- Charcot-Marie Tooth disease (CMT)

Содержание
- 2. Charcot-Marie Tooth disease (CMT) Synonyms Charcot–Marie–Tooth neuropathy Peroneal muscular atrophy Hereditary motor sensory neuropathy (HMSN) type
- 3. Introduction CMT is one of the hereditary motor & sensory neuropathies, a group of inherited
- 4. Epidemiology CMT is the most commonly inherited neurological disorder(autosomal dominant or recessive or an X-linked
- 5. Clinical Features Affects both motor and sensory nerves Symptom onset depends on type of
- 6. Clinical Features Foot drop (usually the initial symptom) High stepped gait Frequent falls
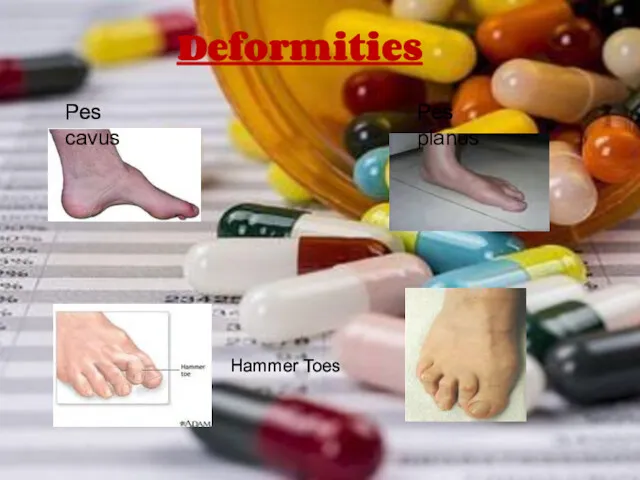
- 7. Deformities Pes cavus Pes planus Hammer Toes
- 8. Clinical Features Inverted champagne bottle legs(Stork Legs): -Hypertrophy of the proximal muscles -Marked peroneal muscle atrophy
- 9. Clinical Features Sensory changes Usually no sensory symptoms in early stages Touch, vibratory and
- 10. Clinical Features Other features: Weakness in neck and shoulder muscles Tremor Involuntary grinding
- 11. Exacerbating Factors Emotional stress Periods of prolonged immobility Pregnancy Drugs: Amiodarone,Bortezomib,Cisplatin, carboplatin,
- 12. Pathophysiology/Etiology Pathophysiology is either a demyelinating process or an axonal process Etiology is intragenic
- 13. Mutation results in defects of myelin structure, maintenance,and formation Demyelinating Schwann cells causes abnormal
- 14. Defective Myelin Defective Axon
- 15. Mode of inheritance Autosomal Dominant( most common) Autosomal Recessive X-linked
- 16. Classification Genetically heterogeneous with more than 50 genes identified to date Classified as types
- 17. TYPES OF CMT CMT1 (Hypertrophic demyelinating) CMT2 (Axonal) CMT3 (Dejerine-sotta’s disease) CMT4
- 18. Diagnosis Clinical History( *including family history): -Weakness in muscles of legs/arms, foot drop, deformities( pes cavus,
- 19. Diagnosis Nerve Biopsy: Not necessary for diagnosis -Fiber type grouping, a similarly non-specific finding which
- 20. “Onion bulbs” Diagnosis
- 21. Diagnosis Genetic testing: DNA testing can give a definitive diagnosis,but not all the genetic markers
- 22. Treatment Treatment of CMT hereditary neuropathy is symptomatic and Supportive. A Cure is not available so
- 24. Скачать презентацию

Charcot-Marie Tooth disease (CMT)
Synonyms
Charcot–Marie–Tooth neuropathy
Peroneal muscular atrophy
Hereditary motor sensory neuropathy (HMSN)
Charcot–Marie–Tooth neuropathy Peroneal muscular atrophy Hereditary motor sensory neuropathy (HMSN)
Introduction
CMT is one of the hereditary motor & sensory
Introduction
CMT is one of the hereditary motor & sensory
Epidemiology
CMT is the most commonly inherited neurological disorder(autosomal dominant or
Epidemiology CMT is the most commonly inherited neurological disorder(autosomal dominant or
Clinical Features
Affects both motor and sensory nerves
Symptom onset depends
Clinical Features
Affects both motor and sensory nerves
Symptom onset depends
Clinical Features
Foot drop (usually the initial symptom)
High stepped gait
Clinical Features Foot drop (usually the initial symptom) High stepped gait
Deformities
Pes cavus
Pes planus
Hammer Toes
Deformities
Pes cavus
Pes planus
Hammer Toes

