- Cardiac rhythm disorders in children

Содержание
- 2. Plan of the lecture 1. Definition of cardiac rhythm disorders in children 2. Etiologic factors 3.
- 6. Arrhythmia reasons Cardial CHD Acquired chronic HD Carditis Cardiomyopathies Mitral valve prolapse Cardiac neoplasms Combined Extracardial
- 7. Rhythm and conductivity disorders classification ( Belokon N.A. 1987) 1 Impulse formation disturbance А. Nomotope disturbance
- 8. Diagnostic approach Superficial ECG (12 traditional leads) Electrophysiologic examining methods (EPM)-intracardiac or transesophageal electrodes HR and
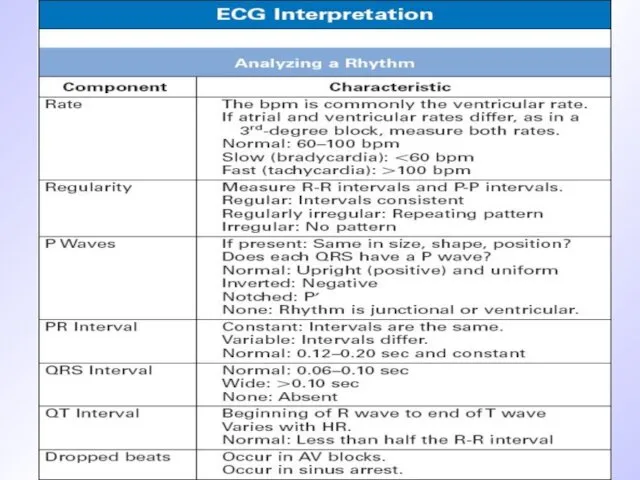
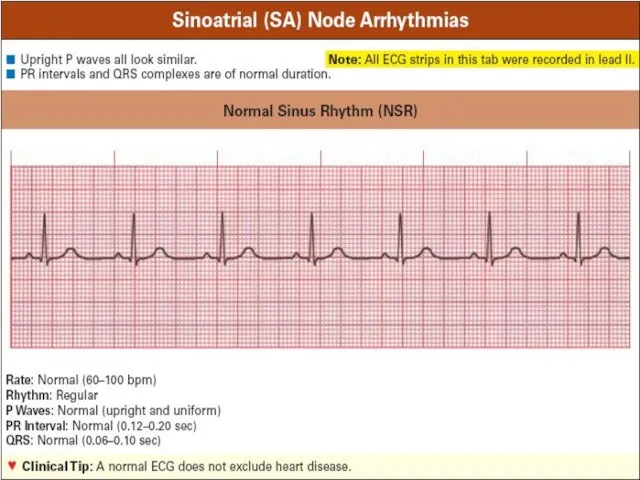
- 12. Normal sinus rhythm criteria Regular consecutive Р-Р row Constant wave P morphology Wave P precedes QRS
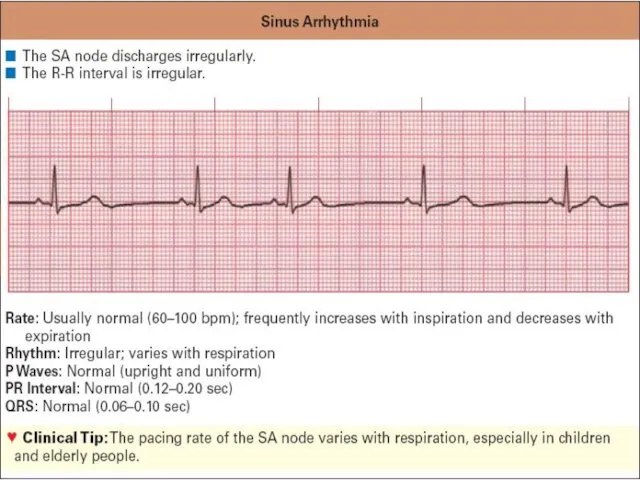
- 14. ECG criteria of sinus arrhythmia R-R interval irregular ( decreases during inspiration) P-P interval irregular Wave
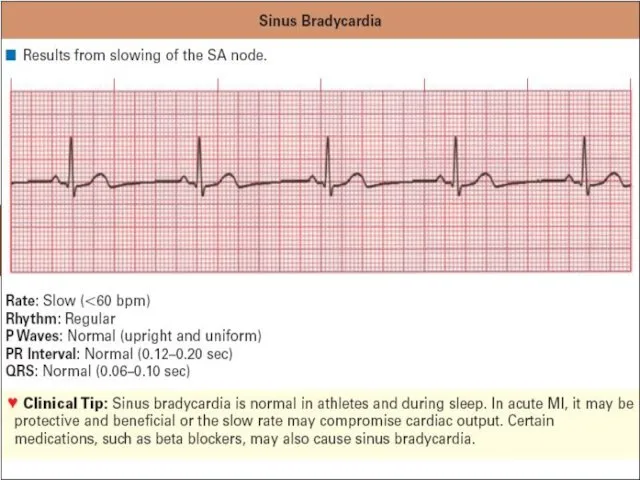
- 16. ECG criteria of sinus bradycardia QRS complexes frequency less than100/min in neonates and infants; less than
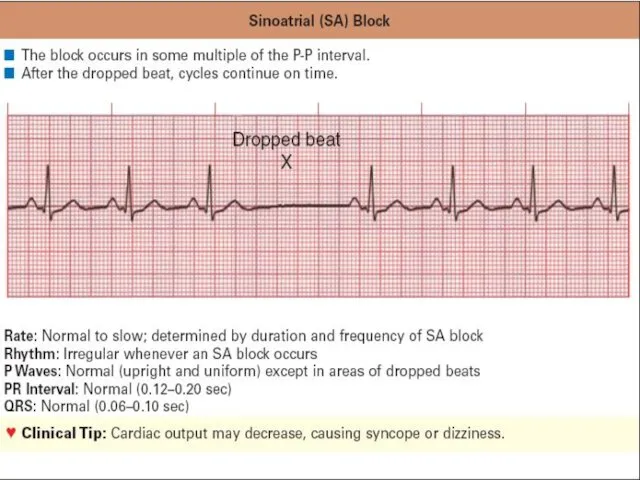
- 18. ECG criteria of sick sinus node syndrome Evident tachy-brady-arrhythmia Sinus-auricularis blockage Atrium or/and cardiac asystolia When
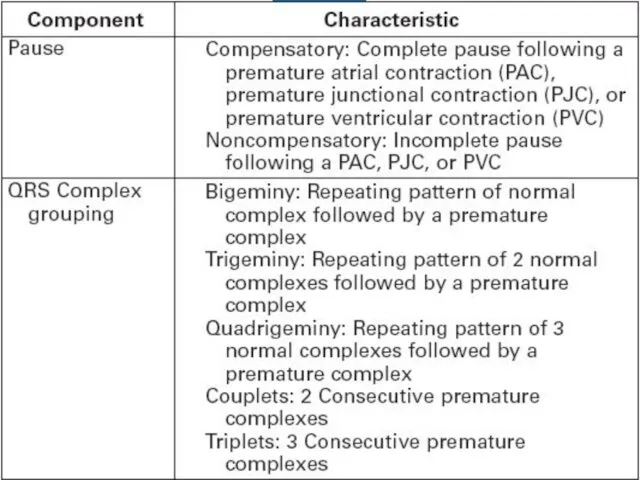
