Addressing significant unmet medical needs in central nervous system diseases with a unique portfolio of product candidates презентация
- Addressing significant unmet medical needs in central nervous system diseases with a unique portfolio of product candidates

Содержание
- 2. All trademarks, trade names and service marks appearing in this presentation are the property of their
- 3. Investment thesis Differentiated assets Lead product in pivotal Phase 3 trial Four Phase 2b studies ongoing
- 4. Pipeline of four innovative CNS compounds MoA=mechanism of action
- 5. Antipsychotics do not address negative symptoms and cognitive impairment associated with schizophrenia (and maybe worsen them?)
- 6. Negative vs positive symptoms in schizophrenia Positive symptoms reflect an excess or distortion of normal functions
- 7. Recent survey of psychiatrists ranks negative symptoms as the #1 unmet medical need for patients with
- 8. Roluperidone clinical data Peer-reviewed data publications Davidson, M., et al., Efficacy and Safety of MIN-101: A
- 9. Roluperidone Phase 2b study design: monotherapy, double-blind, placebo-controlled in schizophrenic patients with negative symptoms Specific effects
- 10. Phase 2b study showed specific improvements in negative symptoms over 12 weeks and 36 weeks in
- 11. Roluperidone: Paradigm change in schizophrenia treatment DA blockers DA blockers + 5HT2A blockers Typicals (1960 –
