- Anatomy of the Breast

Содержание
- 2. Anatomy of the Breast
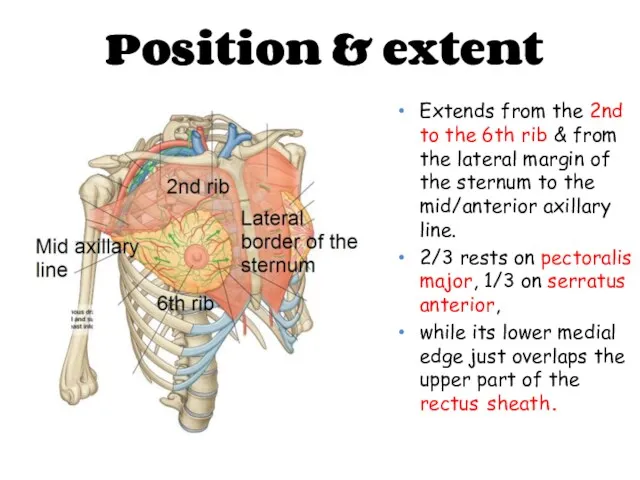
- 3. Position & extent Extends from the 2nd to the 6th rib & from the lateral margin
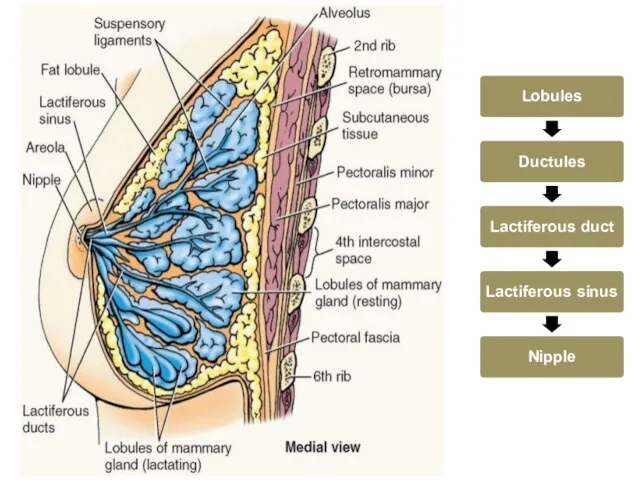
- 4. Structure of the Breast The lobule is the basic structural unit of the mammary gland.The number
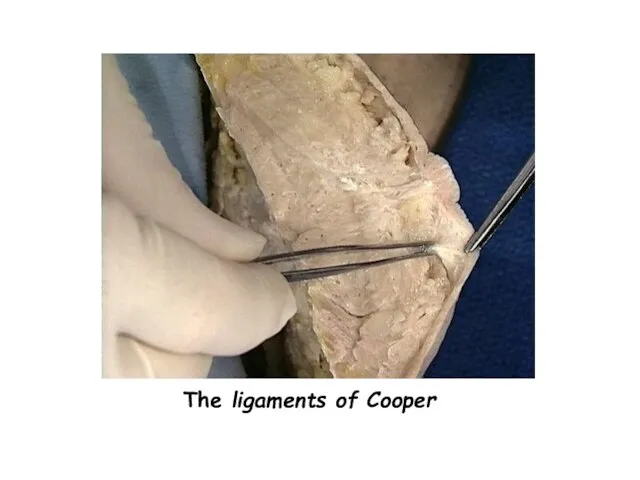
- 5. The ligaments of Cooper are hollow conical projections of fibrous tissue filled with breast tissue; the
- 7. The ligaments of Cooper
- 8. Blood supply
- 9. Internal thoracic”mammary” artery – perforating branches Axillary artery – Lateral thoracic artery ”mainly” Superior thoracic artery
- 10. Venous drainage Sub areolar venous plexus Posterior intercostal veins communicate with internal vertebral venous plexus veins
- 11. • Cutaneous innervation • Medial pectoral nerve • Lateral pectoral nerve • Long thoracic nerve Nerves
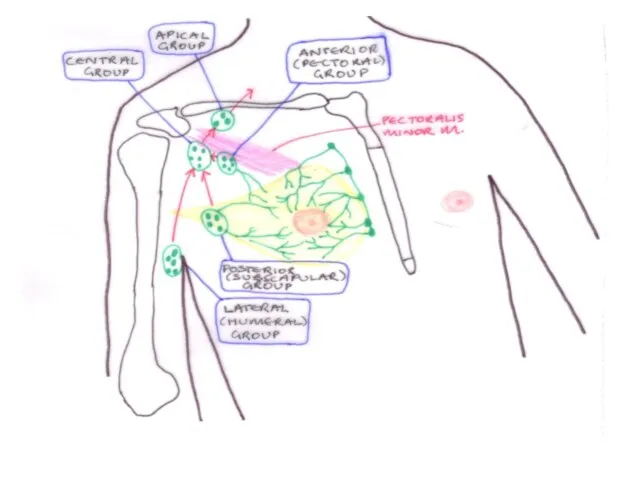
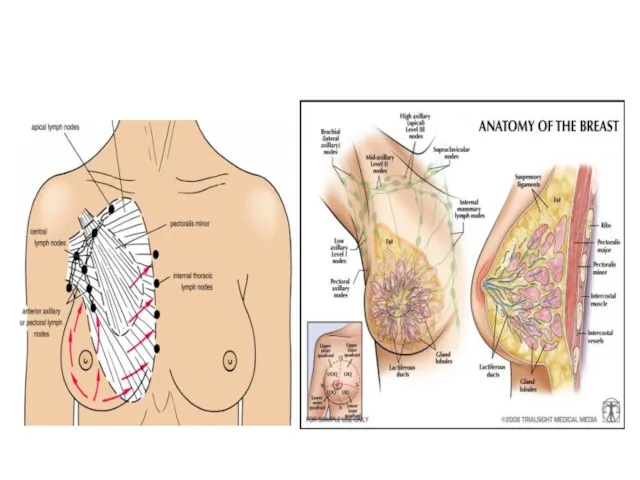
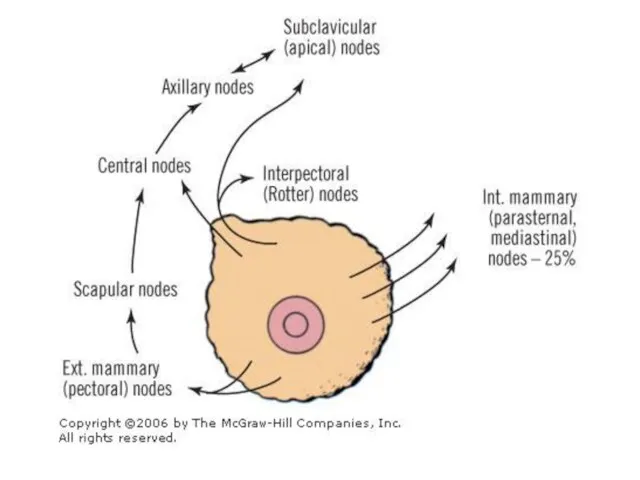
- 12. The lymphatics of the breast drain predominantly into the axillary and internal mammary lymph nodes. The
- 17. Physiology of the Breast
- 18. GROWTH HORMONE , PROLACTIN , ADRENAL GLUCOCORTICOIDS , INSULIN
- 20. Hypothalamic-hypophysial Portal system Growth hormone , Parathyriod hormone, cortisol insulin
- 22. The breast glands and ducts begin to shrink and disappear. Connective tissue supporting the glands becomes
- 23. Benign Breast Disease
- 24. Benign Breast Disease The most common cause of breast problems. 30% of women will suffer from
- 25. Benign breast disease Benign conditions of the nipple. Aberrations of normal development & involution. Fibroadenomas &
- 26. Conditions of the nipple 1-Nipple retraction
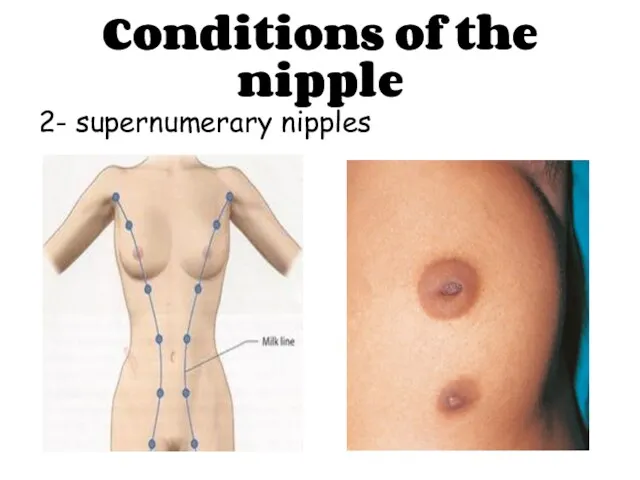
- 27. Conditions of the nipple 2- supernumerary nipples
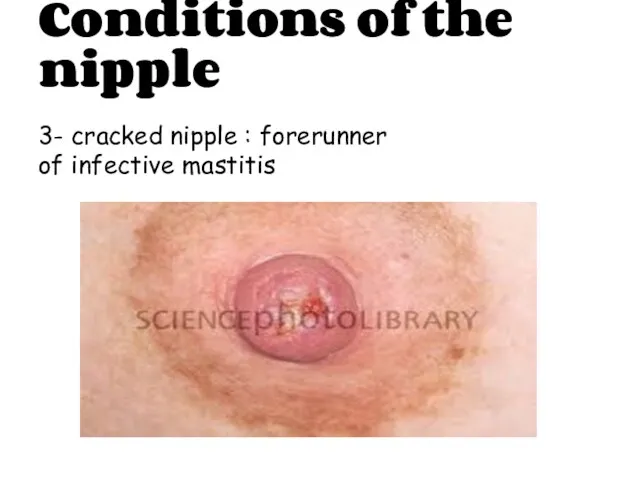
- 28. Conditions of the nipple 3- cracked nipple : forerunner of infective mastitis
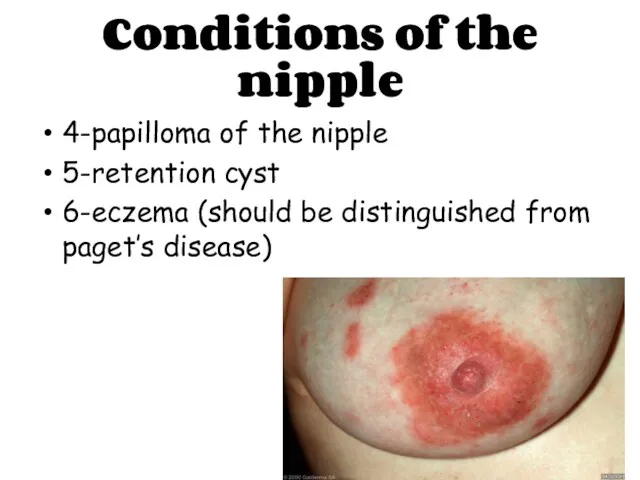
- 29. Conditions of the nipple 4-papilloma of the nipple 5-retention cyst 6-eczema (should be distinguished from paget’s
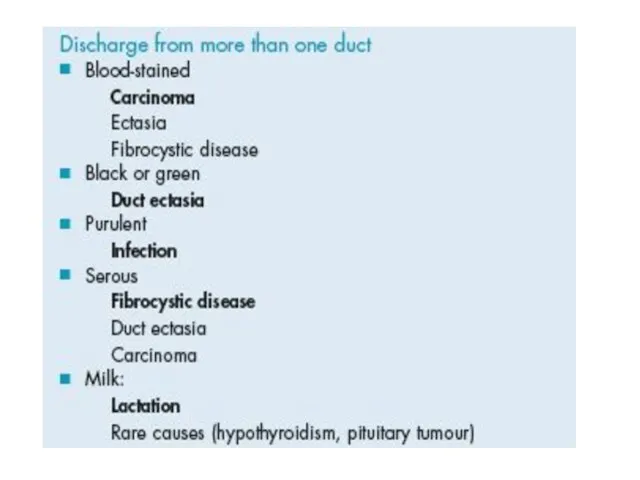
- 31. 7- Nipple discharge
- 33. Aberrations of normal development & involution
- 34. Aberrations of normal development & involution Cyst formation Fibrosis Hyperplasia Papillomatosis
- 35. ANDI Breast cysts
- 36. Fibroadenomas & Phyllodes Tumor:
