- Clinical anatomy, physiology and methods of examination of the larynx

Содержание
- 2. Larynx being a part of the air conducting tracts of the organism, participates in fulfilling the
- 3. ANATOMY OF LARYNX The larynx lies in front of the hypopharynx opposite the third to sixth
- 4. There are 3 unpaired and 3 paired cartilages. Thyroid. It is the largest of all the
- 5. Extrinsic laryngeal membranes: Thyrohyoid membrane. Connects thyroid cartilage to hyoid bone. Cricothyroid membrane. Connects thyroid cartilage
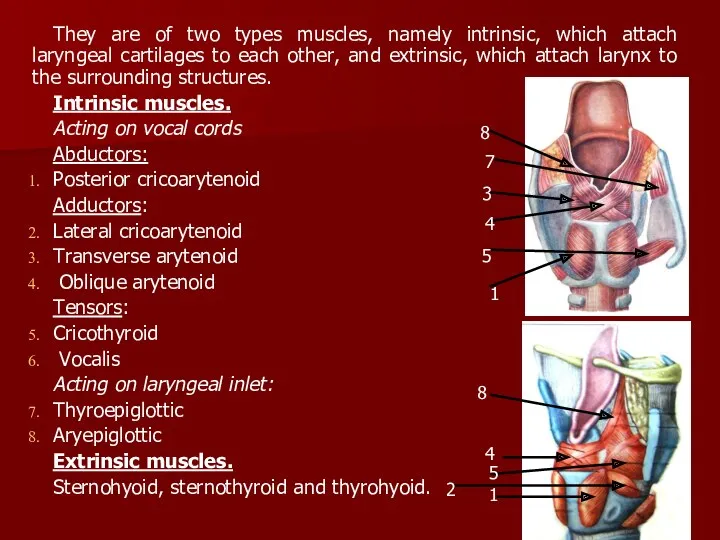
- 6. They are of two types muscles, namely intrinsic, which attach laryngeal cartilages to each other, and
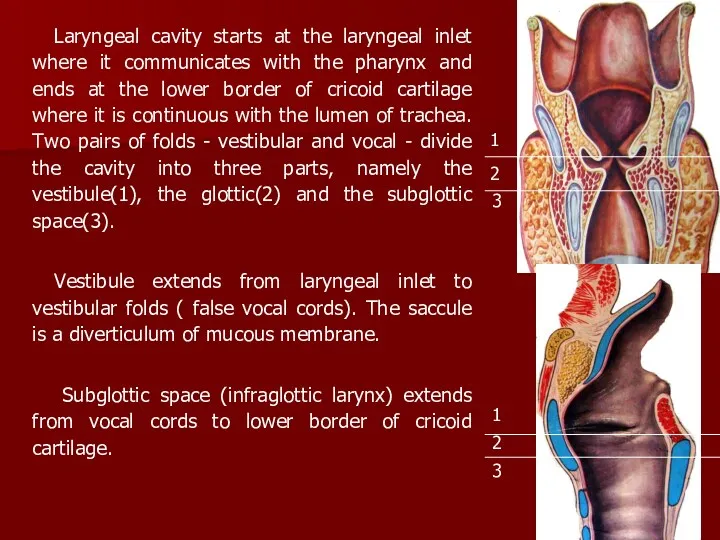
- 7. Laryngeal cavity starts at the laryngeal inlet where it communicates with the pharynx and ends at
- 8. Vocal folds (true vocal cords). They are two pearly-white sharp bands extending from thyroid angle to
- 9. The larynx performs the following important functions: 1. Protection of lower airways 2. Phonation 3. Respiration
- 10. Nerve supply of larynx Motor. All the muscles which move the vocal cord (abductors, adductors or
- 11. METHODS OF EXAMINATION Laryngoscopy is visual inspection of the larynx interior. Direct and indirect laryngoscopy are
- 12. Indirect laryngoscopy is carried out using a laryngeal speculum. The patient is asked to utter a
- 13. Acute catarrhal laryngitis. Acute inflammation of the laryngeal mucosa is usually extension of catarrhal inflammation of
- 14. Treatment. The larynx should first of all be spared. The patient is not allowed to talk
- 15. The child wakes up and tosses in his bed. Breathing becomes very difficult and whistling; inspiratory
- 16. Treatment includes common hygienic measures, ventilation in the room, and therapeutic measures. лаферон, ереспал,биопарокс преднизолон,димедрол,лазикс. Phlegmonous
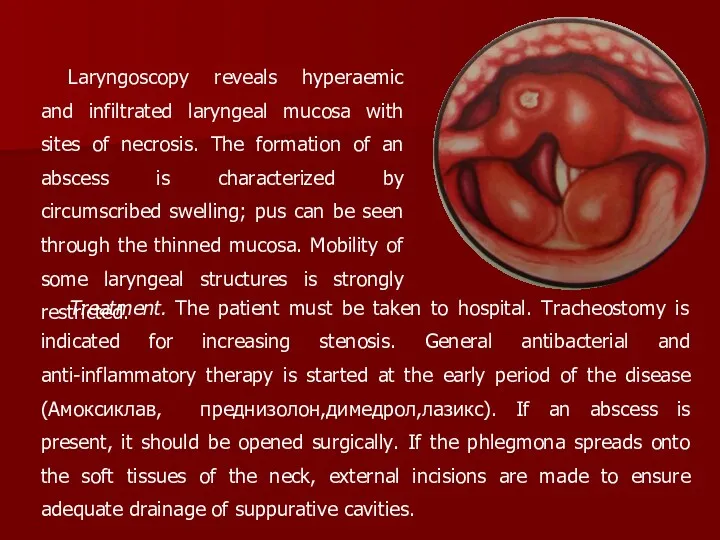
- 17. Laryngoscopy reveals hyperaemic and infiltrated laryngeal mucosa with sites of necrosis. The formation of an abscess
- 18. Chronic inflammatory diseases of the larynx is in the majority of cases secondary to acute inflammations.