- 12. ≈60% of adult patients with schizophrenia who are treated have negative symptoms and are relapse free
- 13. Roluperidone Phase 3 Designed to replicate successful Phase 2b Design reviewed at end-of-Phase 2 meeting with
- 14. Roluperidone Phase 3 study design: monotherapy, double-blind, placebo-controlled in schizophrenic patients with negative symptoms Phase 3
- 15. Phase 3 efficacy study: confirmatory study design guided by insights from Phase 2b and dialogue with
- 16. Seltorexant MIN-202 / JNJ-42847922 A drug to treat insomnia and major depressive disorder by restoring physiological
- 17. Orexin system: Neurobiology targets circuits that mediate sleep and mood symptoms
- 18. Seltorexant study in MDD with comorbid insomnia shows improvements in insomnia and depressive symptoms Exploratory Phase
- 19. Seltorexant Phase 2b program: 2 trials in MDD and 1 in insomnia ongoing, with data read-outs
- 20. MIN-117 Addressing the unmet medical needs of patients with major depressive disorder and anxiety symptoms
- 21. The Phase 2a results show effect on primary endpoint in depression as well as noted effect
- 22. Sleep PSG shows intact REM latency resulting in preservation of sleep architecture and continuity of sleep,
- 23. Ongoing Phase 2b study designed to evaluate MIN-117 in patients with moderate to severe MDD Treatment