- 37. Acute and Subacute Inflammations of the Breast:
- 38. 1- Bacterial mastitis & breast abscess:
- 39. 2- Mondor’s disease: ? Should be distinguished from Lymphangitis caused by cancer.
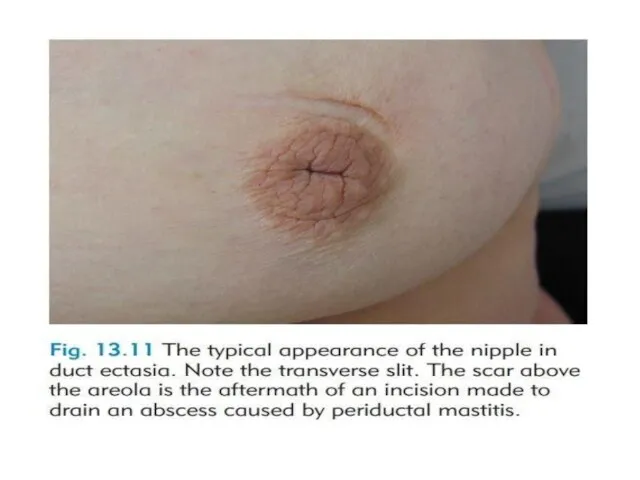
- 40. 3- Duct ectasia/periductal mastitis: Nipple Discharge. Periductal Mastitis. Abscess. Fistula. Nipple retraction. mass.
- 42. Injuries to the Breast: 1- Haematoma. 2-Traumatic fat necrosis.
- 43. Congenital Abnormalities:
- 44. 1- Amazia & polymazia:
- 45. 2- Mastitis of infants:
- 46. 3- Diffuse hypertrophy:
- 47. Malignant diseases CARCINOMA OF THE BREAST
- 48. Breast cancer is the second most common cancer with nearly 1.7 million new cases in 2012.
- 49. Aetiological factors Geographical… Age… Gender… Genetic… Diet… Endocrine… Previous radiation…
- 50. Pathogenesis Genetic factor… Hormonal factor… Enviromental factor…
- 51. Histopathologic classification Ductal ------ Lobular Invasive ------ In situ
- 52. Breast carcinoma in situ
- 53. Ductal carcinoma in situ (DCIS)
- 54. Lobular carcinoma in situ (LCIS)
- 55. In situ carcinoma is pre-invasive cancer. Becoming increasingly common. At least 20% of patients will develop
- 56. Treatment Surgical excision Mastectomy? Partial mastectomy with safety margins > 1cm Radiotherapy?
- 57. Invasive breast carcinoma
- 58. Invasive Ductal carcinoma (IDC)
- 59. Invasive Lobular carcinoma (ILC)
- 60. Other rarer variants Colloid (mucinous) carcinoma: produce abundant mucin. Medullary carcinoma: solid sheets of large cells
- 61. Inflammatory breast cancer
- 62. Rare, highly aggressive cancer that presents as a painful, swollen breast, which is warm with cutaneous
- 63. Paget Disease of the Nipple
- 64. It is a superficial manifestation of an underlying breast carcinoma (IDC or DCIS). Presents as an
- 65. The spread of breast cancer Local spread… Lymphatic metastasis… Hematogenous spread…
- 66. Phenomena resulting from lymphatic obstruction in advanced breast cancer:
- 67. Peau d’orange
- 68. Cancer-en-cuirasse
- 69. Lymphangiosarcoma
- 71. Breast Carcinoma Grading The degree of differentiation: Well differentiated. Moderately differentiated. Poorly differentiated.
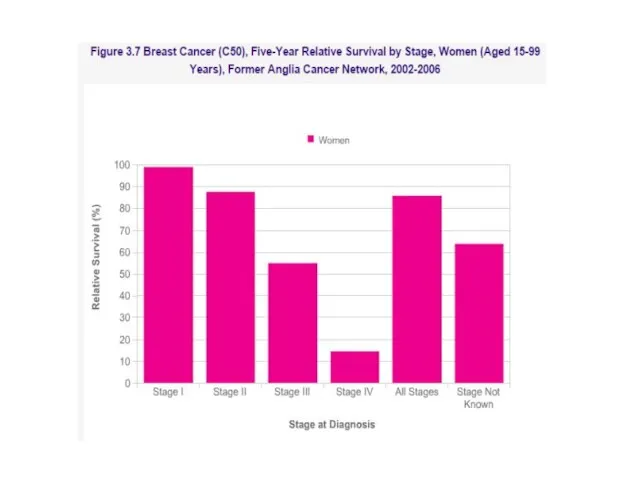
- 72. Breast cancer staging TNM staging takes into account: The size of the tumour (T). Whether the
- 75. Skeletal isotope bone scan showing multiple ‘hot-spots’ due to metastases.
