- Campylobacter & Helicobacter

Содержание
- 2. rRNA Superfamily VI of Class Proteobacteria
- 3. Gram-negative Helical (spiral or curved) morphology; Tend to be pleomorphic Characteristics that facilitate penetration and colonization
- 4. First isolated as Vibrio fetus in 1909 from spontaneous abortions in livestock Campylobacter enteritis was not
- 5. Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um), helical (spiral or curved) cells
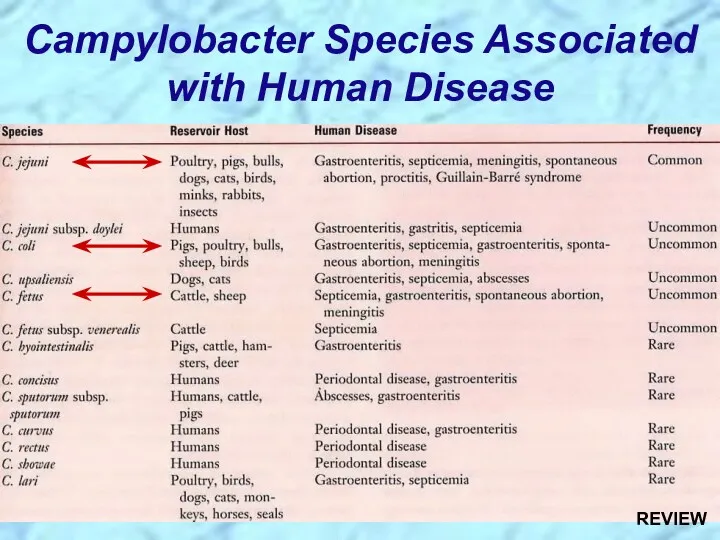
- 6. Campylobacter Species Associated with Human Disease
- 7. Low incidence potential sequela Reactive, self-limited, autoimmune disease Campylobacter jejuni most frequent antecedent pathogen Immune response
- 8. Zoonotic infections in many animals particularly avian (bird) reservoirs Spontaneous abortions in cattle, sheep, and swine,
- 9. Contaminated poultry accounts for more than half of the camylobacteriosis cases in developed countries but different
- 10. Sporadic infections in humans far outnumber those affected in point-source outbreaks Sporadic cases peak in the
- 12. Infectious dose and host immunity determine whether gastroenteric disease develops Some people infected with as few
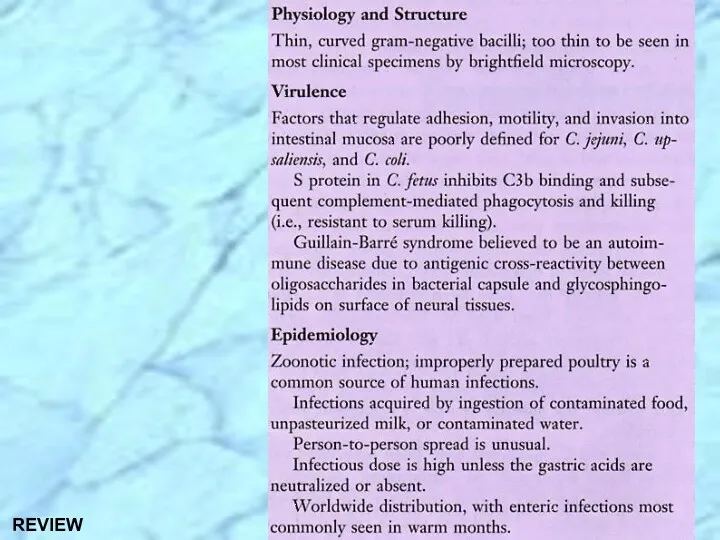
- 13. Cellular components: Endotoxin Flagellum: Motility Adhesins: Mediate attachment to mucosa Invasins GBS is associated with C.
