- Cardiotonic drugs. Antiarrhythmic agents

Содержание
- 2. CARDIOTONIC DRUGS (Cardiostimulants, or Inotropic Drugs) 1. Cardiac Glycosides 2. Agents of Non-Glycoside Structure
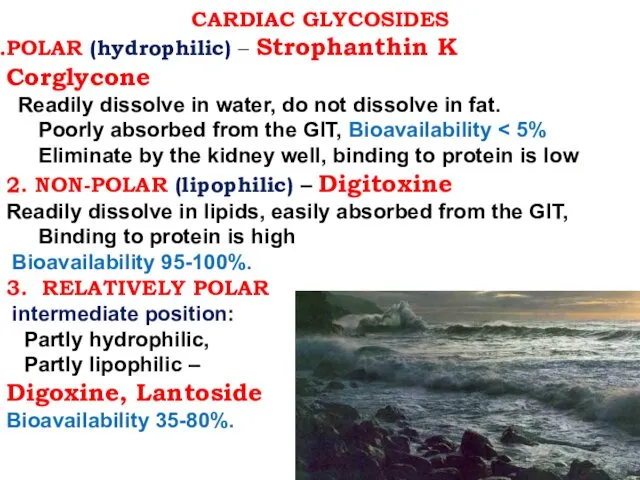
- 3. CARDIAC GLYCOSIDES POLAR (hydrophilic) – Strophanthin K Corglycone Readily dissolve in water, do not dissolve in
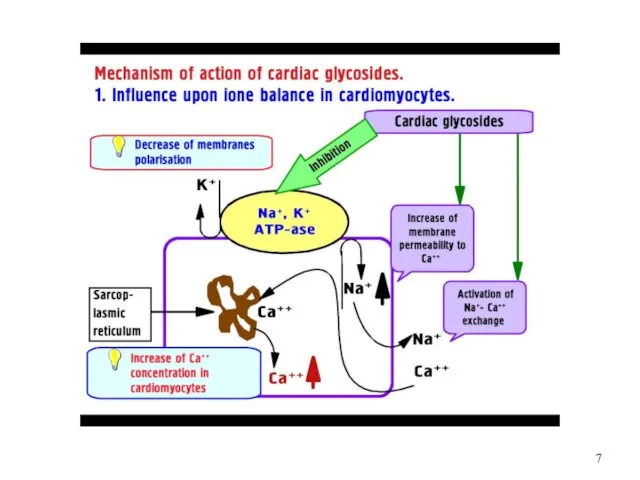
- 8. MECHANISM of ACTION of CARDIAC GLYCOSIDES 1. Na+/K+ ATPase inhibition => 2. ? Intracellular Na+ concentration
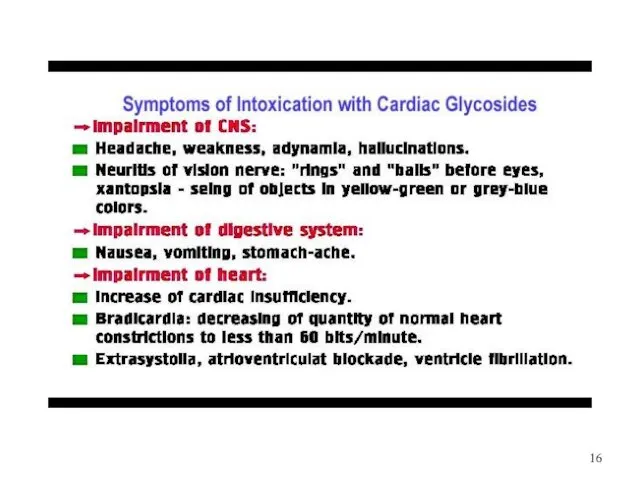
- 12. BASIC EFFECTS OF CGs ON HEART: 1.«+» Inotropic effect: ?Force of Contraction 2.«-» Chronotropic effect: ?HR
- 13. The ECG effects of CSs: 1. P-R interval is prolonged (Delayed Conduction) 2. Q-T interval is
- 14. CLINICAL USES of CGs: Acute and Chronic Heart Failure Pulmonary Edema Atrial Fibrillation and Flutter Paroxysmal
- 15. .