- 24. MIN-117 Phase 2b study objectives Primary: To evaluate the efficacy of 5.0 mg or 2.5 mg
- 25. MIN-301 A protein drug with disease-modifying potential for the treatment of unmet medical needs in Parkinson’s
- 26. Neuregulin-1 (NGR-1) has multiple roles in neuronal development offering potential for neuronal repair in several CNS
- 27. Strong financial position to deliver on major milestones ≈$121.1 million cash balance (cash, cash equivalents, and
- 29. Скачать презентацию
All trademarks, trade names and service marks appearing in this presentation
All trademarks, trade names and service marks appearing in this presentation
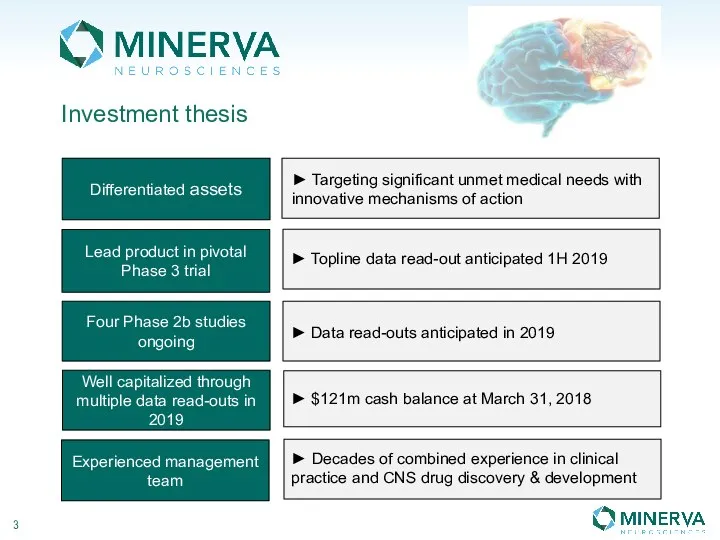
Investment thesis
Differentiated assets
Lead product in pivotal Phase 3 trial
Four Phase 2b
Investment thesis
Differentiated assets
Lead product in pivotal Phase 3 trial
Four Phase 2b
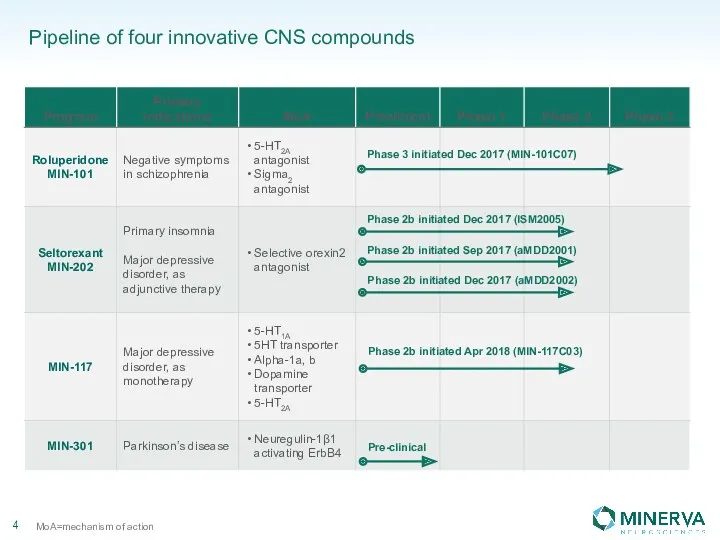
Pipeline of four innovative CNS compounds
MoA=mechanism of action
Pipeline of four innovative CNS compounds
MoA=mechanism of action
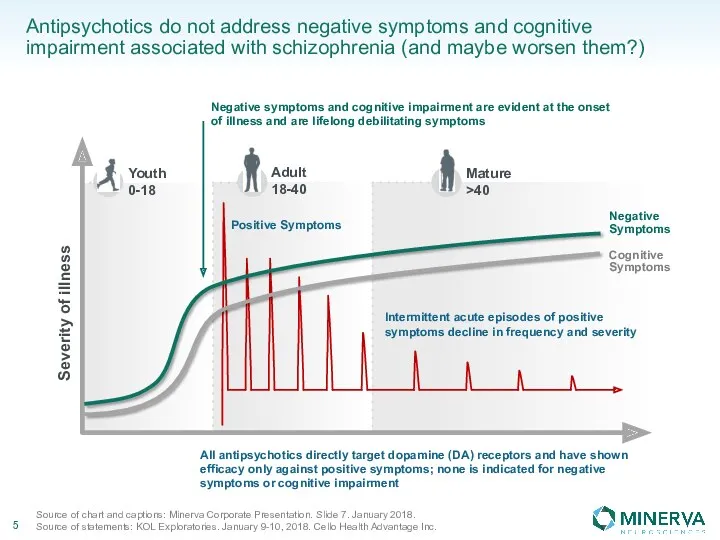
Antipsychotics do not address negative symptoms and cognitive impairment associated with
Antipsychotics do not address negative symptoms and cognitive impairment associated with
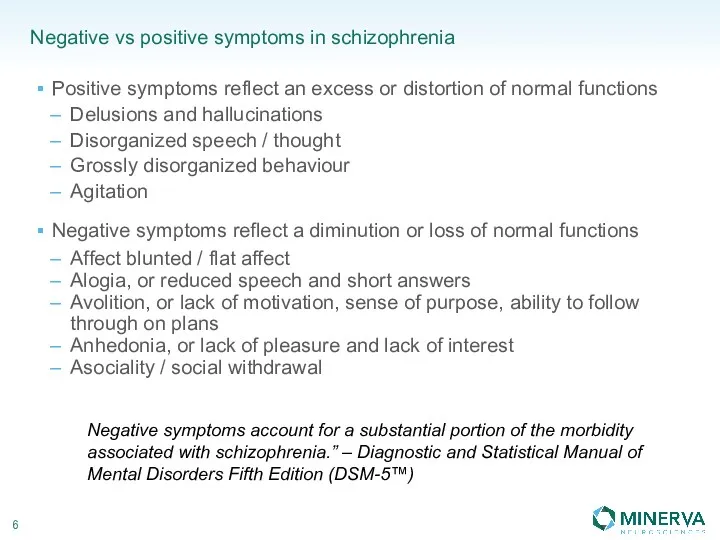
Negative vs positive symptoms in schizophrenia
Positive symptoms reflect an excess or
Negative vs positive symptoms in schizophrenia
