- Deparment of infectious diseases

Содержание
- 2. ABOUT MYSELF AJAY . GUNDAWAR GROUP:18A COURSE: 5TH
- 4. Malaria Malaria is a mosquito-borne infectious disease of humans and other animals caused by parasitic protozoans
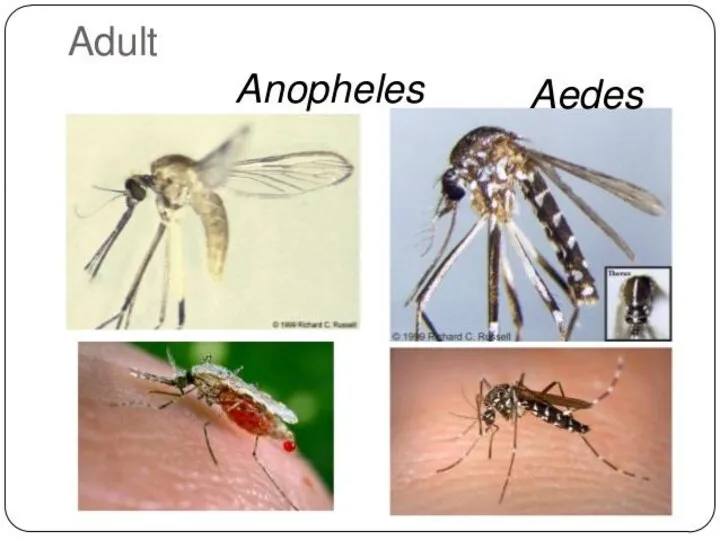
- 5. The disease is transmitted most commonly by an infected female Anopheles mosquito. The mosquito bite introduces
- 6. Plasmodium Falciparum - Malaria Plasmodium falciparum is the Plasmodium species responsible for 85 % of the
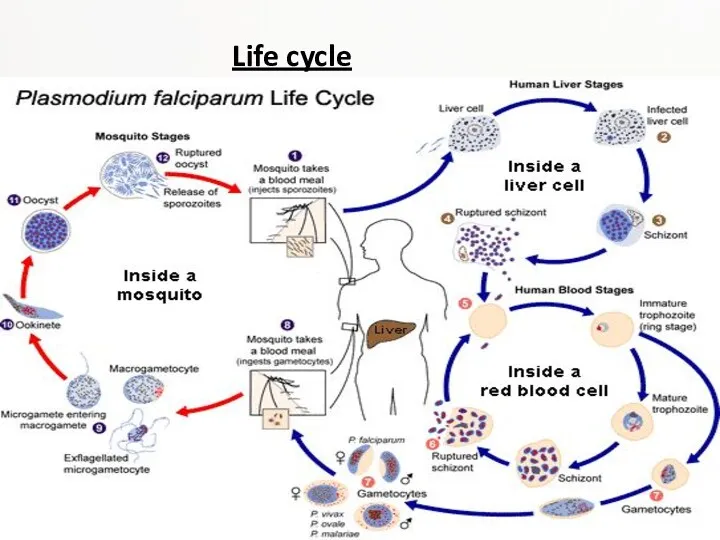
- 7. Life cycle
- 8. Malaria is carried by Anopheles mosquitoes. Of the over 400 Anopheles species, only 30–40 can transmit
- 9. Pathogenesis Transmission of P. falciparum occurs between humans and Anopheles mosquitoes. Mosquito vectors pass malaria from
- 10. Infectious Dose, Incubation, Colonization Symptoms of Malaria typically begin 8-25 days following infection however, in a
- 11. Epidemiology The key to Malaria-endemic is Anopheles the mosquito’s ability to live in a certain area.