- 19. Chronic hyperplastic laryngitis is characterized by hyperplasia of the laryngeal mucosa. Local and diffuse forms of
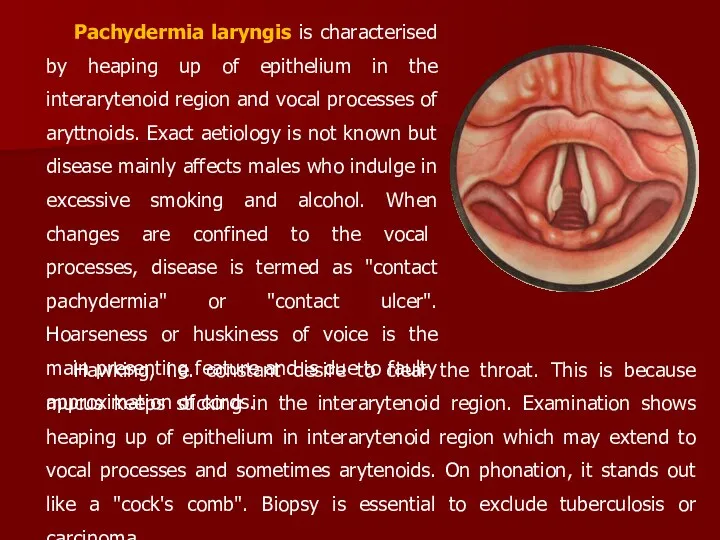
- 20. Pachydermia laryngis is characterised by heaping up of epithelium in the interarytenoid region and vocal processes
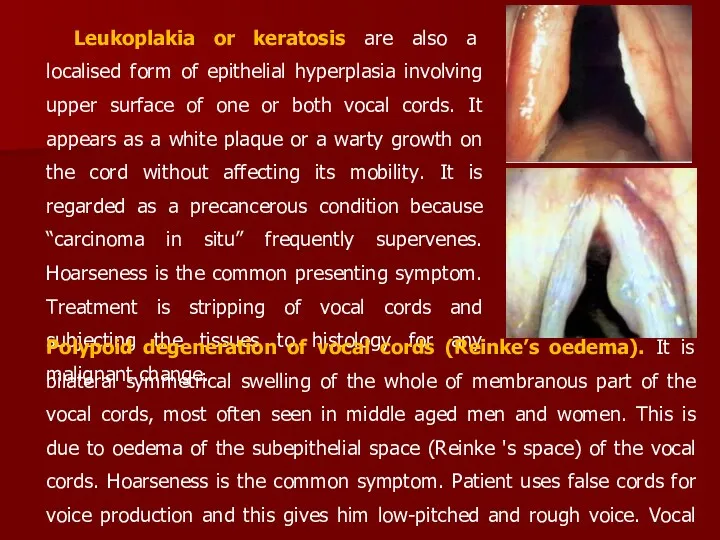
- 21. Leukoplakia or keratosis are also a localised form of epithelial hyperplasia involving upper surface of one
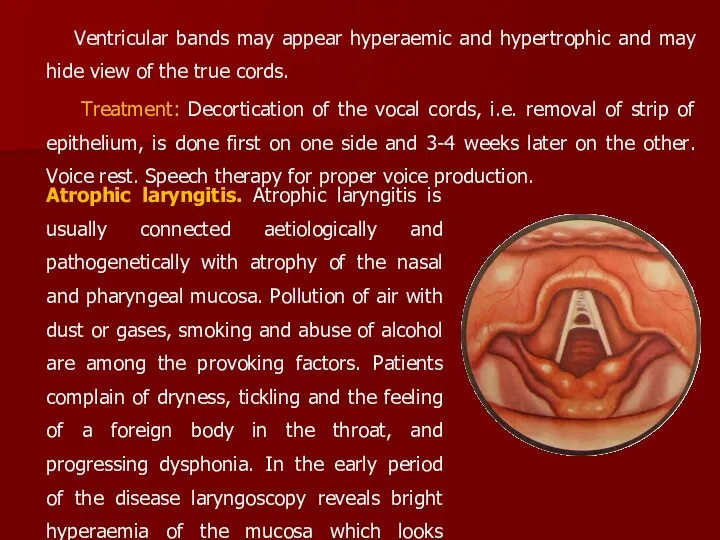
- 22. Ventricular bands may appear hyperaemic and hypertrophic and may hide view of the true cords. Treatment:
- 23. Treatment. The patient must not smoke or take irritating food; he should rest his voice. Preparations
- 24. In order to stimulate the action of the glandular apparatus of the mucosa, Флюдитек 1 ст.ложка
- 25. The haemodynamic compensatory reactions are characterized by tachycardia and increased vascular tone, which increase the minute