Positive symptoms reflect an excess or
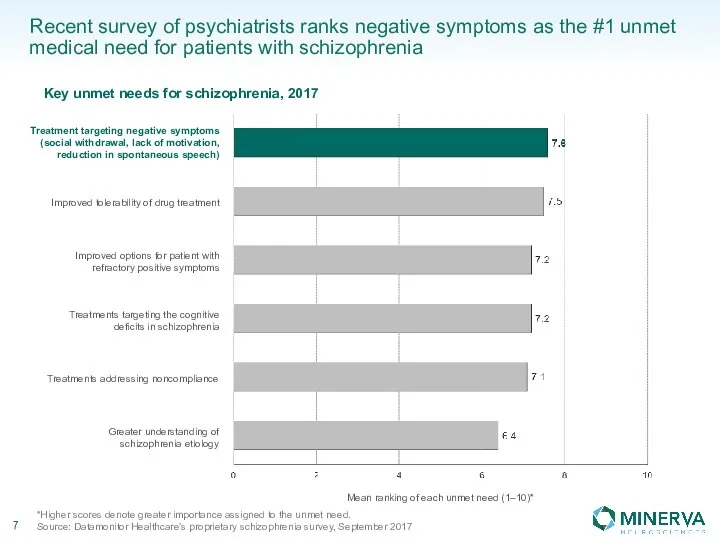
Recent survey of psychiatrists ranks negative symptoms as the #1 unmet
Recent survey of psychiatrists ranks negative symptoms as the #1 unmet
Roluperidone clinical data
Peer-reviewed data publications
Davidson, M., et al., Efficacy and Safety
Roluperidone clinical data
Peer-reviewed data publications
Davidson, M., et al., Efficacy and Safety
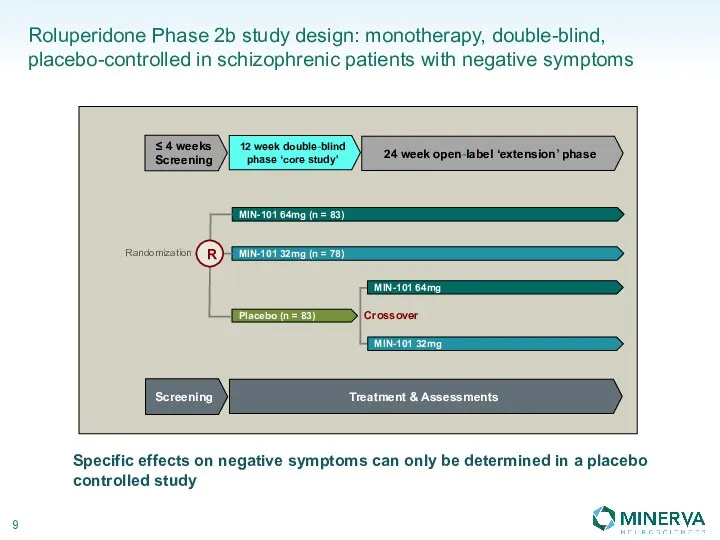
Roluperidone Phase 2b study design: monotherapy, double-blind,
placebo-controlled in schizophrenic patients
Roluperidone Phase 2b study design: monotherapy, double-blind, placebo-controlled in schizophrenic patients
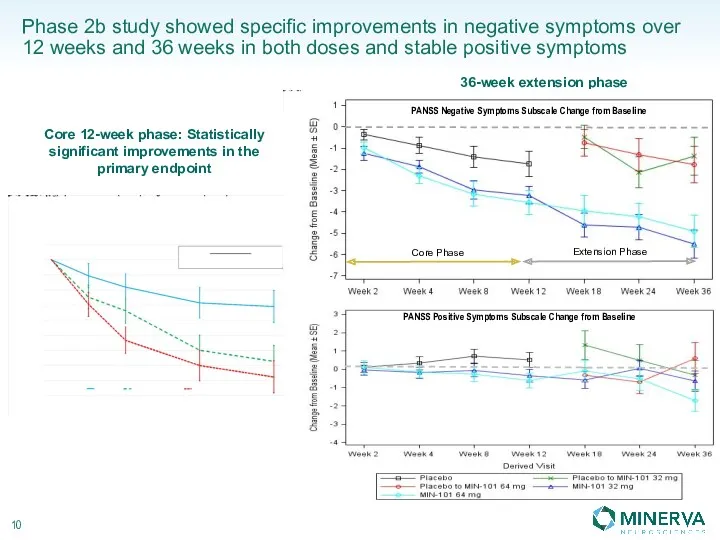
Phase 2b study showed specific improvements in negative symptoms over 12
Phase 2b study showed specific improvements in negative symptoms over 12
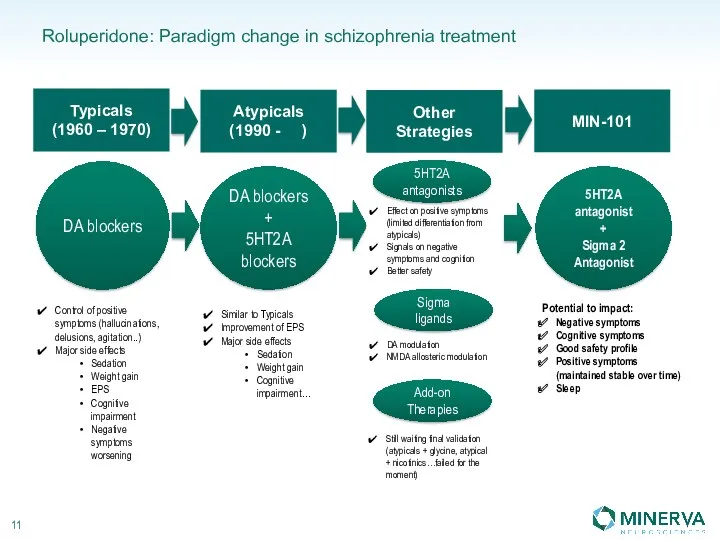
Roluperidone: Paradigm change in schizophrenia treatment
DA blockers
DA blockers
+
5HT2A
blockers
Typicals
(1960
Roluperidone: Paradigm change in schizophrenia treatment
DA blockers
DA blockers
+
5HT2A
blockers
Typicals
(1960
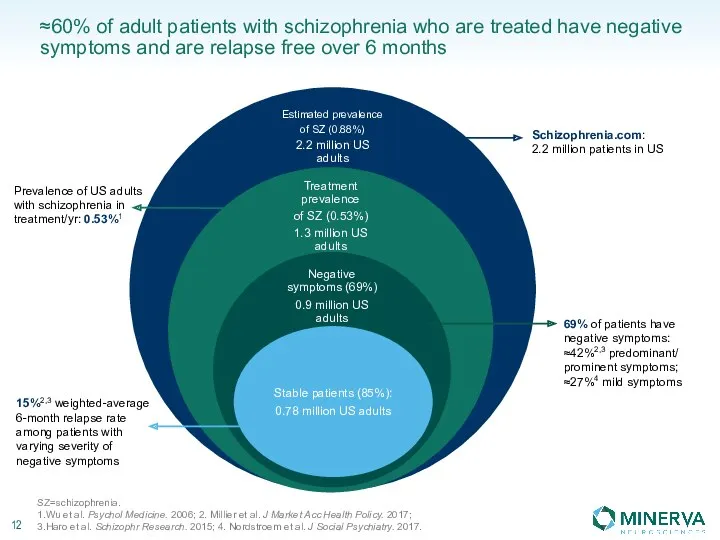
≈60% of adult patients with schizophrenia who are treated have negative
≈60% of adult patients with schizophrenia who are treated have negative
Roluperidone Phase 3
Designed to replicate successful Phase 2b