- 17. TREATMENT of OVERDOSE with Cardiac Glycosides Discontinuation of the drug , Emesis Induction, Gastric Lavage Activated
- 18. POSITIVE INOTROPIC DRUGS of NON-GLYCOSIDE STRUCTURE 1. Inhibitors of Phosphodiesterase III: Amrinone Milrinone Vesnarinone 2. β1
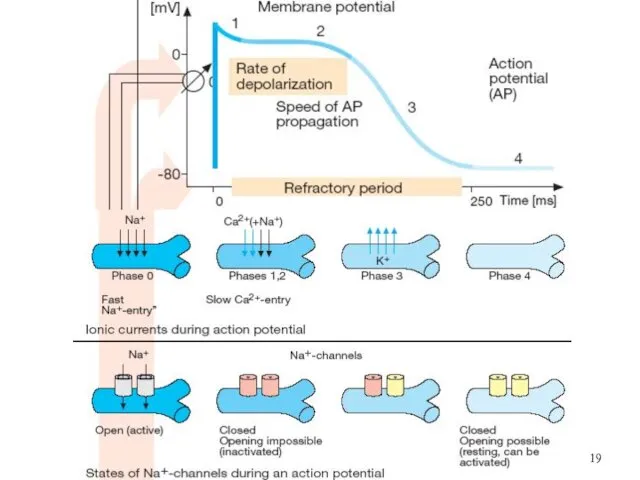
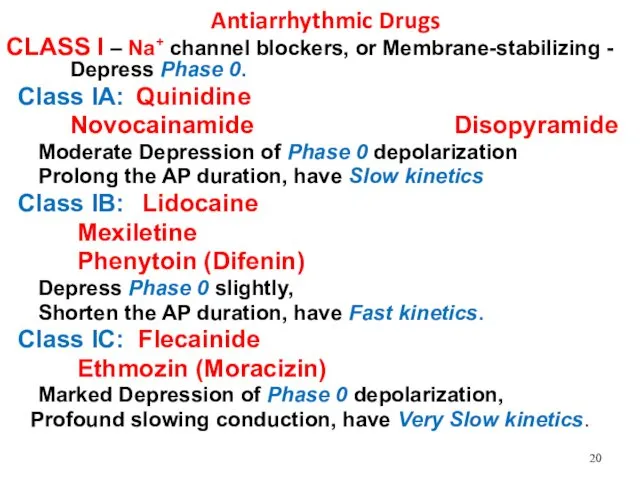
- 20. Antiarrhythmic Drugs CLASS I – Na+ channel blockers, or Membrane-stabilizing - Depress Phase 0. Class IA:
- 21. CLASS II – β-Blockers - ▶ Suppress Phase 4 Depolarization: Propronalol (Anaprilin) Oxprenolol (Trasicor) Nadolol (Corgard)
- 22. Novocainamide (Procainamide) – amp. 10% - 5 ml; Tab 0.25 g interacts moderately with Na+ channels,
- 23. Lidocaine amp. 2%-10 ml, 10%-2 ml rapidly associates and dissociates from Na+ channels. ?Duration of Phase
- 24. CAST I and CAST II (1993-1994) – Cardiac Arrhythmia Suppression Trial I and II Encainide Flecainide
- 25. Amiodarone (Kordarone) – Tab. 0.2 g, amp. 5% – 3ml contains 37% of iodine (1tab.– 75
- 26. Verapamil - Tab 0.04, 0.08 g; amp. 0.25% - 2 ml, is a Ca2+ channel Blocker
- 27. Miscellaneous Antiarrhythmic Agents ◼ Cardiac Glycosides: Strophanthin, Digoxin Adenosine - ATP - is the drug of
- 28. AGENTS used to treat BRADYARRHYTHMIAS 1. M-Cholinoblockers: Atropine sulfate – symptomatic bradycardia, bradyarrhythmia, supranodal and AV
- 30. Скачать презентацию
CARDIOTONIC DRUGS
(Cardiostimulants, or Inotropic Drugs)
1. Cardiac Glycosides
2. Agents of Non-Glycoside Structure
CARDIOTONIC DRUGS
(Cardiostimulants, or Inotropic Drugs)
1. Cardiac Glycosides
2. Agents of Non-Glycoside Structure
CARDIAC GLYCOSIDES
POLAR (hydrophilic) – Strophanthin K Corglycone
Readily dissolve in
CARDIAC GLYCOSIDES
POLAR (hydrophilic) – Strophanthin K Corglycone
Readily dissolve in


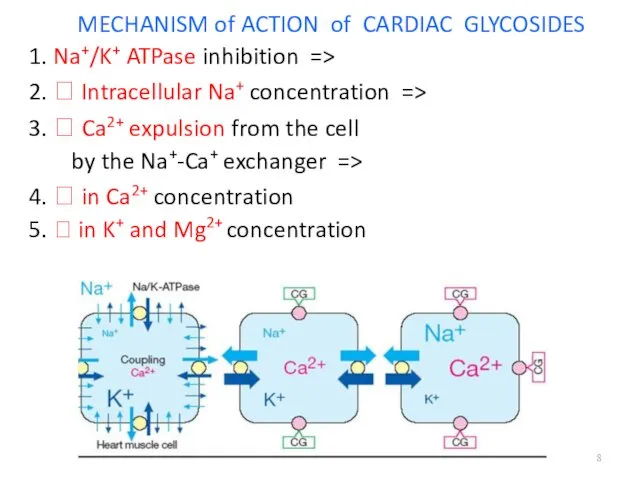
MECHANISM of ACTION of CARDIAC GLYCOSIDES
1. Na+/K+ ATPase inhibition =>
2. ?