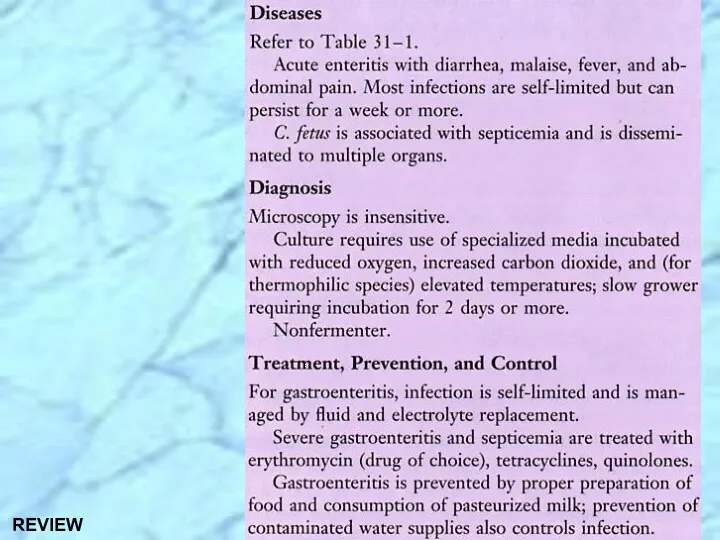
- 14. Specimen Collection and Processing: Feces refrigerated & examined within few hours Rectal swabs in semisolid transport
- 15. Laboratory Identification (cont.)
- 16. Gastroenteritis: Self-limiting; Replace fluids and electrolytes Antibiotic treatment can shorten the excretion period; Erythromycin is drug
- 18. History & Taxonomy of Helicobacter Family not yet named (17 species by rRNA sequencing) First observed
- 19. Helicobacter pylori is major human pathogen associated with gastric antral epithelium in patients with active chronic
- 20. Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded ends in gastric biopsy specimens;
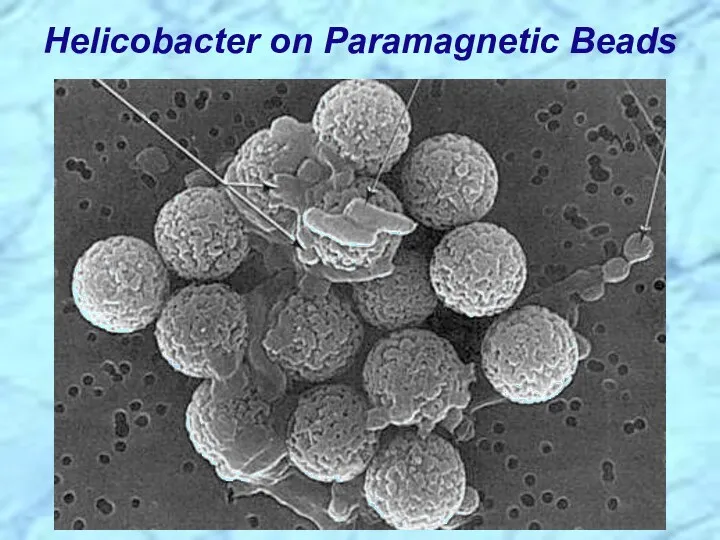
- 21. Helicobacter on Paramagnetic Beads
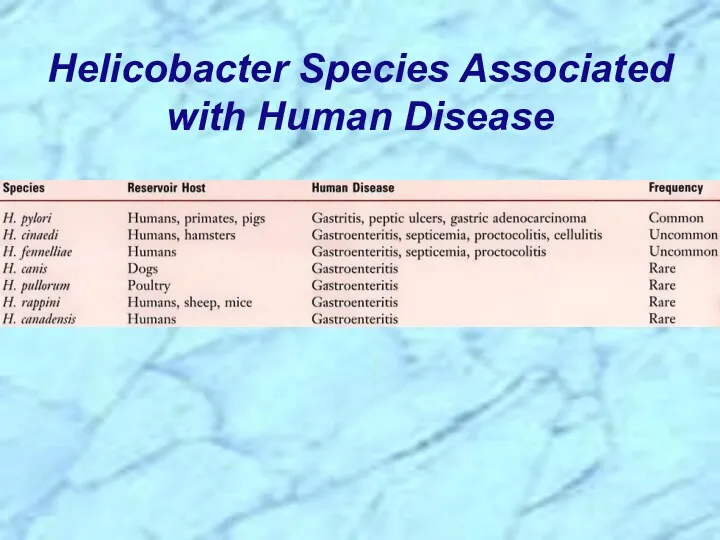
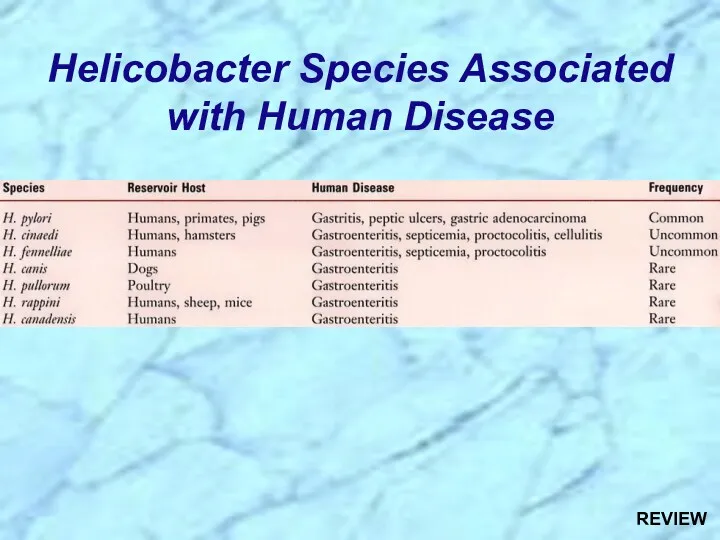
- 22. Helicobacter Species Associated with Human Disease
- 23. Family Clusters Orally transmitted person-to-person (?) Worldwide: ~ 20% below the age of 40 years are
- 24. Developed Countries: United States: 30% of total population infected Of those, ~1% per year develop duodenal
- 25. Colonize mucosal lining of stomach & duodenum in man & animals Adherent to gastric surface epithelium
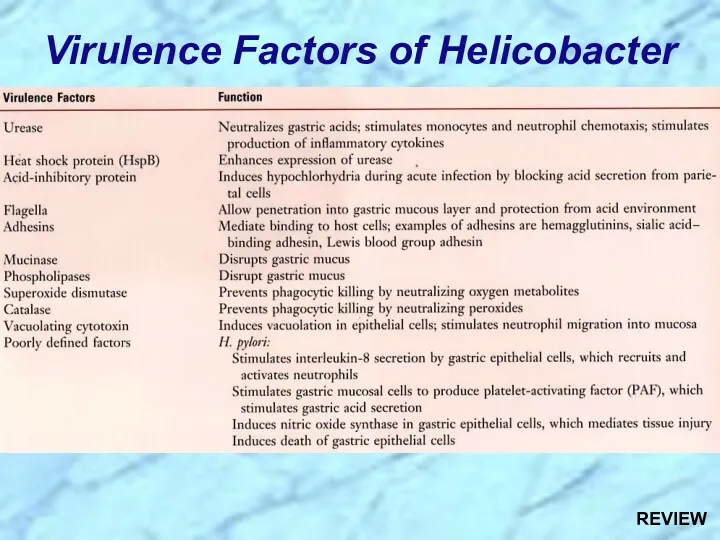
- 26. Virulence Factors of Helicobacter
- 27. Multiple polar, sheathed flagella Corkscrew motility enables penetration into viscous environment (mucus) Adhesins: Hemagglutinins; Sialic acid
- 28. Urease C=O(NH2)2 + H+ + 2H2O ? HCO3- + 2 (NH4+) Urea Bicarbonate Ammonium ions And
- 29. Tissue damage: Vacuolating cytotoxin: Epithelial cell damage Invasin(s)(??): Poorly defined (e.g., hemolysins; phospholipases; alcohol dehydrogenase) Protection
- 30. Laboratory Identification Recovered from or detected in endoscopic antral gastric biopsy material; Multiple biopsies are taken