- 12. Virulence Factors PfEMP1,P. falciparum erythrocye membrane protein 1, is an adhesive ligand protein which is created
- 13. Symptoms After being bitten by an infected mosquito, symptoms usually begin within 10–30 days. Malaria can
- 14. Some less noticeable manifestations: enlargement of the spleen or liver increased breathing frequency mild anemia mild
- 15. Some less noticeable manifestations: abnormalities in blood coagulation hemoglobin in the urine high acidity of the
- 16. Diagnosis Malaria is usually diagnosed by examining a blood sample under a microscope. There are also
- 17. Rapid and accurate diagnosis using microscopic examination of blood smears is the most precise way to
- 18. Treatment Most malaria deaths occur in rural areas. Quick progression from illness to death can be
- 19. P. falciparum and P. vivax have been confirmed to be resistant (in some areas) to many
- 20. Primaquine, is used as an adjunct against certain Plasmodium species. It is active against the dormant
- 21. Prevention Insecticide-treated bed nets may reduce deaths of children under 5 years up to 20 %
- 23. Many malaria-carrying mosquitoes are endophilic, meaning that they typically rest inside the house after taking a
- 24. Recommendations for pregnant women living in malaria endemic areas: Eat iron and folate supplements to prevent
- 25. Additional personal protection methods include: -glass windows (a well-constructed house) repellent white or light-colored clothes covering
- 26. Plasmodium vivax is a protozoal parasite and a human pathogen. The most frequent and widely distributed
- 27. On the pathogenesis of Plasmodium vivax malaria: perspectives from the Brazilian field. Life-threatening Plasmodium vivax malaria
- 28. Plasmodium vivax and P. falciparum epidemiology in Gambella, south-west Ethiopia Plasmodium vivax and P. falciparum epidemiology
- 29. Mouth becomes dry, nausea and loss of appetite • Headache, muscular pain and joint pain •
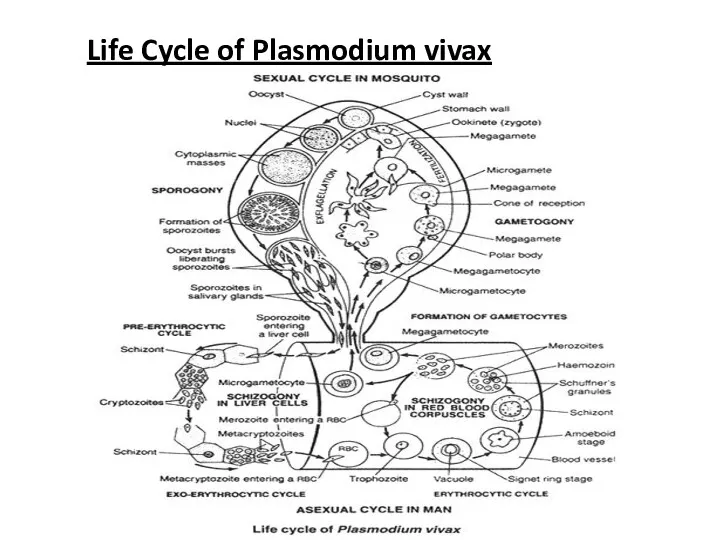
- 30. Life Cycle of Plasmodium vivax
- 31. Hosts:- Plasmodium completes its lifecycle in two hosts (digenetic): Man and female Anopheles mosquito. 1. Primary
- 32. ASEXUAL CYCLE OF Plasmodium, IN MAN Infective form of Plasmodium is known as sporozoites. Sporozoites are
- 33. 1. Asexual Schizogony:- Schizogony is the asexual phase of reproduction of Plasmodium. It takes place in
- 34. b. Exo-erythrocytic schizogony: After re-entering fresh liver cell each cryptozoites divides to form a large number
- 35. ii. Signet Ring Stage:- As the merozoites grow a vacuole appears in the center and the
- 36. d. Post-erythrocytic schizogony:- Sometimes, some merozoites produced in erythrocytic schizogony reach the liver cells and undergo
- 37. SEXUAL CYCLE OF Plasmodium IN MOSQUITO When a female Anopheles sucks the blood of a malaria
- 38. b. Fertilization: The male gamete enters the female gamete through the fertilization cone formed at female
- 39. Incubation period: The period between infection and the appearance of first symptoms is called incubation period.