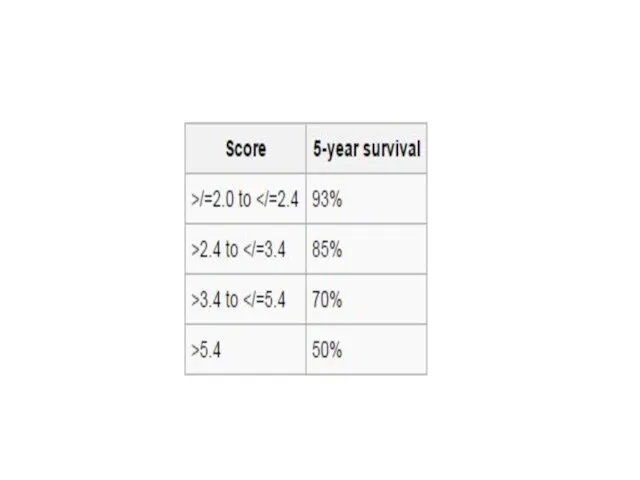
- 76. Prognosis of breast cancer The best indicators of likely prognosis in breast cancer remain tumour size,
- 79. Breast Cancer in Men Breast Cancer in Men accounts for less than 1% of male cancers
- 80. Screening & Imaging Breast screening aims to find breast cancers early. It uses an X-ray test
- 82. Early Detection Plan
- 83. Screening Protocol
- 84. Mammography Soft tissue radiographs are taken by placing the breast in direct contact with ultrasensitive film
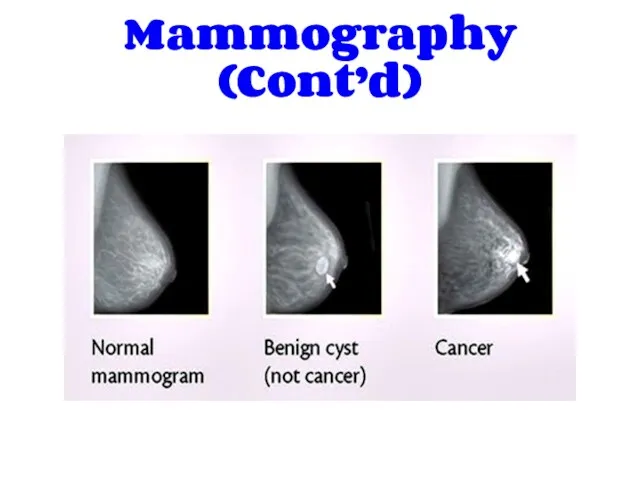
- 85. Mammography (Cont’d)
- 86. Ultrasonography Ultrasound is particularly useful in young women with dense breasts in whom mammograms are difficult
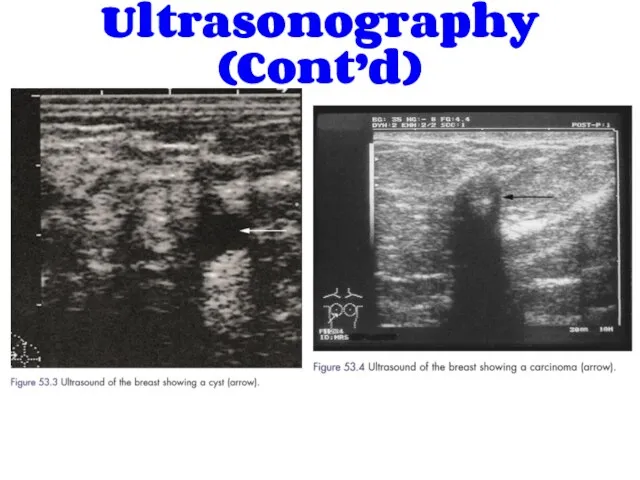
- 87. Ultrasonography (Cont’d)
- 88. Magnetic Resonance Imaging Magnetic resonance imaging (MRI) is of increasing interest to breast surgeons in a
- 89. Magnetic Resonance Imaging (Cont’d) Magnetic resonance imaging scan of the breasts showing carcinoma of the left
- 90. History:
- 91. PRESENTATION OF BREAST DISEASE Breast disease presents in three main ways: lump, which may or may
- 92. Breast lump (Mass) When did the patient first notice it & how? Site Painful or not
- 93. Breast pain Duration SOCRATES Relation with periods Nipple discharge Discoloration and hotness of skin Fever, fatigue,
- 94. Nipple Discharge Site (nipple itself or adjacent area) Episodic or continuous Color Viscosity Passive or induced
- 95. Skin changes Skin dimple Eczema Indrawing of the skin Ulceration Discoloration Redness and hotness Overall swelling
- 96. Nipple changes Is it retracted or destroyed Uni/bilateral Can it be everted easily
- 97. Gynecological symptoms : Last menstrual cycle duration menarche menopause Any changes: Increased blood, clots or irregularity
- 98. Past History (e.g breast cyst) Drug History (e.g oral contraceptives, hormone replacement therapy) Family History (
- 99. Physical Examination:
- 100. Position Inspection Palpation
- 101. position The patient must be fully undressed to the waist. sitting 45 degrees Patients sometimes say
- 102. Inspection Stand or sit directly in front of the patient, inspect both breasts and look for
- 103. 4. Nipples & Areolae: Depression Destruction Discoloration Displacement Deviation Discharge
- 104. To check for accessory nipple: check the nipple line ( axilla-->groin), if the nipple is inverted
- 105. (Supraclavicular fossa) Ectopic breast tissue in the anterior axillary fold Visible LN in arm, axilla and
- 106. B) Arms Over Head : Skin changes (esp. tethering) are more prominent, and to expose the
- 107. PALPATION Ask the patient to lay down with her hand ipsilateral to the breast. Ask where
- 108. The breast should be palpated with the flat of the fingers and not with the palm
- 109. * If there is a lump we should analyze it : Lump Site Size Shape Edge
