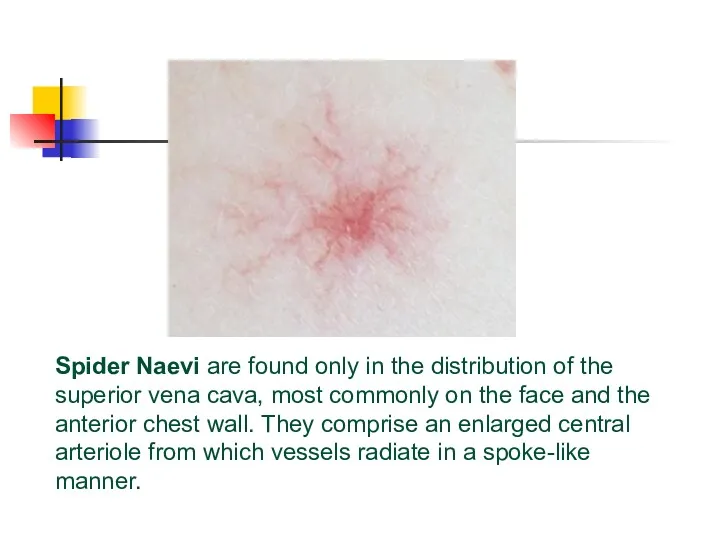
Spider Naevi are found only in the distribution of the superior
Spider Naevi are found only in the distribution of the superior
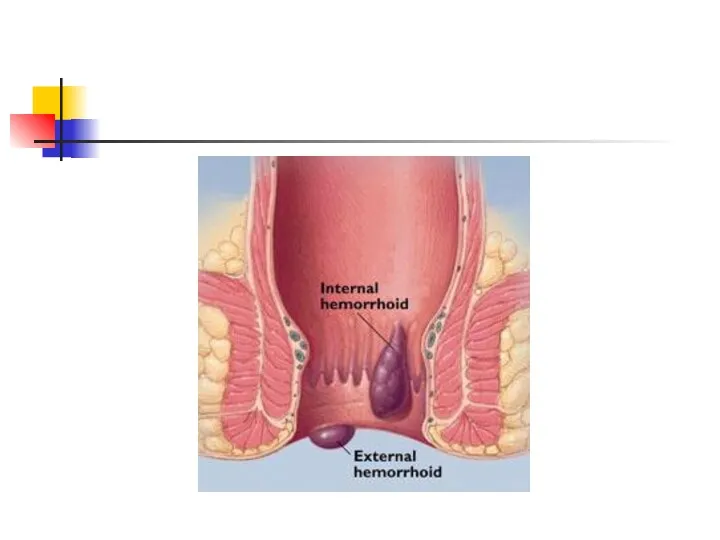

Thrombosed external hemorrhoids (long arrow) and perianal tags from "old" disease
Thrombosed external hemorrhoids (long arrow) and perianal tags from "old" disease
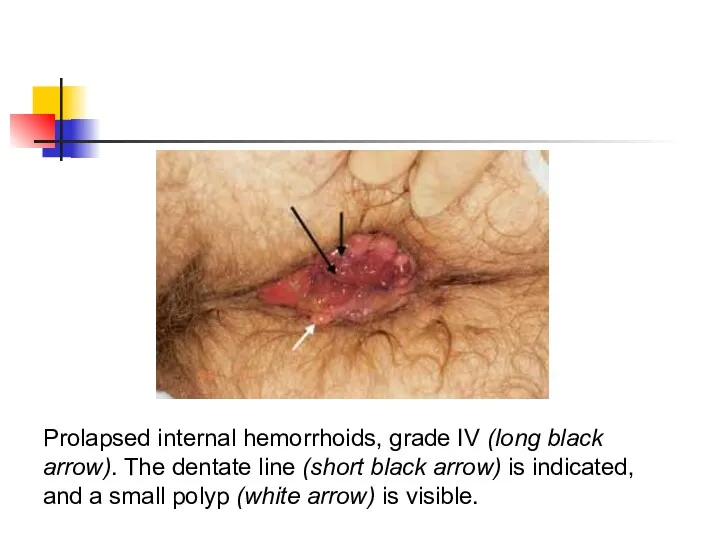
Prolapsed internal hemorrhoids, grade IV (long black arrow). The dentate line
Prolapsed internal hemorrhoids, grade IV (long black arrow). The dentate line
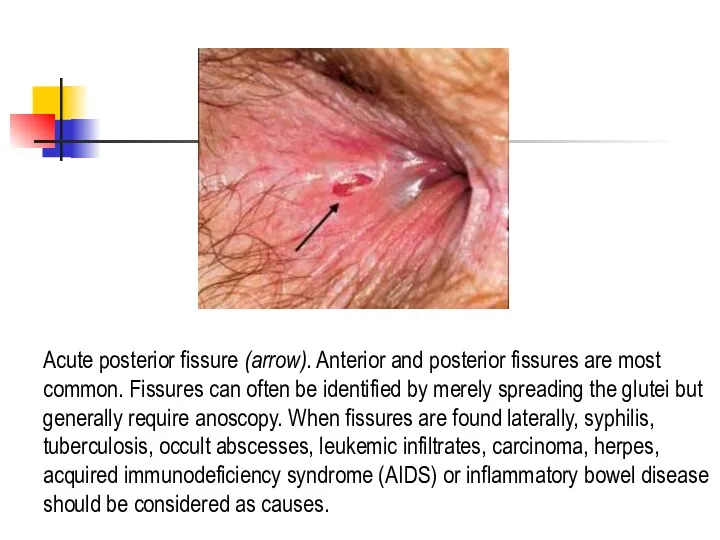
Acute posterior fissure (arrow). Anterior and posterior fissures are most common.
Acute posterior fissure (arrow). Anterior and posterior fissures are most common.
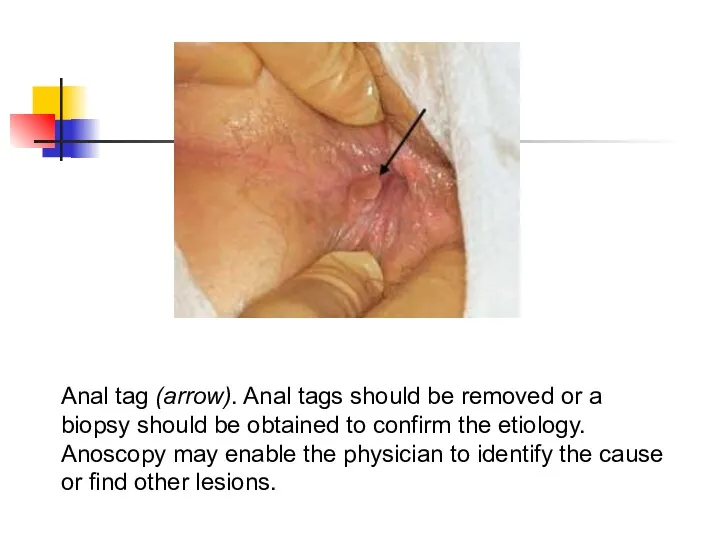
Anal tag (arrow). Anal tags should be removed or a biopsy