- 40. Control controlled by three ways 1. Destruction of vector 2. Prevention of infection(prophylaxis) 3. Treatment of
- 41. 1. Destruction of vector (Anopheles mosquito) • Mosquito can be killed by spraying DDT, BHC, Dieldrin,
- 42. Plasmodium ovale Plasmodium ovale is a species of parasitic protozoa that causes tertian malaria in humans.
- 43. Prepatent period.Humans are the only natural hosts for P. ovale. Much of what is known about
- 44. Epidemiology While it is frequently said that P. ovale is very limited in its range being
- 45. Clinical features The prepatent period in the human ranges from 12 to 20 days. Some forms
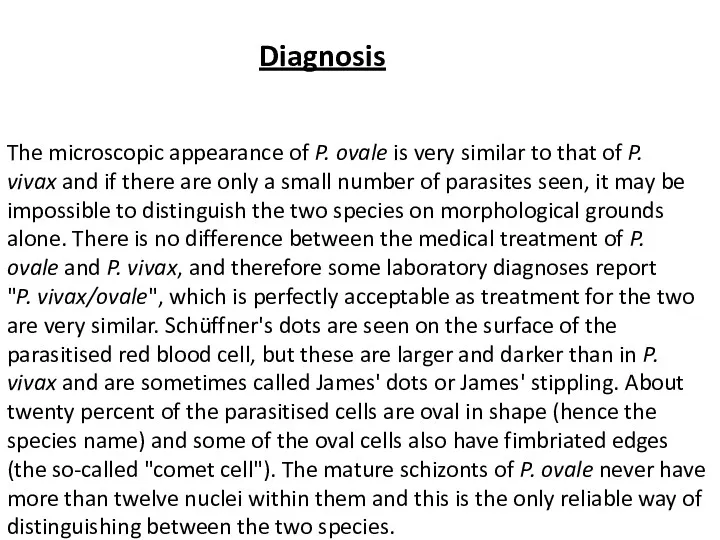
- 46. Diagnosis The microscopic appearance of P. ovale is very similar to that of P. vivax and
- 47. P. vivax and P. ovale that has been sitting in EDTA for more than half-an-hour before
- 48. Treatment Standard treatment is concurrent treatment with chloroquine and primaquine . The combination atovaquone-proguanil may be
- 49. Plasmodium malariae Plasmodium malariae is a parasitic protozoa that causes malaria in humans. It is one
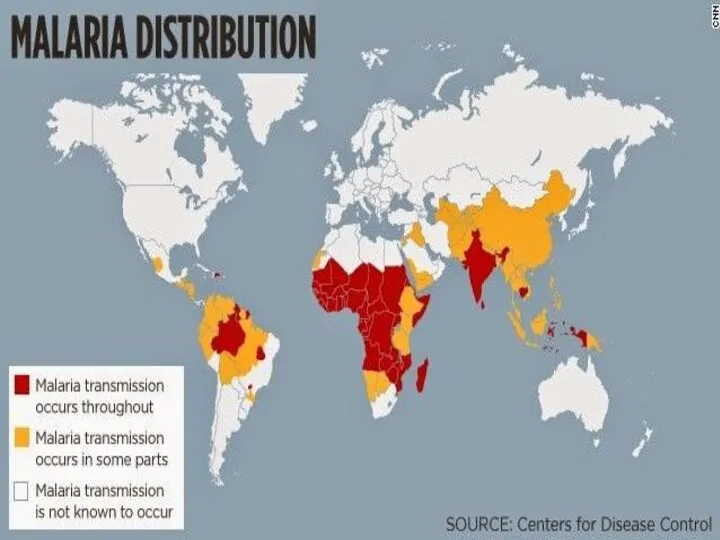
- 50. Epidemiology Each year, approximately 500 million people will be infected with malaria worldwide Of those infected,
- 51. Transmission P. malariae can be maintained at very low infection rates among a sparse and mobile
- 52. Incubation period Information about the prepatent period, or the period of time between the infection of
- 53. Morphology The ring stages that are formed by the invasion of merozoites released by rupturing liver
- 54. Along with bouts of fever and more general clinical symptoms such as chills and nausea, the
- 55. Diagnostics The preferable method for diagnosis of P. malariae is through the examination of peripheral blood
- 56. Life cycle P. malariae is the only human malaria parasite that causes fevers that recur at
- 57. Laboratory considerations P. vivax and P. ovale sitting in EDTA for more than 30 minutes before
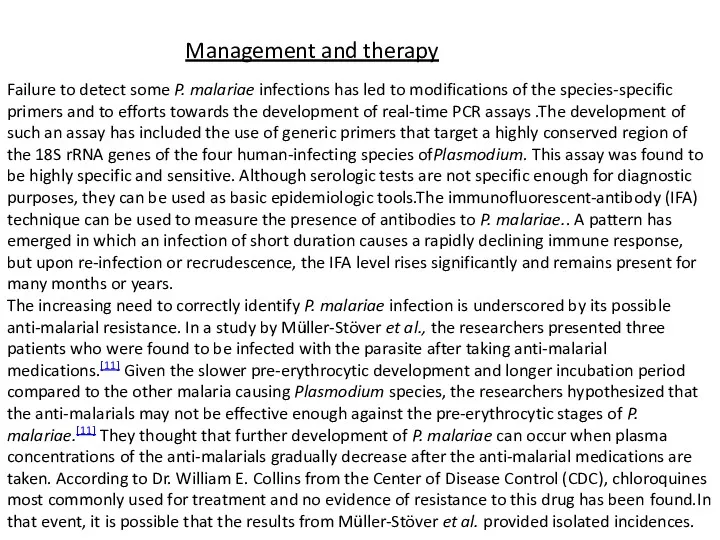
- 58. Management and therapy Failure to detect some P. malariae infections has led to modifications of the
- 59. Public health, prevention strategies and vaccines The food vacuole is the specialized compartment that degrades hemoglobin
- 62. Скачать презентацию
ABOUT MYSELF
AJAY . GUNDAWAR
GROUP:18A
COURSE: 5TH
ABOUT MYSELF
AJAY . GUNDAWAR
GROUP:18A
COURSE: 5TH
Malaria