MECHANISM of ACTION of CARDIAC GLYCOSIDES
1. Na+/K+ ATPase inhibition =>
2. ?
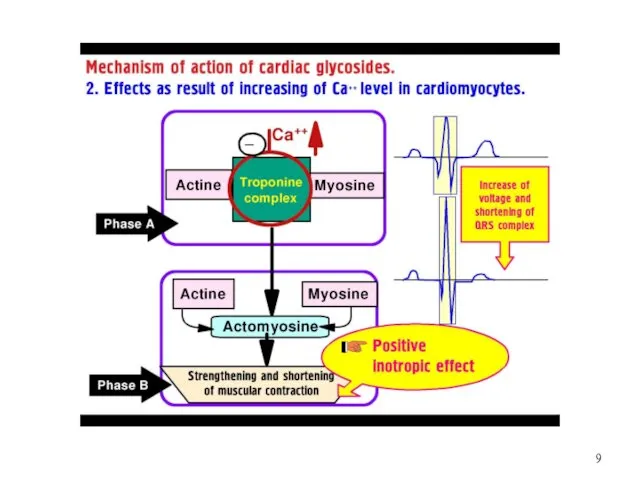
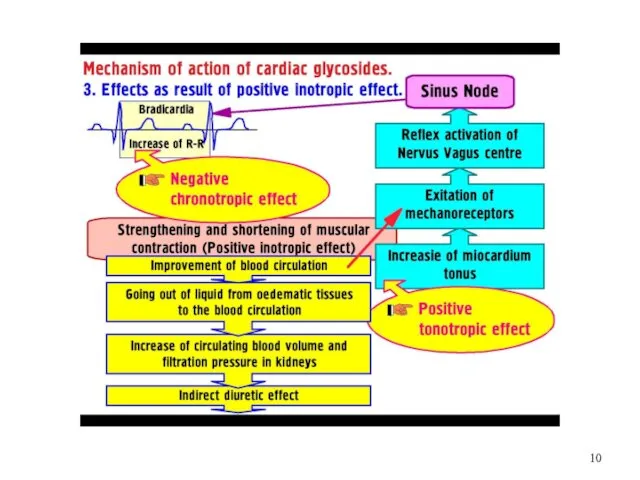
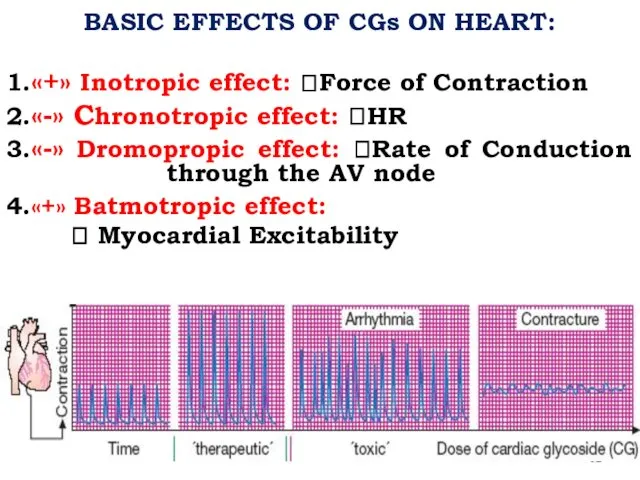
BASIC EFFECTS OF CGs ON HEART:
1.«+» Inotropic effect: ?Force of Contraction
2.«-»
BASIC EFFECTS OF CGs ON HEART:
1.«+» Inotropic effect: ?Force of Contraction
2.«-»
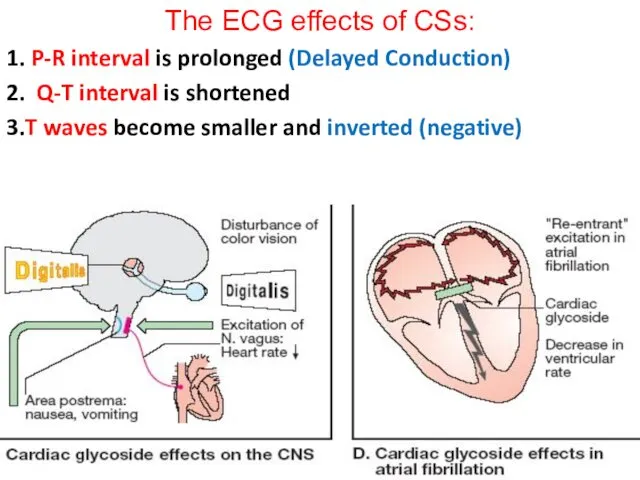
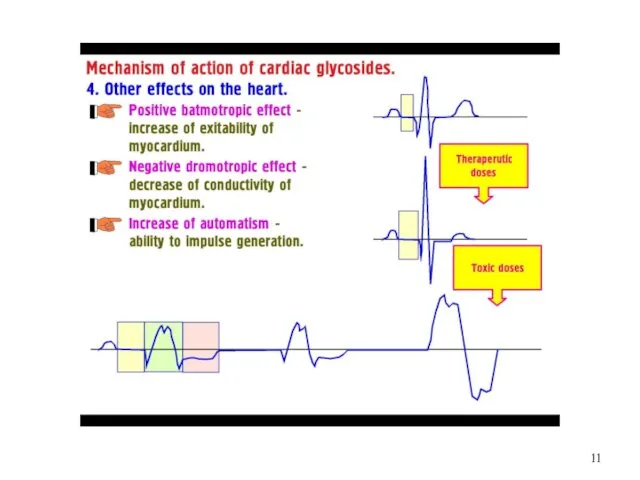
The ECG effects of CSs:
1. P-R interval is prolonged (Delayed Conduction)
2.
The ECG effects of CSs:
1. P-R interval is prolonged (Delayed Conduction)