Design reviewed at end-of-Phase
Roluperidone Phase 3
Designed to replicate successful Phase 2b
Design reviewed at end-of-Phase
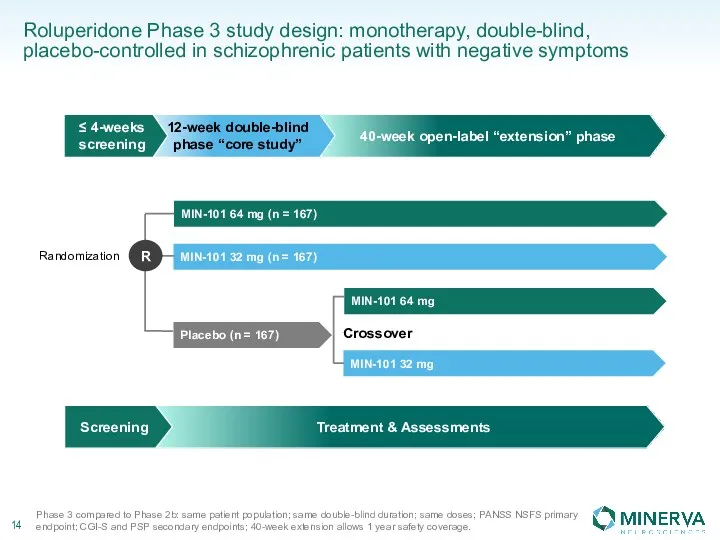
Roluperidone Phase 3 study design: monotherapy, double-blind, placebo-controlled in schizophrenic patients
Roluperidone Phase 3 study design: monotherapy, double-blind, placebo-controlled in schizophrenic patients
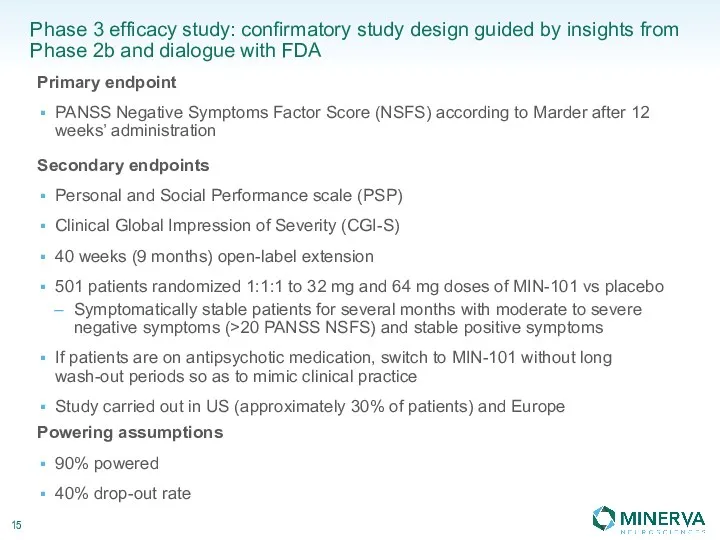
Phase 3 efficacy study: confirmatory study design guided by insights from
Phase 3 efficacy study: confirmatory study design guided by insights from
Seltorexant
MIN-202 / JNJ-42847922
A drug to treat insomnia and major depressive
Seltorexant
MIN-202 / JNJ-42847922 A drug to treat insomnia and major depressive
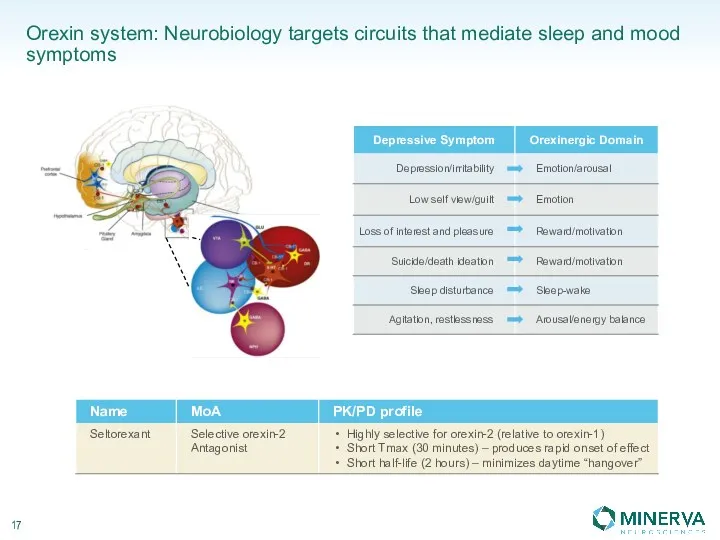
Orexin system: Neurobiology targets circuits that mediate sleep and mood symptoms
Orexin system: Neurobiology targets circuits that mediate sleep and mood symptoms
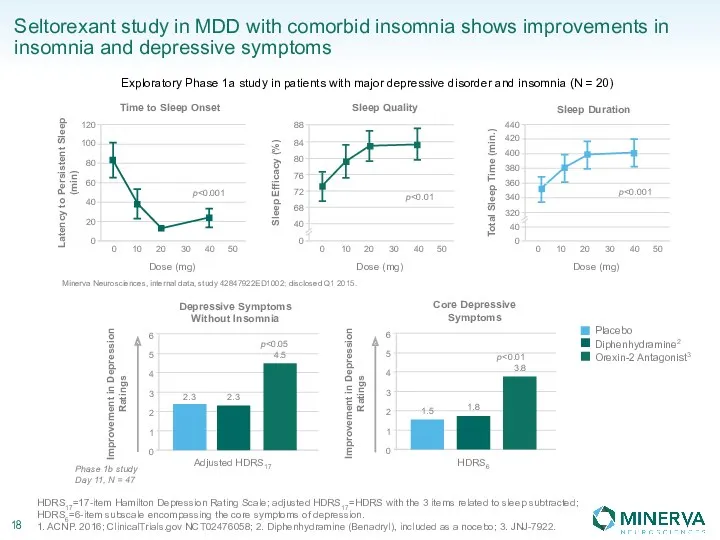
Seltorexant study in MDD with comorbid insomnia shows improvements in insomnia
Seltorexant study in MDD with comorbid insomnia shows improvements in insomnia
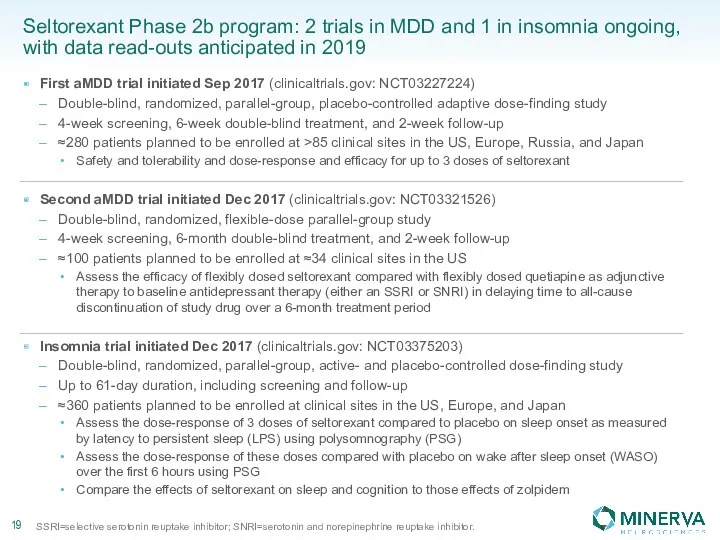
Seltorexant Phase 2b program: 2 trials in MDD and 1 in
Seltorexant Phase 2b program: 2 trials in MDD and 1 in
MIN-117
Addressing the unmet medical needs of patients with major depressive disorder
MIN-117