Anal tag (arrow). Anal tags should be removed or a biopsy
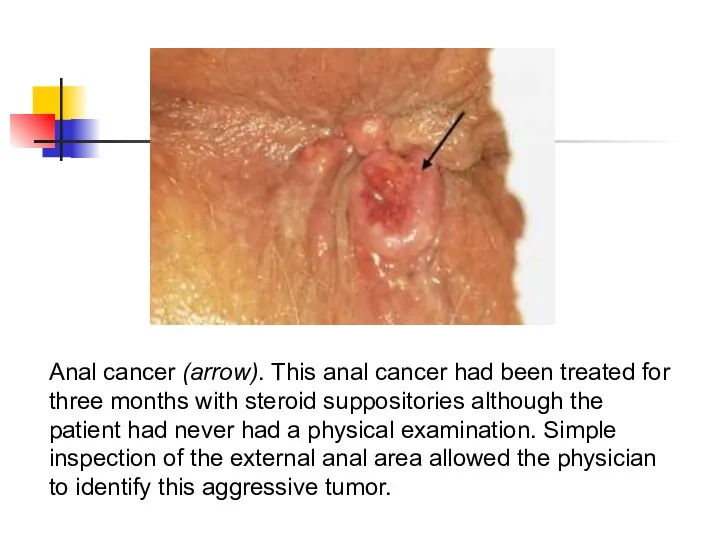
Anal cancer (arrow). This anal cancer had been treated for three
Anal cancer (arrow). This anal cancer had been treated for three
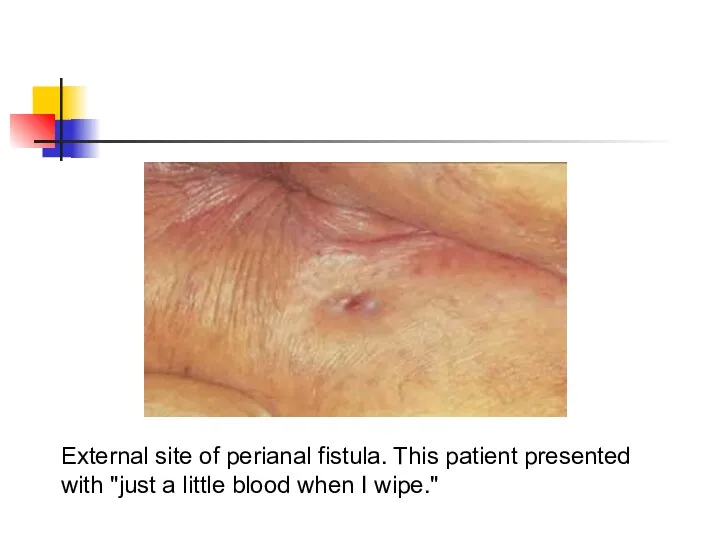
External site of perianal fistula. This patient presented with "just a
External site of perianal fistula. This patient presented with "just a
 My school
My school Глагол. Видо-временные формы глагола
Глагол. Видо-временные формы глагола How to take the Case
How to take the Case Sophie’s town
Sophie’s town The International Women’s Day
The International Women’s Day The United Kingdom of Great Britain and Northern Ireland
The United Kingdom of Great Britain and Northern Ireland The festivals of the world
The festivals of the world A Visit to the City
A Visit to the City Assessment. Types of assessment
Assessment. Types of assessment Halloween spelling game