- 26. If stenosis persists, the pulse is accelerated, the lips, the nose and the nails become cyanotic
- 27. stage I - compensation At the stage of compensation the patient does not develop respiratory distress
- 28. stage IV - asphyxia At the stage of asphyxia, respiration is hardly possible and discontinues at
- 29. Decompensation (stage III) should be treated surgically: immediate tracheostomy or intubation are indicated. The patient can
- 30. Chronic stenosis arises due to persistent morphological changes in the larynx and the adjacent organs and
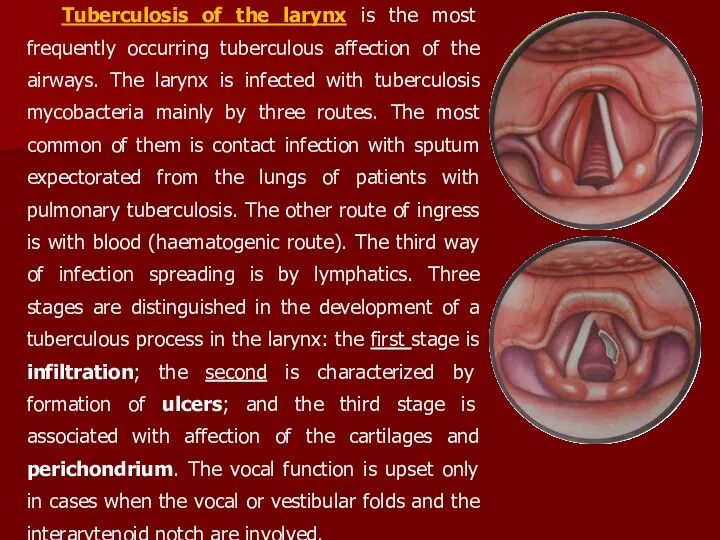
- 31. Tuberculosis of the larynx is the most frequently occurring tuberculous affection of the airways. The larynx
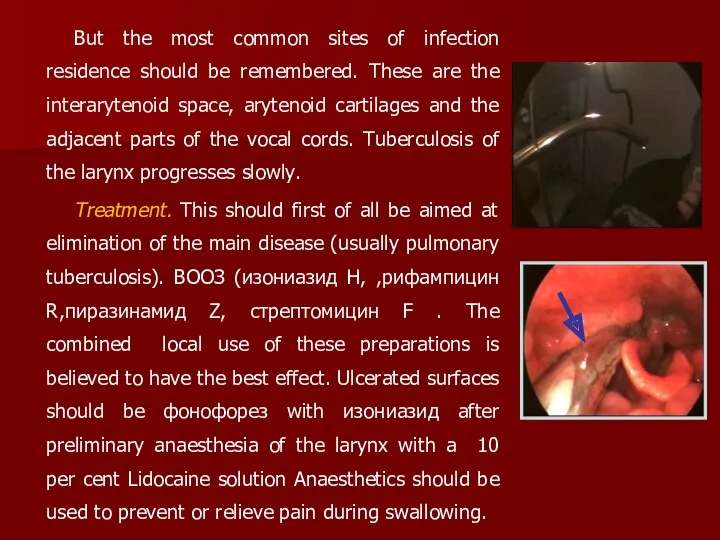
- 32. But the most common sites of infection residence should be remembered. These are the interarytenoid space,
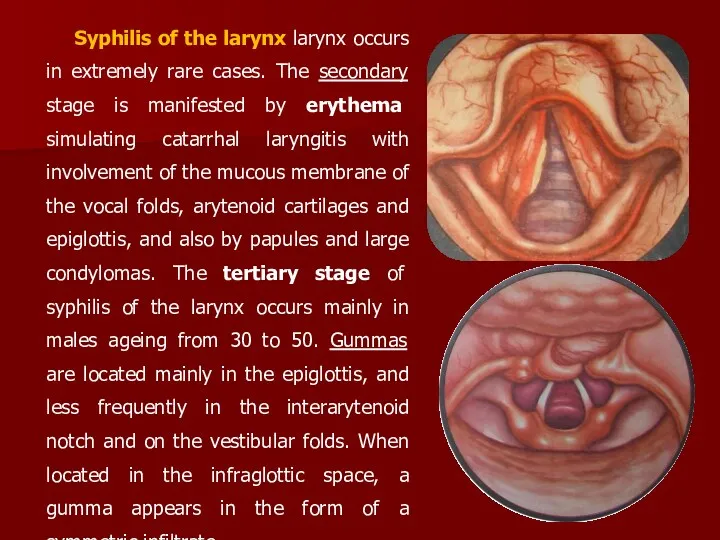
- 33. Syphilis of the larynx larynx occurs in extremely rare cases. The secondary stage is manifested by