2.
CLINICAL USES of CGs:
Acute and Chronic Heart Failure
Pulmonary Edema
Atrial Fibrillation and
CLINICAL USES of CGs:
Acute and Chronic Heart Failure
Pulmonary Edema
Atrial Fibrillation and
.
.
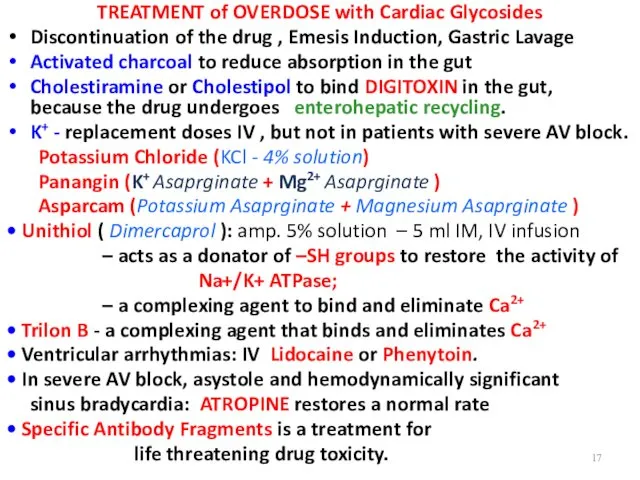
TREATMENT of OVERDOSE with Cardiac Glycosides
Discontinuation of the drug , Emesis
TREATMENT of OVERDOSE with Cardiac Glycosides
Discontinuation of the drug , Emesis
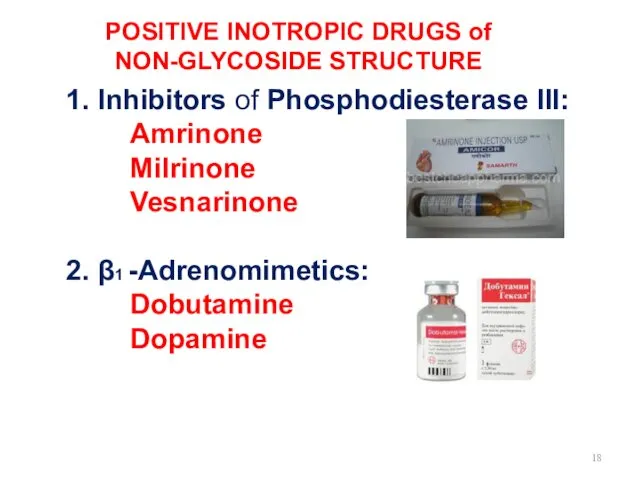
POSITIVE INOTROPIC DRUGS of NON-GLYCOSIDE STRUCTURE
1. Inhibitors of Phosphodiesterase III:
Amrinone
Milrinone
Vesnarinone
2.