- 31. Triple Chemotherapy (synergism): Proton pump inhibitor (e.g., omeprazole = Prilosec(R)) One or more antibiotics (e.g., clarithromycin;
- 33. REVIEW Campylobacter & Helicobacter Superfamily
- 34. Gram-negative Helical (spiral or curved) morphology; Tend to be pleomorphic Characteristics that facilitate penetration and colonization
- 35. Campylobacter Review
- 36. First isolated as Vibrio fetus in 1909 from spontaneous abortions in livestock Campylobacter enteritis was not
- 37. REVIEW
- 38. REVIEW
- 39. Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um), helical (spiral or curved) cells
- 40. Campylobacter Species Associated with Human Disease REVIEW
- 41. Low incidence potential sequela Reactive, self-limited, autoimmune disease Campylobacter jejuni most frequent antecedent pathogen Immune response
- 42. Zoonotic infections in many animals particularly avian (bird) reservoirs Spontaneous abortions in cattle, sheep, and swine,
- 43. Contaminated poultry accounts for more than half of the camylobacteriosis cases in developed countries but different
- 44. Sporadic infections in humans far outnumber those affected in point-source outbreaks Sporadic cases peak in the
- 46. Helicobacter Review
- 47. History & Taxonomy of Helicobacter Family not yet named (17 species by rRNA sequencing) First observed
- 48. Helicobacter pylori is major human pathogen associated with gastric antral epithelium in patients with active chronic
- 49. REVIEW
- 50. REVIEW
- 51. Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded ends in gastric biopsy specimens;
- 52. Helicobacter Species Associated with Human Disease REVIEW
- 53. Family Clusters Orally transmitted person-to-person ~ 20% below the age of 40 years are infected 50%