Malaria is a mosquito-borne infectious disease of humans and other animals caused by
Malaria
Malaria is a mosquito-borne infectious disease of humans and other animals caused by
The disease is transmitted most commonly by an infected female Anopheles mosquito.
The disease is transmitted most commonly by an infected female Anopheles mosquito.
Plasmodium Falciparum - Malaria
Plasmodium falciparum is the Plasmodium species responsible for 85 % of
Plasmodium Falciparum - Malaria
Plasmodium falciparum is the Plasmodium species responsible for 85 % of
Life cycle
Life cycle
Malaria is carried by Anopheles mosquitoes. Of the over 400 Anopheles species, only 30–40 can
Malaria is carried by Anopheles mosquitoes. Of the over 400 Anopheles species, only 30–40 can
Pathogenesis
Transmission of P. falciparum occurs between humans and Anopheles mosquitoes. Mosquito vectors pass
Pathogenesis
Transmission of P. falciparum occurs between humans and Anopheles mosquitoes. Mosquito vectors pass
Infectious Dose, Incubation, Colonization
Symptoms of Malaria typically begin 8-25 days following
Infectious Dose, Incubation, Colonization
Symptoms of Malaria typically begin 8-25 days following
Epidemiology
The key to Malaria-endemic is Anopheles the mosquito’s ability to live
Epidemiology
The key to Malaria-endemic is Anopheles the mosquito’s ability to live
Virulence Factors
PfEMP1,P. falciparum erythrocye membrane protein 1, is an adhesive ligand protein
Virulence Factors
PfEMP1,P. falciparum erythrocye membrane protein 1, is an adhesive ligand protein
Symptoms
After being bitten by an infected mosquito, symptoms usually begin within
Symptoms
After being bitten by an infected mosquito, symptoms usually begin within
Some less noticeable manifestations:
enlargement of the spleen or liver
increased breathing frequency
mild
enlargement of the spleen or liver
increased breathing frequency
mild
Some less noticeable manifestations:
abnormalities in blood coagulation
hemoglobin in the urine
high acidity
Some less noticeable manifestations:
abnormalities in blood coagulation
hemoglobin in the urine
high acidity
Diagnosis
Malaria is usually diagnosed by examining a blood sample under a
Diagnosis
Malaria is usually diagnosed by examining a blood sample under a
Rapid and accurate diagnosis using microscopic examination of blood smears is
Rapid and accurate diagnosis using microscopic examination of blood smears is
Treatment