POSITIVE INOTROPIC DRUGS of NON-GLYCOSIDE STRUCTURE
1. Inhibitors of Phosphodiesterase III:
Amrinone
Milrinone
Vesnarinone
2.
Antiarrhythmic Drugs
CLASS I – Na+ channel blockers, or Membrane-stabilizing - Depress
Antiarrhythmic Drugs
CLASS I – Na+ channel blockers, or Membrane-stabilizing - Depress
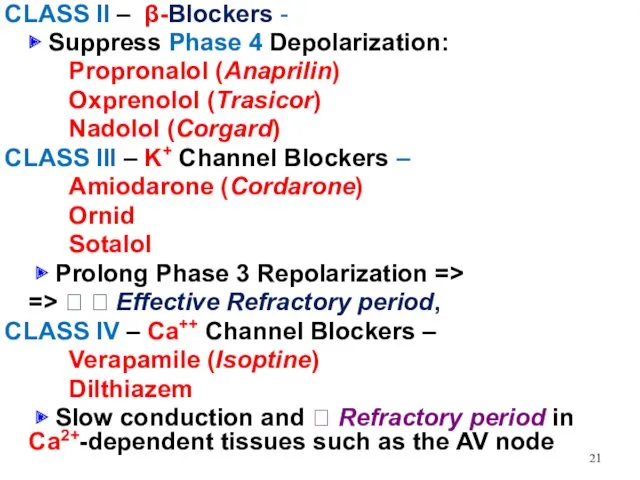
CLASS II – β-Blockers -
▶ Suppress Phase 4 Depolarization:
Propronalol
CLASS II – β-Blockers -
▶ Suppress Phase 4 Depolarization:
Propronalol
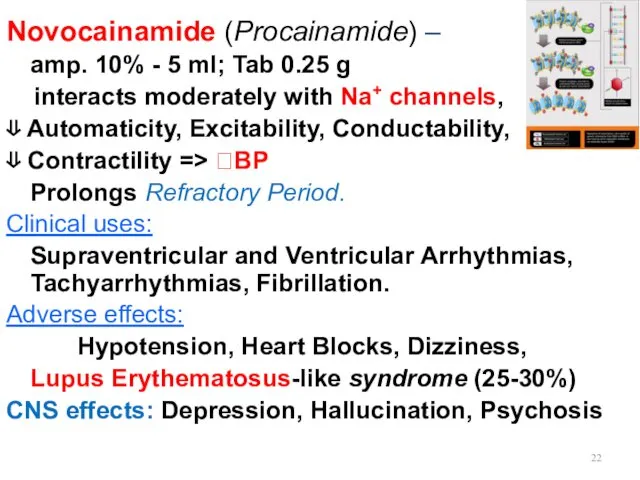
Novocainamide (Procainamide) –
amp. 10% - 5 ml; Tab 0.25 g
Novocainamide (Procainamide) –
amp. 10% - 5 ml; Tab 0.25 g
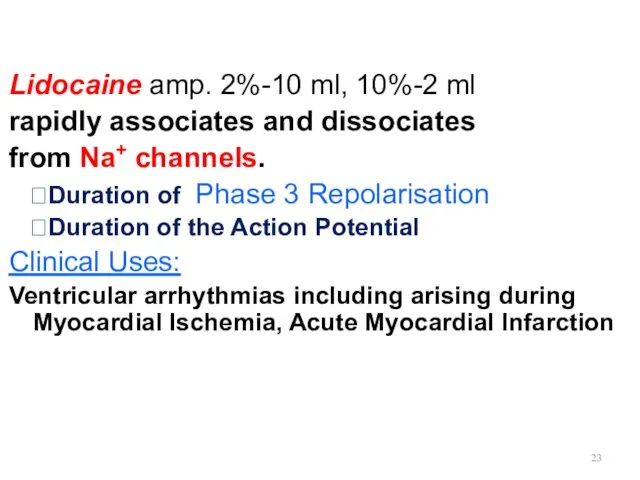
Lidocaine amp. 2%-10 ml, 10%-2 ml
rapidly associates and dissociates
from Na+
Lidocaine amp. 2%-10 ml, 10%-2 ml
rapidly associates and dissociates
from Na+
CAST I and CAST II (1993-1994) –
Cardiac Arrhythmia Suppression
CAST I and CAST II (1993-1994) –
Cardiac Arrhythmia Suppression
Amiodarone (Kordarone) – Tab. 0.2 g, amp. 5% – 3ml
contains
Amiodarone (Kordarone) – Tab. 0.2 g, amp. 5% – 3ml
contains
Verapamil - Tab 0.04, 0.08 g; amp. 0.25% - 2 ml,
Verapamil - Tab 0.04, 0.08 g; amp. 0.25% - 2 ml,
Miscellaneous Antiarrhythmic Agents
◼ Cardiac Glycosides: Strophanthin, Digoxin
Adenosine - ATP -
is
Miscellaneous Antiarrhythmic Agents
◼ Cardiac Glycosides: Strophanthin, Digoxin
Adenosine - ATP -
is
AGENTS used to treat BRADYARRHYTHMIAS
1. M-Cholinoblockers: Atropine sulfate –
symptomatic
AGENTS used to treat BRADYARRHYTHMIAS
1. M-Cholinoblockers: Atropine sulfate –
symptomatic
 Эндовидеолапароскопические вмешательства при опухолях женской мочеполовой системы
Эндовидеолапароскопические вмешательства при опухолях женской мочеполовой системы Профилактика зубочелюстных аномалий у детей
Профилактика зубочелюстных аномалий у детей Жүрек-қантамыр аурулары кезіндегі медициналық-әлеуметтік реабилитация
Жүрек-қантамыр аурулары кезіндегі медициналық-әлеуметтік реабилитация Аутизм
Аутизм Инвазивные методы диагностики ишемической болезни сердца
Инвазивные методы диагностики ишемической болезни сердца Безопасность применения ЛС у беременных