- 21. Premature Contractions (PC) can be Supraventricular or ventricular Monotopic or polytopic Aberrant Ultraearly, early, late Rare,
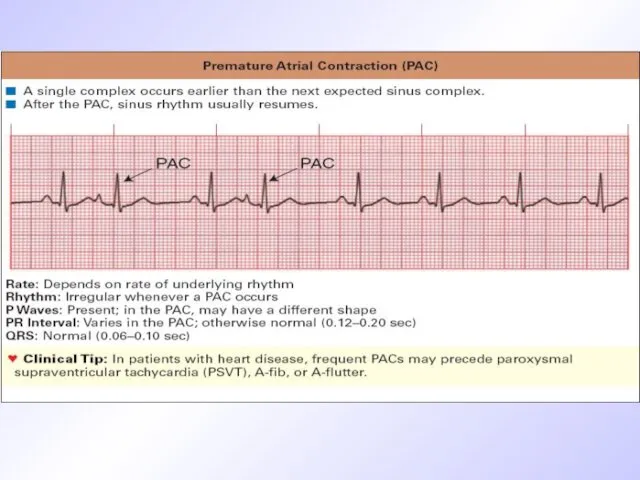
- 22. ECG signs of premature atrium contractions (PAC) Short-cut preectopic interval Wave P is present before complex
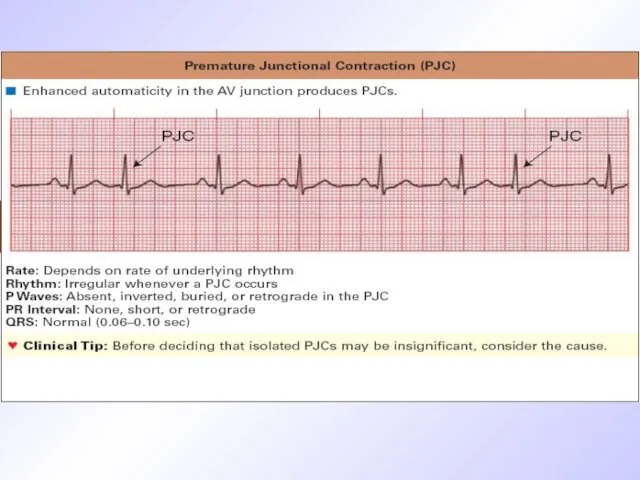
- 24. ECG criteria of PC originated from AV-node Premature unstrained complex QRS P wave is absent before
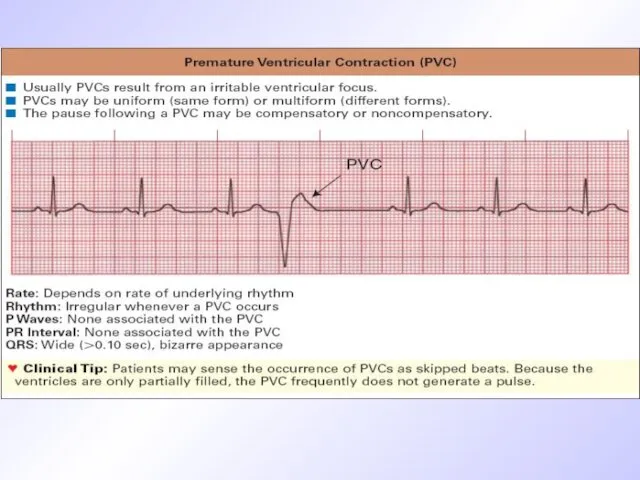
- 27. ECG criteria of premature ventricular contraction (PVC) Wave is absent before QRS QRS is premature aberrant,
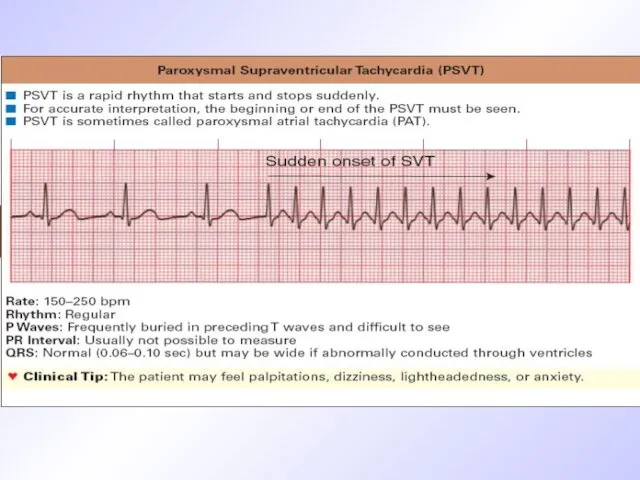
- 29. Signs of atrium paroxysmal tachycardia (PT) Wave Р is present before QRS QRS is unstrained HR
- 31. ECG signs of AV PT Wave P is absent before QRS QRS is unstrained HR is
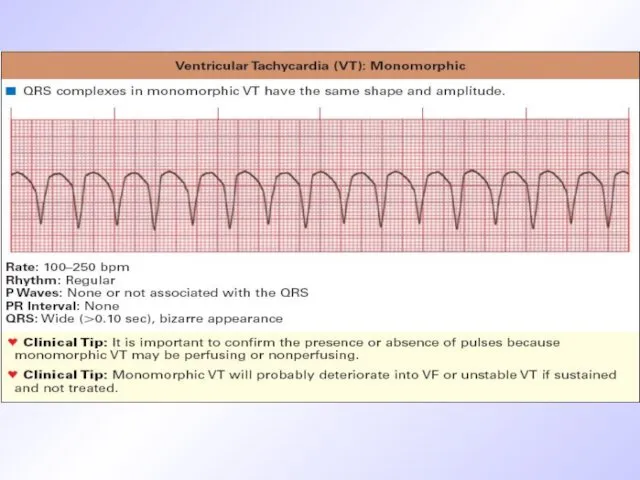
- 32. ECG signs of ventricular PT Aberrant wide regular QRS HR 150-200/min Constant R-R interval Secondary discordant
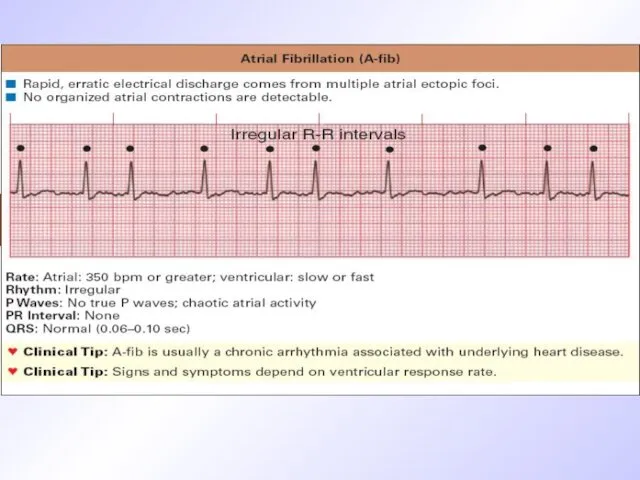
- 34. ECG signs of atrium fibrillation P-wave is displaced by F-waves of different shape and amplitude QRS
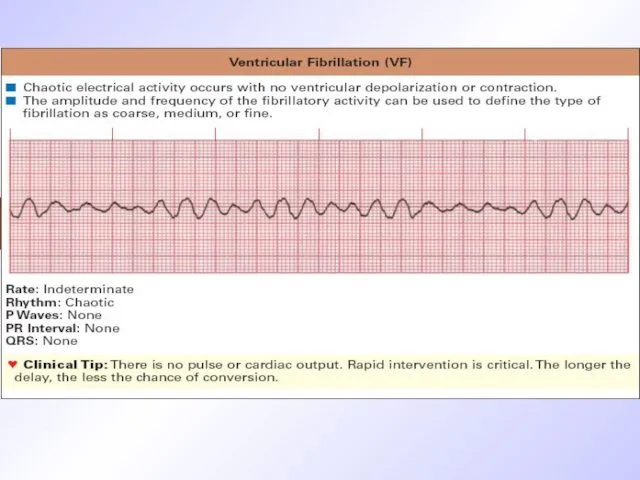
- 37. ECG signs of ventricular fibrillation QRS are wide of the same shape and amplitude End part