- 110. Relations of the lump to skin
- 112. Скачать презентацию
Anatomy of the Breast
Anatomy of the Breast
Position & extent
Extends from the 2nd to the 6th rib &
Position & extent
Extends from the 2nd to the 6th rib &
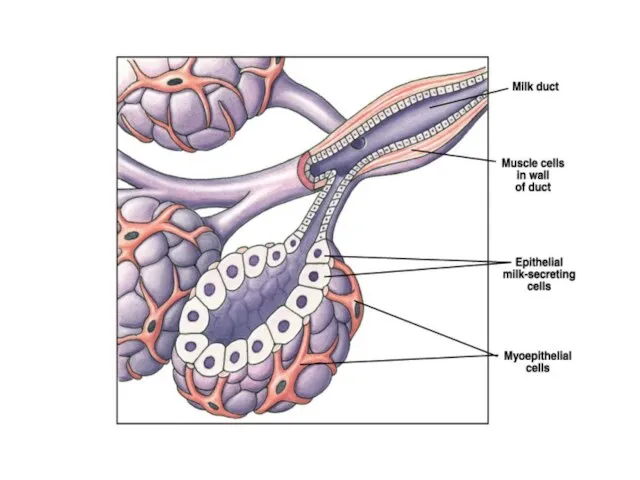
Structure of the Breast
The lobule is the basic structural unit of
Structure of the Breast
The lobule is the basic structural unit of
The ligaments of Cooper are hollow conical projections of fibrous tissue
The ligaments of Cooper are hollow conical projections of fibrous tissue
The ligaments of Cooper
The ligaments of Cooper
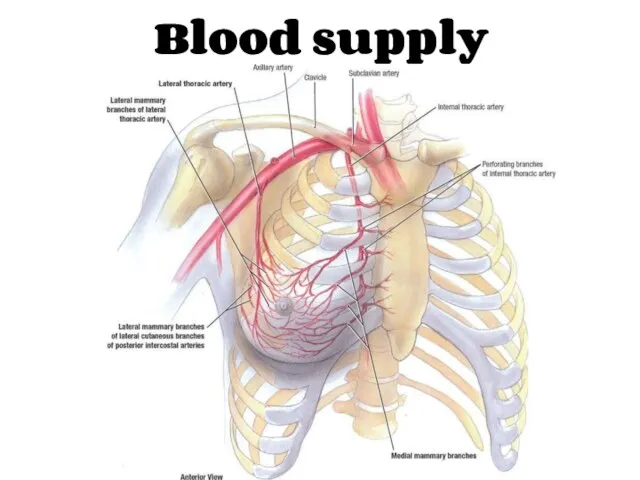
Blood supply
Blood supply
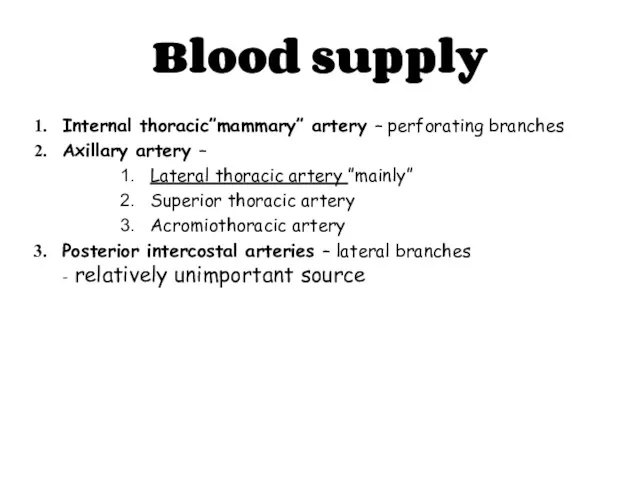
Internal thoracic”mammary” artery – perforating branches
Axillary artery –
Lateral thoracic artery
Internal thoracic”mammary” artery – perforating branches
Axillary artery –
Lateral thoracic artery
Venous drainage
Sub areolar venous plexus
Posterior intercostal veins communicate with internal vertebral
Venous drainage
Sub areolar venous plexus
Posterior intercostal veins communicate with internal vertebral
• Cutaneous innervation
• Medial pectoral nerve
• Lateral pectoral nerve
• Long thoracic
• Medial pectoral nerve
• Lateral pectoral nerve
• Long thoracic
The lymphatics of the breast drain predominantly into the axillary and
The lymphatics of the breast drain predominantly into the axillary and
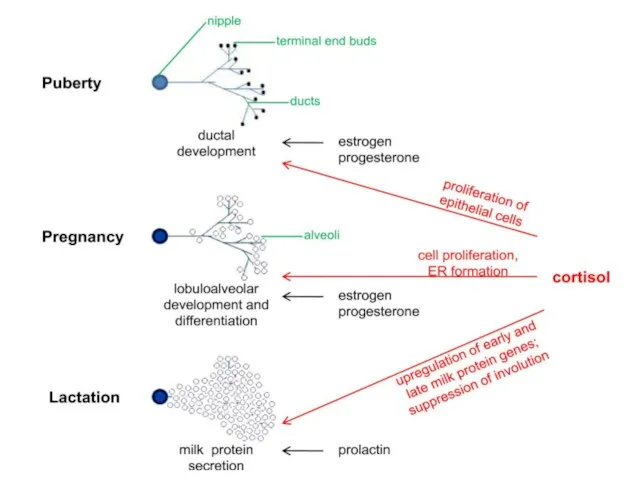
Physiology of the Breast
Physiology of the Breast
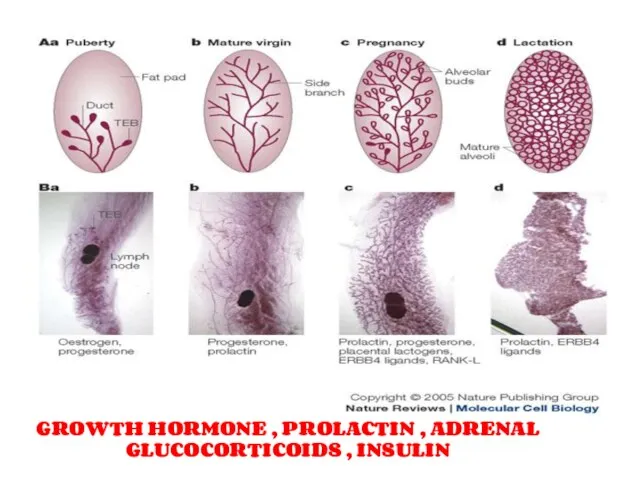
GROWTH HORMONE , PROLACTIN , ADRENAL GLUCOCORTICOIDS , INSULIN
GROWTH HORMONE , PROLACTIN , ADRENAL GLUCOCORTICOIDS , INSULIN
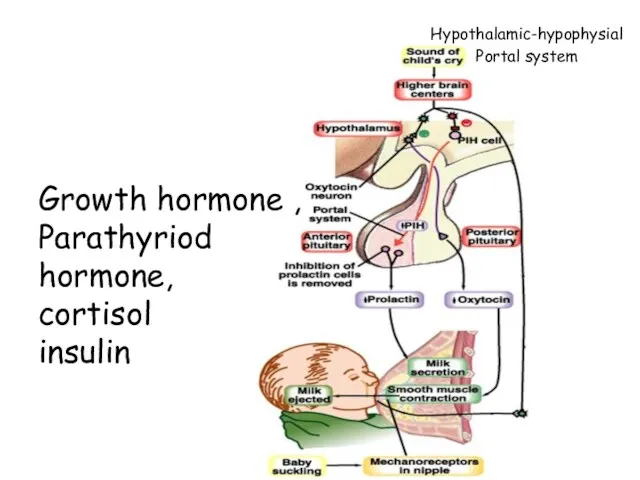
Hypothalamic-hypophysial
Portal system
Growth hormone ,
Parathyriod hormone,
cortisol
insulin
Hypothalamic-hypophysial
Portal system
Growth hormone ,
Parathyriod hormone,
cortisol
insulin
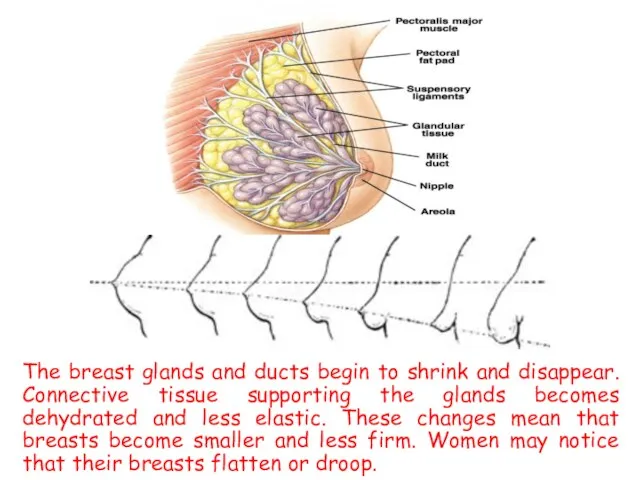
The breast glands and ducts begin to shrink and disappear. Connective
The breast glands and ducts begin to shrink and disappear. Connective

Benign Breast Disease
Benign Breast Disease
Benign Breast Disease
The most common cause of breast problems.
30% of
Benign Breast Disease
The most common cause of breast problems.
30% of
Benign breast disease
Benign conditions of the nipple.
Aberrations of normal development &
Benign breast disease
Benign conditions of the nipple.
Aberrations of normal development &
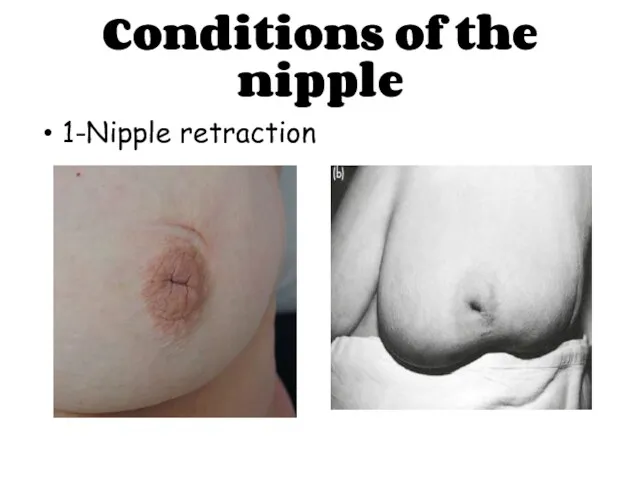
Conditions of the nipple
1-Nipple retraction
Conditions of the nipple
1-Nipple retraction
Conditions of the nipple
2- supernumerary nipples
Conditions of the nipple
2- supernumerary nipples
Conditions of the nipple
3- cracked nipple : forerunner of infective mastitis
Conditions of the nipple