Addressing the unmet medical needs of patients with major depressive disorder
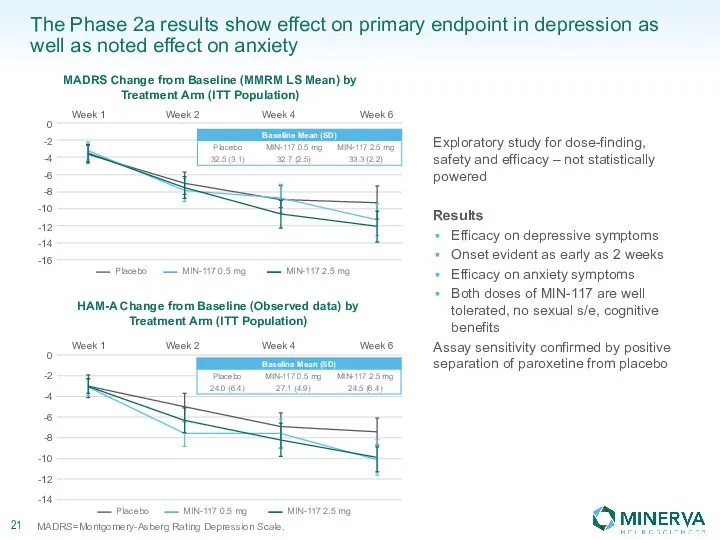
The Phase 2a results show effect on primary endpoint in depression
The Phase 2a results show effect on primary endpoint in depression
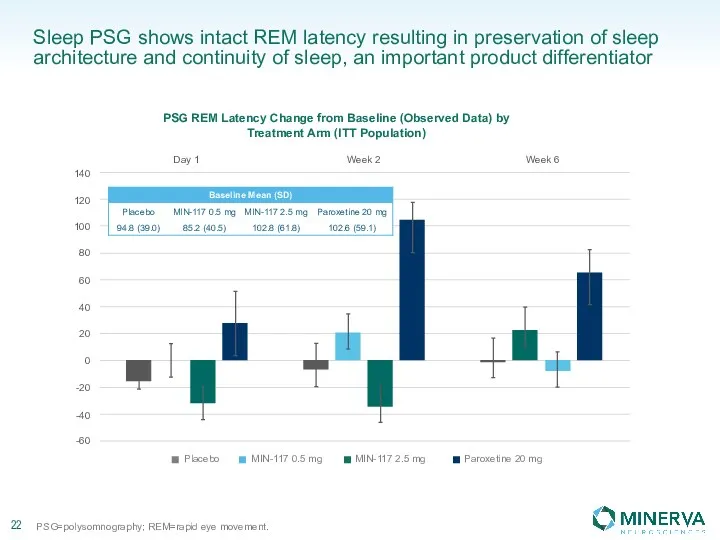
Sleep PSG shows intact REM latency resulting in preservation of sleep
Sleep PSG shows intact REM latency resulting in preservation of sleep
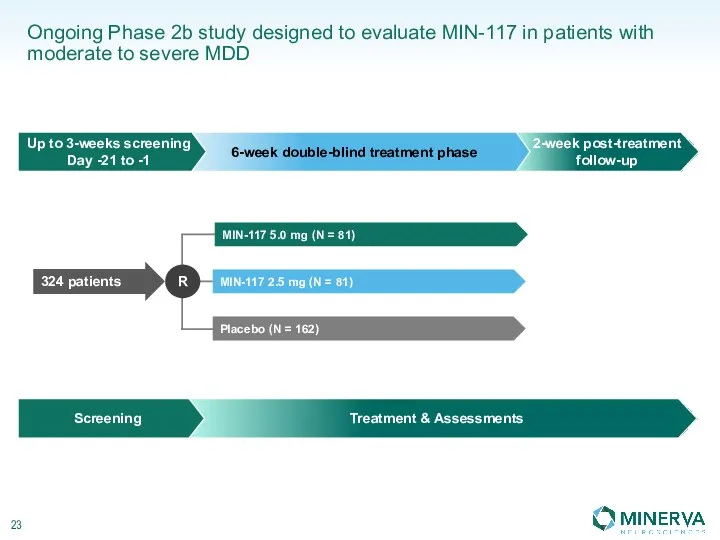
Ongoing Phase 2b study designed to evaluate MIN-117 in patients with
Ongoing Phase 2b study designed to evaluate MIN-117 in patients with
MIN-117 Phase 2b study objectives
Primary:
To evaluate the efficacy of 5.0
MIN-117 Phase 2b study objectives
Primary:
To evaluate the efficacy of 5.0
MIN-301
A protein drug with disease-modifying potential for the treatment of unmet
MIN-301
A protein drug with disease-modifying potential for the treatment of unmet
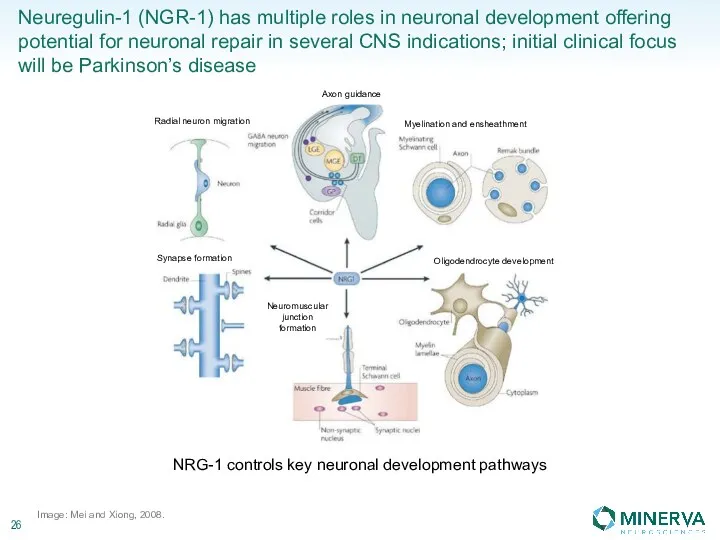
Neuregulin-1 (NGR-1) has multiple roles in neuronal development offering potential for
Neuregulin-1 (NGR-1) has multiple roles in neuronal development offering potential for
Strong financial position to deliver on major milestones
≈$121.1 million cash balance
(cash,
Strong financial position to deliver on major milestones
≈$121.1 million cash balance (cash,
 Стоматологическое материаловедение. Классификация материалов