- 39. ECG signs of atrium blockage Wave P is wide ( elongation to 120msec (normal one isn’t
- 41. ECG signs of I grade AV blockage Interval PQ elongation more than 170 ms for younger
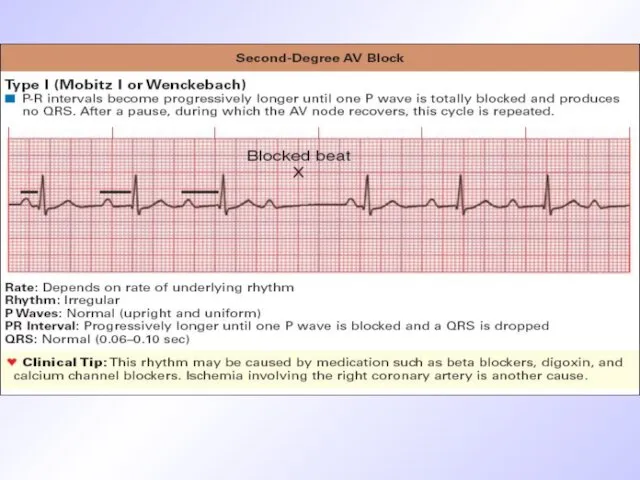
- 43. Ecg signs of Mobitz-I type AV block Consecutive AV-conductivity retardation from cycle to cycle and elongation
- 45. ECG signs of Mobitz-II AV blockage Periodic conductivity atrium impulse to ventricular blockage and QRS fallout.
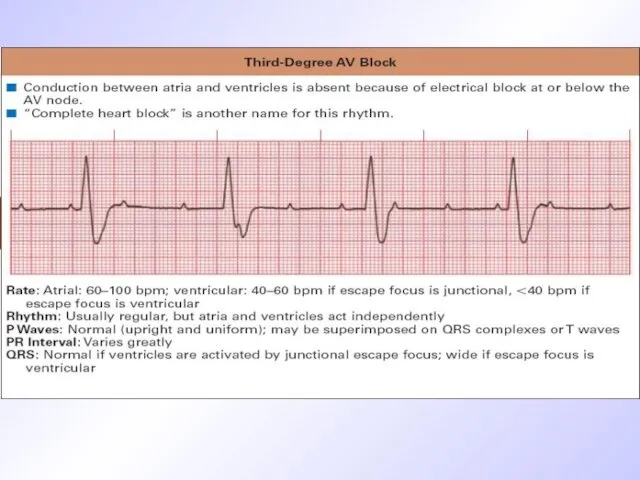
- 46. ECG signs of III grade AV -blockage Complete dissociation of atrium and ventricular contractility P waves
- 48. Arrhythmias treatment Treatment of arrhythmia in children differs from therapy in adults. Main approach is to
- 49. Arrhythmias treatment Antiarrhythmic drugs are classified according E. Vaughan-Williams (1984) for IV classes Class I membrane
- 50. Arrhythmias treatment Beta-blockers ( propranolol-0,5 mg/kg increasing dosage to 3-5 mg/kg/day steadily, atenolol 1-2 mg/kg bid,
- 51. Arrhythmias treatment Some medications that improve metabolism of cardiomyocytes has also indirect anti-arrhythmic activity mildronat, L-carnitin,
- 53. Скачать презентацию
Plan of the lecture
1. Definition of cardiac rhythm disorders in
Plan of the lecture
1. Definition of cardiac rhythm disorders in
Arrhythmia reasons
Cardial