3- cracked nipple : forerunner of infective mastitis
Conditions of the nipple
4-papilloma of the nipple
5-retention cyst
6-eczema (should be distinguished
Conditions of the nipple
4-papilloma of the nipple
5-retention cyst
6-eczema (should be distinguished

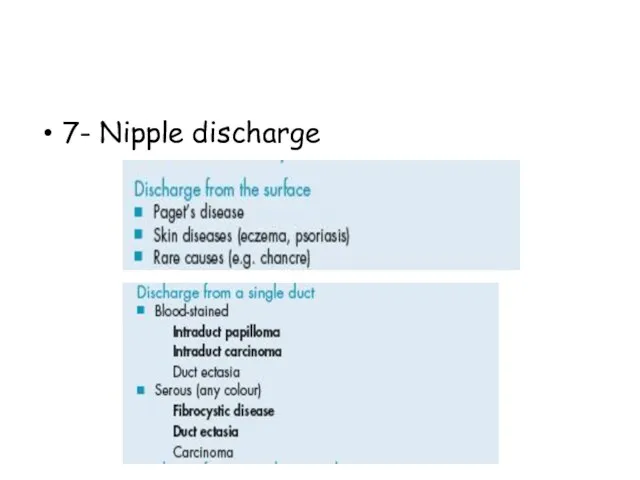
7- Nipple discharge
7- Nipple discharge
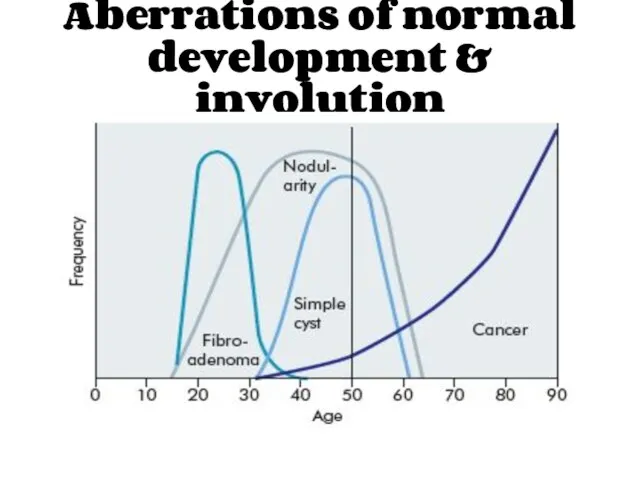
Aberrations of normal development & involution
Aberrations of normal development & involution
Aberrations of normal development & involution
Cyst formation
Fibrosis
Hyperplasia
Papillomatosis
Aberrations of normal development & involution
Cyst formation
Fibrosis
Hyperplasia
Papillomatosis
ANDI
Breast cysts
ANDI
Breast cysts
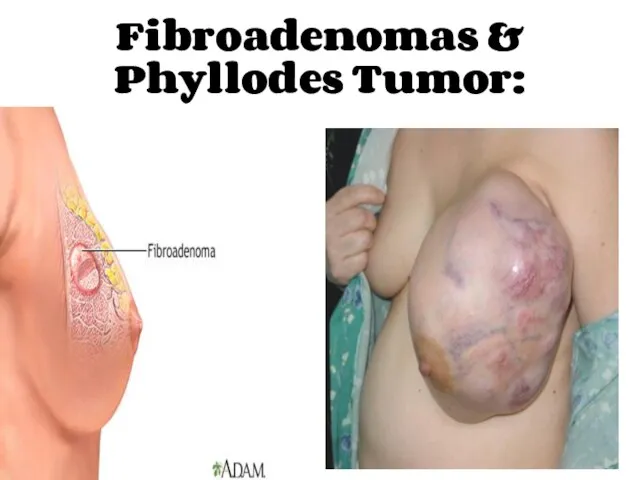
Fibroadenomas & Phyllodes Tumor:
Fibroadenomas & Phyllodes Tumor:
Acute and Subacute Inflammations of the Breast:
Acute and Subacute Inflammations of the Breast:

1- Bacterial mastitis & breast abscess:
1- Bacterial mastitis & breast abscess:
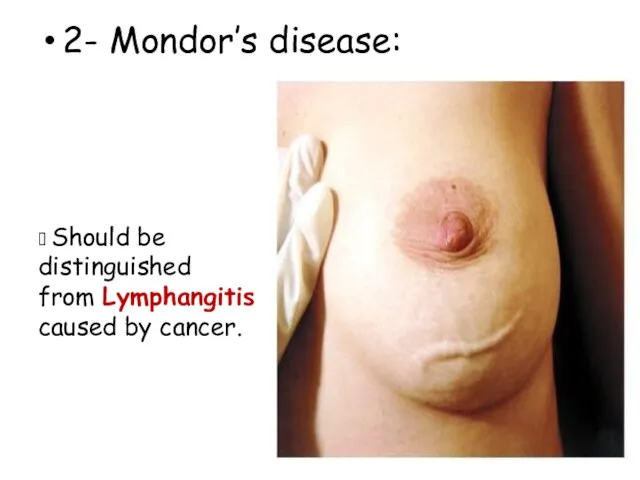
2- Mondor’s disease:
? Should be distinguished from Lymphangitis caused by cancer.
2- Mondor’s disease:
? Should be distinguished from Lymphangitis caused by cancer.
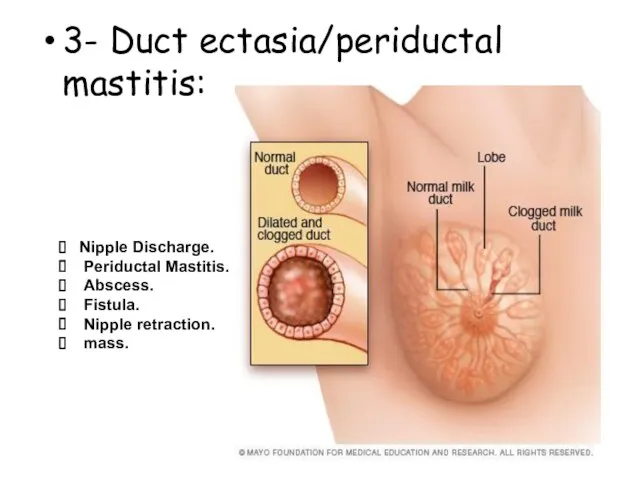
3- Duct ectasia/periductal mastitis:
Nipple Discharge.
Periductal Mastitis.
Abscess.
Fistula.
Nipple
3- Duct ectasia/periductal mastitis:
Nipple Discharge.
Periductal Mastitis.
Abscess.
Fistula.
Nipple
Injuries to the Breast:
1- Haematoma.
2-Traumatic fat necrosis.
Injuries to the Breast:
1- Haematoma.
2-Traumatic fat necrosis.
Congenital Abnormalities:
Congenital Abnormalities:
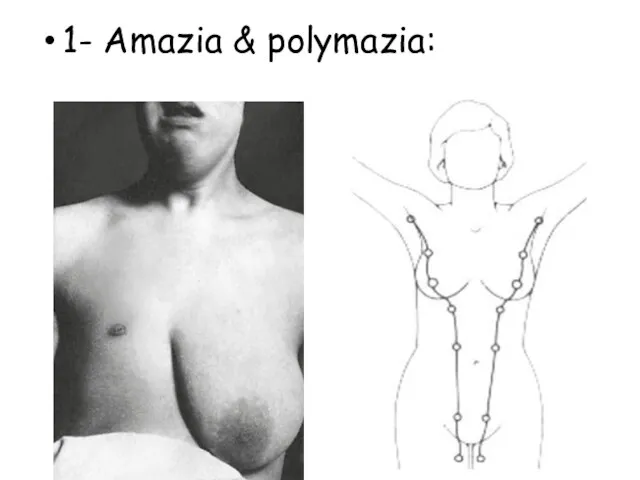
1- Amazia & polymazia:
1- Amazia & polymazia:
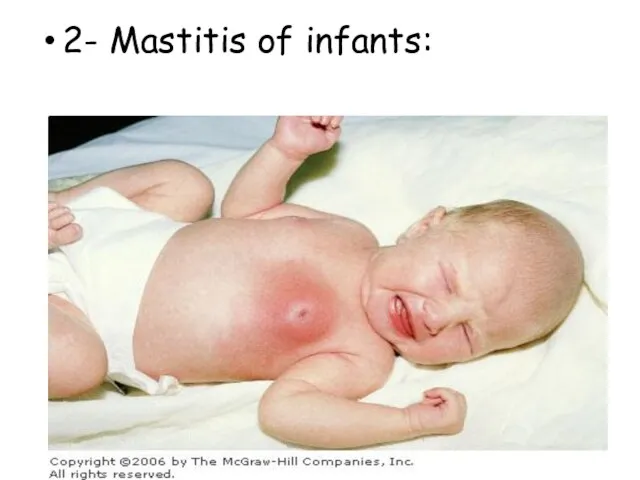
2- Mastitis of infants:
2- Mastitis of infants:
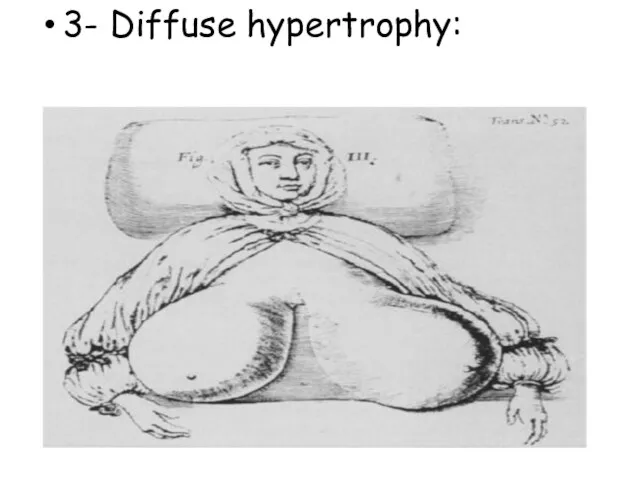
3- Diffuse hypertrophy:
3- Diffuse hypertrophy:
Malignant diseases
CARCINOMA OF THE BREAST
Malignant diseases
CARCINOMA OF THE BREAST
Breast cancer is the second most common cancer with nearly 1.7
Breast cancer is the second most common cancer with nearly 1.7
Aetiological factors
Geographical…
Age…
Gender…
Genetic…
Diet…
Endocrine…
Previous radiation…
Aetiological factors
Geographical…
Age…
Gender…
Genetic…
Diet…
Endocrine…
Previous radiation…
Pathogenesis
Genetic factor…
Hormonal factor…
Enviromental factor…
Pathogenesis
Genetic factor…
Hormonal factor…
Enviromental factor…
Histopathologic classification
Ductal ------ Lobular
Invasive ------ In situ
Histopathologic classification
Ductal ------ Lobular
Invasive ------ In situ
Breast carcinoma in situ
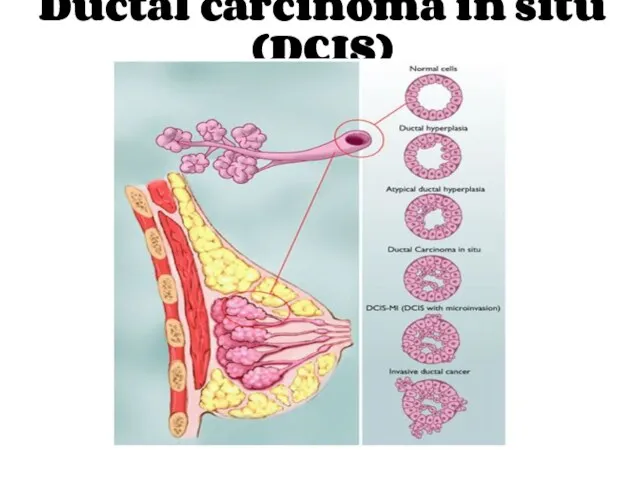
Ductal carcinoma in situ (DCIS)
Ductal carcinoma in situ (DCIS)
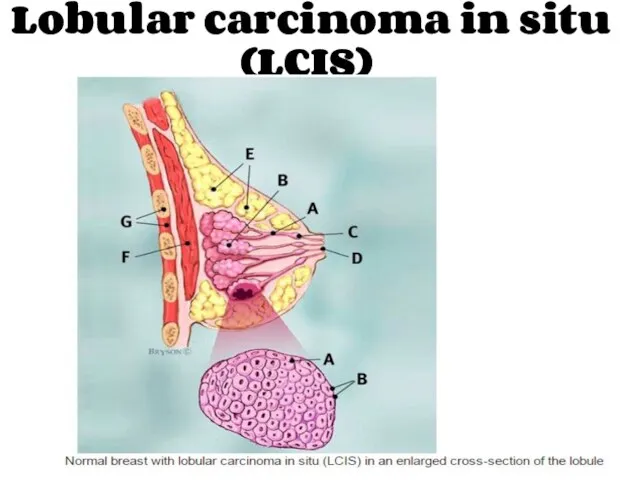
Lobular carcinoma in situ (LCIS)
Lobular carcinoma in situ (LCIS)
In situ carcinoma is pre-invasive cancer.