- 54. Developed Countries: United States: 30% of total population infected Of those, ~1% per year develop duodenal
- 55. Colonize mucosal lining of stomach & duodenum in man & animals Adherent to gastric surface epithelium
- 56. Virulence Factors of Helicobacter REVIEW
- 57. Triple Chemotherapy (synergism): Proton pump inhibitor (e.g., omeprazole = Prilosec(R)) One or more antibiotics (e.g., clarithromycin;
- 59. Скачать презентацию
rRNA Superfamily VI of Class Proteobacteria
rRNA Superfamily VI of Class Proteobacteria
Gram-negative
Helical (spiral or curved) morphology; Tend to be pleomorphic
Characteristics that facilitate
Gram-negative
Helical (spiral or curved) morphology; Tend to be pleomorphic
Characteristics that facilitate
First isolated as Vibrio fetus in 1909 from spontaneous abortions in
First isolated as Vibrio fetus in 1909 from spontaneous abortions in
Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um),
Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um),
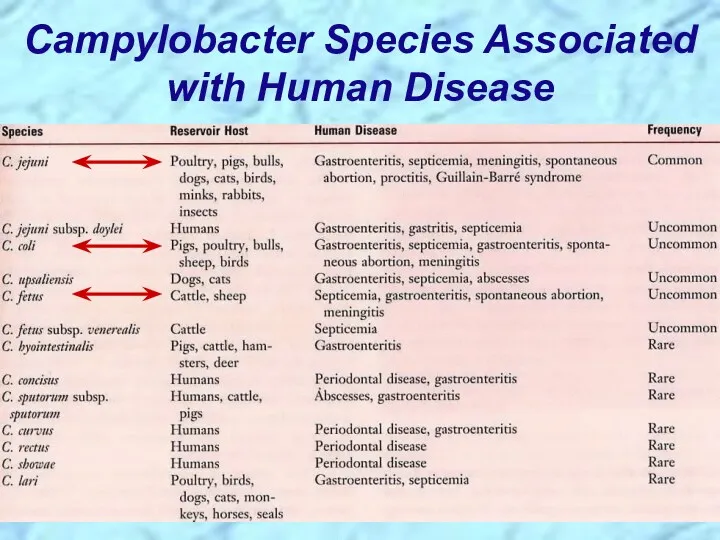
Campylobacter Species Associated with Human Disease
Campylobacter Species Associated with Human Disease
Low incidence potential sequela
Reactive, self-limited, autoimmune disease
Campylobacter jejuni most frequent antecedent
Low incidence potential sequela
Reactive, self-limited, autoimmune disease
Campylobacter jejuni most frequent antecedent
Zoonotic infections in many animals particularly avian (bird) reservoirs
Spontaneous abortions in
Zoonotic infections in many animals particularly avian (bird) reservoirs
Spontaneous abortions in
Contaminated poultry accounts for more than half of the camylobacteriosis cases
Contaminated poultry accounts for more than half of the camylobacteriosis cases
Sporadic infections in humans far outnumber those affected in point-source outbreaks