- 34. Tumors of the upper respiratory tract. Neoplasms of the upper respiratory tract average 3-4 % of
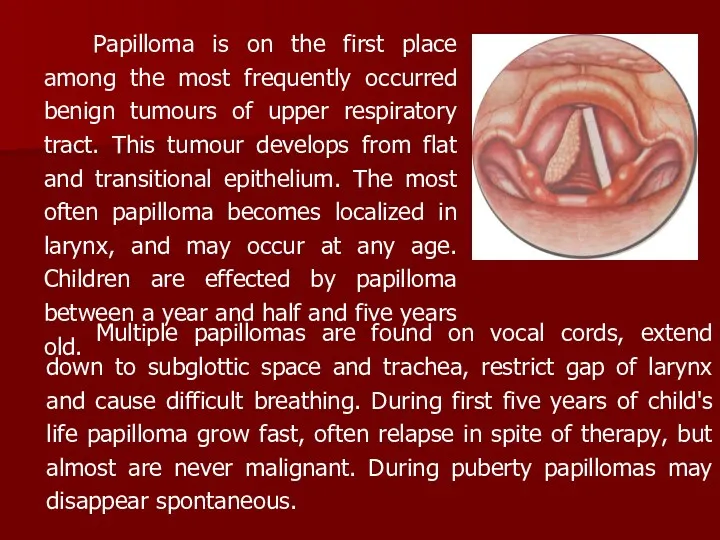
- 35. Papilloma is on the first place among the most frequently occurred benign tumours of upper respiratory
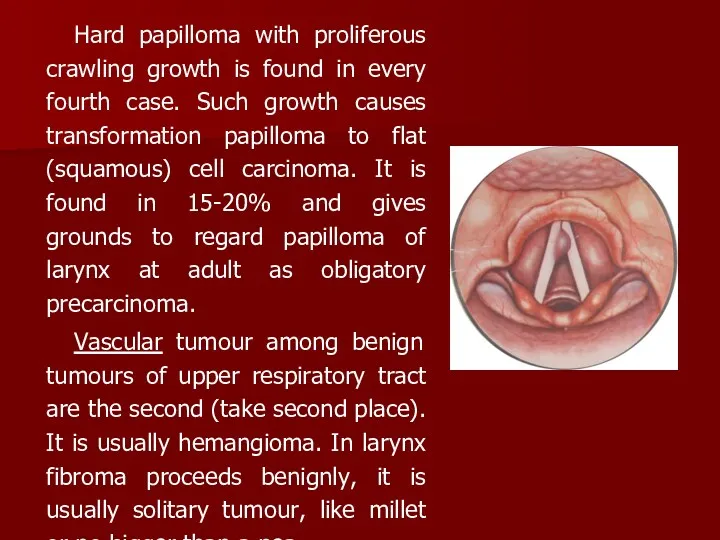
- 36. Hard papilloma with proliferous crawling growth is found in every fourth case. Such growth causes transformation
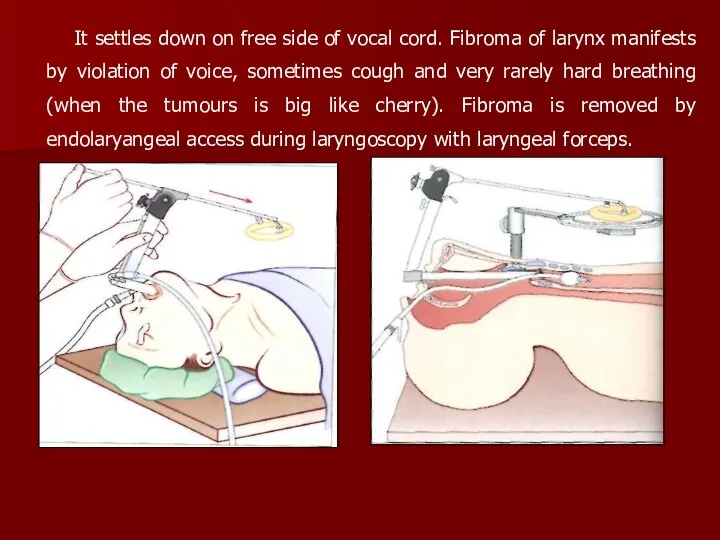
- 37. It settles down on free side of vocal cord. Fibroma of larynx manifests by violation of
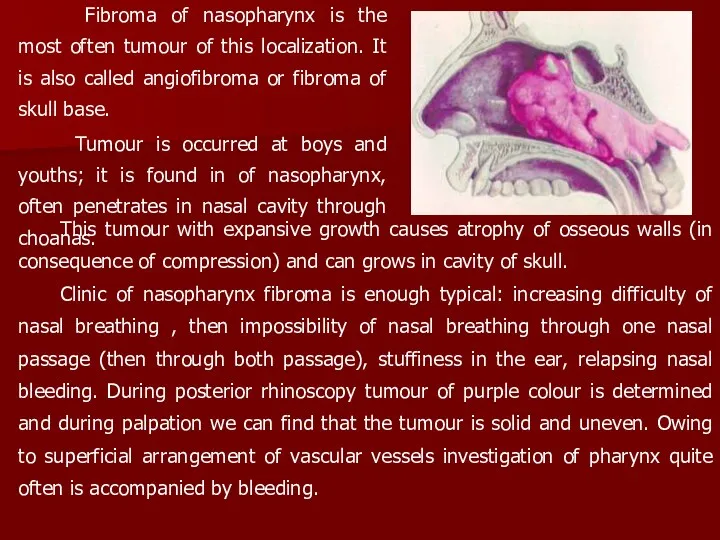
- 38. Fibroma of nasopharynx is the most often tumour of this localization. It is also called angiofibroma
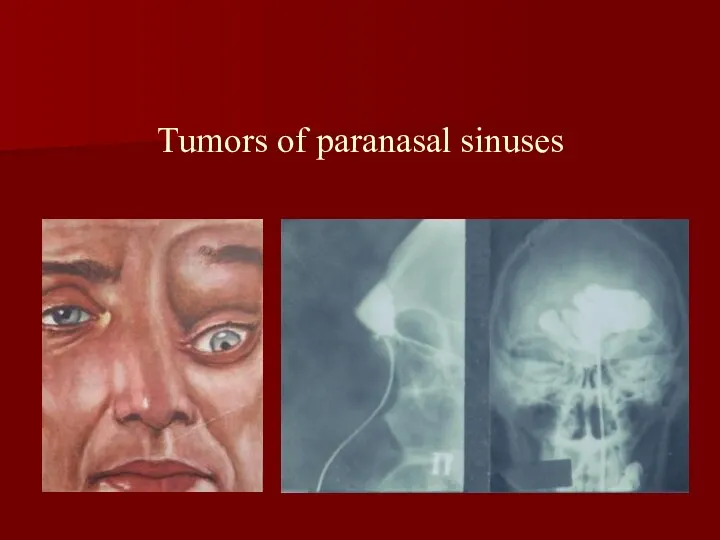
- 39. Tumors of paranasal sinuses
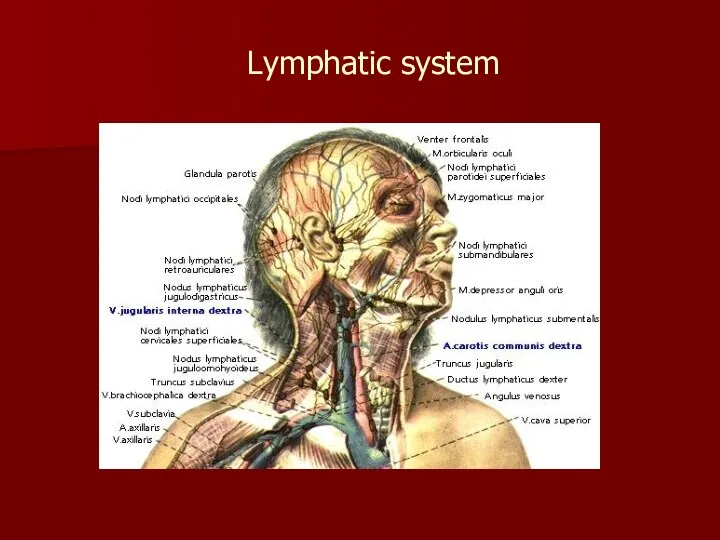
- 40. Lymphatic system
- 41. Malignant tumour. Frequency of damages of different parts of upper respiratory tract and ear by malignant
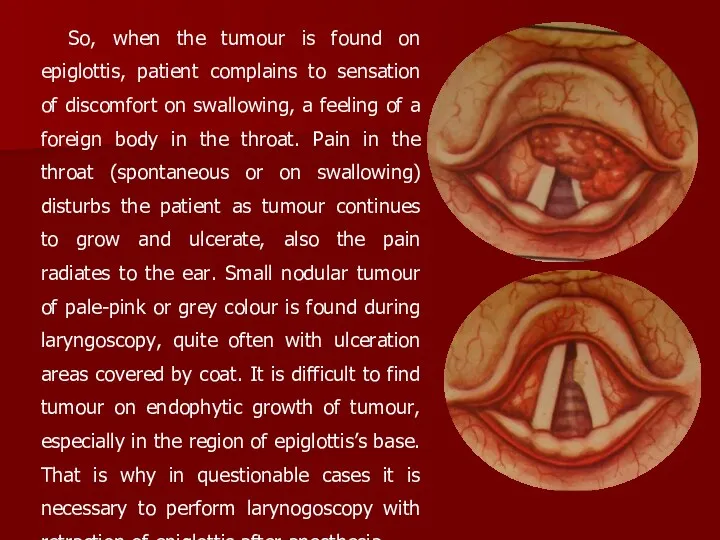