Most malaria deaths occur in rural areas. Quick progression from illness
Treatment
Most malaria deaths occur in rural areas. Quick progression from illness
P. falciparum and P. vivax have been confirmed to be resistant (in some areas)
P. falciparum and P. vivax have been confirmed to be resistant (in some areas)
Primaquine, is used as an adjunct against certain Plasmodium species. It is active
Primaquine, is used as an adjunct against certain Plasmodium species. It is active
Prevention
Insecticide-treated bed nets may reduce deaths of children under 5 years up to
Prevention
Insecticide-treated bed nets may reduce deaths of children under 5 years up to
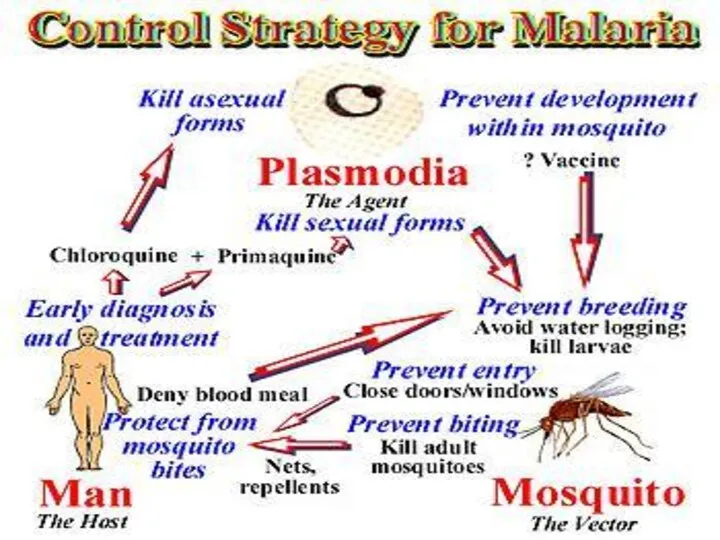
Many malaria-carrying mosquitoes are endophilic, meaning that they typically rest inside
Many malaria-carrying mosquitoes are endophilic, meaning that they typically rest inside
Recommendations for pregnant women living in malaria endemic areas:
Eat iron and
Recommendations for pregnant women living in malaria endemic areas:
Eat iron and
Additional personal protection methods include:
-glass windows (a well-constructed house)
repellent
white or light-colored clothes
Additional personal protection methods include:
-glass windows (a well-constructed house)
repellent
white or light-colored clothes
Plasmodium vivax
is a protozoal parasite and a human pathogen. The most frequent and widely
Plasmodium vivax
is a protozoal parasite and a human pathogen. The most frequent and widely
On the pathogenesis of Plasmodium vivax malaria: perspectives from the Brazilian
On the pathogenesis of Plasmodium vivax malaria: perspectives from the Brazilian
Plasmodium vivax and P. falciparum epidemiology in Gambella, south-west Ethiopia
Plasmodium vivax
Plasmodium vivax and P. falciparum epidemiology in Gambella, south-west Ethiopia
Plasmodium vivax
Mouth becomes dry, nausea and loss of appetite
• Headache, muscular pain
Mouth becomes dry, nausea and loss of appetite
• Headache, muscular pain
Life Cycle of Plasmodium vivax
Life Cycle of Plasmodium vivax
Hosts:-
Plasmodium completes its lifecycle in two hosts (digenetic): Man and female
Hosts:-
Plasmodium completes its lifecycle in two hosts (digenetic): Man and female
ASEXUAL CYCLE OF Plasmodium, IN MAN
Infective form of Plasmodium is known
ASEXUAL CYCLE OF Plasmodium, IN MAN
Infective form of Plasmodium is known
1. Asexual Schizogony:-
Schizogony is the asexual phase of reproduction of Plasmodium.