Becoming increasingly common.
At least 20% of
In situ carcinoma is pre-invasive cancer.
Becoming increasingly common.
At least 20% of
Treatment
Surgical excision
Mastectomy?
Partial mastectomy with safety margins > 1cm
Radiotherapy?
Treatment
Surgical excision
Mastectomy?
Partial mastectomy with safety margins > 1cm
Radiotherapy?
Invasive breast carcinoma
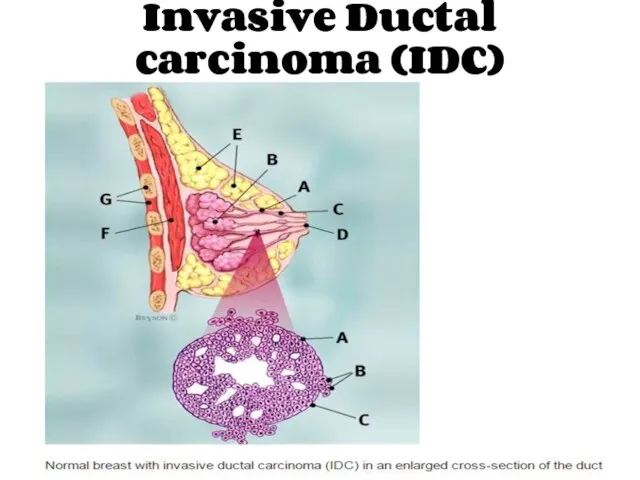
Invasive Ductal carcinoma (IDC)
Invasive Ductal carcinoma (IDC)
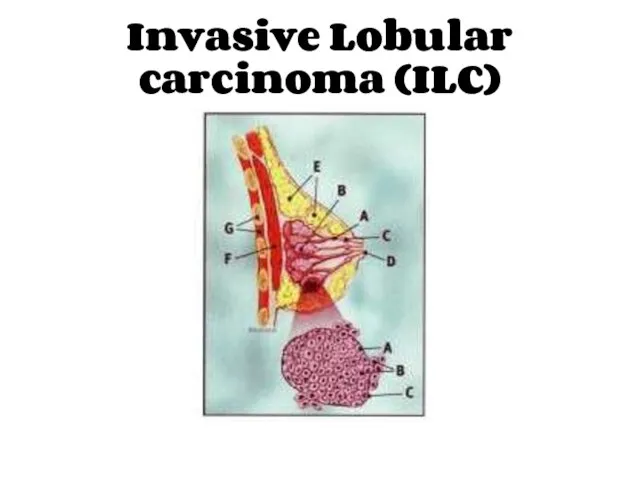
Invasive Lobular carcinoma (ILC)
Invasive Lobular carcinoma (ILC)
Other rarer variants
Colloid (mucinous) carcinoma: produce abundant mucin.
Medullary carcinoma: solid sheets
Other rarer variants
Colloid (mucinous) carcinoma: produce abundant mucin.
Medullary carcinoma: solid sheets
Inflammatory breast cancer
Inflammatory breast cancer
Rare, highly aggressive cancer that presents as a painful, swollen breast,
Rare, highly aggressive cancer that presents as a painful, swollen breast,

Paget Disease of the Nipple
Paget Disease of the Nipple
It is a superficial manifestation of an underlying breast carcinoma (IDC
It is a superficial manifestation of an underlying breast carcinoma (IDC
The spread of breast cancer
Local spread…
Lymphatic metastasis…
Hematogenous spread…
The spread of breast cancer
Local spread…
Lymphatic metastasis…
Hematogenous spread…
Phenomena resulting from lymphatic obstruction in advanced breast cancer:
Phenomena resulting from lymphatic obstruction in advanced breast cancer:
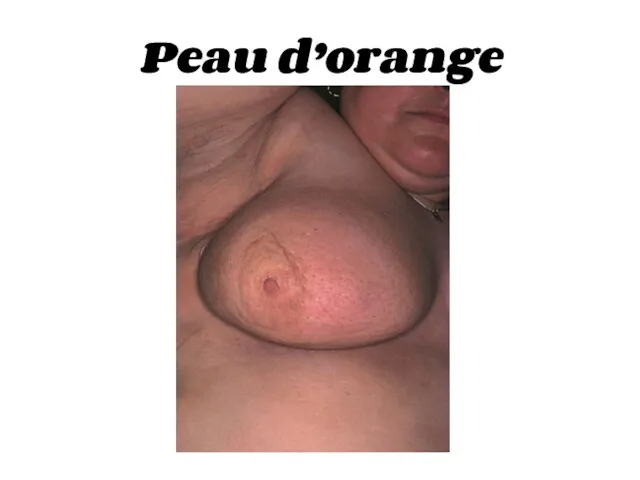
Peau d’orange
Peau d’orange

Cancer-en-cuirasse
Cancer-en-cuirasse

Lymphangiosarcoma
Lymphangiosarcoma

Breast Carcinoma Grading
The degree of differentiation:
Well differentiated.
Moderately differentiated.
Poorly differentiated.
Breast Carcinoma Grading
The degree of differentiation:
Well differentiated.
Moderately differentiated.
Poorly differentiated.
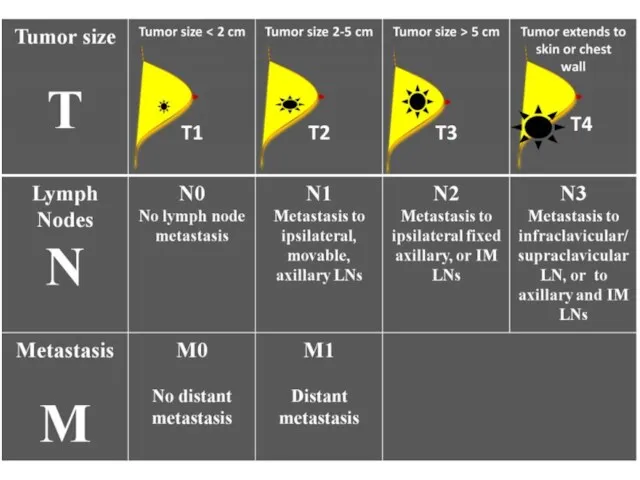
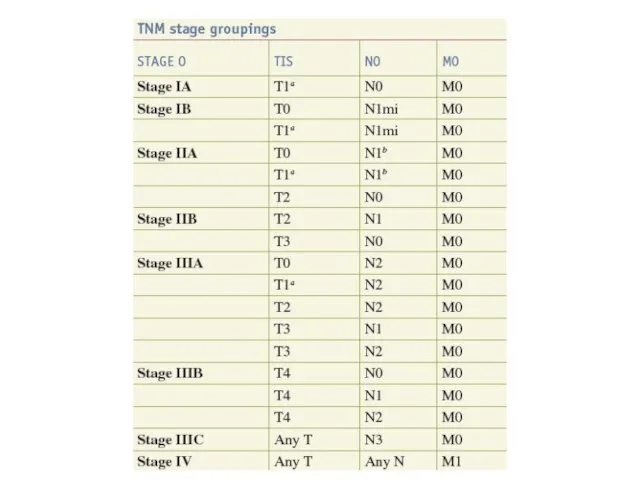
Breast cancer staging
TNM staging takes into account:
The size of the tumour
Breast cancer staging
TNM staging takes into account:
The size of the tumour
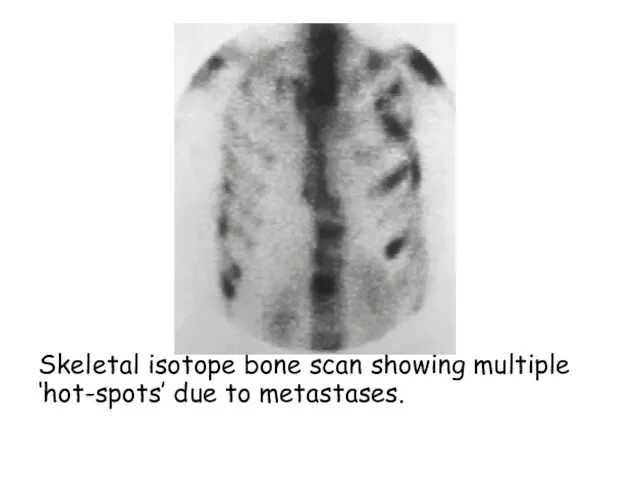
Skeletal isotope bone scan showing multiple ‘hot-spots’ due to metastases.