- 42. So, when the tumour is found on epiglottis, patient complains to sensation of discomfort on swallowing,
- 43. The beginning of cancer of larynx’s upper floor (cord of vestibule, ventricle of larynx) doesn’t accompany
- 44. The final diagnosis is made after carrying out biopsy. At the initial stages of the affection
- 45. The choice of the method of treatment depends upon the stage of cancer of larynx, its
- 46. There are various surgical interventions as to the cancer of the larynx depending on the spreading
- 48. Скачать презентацию
Larynx being a part of the air conducting tracts of the
Larynx being a part of the air conducting tracts of the
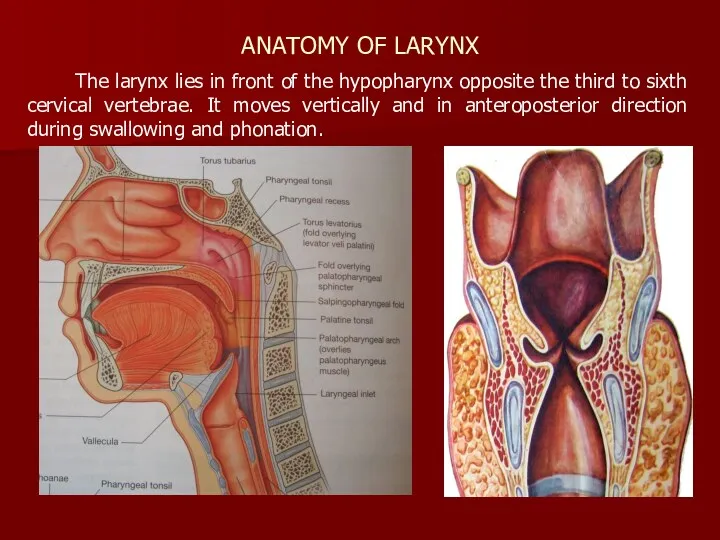
ANATOMY OF LARYNX
The larynx lies in front of the hypopharynx opposite
ANATOMY OF LARYNX
The larynx lies in front of the hypopharynx opposite
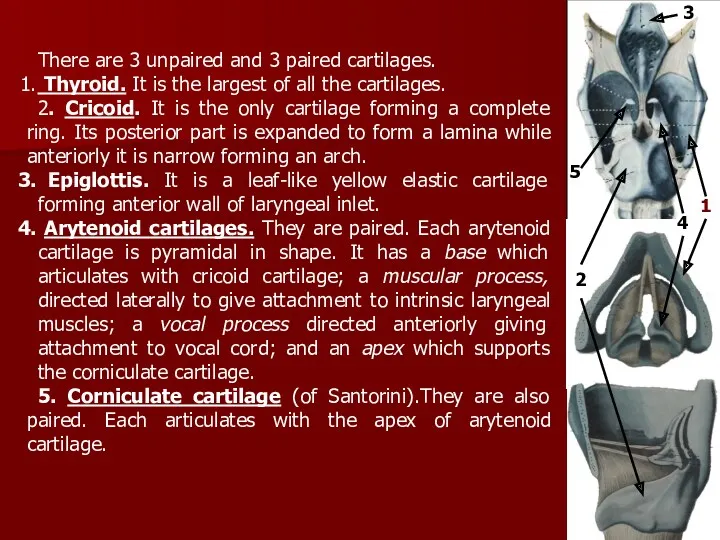
There are 3 unpaired and 3 paired cartilages.
Thyroid. It is
There are 3 unpaired and 3 paired cartilages.