Clinical Features
Inverted champagne bottle legs(Stork Legs):
-Hypertrophy of the proximal muscles
-Marked peroneal
Clinical Features Inverted champagne bottle legs(Stork Legs): -Hypertrophy of the proximal muscles -Marked peroneal
Clinical Features
Sensory changes
Usually no sensory symptoms in early
Clinical Features Sensory changes Usually no sensory symptoms in early

Clinical Features
Other features:
Weakness in neck and shoulder muscles
Tremor
Involuntary
Clinical Features Other features: Weakness in neck and shoulder muscles Tremor Involuntary
Exacerbating Factors
Emotional stress
Periods of prolonged immobility
Pregnancy
Drugs:
Amiodarone,Bortezomib,Cisplatin,
Exacerbating Factors
Emotional stress
Periods of prolonged immobility
Pregnancy
Drugs:
Amiodarone,Bortezomib,Cisplatin,
Pathophysiology/Etiology
Pathophysiology is either a demyelinating process or an axonal process
Pathophysiology/Etiology
Pathophysiology is either a demyelinating process or an axonal process
Mutation results in defects of myelin structure, maintenance,and formation
Demyelinating
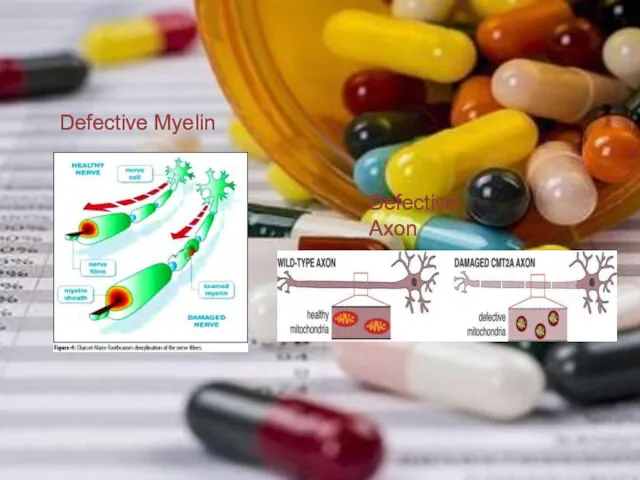
Defective Myelin
Defective Axon
Defective Myelin
Defective Axon

Mode of inheritance
Autosomal Dominant( most common)
Autosomal Recessive
X-linked
Mode of inheritance
Autosomal Dominant( most common)
Autosomal Recessive
X-linked
Classification
Genetically heterogeneous with more than 50 genes identified to date
Classification
Genetically heterogeneous with more than 50 genes identified to date
TYPES OF CMT
CMT1 (Hypertrophic demyelinating)
CMT2 (Axonal)
CMT3 (Dejerine-sotta’s
TYPES OF CMT
CMT1 (Hypertrophic demyelinating)
CMT2 (Axonal)
CMT3 (Dejerine-sotta’s

Diagnosis
Clinical History( *including family history):
-Weakness in muscles of legs/arms, foot
Diagnosis
Clinical History( *including family history):
-Weakness in muscles of legs/arms, foot
Diagnosis
Nerve Biopsy: Not necessary for diagnosis
-Fiber type grouping, a
Diagnosis
Nerve Biopsy: Not necessary for diagnosis
-Fiber type grouping, a
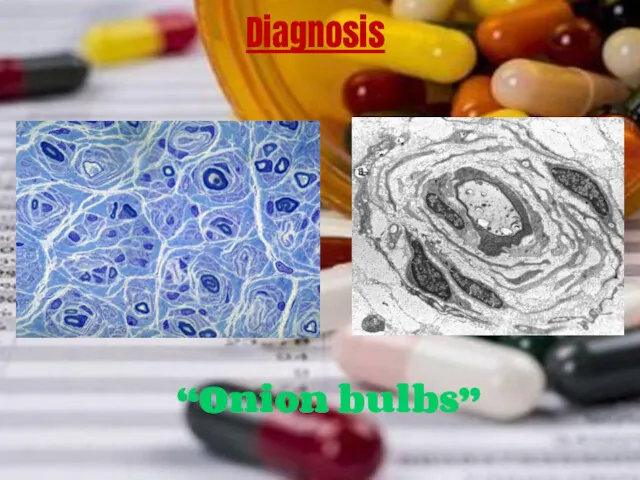
“Onion bulbs”
Diagnosis
“Onion bulbs”
Diagnosis