CHD
Acquired chronic HD
Carditis
Cardiomyopathies
Mitral valve prolapse
Cardiac neoplasms
Combined
Extracardial
Vegetative nervous system dysregulation
Endocrine disorders
CNS
Arrhythmia reasons
Cardial
CHD
Acquired chronic HD
Carditis
Cardiomyopathies
Mitral valve prolapse
Cardiac neoplasms
Combined
Extracardial
Vegetative nervous system dysregulation
Endocrine disorders
CNS
Rhythm and conductivity disorders classification ( Belokon N.A. 1987)
1 Impulse formation
Rhythm and conductivity disorders classification ( Belokon N.A. 1987)
1 Impulse formation
Diagnostic approach
Superficial ECG (12 traditional leads)
Electrophysiologic examining methods (EPM)-intracardiac or transesophageal
Diagnostic approach
Superficial ECG (12 traditional leads)
Electrophysiologic examining methods (EPM)-intracardiac or transesophageal
Normal sinus rhythm criteria
Regular consecutive Р-Р row
Constant wave P morphology
Wave P
Normal sinus rhythm criteria
Regular consecutive Р-Р row
Constant wave P morphology
Wave P
ECG criteria of sinus arrhythmia
R-R interval irregular ( decreases during
ECG criteria of sinus arrhythmia
R-R interval irregular ( decreases during
ECG criteria of sinus bradycardia
QRS complexes frequency less than100/min in neonates
ECG criteria of sinus bradycardia
QRS complexes frequency less than100/min in neonates