Thyroid. It is
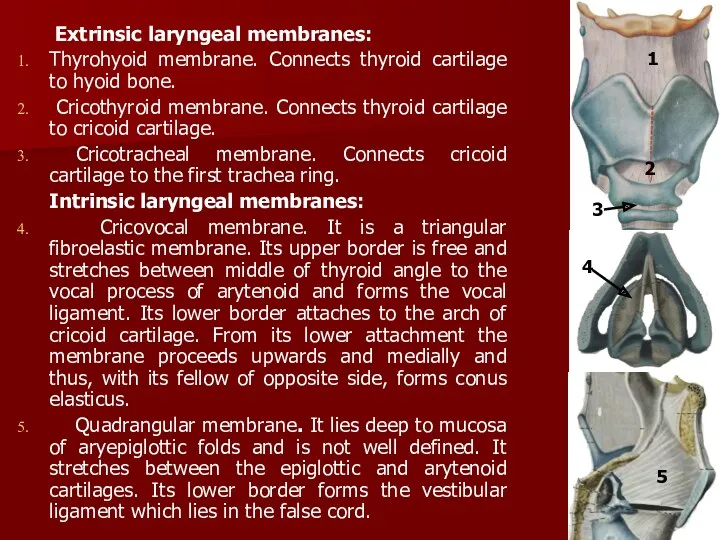
Extrinsic laryngeal membranes:
Thyrohyoid membrane. Connects thyroid cartilage to hyoid bone.
Extrinsic laryngeal membranes:
Thyrohyoid membrane. Connects thyroid cartilage to hyoid bone.
They are of two types muscles, namely intrinsic, which attach laryngeal
They are of two types muscles, namely intrinsic, which attach laryngeal
Laryngeal cavity starts at the laryngeal inlet where it communicates with
Laryngeal cavity starts at the laryngeal inlet where it communicates with
Vocal folds (true vocal cords). They are two pearly-white sharp bands
Vocal folds (true vocal cords). They are two pearly-white sharp bands
The larynx performs the following important functions:
1. Protection of lower airways
2.
The larynx performs the following important functions:
1. Protection of lower airways
2.
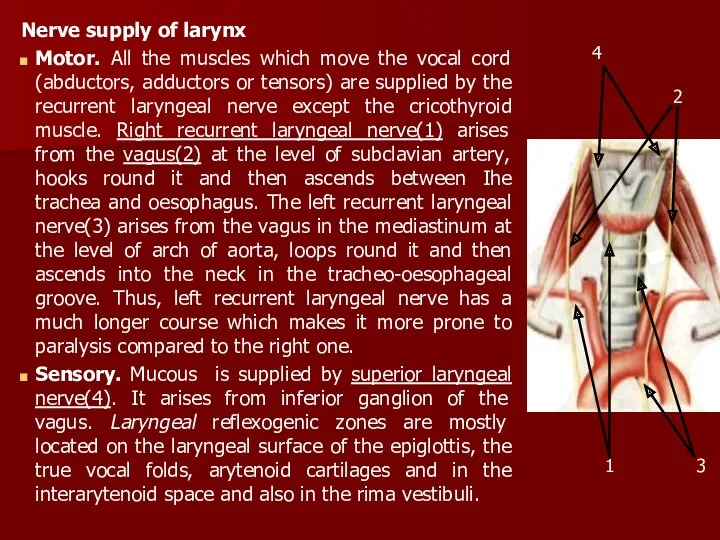
Nerve supply of larynx
Motor. All the muscles which move the vocal
Nerve supply of larynx
Motor. All the muscles which move the vocal
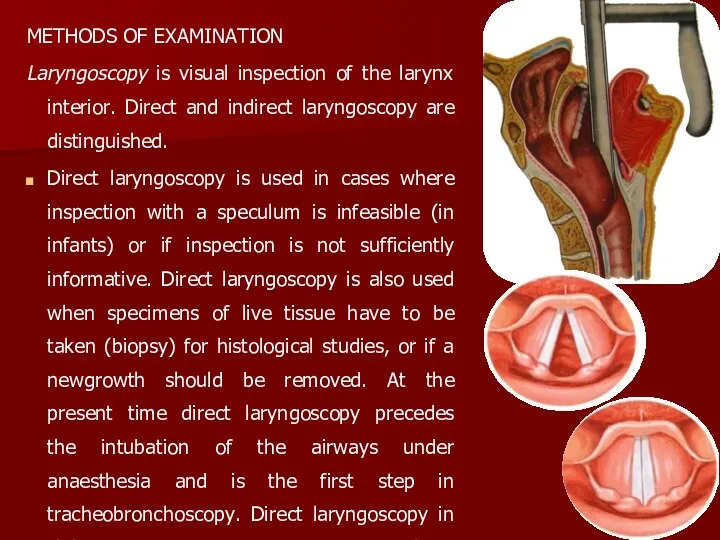
METHODS OF EXAMINATION
Laryngoscopy is visual inspection of the larynx interior. Direct
METHODS OF EXAMINATION
Laryngoscopy is visual inspection of the larynx interior. Direct
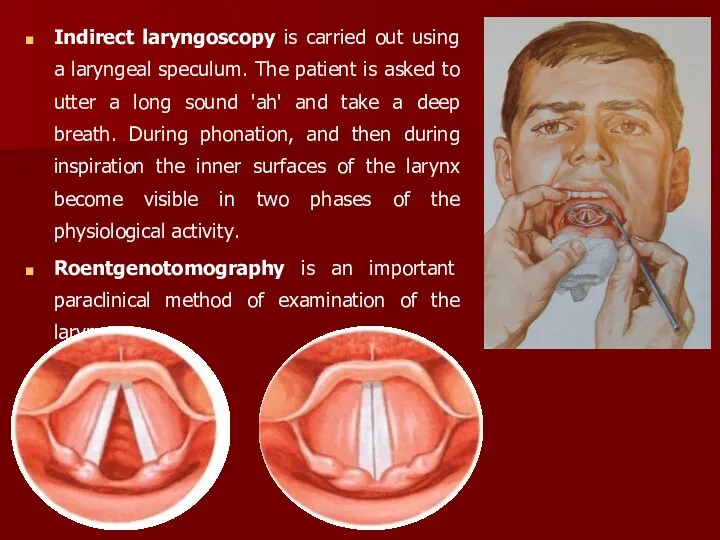
Indirect laryngoscopy is carried out using a laryngeal speculum. The patient
Indirect laryngoscopy is carried out using a laryngeal speculum. The patient
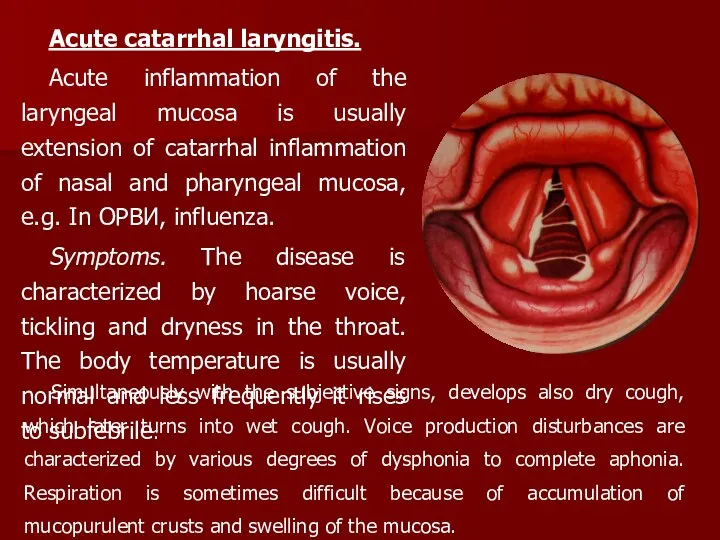
Acute catarrhal laryngitis.
