- Acute abdomen and peritonitis

Содержание
- 2. An abdominal condition of abrupt onset associated with severe abdominal pain (resulting from inflammation, obstruction, infarction,
- 3. Visceral pain Comes from abdominal/pelvic viscera Transmitted by visceral afferent nerve fibres in response to stretching
- 4. Intestinal Acute appendicitis, mesenteric adenitis, mekel’s diverticulitis, perforated peptic ulcer, gastroenteritis, diverticulitis, intestinal obstruction, strangulated hernia
- 5. History Examination Simple Investigations More complex investigations based on findings of the above Most diagnosis can
- 6. Abdominal pain – features will point you towards diagnosis SOCRATES Site and duration Onset – sudden
- 7. Associated symptoms GI: bowels last opened, bowel habit (diarrhoea/constipation), PR bleeding/melaena, dyspeptic symptoms, vomiting Urine: dysuria,
- 8. Inspection: scars/asymmetry/distention Palaption: Point of maximal tenderness Features of peritonitis (localised vs generalised) Guarding Percussion tenderness
- 9. Liver (hepatitis) Gall bladder (gallstones) Stomach (peptic ulcer, gastritis) Hepatic flexure colon (cancer) Lung (pneumonia) Acute
- 10. Simple Investigations: Bloods tests (FBC, U&E, LFT, amylase, clotting, CRP, G&S, ABG) Urine dipstick Pregnancy test
- 11. Urgent surgery should not be delayed for time consuming tests when an indication for surgery is
- 12. Peritonitis – inflammation of the peritoneum which maybe localised or generalised Peritonism – refers to specific
- 13. Infective – bacteria cause peritonitis e.g. due to gangrene or perforation of a viscus (appendicitis/diverticulitis/perforated ulcer).
- 14. Pain Constant and severe (site will give clue as to cause, or maybe generalised) Worse on
- 15. Diagnosis most often made on history and examination If localised peritonitis Investigations are those listed on
- 16. ABC Oxygen Fluid resuscitation (large bore cannule, bloods, IVF, catheter) IV antibiotics (Augmentin and metronidazole) Analgesia
- 18. Скачать презентацию
An abdominal condition of abrupt onset associated with severe abdominal pain
An abdominal condition of abrupt onset associated with severe abdominal pain
Visceral pain
Comes from abdominal/pelvic viscera
Transmitted by visceral afferent nerve fibres in
Visceral pain
Comes from abdominal/pelvic viscera
Transmitted by visceral afferent nerve fibres in
Intestinal
Acute appendicitis, mesenteric adenitis, mekel’s diverticulitis, perforated peptic ulcer, gastroenteritis, diverticulitis,
Intestinal
Acute appendicitis, mesenteric adenitis, mekel’s diverticulitis, perforated peptic ulcer, gastroenteritis, diverticulitis,
History
Examination
Simple Investigations
More complex investigations based on findings of the above
Most diagnosis
History
Examination
Simple Investigations
More complex investigations based on findings of the above
Most diagnosis
Abdominal pain – features will point you towards diagnosis
SOCRATES
Site and duration
Onset
Abdominal pain – features will point you towards diagnosis
SOCRATES
Site and duration
Onset
Associated symptoms
GI: bowels last opened, bowel habit (diarrhoea/constipation), PR bleeding/melaena, dyspeptic
Associated symptoms
GI: bowels last opened, bowel habit (diarrhoea/constipation), PR bleeding/melaena, dyspeptic
Inspection: scars/asymmetry/distention
Palaption:
Point of maximal tenderness
Features of peritonitis (localised vs generalised)
Guarding
Percussion tenderness
Rebound
Inspection: scars/asymmetry/distention
Palaption:
Point of maximal tenderness
Features of peritonitis (localised vs generalised)
Guarding
Percussion tenderness
Rebound
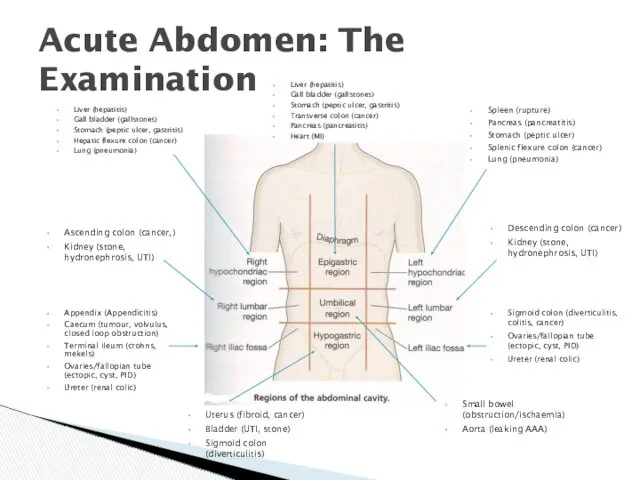
Liver (hepatitis)
Gall bladder (gallstones)
Stomach (peptic ulcer, gastritis)
Hepatic flexure colon (cancer)