Skeletal isotope bone scan showing multiple ‘hot-spots’ due to metastases.
Prognosis of breast cancer
The best indicators of likely prognosis in breast
Prognosis of breast cancer
The best indicators of likely prognosis in breast
Breast Cancer in Men
Breast Cancer in Men accounts for less than
Breast Cancer in Men
Breast Cancer in Men accounts for less than
Screening & Imaging
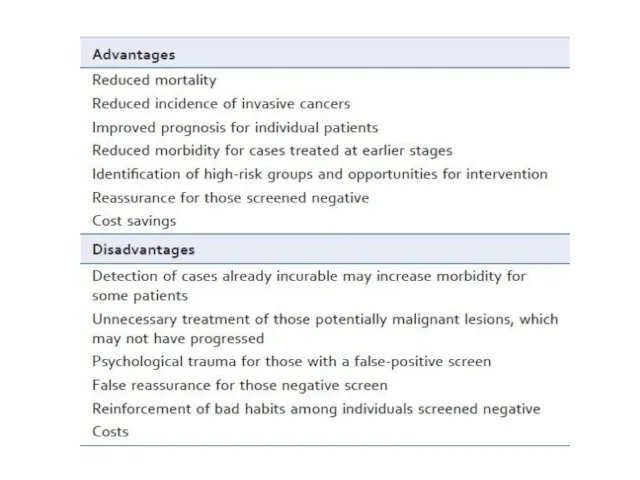
Breast screening aims to find breast cancers early. It
Screening & Imaging
Breast screening aims to find breast cancers early. It
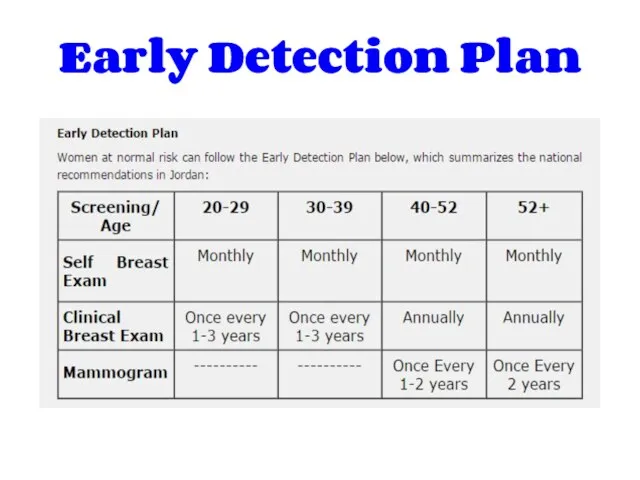
Early Detection Plan
Early Detection Plan
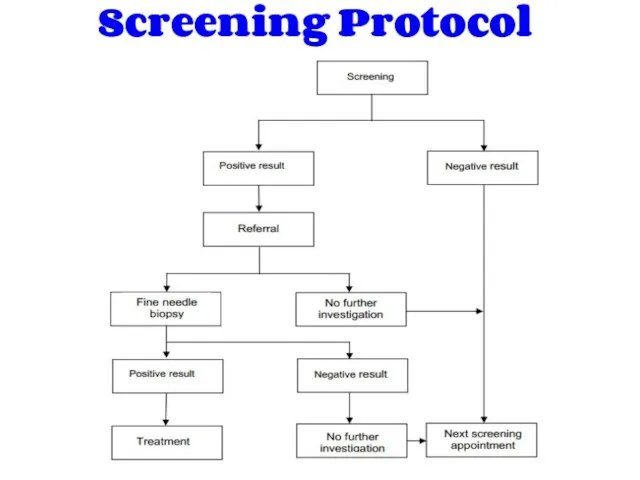
Screening Protocol
Screening Protocol
Mammography
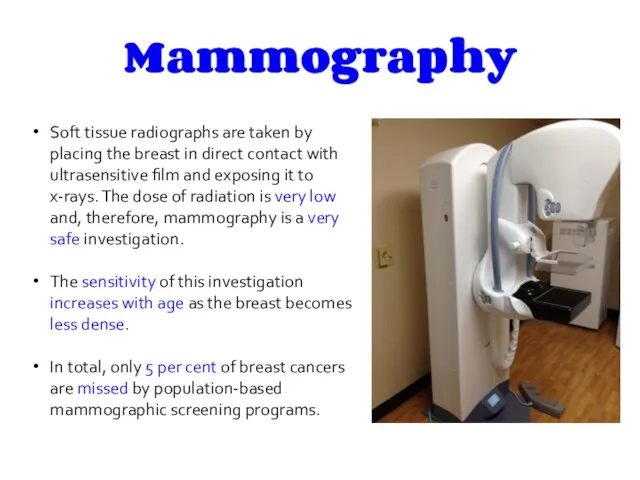
Soft tissue radiographs are taken by placing the breast in direct
Mammography
Soft tissue radiographs are taken by placing the breast in direct
Mammography (Cont’d)
Mammography (Cont’d)
Ultrasonography
Ultrasound is particularly useful in young women with dense breasts in
Ultrasonography
Ultrasound is particularly useful in young women with dense breasts in
Ultrasonography (Cont’d)
Ultrasonography (Cont’d)
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is of increasing interest to
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is of increasing interest to
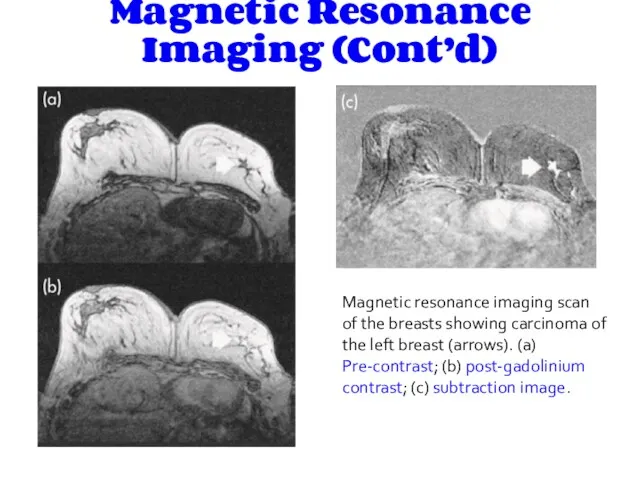
Magnetic Resonance Imaging (Cont’d)
Magnetic resonance imaging scan of the breasts showing
Magnetic Resonance Imaging (Cont’d)
Magnetic resonance imaging scan of the breasts showing
History:
History:
PRESENTATION OF BREAST DISEASE
Breast disease presents in three main ways:
lump,
PRESENTATION OF BREAST DISEASE
Breast disease presents in three main ways:
lump,
Breast lump (Mass)
When did the patient first notice it &
Breast lump (Mass)
When did the patient first notice it &
Breast pain
Duration
SOCRATES
Relation with periods
Nipple discharge
Discoloration and hotness of skin
Fever,
Breast pain
Duration
SOCRATES
Relation with periods
Nipple discharge
Discoloration and hotness of skin
Fever,
Nipple Discharge
Site (nipple itself or adjacent area)
Episodic or continuous
Color
Viscosity
Passive or induced
Uni/bilateral
Nipple Discharge
Site (nipple itself or adjacent area)
Episodic or continuous
Color
Viscosity
Passive or induced
Uni/bilateral
Skin changes
Skin dimple
Eczema
Indrawing of the skin
Ulceration
Discoloration
Redness and hotness
Overall swelling of
Skin changes
Skin dimple
Eczema
Indrawing of the skin
Ulceration
Discoloration
Redness and hotness
Overall swelling of
Nipple changes
Is it retracted or destroyed
Uni/bilateral
Can it be everted easily
Nipple changes
Is it retracted or destroyed
Uni/bilateral
Can it be everted easily
Gynecological symptoms :
Last menstrual cycle
duration
menarche
menopause
Any changes: Increased blood, clots or
Gynecological symptoms :
Last menstrual cycle
duration
menarche
menopause
Any changes: Increased blood, clots or
Past History (e.g breast cyst)
Drug History (e.g oral contraceptives, hormone replacement
Past History (e.g breast cyst)
Drug History (e.g oral contraceptives, hormone replacement
Physical Examination:
Physical Examination:
Position
Inspection
Palpation
Position
Inspection
Palpation
position
The patient must be fully undressed to the waist.