Acute inflammation of the laryngeal mucosa is usually
Acute catarrhal laryngitis.
Acute inflammation of the laryngeal mucosa is usually
Treatment. The larynx should first of all be spared. The patient
Treatment. The larynx should first of all be spared. The patient

The child wakes up and tosses in his bed. Breathing becomes
The child wakes up and tosses in his bed. Breathing becomes
Treatment includes common hygienic measures, ventilation in the room, and therapeutic
Treatment includes common hygienic measures, ventilation in the room, and therapeutic
Laryngoscopy reveals hyperaemic and infiltrated laryngeal mucosa with sites of necrosis.
Laryngoscopy reveals hyperaemic and infiltrated laryngeal mucosa with sites of necrosis.
Chronic inflammatory diseases of the larynx is in the majority of
Chronic inflammatory diseases of the larynx is in the majority of
Chronic hyperplastic laryngitis is characterized by hyperplasia of the laryngeal mucosa.
Chronic hyperplastic laryngitis is characterized by hyperplasia of the laryngeal mucosa.
Pachydermia laryngis is characterised by heaping up of epithelium in the
Pachydermia laryngis is characterised by heaping up of epithelium in the
Leukoplakia or keratosis are also a localised form of epithelial hyperplasia
Leukoplakia or keratosis are also a localised form of epithelial hyperplasia
Ventricular bands may appear hyperaemic and hypertrophic and may hide view
Ventricular bands may appear hyperaemic and hypertrophic and may hide view
Treatment. The patient must not smoke or take irritating food; he
Treatment. The patient must not smoke or take irritating food; he
In order to stimulate the action of the glandular apparatus
In order to stimulate the action of the glandular apparatus
The haemodynamic compensatory reactions are characterized by tachycardia and increased vascular
The haemodynamic compensatory reactions are characterized by tachycardia and increased vascular
If stenosis persists, the pulse is accelerated, the lips, the
If stenosis persists, the pulse is accelerated, the lips, the
stage I - compensation
At the stage of compensation the patient does
stage I - compensation
At the stage of compensation the patient does
stage IV - asphyxia
At the stage of asphyxia, respiration is hardly
stage IV - asphyxia
At the stage of asphyxia, respiration is hardly
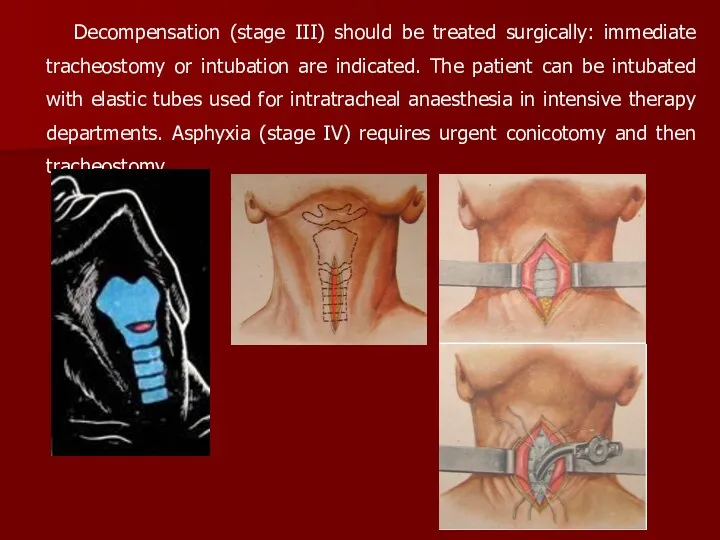
Decompensation (stage III) should be treated surgically: immediate tracheostomy or intubation
Decompensation (stage III) should be treated surgically: immediate tracheostomy or intubation
Chronic stenosis arises due to persistent morphological changes in the larynx
Chronic stenosis arises due to persistent morphological changes in the larynx
Tuberculosis of the larynx is the most frequently occurring tuberculous affection
Tuberculosis of the larynx is the most frequently occurring tuberculous affection
But the most common sites of infection residence should be remembered.
But the most common sites of infection residence should be remembered.
Syphilis of the larynx larynx occurs in extremely rare cases. The
Syphilis of the larynx larynx occurs in extremely rare cases. The
Tumors of the upper respiratory tract.
Neoplasms of the upper respiratory tract
Tumors of the upper respiratory tract.