Sporadic
Sporadic infections in humans far outnumber those affected in point-source outbreaks
Sporadic

Infectious dose and host immunity determine whether gastroenteric disease develops
Some people
Infectious dose and host immunity determine whether gastroenteric disease develops
Some people
Cellular components:
Endotoxin
Flagellum: Motility
Adhesins: Mediate attachment to mucosa
Invasins
GBS is associated with
Cellular components:
Endotoxin
Flagellum: Motility
Adhesins: Mediate attachment to mucosa
Invasins
GBS is associated with
Specimen Collection and Processing:
Feces refrigerated & examined within few hours
Specimen Collection and Processing:
Feces refrigerated & examined within few hours
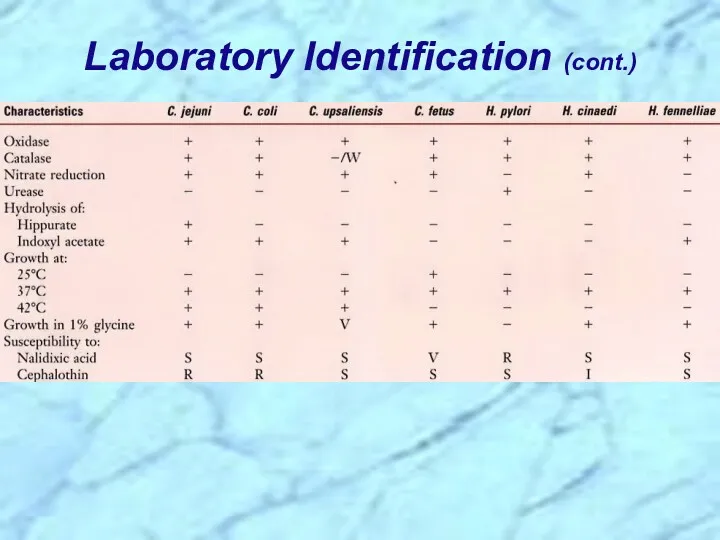
Laboratory Identification (cont.)
Laboratory Identification (cont.)
Gastroenteritis:
Self-limiting; Replace fluids and electrolytes
Antibiotic treatment can shorten the
Gastroenteritis:
Self-limiting; Replace fluids and electrolytes
Antibiotic treatment can shorten the
History & Taxonomy of Helicobacter
Family not yet named (17 species by
History & Taxonomy of Helicobacter
Family not yet named (17 species by
Helicobacter pylori is major human pathogen associated with gastric antral epithelium
Helicobacter pylori is major human pathogen associated with gastric antral epithelium
Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded
Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded
Helicobacter on Paramagnetic Beads
Helicobacter on Paramagnetic Beads
Helicobacter Species Associated with Human Disease
Helicobacter Species Associated with Human Disease
Family Clusters
Orally transmitted person-to-person (?)
Worldwide:
~ 20% below the age of 40
Family Clusters
Orally transmitted person-to-person (?)