Lung (pneumonia)
Acute
Liver (hepatitis)
Gall bladder (gallstones)
Stomach (peptic ulcer, gastritis)
Hepatic flexure colon (cancer)
Lung (pneumonia)
Acute
Simple Investigations:
Bloods tests (FBC, U&E, LFT, amylase, clotting, CRP, G&S, ABG)
Simple Investigations:
Bloods tests (FBC, U&E, LFT, amylase, clotting, CRP, G&S, ABG)
Urgent surgery should not be delayed for time consuming tests when
Urgent surgery should not be delayed for time consuming tests when
Peritonitis – inflammation of the peritoneum which maybe localised or generalised
Peritonism
Peritonitis – inflammation of the peritoneum which maybe localised or generalised
Peritonism
Infective – bacteria cause peritonitis e.g. due to gangrene or perforation
Infective – bacteria cause peritonitis e.g. due to gangrene or perforation
Pain
Constant and severe (site will give clue as to cause, or
Pain
Constant and severe (site will give clue as to cause, or
Diagnosis most often made on history and examination
If localised peritonitis
Investigations are
Diagnosis most often made on history and examination
If localised peritonitis
Investigations are
ABC
Oxygen
Fluid resuscitation (large bore cannule, bloods, IVF, catheter)
IV antibiotics (Augmentin and
ABC
Oxygen
Fluid resuscitation (large bore cannule, bloods, IVF, catheter)
IV antibiotics (Augmentin and
 Питание кормящей матери
Питание кормящей матери Эффект Допплера
Эффект Допплера Управление качеством медицинской помощи
Управление качеством медицинской помощи Медицинские приборно-компьютерные системы. (Лекция 4)
Медицинские приборно-компьютерные системы. (Лекция 4) Вакцинопрофилактика коклюша. Часть 2
Вакцинопрофилактика коклюша. Часть 2 Хронические миелопролиферативные заболевания
Хронические миелопролиферативные заболевания Дәрілік өсімдіктерді халық медицинасында қолдану тарихы
Дәрілік өсімдіктерді халық медицинасында қолдану тарихы Естественные факторы защиты организма. Механизмы иммунной защиты
Естественные факторы защиты организма. Механизмы иммунной защиты Энтеровирусная инфекция
Энтеровирусная инфекция Определение и оценка физического развития
Определение и оценка физического развития Токсоплазмоз. Распространённость токсоплазмоза
Токсоплазмоз. Распространённость токсоплазмоза Науқасқа, оның отбасына және туыстарына каралы хабарды жеткiзу
Науқасқа, оның отбасына және туыстарына каралы хабарды жеткiзу Философия сестринского дела
Философия сестринского дела Респираторлық дистресс синдромы
Респираторлық дистресс синдромы Шизофрения, шизотипические и бредовые расстройства
Шизофрения, шизотипические и бредовые расстройства Хирургическое лечение приобретенных пороков сердца. Митральный, аортальный порок, сочетанное поражение двух клапанов сердца
Хирургическое лечение приобретенных пороков сердца. Митральный, аортальный порок, сочетанное поражение двух клапанов сердца Клинический случай миелодиспластического синдрома
Клинический случай миелодиспластического синдрома Морфологические элементы сыпи
Морфологические элементы сыпи Деонтология.Дәрігер-стоматолог
Деонтология.Дәрігер-стоматолог Проблемы нормативного обеспечения в сфере информатизации здравоохранения
Проблемы нормативного обеспечения в сфере информатизации здравоохранения Портфели влияют на нашу осанку
Портфели влияют на нашу осанку Симптомы, проявления, диагностика и лечение васкулита
Симптомы, проявления, диагностика и лечение васкулита Жылқының шаншу түрінде өтетін аурулары
Жылқының шаншу түрінде өтетін аурулары Техника кесарева сечения
Техника кесарева сечения Массаж
Массаж Новое рентгеновское оборудование в медицине
Новое рентгеновское оборудование в медицине Заболевания конечностей и их лечение. Ортопедическая ковка
Заболевания конечностей и их лечение. Ортопедическая ковка ЛФК в хирургии после оперативных вмешательств
ЛФК в хирургии после оперативных вмешательств