Neoplasms of the upper respiratory tract
Papilloma is on the first place among the most frequently occurred
Papilloma is on the first place among the most frequently occurred
Hard papilloma with proliferous crawling growth is found in every fourth
Hard papilloma with proliferous crawling growth is found in every fourth
It settles down on free side of vocal cord. Fibroma of
It settles down on free side of vocal cord. Fibroma of
Fibroma of nasopharynx is the most often tumour of this
Fibroma of nasopharynx is the most often tumour of this
Tumors of paranasal sinuses
Tumors of paranasal sinuses
Lymphatic system
Lymphatic system
Malignant tumour. Frequency of damages of different parts of upper respiratory
Malignant tumour. Frequency of damages of different parts of upper respiratory
So, when the tumour is found on epiglottis, patient complains to
So, when the tumour is found on epiglottis, patient complains to
The beginning of cancer of larynx’s upper floor (cord of vestibule,
The beginning of cancer of larynx’s upper floor (cord of vestibule,
The final diagnosis is made after carrying out biopsy.
At the initial
The final diagnosis is made after carrying out biopsy.
At the initial
The choice of the method of treatment depends upon the stage
The choice of the method of treatment depends upon the stage
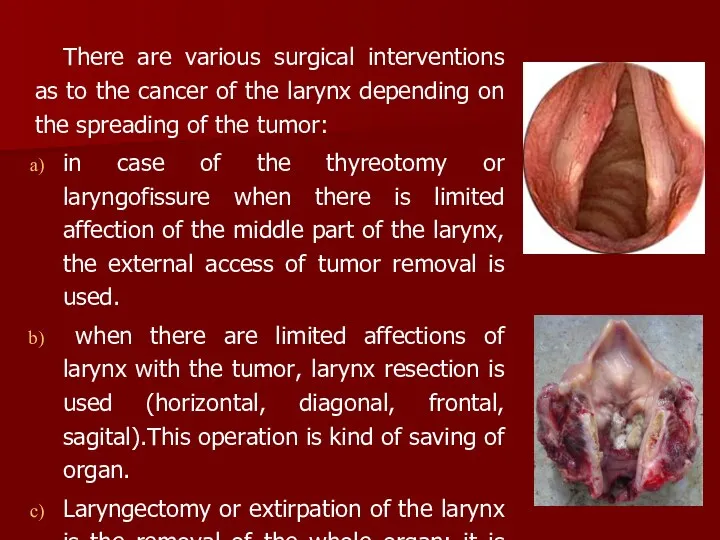
There are various surgical interventions as to the cancer of the
There are various surgical interventions as to the cancer of the
 Терінің вирусты аурулары
Терінің вирусты аурулары Физиология системы крови. Функции, состав, количество и свойства крови
Физиология системы крови. Функции, состав, количество и свойства крови Опухолевый рост
Опухолевый рост Средства, влияющие на функции органов дыхания
Средства, влияющие на функции органов дыхания Сестринский уход при заболеваниях почек и МВП
Сестринский уход при заболеваниях почек и МВП Строение молочных зубов
Строение молочных зубов Организация и содержание работы медицинской сестры палатной (постовой)
Организация и содержание работы медицинской сестры палатной (постовой) Урологические заболевания
Урологические заболевания Синдромы нарушения высших психических функций
Синдромы нарушения высших психических функций Бет-жақ ауытқулары бар балаларды диспансерлік бақылау
Бет-жақ ауытқулары бар балаларды диспансерлік бақылау Иннервация зубов и челюстей. Топографическая анатомия тройничного нерва
Иннервация зубов и челюстей. Топографическая анатомия тройничного нерва Медико-генетикалық кеңестің нәрестенің туа біткен ақаулықтарын алдын-алудағы рөлі және диагностикасы
Медико-генетикалық кеңестің нәрестенің туа біткен ақаулықтарын алдын-алудағы рөлі және диагностикасы Острая сердечная недостаточность
Острая сердечная недостаточность Kyasanur forest disease (KFD)
Kyasanur forest disease (KFD) Расстройства внимания
Расстройства внимания Клиникалық зерттеулерді жүргізу және ұйымдастыру. КЗ этикалық аспектілері
Клиникалық зерттеулерді жүргізу және ұйымдастыру. КЗ этикалық аспектілері Сестринский уход и введение центрального венозного катетера
Сестринский уход и введение центрального венозного катетера Медицина катастроф. Основные понятия
Медицина катастроф. Основные понятия Бауыр –өт жолы мен ұйқы безінің. ауруларын тағаммен емдеу
Бауыр –өт жолы мен ұйқы безінің. ауруларын тағаммен емдеу Ретинопатия у новорожденных
Ретинопатия у новорожденных Холера. Лечение. Профилактика
Холера. Лечение. Профилактика Билиарлы жүйенің және өт шығару жолдарының дисфункциясы
Билиарлы жүйенің және өт шығару жолдарының дисфункциясы Патофізіологія сенсорних систем. Порушення функцій зорового аналізатора
Патофізіологія сенсорних систем. Порушення функцій зорового аналізатора Жүректің ишемиялық ауруында қолданылатын диуретик тиазидиннің әсері
Жүректің ишемиялық ауруында қолданылатын диуретик тиазидиннің әсері Новое в медицинском образовании
Новое в медицинском образовании Основні напрямки розвитку соціальної медицини (громадського здоров’я) як основи менеджменту в охороні здоров’я
Основні напрямки розвитку соціальної медицини (громадського здоров’я) як основи менеджменту в охороні здоров’я Редко встречающиеся аллергические заболевания. Экзогенный аллергический альвеолит
Редко встречающиеся аллергические заболевания. Экзогенный аллергический альвеолит Пульмонологиядагы микробиологиялық зерттеу әдістері
Пульмонологиядагы микробиологиялық зерттеу әдістері