Diagnosis
Genetic testing: DNA testing can give a definitive diagnosis,but
Diagnosis Genetic testing: DNA testing can give a definitive diagnosis,but
Treatment
Treatment of CMT hereditary neuropathy is symptomatic and
Treatment
Treatment of CMT hereditary neuropathy is symptomatic and
 Сыртқы сәулеленуден медициналық қорғау
Сыртқы сәулеленуден медициналық қорғау Характеристика лекарственного растительного сырья, влияющего на сердечнососудистую и мочевыделительную систему
Характеристика лекарственного растительного сырья, влияющего на сердечнососудистую и мочевыделительную систему Основы безопасности питания
Основы безопасности питания Компьютерная томография
Компьютерная томография Синдромы и методы функциональной диагностики при патологии ЖВП и печени
Синдромы и методы функциональной диагностики при патологии ЖВП и печени Кокжөтел мен дифтерия кезіндегі шаралар стандарттары мен алгоритмдері
Кокжөтел мен дифтерия кезіндегі шаралар стандарттары мен алгоритмдері Здоровый образ жизни (ЗОЖ)
Здоровый образ жизни (ЗОЖ) Тұқым қуалайтын аурулардың емдеудің негізгі принциптері
Тұқым қуалайтын аурулардың емдеудің негізгі принциптері Состав крови. Плазма крови. Функции эритроцитов. Защитные механизмы крови
Состав крови. Плазма крови. Функции эритроцитов. Защитные механизмы крови Жгутиконосцы - flagellata
Жгутиконосцы - flagellata Сердечно-сосудистая система ребенка
Сердечно-сосудистая система ребенка Острый рассеянный энцефаломиелит
Острый рассеянный энцефаломиелит Применение статистики для оценки здоровья. Лекция 1
Применение статистики для оценки здоровья. Лекция 1 Острый коронарный синдром (ОКС)
Острый коронарный синдром (ОКС) Послеродовые заболевания
Послеродовые заболевания Естің бұзылыстары. Нарушения памяти
Естің бұзылыстары. Нарушения памяти Properties of heart and vessels in children
Properties of heart and vessels in children ACOS: перекрестный синдром ХОБЛ и бронхиальной астмы
ACOS: перекрестный синдром ХОБЛ и бронхиальной астмы Зрительные функции и методы их исследования
Зрительные функции и методы их исследования Параллелометрия. Определение
Параллелометрия. Определение Кишечник. Строение кишечника
Кишечник. Строение кишечника Феохромоцитома
Феохромоцитома Клиникалық жағдай. Интоксикационная энцефалопатия головного мозга. Нейропатия лицевого нерва справа
Клиникалық жағдай. Интоксикационная энцефалопатия головного мозга. Нейропатия лицевого нерва справа Загальні організаційно-методичні основи фізичної терапії при порушенні діяльності дихальної системи
Загальні організаційно-методичні основи фізичної терапії при порушенні діяльності дихальної системи Носовые кровотечения
Носовые кровотечения Служение больницы и учреждения. Анонимные Наркоманы
Служение больницы и учреждения. Анонимные Наркоманы Методы исследования центральной нервной системы
Методы исследования центральной нервной системы Сестринская помощь при заболеваниях прямой кишки трещины заднего прохода, геморрой. Лекция 16
Сестринская помощь при заболеваниях прямой кишки трещины заднего прохода, геморрой. Лекция 16