sitting 45 degrees
position
The patient must be fully undressed to the waist.
sitting 45 degrees
Inspection
Stand or sit directly in front of the patient, inspect both
Inspection
Stand or sit directly in front of the patient, inspect both
4. Nipples & Areolae:
Depression
Destruction
Discoloration
Displacement
Deviation
Discharge
4. Nipples & Areolae:
Depression
Destruction
Discoloration
Displacement
Deviation
Discharge
To check for accessory nipple: check the nipple line ( axilla-->groin),
To check for accessory nipple: check the nipple line ( axilla-->groin),
(Supraclavicular fossa)
Ectopic breast tissue in the anterior axillary fold
Visible
(Supraclavicular fossa)
Ectopic breast tissue in the anterior axillary fold
Visible
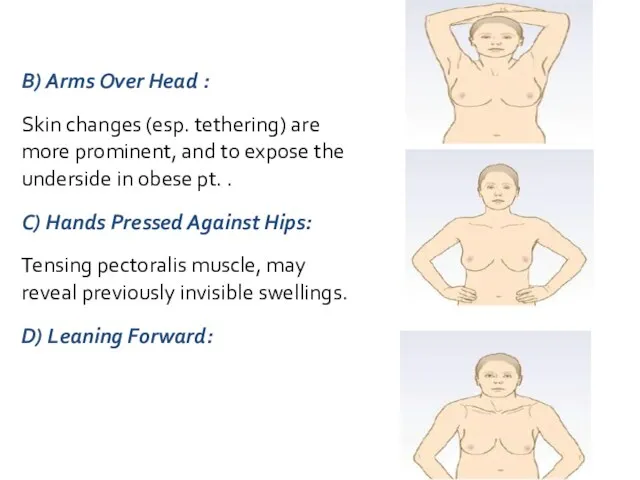
B) Arms Over Head :
Skin changes (esp. tethering) are more prominent,
B) Arms Over Head :
Skin changes (esp. tethering) are more prominent,
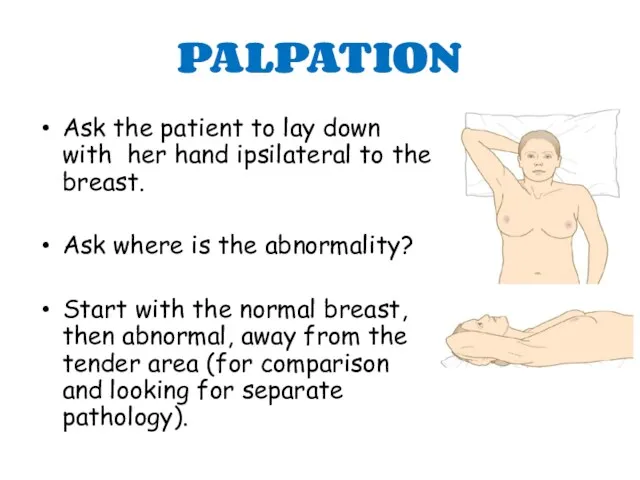
PALPATION
Ask the patient to lay down with her hand ipsilateral
PALPATION
Ask the patient to lay down with her hand ipsilateral
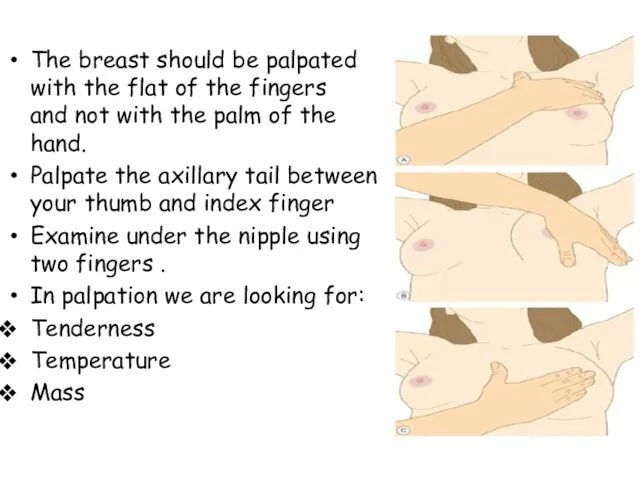
The breast should be palpated with the flat of the fingers
The breast should be palpated with the flat of the fingers

* If there is a lump we should analyze it :
Lump
Site
* If there is a lump we should analyze it :
Lump
Site
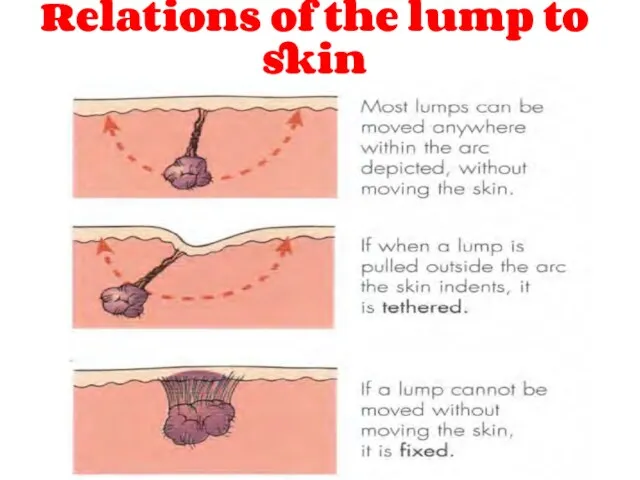
Relations of the lump to skin
Relations of the lump to skin
 Терминальное состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного
Терминальное состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного Абдомінальний ішемічний синдром. Тема 05
Абдомінальний ішемічний синдром. Тема 05 Нутритивная поддержка в хирургии. Обзор современных клинических рекомендаций
Нутритивная поддержка в хирургии. Обзор современных клинических рекомендаций История изучения сердечно-сосудистой системы
История изучения сердечно-сосудистой системы Учение о биосфере. Ноосфера. (Лекция 18)
Учение о биосфере. Ноосфера. (Лекция 18) Клинические рекомендации пациенту с заболеванием мочеполовой системы. Тактика ведения пациента на уровне ПМСП
Клинические рекомендации пациенту с заболеванием мочеполовой системы. Тактика ведения пациента на уровне ПМСП Кроветворение (гемопоэз) – образование клеток крови в красном костном мозге
Кроветворение (гемопоэз) – образование клеток крови в красном костном мозге Обмороження та його періоди. Класифікація обмороження. Домедична допомога при обмороженнях
Обмороження та його періоди. Класифікація обмороження. Домедична допомога при обмороженнях ХТА пестицидов ФОС
ХТА пестицидов ФОС Атомная медицина и медицинская физика
Атомная медицина и медицинская физика Внематочная беременность
Внематочная беременность История сестринского дела
История сестринского дела Гирсутизм. Вирилизация. Гипертрихоз
Гирсутизм. Вирилизация. Гипертрихоз Коронавирус 2019, профилактика, санитарно-просветительская работа
Коронавирус 2019, профилактика, санитарно-просветительская работа Қарыншалар гипертрофиясының ЭКГ белгілері
Қарыншалар гипертрофиясының ЭКГ белгілері Багатоплідна вагітність
Багатоплідна вагітність Фізіологічні основи оздоровчої фізичної культури
Фізіологічні основи оздоровчої фізичної культури Больные с заболеваниями крови и органов кроветворения
Больные с заболеваниями крови и органов кроветворения Возрастные особенности строения уха
Возрастные особенности строения уха Раны. Классификация ран. Лечение чистой раны
Раны. Классификация ран. Лечение чистой раны Обмен нуклеотидов. Матричные биосинтезы
Обмен нуклеотидов. Матричные биосинтезы Переломы скуловых костей и дуг
Переломы скуловых костей и дуг Бейспецификалық жаралы колит
Бейспецификалық жаралы колит Травма позвоночника
Травма позвоночника Фенотипические особенности наследственных синдромов рака молочной железы и яичников среди татарского этноса
Фенотипические особенности наследственных синдромов рака молочной железы и яичников среди татарского этноса Профессиональное здоровье педагогов по результатам социологического опроса
Профессиональное здоровье педагогов по результатам социологического опроса בן 45עם כאבי פרקים סימטרים עם נפיחויות ,קשיון בוקר מעל שעה חודשיים
בן 45עם כאבי פרקים סימטרים עם נפיחויות ,קשיון בוקר מעל שעה חודשיים Демография. Медицинская демография
Демография. Медицинская демография