Стоматологическое материаловедение. Классификация материалов Диффузные болезни соединительной ткани: системная красная волчанка, узелковой периартериит, склеродермия,дерматомиозит
Диффузные болезни соединительной ткани: системная красная волчанка, узелковой периартериит, склеродермия,дерматомиозит Пульпит временных зубов. Клиника
Пульпит временных зубов. Клиника Тұқым қуалайтын мултьфакторлы аурулар
Тұқым қуалайтын мултьфакторлы аурулар Лекарственные средства, влияющие на эфферентную иннервацию. Вегетотропные средства (Лекция 4)
Лекарственные средства, влияющие на эфферентную иннервацию. Вегетотропные средства (Лекция 4) Сәулелену.Ғарыштық сәулелену
Сәулелену.Ғарыштық сәулелену Autoimmune disease of the skin
Autoimmune disease of the skin Гипоксия
Гипоксия Легионеллездің стандартты анықтамасы
Легионеллездің стандартты анықтамасы Хвороби викликані вірусом
Хвороби викликані вірусом Отбасын құруды жоспарлау
Отбасын құруды жоспарлау Заболевания щитовидной железы. Анатомия, синдромы
Заболевания щитовидной железы. Анатомия, синдромы Мышцы человека
Мышцы человека Взаимосвязь пищевых аддикций с уровнем тревоги и депрессии
Взаимосвязь пищевых аддикций с уровнем тревоги и депрессии Пародонтологический инструментарий
Пародонтологический инструментарий Кисты и кистозные опухоли поджелудочной железы. Классификация, диагностика, принципы лечения