1. Asexual Schizogony:-
Schizogony is the asexual phase of reproduction of Plasmodium.
b. Exo-erythrocytic schizogony:
After re-entering fresh liver cell each cryptozoites divides to
b. Exo-erythrocytic schizogony:
After re-entering fresh liver cell each cryptozoites divides to
ii. Signet Ring Stage:-
As the merozoites grow a vacuole appears in
ii. Signet Ring Stage:-
As the merozoites grow a vacuole appears in
d. Post-erythrocytic schizogony:-
Sometimes, some merozoites produced in erythrocytic schizogony reach the
d. Post-erythrocytic schizogony:-
Sometimes, some merozoites produced in erythrocytic schizogony reach the
SEXUAL CYCLE OF Plasmodium IN MOSQUITO
When a female Anopheles sucks the
SEXUAL CYCLE OF Plasmodium IN MOSQUITO
When a female Anopheles sucks the
b. Fertilization:
The male gamete enters the female gamete through the fertilization
b. Fertilization:
The male gamete enters the female gamete through the fertilization
Incubation period:
The period between infection and the appearance of first symptoms
Incubation period:
The period between infection and the appearance of first symptoms
Control
controlled by three ways
1. Destruction of vector
2. Prevention of infection(prophylaxis)
3. Treatment
Control
controlled by three ways
1. Destruction of vector
2. Prevention of infection(prophylaxis)
3. Treatment
1. Destruction of vector (Anopheles mosquito)
• Mosquito can be killed by
1. Destruction of vector (Anopheles mosquito)
• Mosquito can be killed by
Plasmodium ovale
Plasmodium ovale is a species of parasitic protozoa that causes tertian malaria in humans. It
Plasmodium ovale
Plasmodium ovale is a species of parasitic protozoa that causes tertian malaria in humans. It
Prepatent period.Humans are the only natural hosts for P. ovale. Much of
Prepatent period.Humans are the only natural hosts for P. ovale. Much of
Epidemiology
While it is frequently said that P. ovale is very limited in its range
Epidemiology
While it is frequently said that P. ovale is very limited in its range
Clinical features
The prepatent period in the human ranges from 12 to
Clinical features
The prepatent period in the human ranges from 12 to
Diagnosis
The microscopic appearance of P. ovale is very similar to that of P. vivax and
Diagnosis
The microscopic appearance of P. ovale is very similar to that of P. vivax and
P. vivax and P. ovale that has been sitting in EDTA for more than half-an-hour before
P. vivax and P. ovale that has been sitting in EDTA for more than half-an-hour before
Treatment
Standard treatment is concurrent treatment with chloroquine and primaquine . The combination atovaquone-proguanil may
Treatment
Standard treatment is concurrent treatment with chloroquine and primaquine . The combination atovaquone-proguanil may
Plasmodium malariae
Plasmodium malariae is a parasitic protozoa that causes malaria in humans. It is one of several
Plasmodium malariae
Plasmodium malariae is a parasitic protozoa that causes malaria in humans. It is one of several
Epidemiology
Each year, approximately 500 million people will be infected with malaria
Epidemiology
Each year, approximately 500 million people will be infected with malaria
Transmission
P. malariae can be maintained at very low infection rates among a
Transmission
P. malariae can be maintained at very low infection rates among a
Incubation period
Information about the prepatent period, or the period of time between
Incubation period
Information about the prepatent period, or the period of time between
Morphology
The ring stages that are formed by the invasion of merozoites released
Morphology
The ring stages that are formed by the invasion of merozoites released
Along with bouts of fever and more general clinical symptoms such