ECG criteria of sick sinus node syndrome
Evident tachy-brady-arrhythmia
Sinus-auricularis blockage
Atrium or/and cardiac
ECG criteria of sick sinus node syndrome
Evident tachy-brady-arrhythmia
Sinus-auricularis blockage
Atrium or/and cardiac
Premature Contractions (PC) can be
Supraventricular or ventricular
Monotopic or polytopic
Aberrant
Ultraearly, early, late
Rare,
Premature Contractions (PC) can be
Supraventricular or ventricular
Monotopic or polytopic
Aberrant
Ultraearly, early, late
Rare,
ECG signs of premature atrium contractions (PAC)
Short-cut preectopic interval
Wave P is
ECG signs of premature atrium contractions (PAC)
Short-cut preectopic interval
Wave P is
ECG criteria of PC originated from AV-node
Premature unstrained complex QRS
P wave
ECG criteria of PC originated from AV-node
Premature unstrained complex QRS
P wave
ECG criteria of premature ventricular contraction (PVC)
Wave is absent before QRS
ECG criteria of premature ventricular contraction (PVC)
Wave is absent before QRS
Signs of atrium paroxysmal tachycardia (PT)
Wave Р is present before QRS
QRS
Signs of atrium paroxysmal tachycardia (PT)
Wave Р is present before QRS
QRS
ECG signs of AV PT
Wave P is absent before QRS
QRS is
ECG signs of AV PT
Wave P is absent before QRS
QRS is