Halloween spelling game ОГЭ. Чтение текста вслух
ОГЭ. Чтение текста вслух Traditional American Food
Traditional American Food On, in, under
On, in, under Housework
Housework Simple present: questions
Simple present: questions The christmas quiz
The christmas quiz Олимпиадные задания. Английский язык
Олимпиадные задания. Английский язык Australia
Australia Information about me
Information about me Attractions of London
Attractions of London Cleopatra - the greatest ruler
Cleopatra - the greatest ruler Lobbying. What it is and how it goes
Lobbying. What it is and how it goes White auto
White auto Food by english inn
Food by english inn How to improve your English
How to improve your English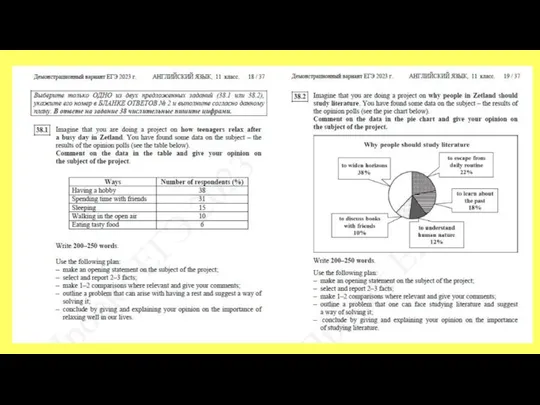 Эссе. Задание 38
Эссе. Задание 38 Superheroes. Match the verbs to the nouns
Superheroes. Match the verbs to the nouns Имена существительные
Имена существительные