Along with bouts of fever and more general clinical symptoms such
Diagnostics
The preferable method for diagnosis of P. malariae is through the examination of
Diagnostics
The preferable method for diagnosis of P. malariae is through the examination of
Life cycle
P. malariae is the only human malaria parasite that causes fevers that recur
Life cycle
P. malariae is the only human malaria parasite that causes fevers that recur
Laboratory considerations
P. vivax and P. ovale sitting in EDTA for more than 30 minutes
Laboratory considerations
P. vivax and P. ovale sitting in EDTA for more than 30 minutes
Management and therapy
Failure to detect some P. malariae infections has led to modifications
Management and therapy
Failure to detect some P. malariae infections has led to modifications

Public health, prevention strategies and vaccines
The food vacuole is the specialized
Public health, prevention strategies and vaccines
The food vacuole is the specialized
 Дәнекер жүйесі ауруларының емдеу және диагностика стандарттары
Дәнекер жүйесі ауруларының емдеу және диагностика стандарттары Профилактика и лечение ОРИ и гриппа у беременных
Профилактика и лечение ОРИ и гриппа у беременных Предотвращение распространения гриппа, острых респираторных вирусных инфекций и коронавирусной инфекции
Предотвращение распространения гриппа, острых респираторных вирусных инфекций и коронавирусной инфекции Атопический дерматит. Клиническая классификация
Атопический дерматит. Клиническая классификация Личностные особенности медицинской сестры и их влияние на профессиональное общение с пациентом
Личностные особенности медицинской сестры и их влияние на профессиональное общение с пациентом Рассеянный склероз, орэм. Диагностика, дифференциальная диагностика, реабилитация
Рассеянный склероз, орэм. Диагностика, дифференциальная диагностика, реабилитация Буйрек трансплантациясы
Буйрек трансплантациясы Мужская половая система, женская половая система, выделительная система, эмбриология
Мужская половая система, женская половая система, выделительная система, эмбриология Здравоохранение как социальный институт
Здравоохранение как социальный институт Болезни органов дыхания у детей
Болезни органов дыхания у детей Патологія слинних залоз
Патологія слинних залоз Рак молочной железы
Рак молочной железы Жоғарғы интенсивті лазерлік сәулелердің биологиялық ұлпаларға әсерінің механизмі
Жоғарғы интенсивті лазерлік сәулелердің биологиялық ұлпаларға әсерінің механизмі Современные методы фармацевтического анализа
Современные методы фармацевтического анализа Системные васкулиты
Системные васкулиты ГЭРБ и бронхиальная астма
ГЭРБ и бронхиальная астма Диспансеризация при заболевании органов пищевареня
Диспансеризация при заболевании органов пищевареня Иммунология и иммунитет
Иммунология и иммунитет Бастапқы медициналық-санитариялық көмек көрсету деңгейінде ұйымдастыру
Бастапқы медициналық-санитариялық көмек көрсету деңгейінде ұйымдастыру Виды травм мягких тканей лица
Виды травм мягких тканей лица Гигиена труда медицинских работников при использовании лазеров и в барокамерах
Гигиена труда медицинских работников при использовании лазеров и в барокамерах Гострий апендицит у дітей
Гострий апендицит у дітей Ортопедиялық стоматологиядағы тексеру әдістері
Ортопедиялық стоматологиядағы тексеру әдістері Фармакокинетика и фармакодинамика
Фармакокинетика и фармакодинамика Салауатты өмір салты
Салауатты өмір салты Неинфекционные и инфекционные гнойно-септические заболевания кожи и пупка, сепсис новорожденных
Неинфекционные и инфекционные гнойно-септические заболевания кожи и пупка, сепсис новорожденных Неотложная помощь при заболевавниях органа зрения
Неотложная помощь при заболевавниях органа зрения Острая дыхательная недостаточность
Острая дыхательная недостаточность