ECG signs of ventricular PT
Aberrant wide regular QRS
HR 150-200/min
Constant R-R interval
Secondary
ECG signs of ventricular PT
Aberrant wide regular QRS
HR 150-200/min
Constant R-R interval
Secondary
ECG signs of atrium fibrillation
P-wave is displaced by F-waves of different
ECG signs of atrium fibrillation
P-wave is displaced by F-waves of different
ECG signs of ventricular fibrillation
QRS are wide of the same
ECG signs of ventricular fibrillation
QRS are wide of the same
ECG signs of atrium blockage
Wave P is wide ( elongation to
ECG signs of atrium blockage
Wave P is wide ( elongation to
ECG signs of I grade AV blockage
Interval PQ elongation more than
ECG signs of I grade AV blockage
Interval PQ elongation more than

Ecg signs of Mobitz-I type AV block
Consecutive AV-conductivity retardation from cycle
Ecg signs of Mobitz-I type AV block
Consecutive AV-conductivity retardation from cycle
ECG signs of Mobitz-II AV blockage
Periodic conductivity atrium impulse to ventricular
ECG signs of Mobitz-II AV blockage
Periodic conductivity atrium impulse to ventricular
ECG signs of III grade AV -blockage
Complete dissociation of atrium and
ECG signs of III grade AV -blockage
Complete dissociation of atrium and
Arrhythmias treatment
Treatment of arrhythmia in children differs from therapy in adults.