Worldwide:
~ 20% below the age of 40
Developed Countries:
United States: 30% of total population infected
Of those, ~1%
Developed Countries:
United States: 30% of total population infected
Of those, ~1%
Colonize mucosal lining of stomach & duodenum in man & animals
Colonize mucosal lining of stomach & duodenum in man & animals
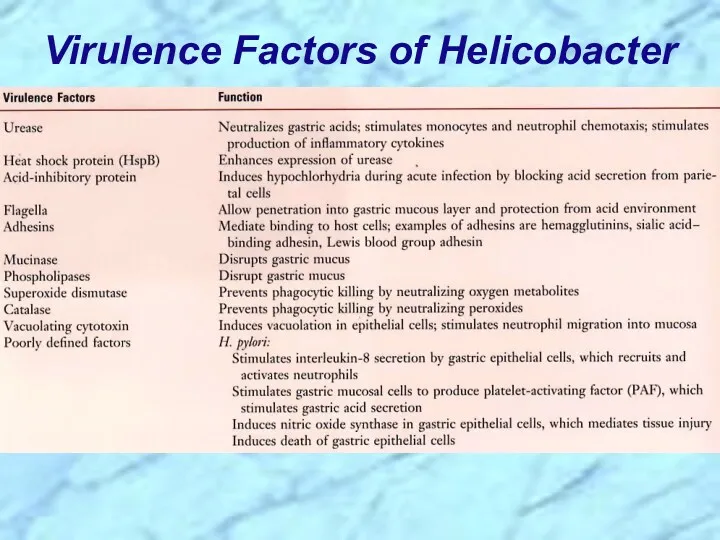
Virulence Factors of Helicobacter
Virulence Factors of Helicobacter
Multiple polar, sheathed flagella
Corkscrew motility enables penetration into viscous environment (mucus)
Adhesins:
Multiple polar, sheathed flagella
Corkscrew motility enables penetration into viscous environment (mucus)
Adhesins:
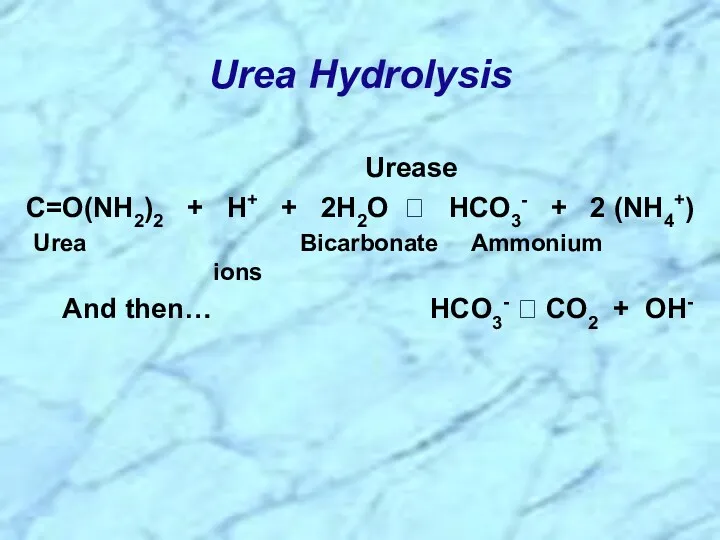
Urease
C=O(NH2)2 + H+ + 2H2O ? HCO3- + 2
Urease
C=O(NH2)2 + H+ + 2H2O ? HCO3- + 2
Tissue damage:
Vacuolating cytotoxin: Epithelial cell damage
Invasin(s)(??): Poorly defined (e.g., hemolysins;
Tissue damage:
Vacuolating cytotoxin: Epithelial cell damage
Invasin(s)(??): Poorly defined (e.g., hemolysins;
Laboratory Identification
Recovered from or detected in endoscopic antral gastric biopsy material;
Laboratory Identification
Recovered from or detected in endoscopic antral gastric biopsy material;
Triple Chemotherapy (synergism):
Proton pump inhibitor (e.g., omeprazole = Prilosec(R))
One or more
Proton pump inhibitor (e.g., omeprazole = Prilosec(R))
One or more
REVIEW
Campylobacter & Helicobacter Superfamily
REVIEW
Campylobacter & Helicobacter Superfamily
Gram-negative
Helical (spiral or curved) morphology; Tend to be pleomorphic
Characteristics that facilitate
Gram-negative
Helical (spiral or curved) morphology; Tend to be pleomorphic
Characteristics that facilitate
Campylobacter Review
Campylobacter Review
First isolated as Vibrio fetus in 1909 from spontaneous abortions in
First isolated as Vibrio fetus in 1909 from spontaneous abortions in
REVIEW
REVIEW
REVIEW
REVIEW
Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um),
Small, thin (0.2 - 0.5 um X 0.5 - 5.0 um),
Campylobacter Species Associated with Human Disease
REVIEW
Campylobacter Species Associated with Human Disease
REVIEW
Low incidence potential sequela
Reactive, self-limited, autoimmune disease
Campylobacter jejuni most frequent antecedent
Low incidence potential sequela
Reactive, self-limited, autoimmune disease
Campylobacter jejuni most frequent antecedent
Zoonotic infections in many animals particularly avian (bird) reservoirs
Spontaneous abortions in
Zoonotic infections in many animals particularly avian (bird) reservoirs
Spontaneous abortions in
Contaminated poultry accounts for more than half of the camylobacteriosis cases
Contaminated poultry accounts for more than half of the camylobacteriosis cases
Sporadic infections in humans far outnumber those affected in point-source outbreaks
Sporadic
Sporadic infections in humans far outnumber those affected in point-source outbreaks
Sporadic
Helicobacter Review
Helicobacter Review
History & Taxonomy of Helicobacter
Family not yet named (17 species by
History & Taxonomy of Helicobacter
Family not yet named (17 species by
Helicobacter pylori is major human pathogen associated with gastric antral epithelium
Helicobacter pylori is major human pathogen associated with gastric antral epithelium