Кисты и кистозные опухоли поджелудочной железы. Классификация, диагностика, принципы лечения Порядок медицинского отбора и направления больных на санаторно-курортное лечение
Порядок медицинского отбора и направления больных на санаторно-курортное лечение Профилактика и лечение ОРЗ и гриппа
Профилактика и лечение ОРЗ и гриппа Болезни, обусловленные воздействием производственной пыли (пневмокониозы, пылевой бронхит, бронхиальная астма)
Болезни, обусловленные воздействием производственной пыли (пневмокониозы, пылевой бронхит, бронхиальная астма) Особенности терапии ОНМК (ИИ) в остром периоде
Особенности терапии ОНМК (ИИ) в остром периоде Тазовое предлежание плода (КубГМУ Live)
Тазовое предлежание плода (КубГМУ Live) Повреждения: некроз, атрофия, апоптоз
Повреждения: некроз, атрофия, апоптоз Психотерапия кризисных состояний. Кризисы – определение понятий
Психотерапия кризисных состояний. Кризисы – определение понятий Первые рекомендации МФККи КП по первой помощи и реанимации
Первые рекомендации МФККи КП по первой помощи и реанимации Анафилактические и анафилактоидные реакции в практике анестезиолога
Анафилактические и анафилактоидные реакции в практике анестезиолога Общие принципы диагностики и лечения сифилиса
Общие принципы диагностики и лечения сифилиса Безсоння
Безсоння Гестоз кезінде жүктілікті, босануды жүргізу. Гестоздың қарқынды терапиясының принциптері
Гестоз кезінде жүктілікті, босануды жүргізу. Гестоздың қарқынды терапиясының принциптері