Arrhythmias treatment
Treatment of arrhythmia in children differs from therapy in adults.
Arrhythmias treatment
Antiarrhythmic drugs are classified according E. Vaughan-Williams (1984) for IV
Arrhythmias treatment
Antiarrhythmic drugs are classified according E. Vaughan-Williams (1984) for IV
Arrhythmias treatment
Beta-blockers ( propranolol-0,5 mg/kg increasing dosage to 3-5 mg/kg/day steadily,
Arrhythmias treatment
Beta-blockers ( propranolol-0,5 mg/kg increasing dosage to 3-5 mg/kg/day steadily,
Arrhythmias treatment
Some medications that improve metabolism of cardiomyocytes has also indirect
Arrhythmias treatment
Some medications that improve metabolism of cardiomyocytes has also indirect
 Плоскостопие у детей
Плоскостопие у детей Планирование выполнения операции Лабиринт IIIВ
Планирование выполнения операции Лабиринт IIIВ Терминальды жағдай
Терминальды жағдай Профилактика заболеваний. СПИД
Профилактика заболеваний. СПИД Диагностика геморрагических лихорадок, клещевого энцефалита, лайм-боррелиоза
Диагностика геморрагических лихорадок, клещевого энцефалита, лайм-боррелиоза Кома жағдайлардың ажырату диагностикасы
Кома жағдайлардың ажырату диагностикасы Лептоспироз
Лептоспироз Дислипопротеинеми и атеросклероз
Дислипопротеинеми и атеросклероз Принципы фармакотерапии у беременных
Принципы фармакотерапии у беременных Психологія, патопсихологія, психопатологія мислення
Психологія, патопсихологія, психопатологія мислення Қан кету (қансырау)
Қан кету (қансырау) Нужны ли беременной женщине омега-3 ПНЖК
Нужны ли беременной женщине омега-3 ПНЖК Әртүрлі жастағы әйелдер ағзасының клиникалық - физиологиялық ерекшеліктері
Әртүрлі жастағы әйелдер ағзасының клиникалық - физиологиялық ерекшеліктері Синдром Стивенса-Джонсона
Синдром Стивенса-Джонсона Мегалобластические анемии
Мегалобластические анемии Анатомия сердца
Анатомия сердца Координаторная система. Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения
Координаторная система. Мозжечок, синдромы поражения. Экстрапирамидная система, синдромы поражения Микробиология чумы
Микробиология чумы GU tumors. Renal cell carcinoma
GU tumors. Renal cell carcinoma Тактика ведения больных в постинсультном периоде
Тактика ведения больных в постинсультном периоде Трансформация патологии населения. Основные социально-гигиенические проблемы современного общества
Трансформация патологии населения. Основные социально-гигиенические проблемы современного общества Наследственные заболевания
Наследственные заболевания Нейросифилис. Пути передачи сифилиса
Нейросифилис. Пути передачи сифилиса Диагностика экстрагенитальной патологии у беременных
Диагностика экстрагенитальной патологии у беременных Виды взаимодействия лекарственных средств
Виды взаимодействия лекарственных средств Хирургическое отделение (охрана труда)
Хирургическое отделение (охрана труда) Сестринский процесс как основа оказания сестринской помощи
Сестринский процесс как основа оказания сестринской помощи Первая помощь при травмах скелета и мышц
Первая помощь при травмах скелета и мышц