Безопасность применения ЛС у беременных Основные функции печени
Основные функции печени Алгоритм диагностики и оказания скорой помощи при отравлениях и укусах
Алгоритм диагностики и оказания скорой помощи при отравлениях и укусах Cardiology
Cardiology Фізіологія, гігієна праці та виробнича санітарія. Виробничий травматизм
Фізіологія, гігієна праці та виробнича санітарія. Виробничий травматизм Дені сау балаларды диспансерлік бақылау
Дені сау балаларды диспансерлік бақылау Захворювання щитовидної залози у дітей
Захворювання щитовидної залози у дітей Жан тазалығы, тән тазалығы
Жан тазалығы, тән тазалығы Жеңіл, ауыр және өте ауыр пневмонияны емдеудің негізгі
Жеңіл, ауыр және өте ауыр пневмонияны емдеудің негізгі Школа здоровья для больных с артериальной гипертензией
Школа здоровья для больных с артериальной гипертензией Проявления соматических заболеваний в полости рта
Проявления соматических заболеваний в полости рта влияние комплексных физических упражнений на коррекцию нарушений осанки у детей школьного возраста
влияние комплексных физических упражнений на коррекцию нарушений осанки у детей школьного возраста Сучасні проблеми молекулярної біології. Генна терапія. (Лекція 8)
Сучасні проблеми молекулярної біології. Генна терапія. (Лекція 8) Врожденная дисфункция коры надпочечников
Врожденная дисфункция коры надпочечников Пропаганда здорового образа жизни, как средство профилактики наркомании среди подрастающего поколения
Пропаганда здорового образа жизни, как средство профилактики наркомании среди подрастающего поколения Опухоли почек, мочеточников, мочевого пузыря
Опухоли почек, мочеточников, мочевого пузыря Пищеварение в ротовой области
Пищеварение в ротовой области Мүмкіндіктері шектеулі науқастармен қарым-қатынас
Мүмкіндіктері шектеулі науқастармен қарым-қатынас Неизлечимые болезни разных времен
Неизлечимые болезни разных времен Тоны сердца
Тоны сердца Усік. Куйік. Электрожарақат
Усік. Куйік. Электрожарақат Кюреты. Методика работы универсальной кюретой
Кюреты. Методика работы универсальной кюретой Біофармація – теоретична основа виробництва лікарських засобів
Біофармація – теоретична основа виробництва лікарських засобів