REVIEW
REVIEW
REVIEW
REVIEW
Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded
Gram-negative; Helical (spiral or curved) (0.5-1.0 um X 2.5-5.0 um); Blunted/rounded
Helicobacter Species Associated with Human Disease
REVIEW
Helicobacter Species Associated with Human Disease
REVIEW
Family Clusters
Orally transmitted person-to-person
~ 20% below the age of 40 years
Family Clusters
Orally transmitted person-to-person
~ 20% below the age of 40 years
Developed Countries:
United States: 30% of total population infected
Of those, ~1%
Developed Countries:
United States: 30% of total population infected
Of those, ~1%
Colonize mucosal lining of stomach & duodenum in man & animals
Colonize mucosal lining of stomach & duodenum in man & animals
Virulence Factors of Helicobacter
REVIEW
Virulence Factors of Helicobacter
REVIEW
Triple Chemotherapy (synergism):
Proton pump inhibitor (e.g., omeprazole = Prilosec(R))
One or more
Proton pump inhibitor (e.g., omeprazole = Prilosec(R))
One or more
 Зеленые водоросли Chlorophyta
Зеленые водоросли Chlorophyta ЕГЭ Биология. Новый формат заданий. 2022
ЕГЭ Биология. Новый формат заданий. 2022 Антиоксидант астаксантин
Антиоксидант астаксантин Кожа. Наружный покров
Кожа. Наружный покров Генетический материал клетки. Генный уровень
Генетический материал клетки. Генный уровень Нуклеїнові кислоти. Класифікація. Будова. Біологічне значення. Нуклеопротеїни
Нуклеїнові кислоти. Класифікація. Будова. Біологічне значення. Нуклеопротеїни Vitamins. Classes of Vitamins
Vitamins. Classes of Vitamins Нуклеиновые кислоты
Нуклеиновые кислоты Урок обобщение по главе Класс птицы
Урок обобщение по главе Класс птицы Кожно-двигательный, зрительный, слуховой,вестибулярный, обонятельный и вкусовой анализаторы
Кожно-двигательный, зрительный, слуховой,вестибулярный, обонятельный и вкусовой анализаторы Птичьи рекорды
Птичьи рекорды Столовые сорта винограда (районированные и перспективные)
Столовые сорта винограда (районированные и перспективные) Охраняемые растения Крыма
Охраняемые растения Крыма Презентация для урока-обобщения по биологии в 5 классе
Презентация для урока-обобщения по биологии в 5 классе Культурні рослини
Культурні рослини Нужны ли минеральные соли животным и человеку
Нужны ли минеральные соли животным и человеку История развития эволюционных идей
История развития эволюционных идей Тестовыя работа по теме: Вирусы
Тестовыя работа по теме: Вирусы Molecular genetic factors controlling plant resistance to diseases
Molecular genetic factors controlling plant resistance to diseases Эпиграф
Эпиграф Биология полорогих: дзерена, сайгака, горала
Биология полорогих: дзерена, сайгака, горала Предмет и задачи токсикологической химии. Взаимосвязь с другими дисциплинами. (Лекция 1)
Предмет и задачи токсикологической химии. Взаимосвязь с другими дисциплинами. (Лекция 1) Становление систематики. 9 класс
Становление систематики. 9 класс Ищите доктора в природе
Ищите доктора в природе Откуда берутся шоколад, изюм и мед
Откуда берутся шоколад, изюм и мед Экзаменационные микропрепараты
Экзаменационные микропрепараты Отряд Пчёлы
Отряд Пчёлы Пищеварение в полости рта: состав и свойства слюны
Пищеварение в полости рта: состав и свойства слюны