- Diabetes mellitus. (Subject 8)

Содержание
- 2. General information First reports – ancient times ‘diabetes’ – excessive urination ‘mellitus’ –honey. 1922 – insulin
- 3. DM statistics (IDF) 382 millions diabetic patients worldwide (8,3%) 46% undiagnosed (in Sub-Saharan Africa up to
- 4. Insulin effects Carbohydrate Metabolism Insulin dependent tissues– muscles, adipose tissue, liver - can uptake glucose ONLY
- 5. Insulin effects Carbohydrate Metabolism Increases glycogen synthesis in the liver. ↓ blood glucose concentration. In the
- 6. Insulin effects Lipid metabolism ? synthesis of fatty acids in the liver. ? lipolysis in adipose
- 7. Biological effects of insulin Very fast effect – ? glucose and ions transport into the cells.
- 8. DIABETES - is a complex metabolic disorder resulting from absolute or relative insulin deficiency
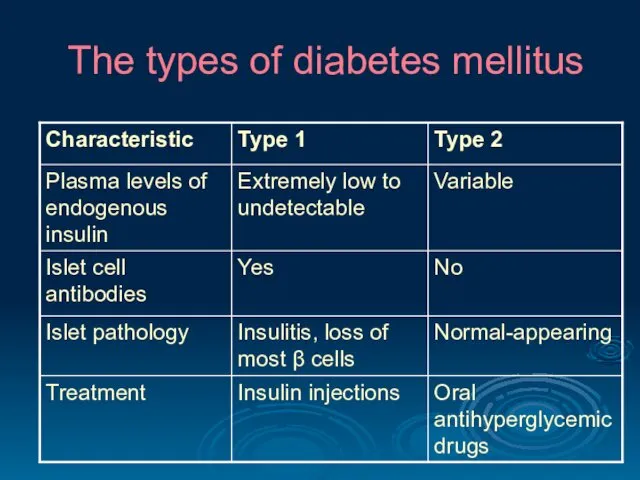
- 9. The types of diabetes mellitus
- 10. The types of diabetes mellitus
- 11. Diabetes Mellitus type 1 Type 1 DM was previously named insulin-dependent. Insulin production is low or
- 12. Diabetes Mellitus Type 1 Pathogenesis NORMAL ISLET DIABETIC ISLET
- 13. Diabetes Mellitus Type 2 90% of adults with DM Key pathogenic factor is insulin resistance In
- 14. DM pathogenesis Hyperglycemia Low insulin Insulin resistance decrease of glucose consumption by muscles and adipose tissue
- 15. DM pathogenesis decrease of glucose consumption by muscles and adipose tissue Disturbance of energy metabolism Activation
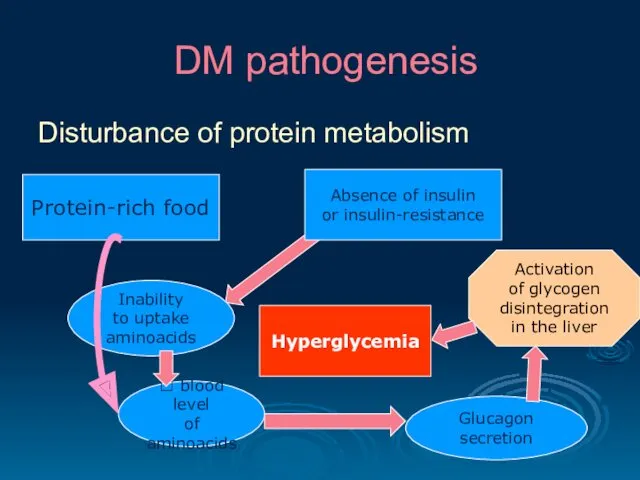
- 16. DM pathogenesis Disturbance of protein metabolism Protein-rich food Inability to uptake aminoacids Absence of insulin or
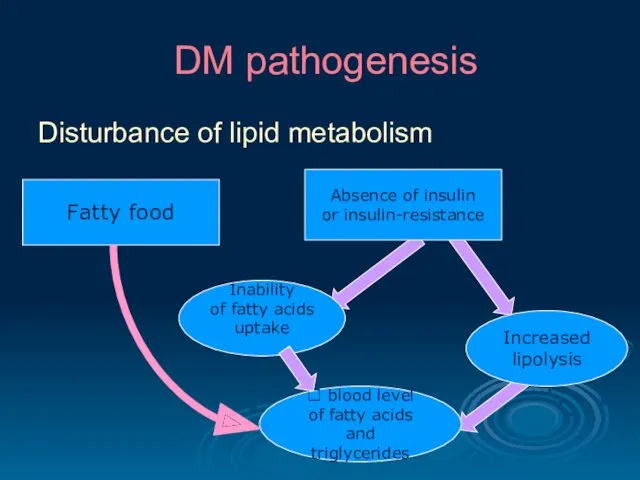
- 17. DM pathogenesis Disturbance of lipid metabolism Fatty food Inability of fatty acids uptake Absence of insulin
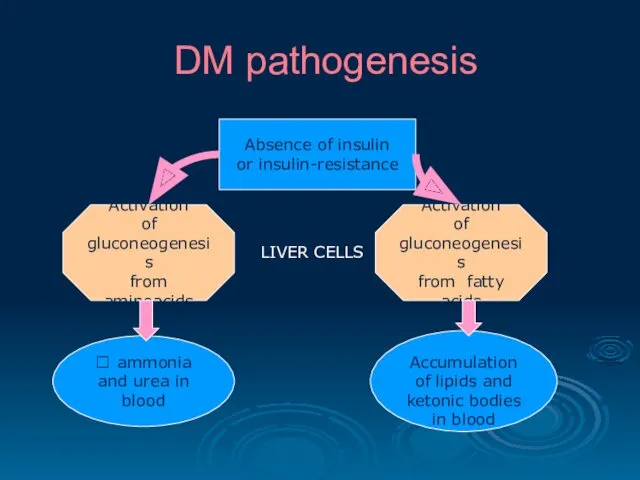
- 18. DM pathogenesis Absence of insulin or insulin-resistance Activation of gluconeogenesis from aminoacids Activation of gluconeogenesis from
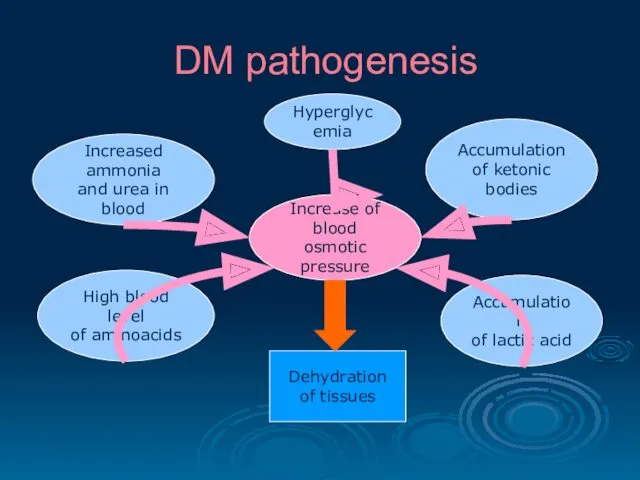
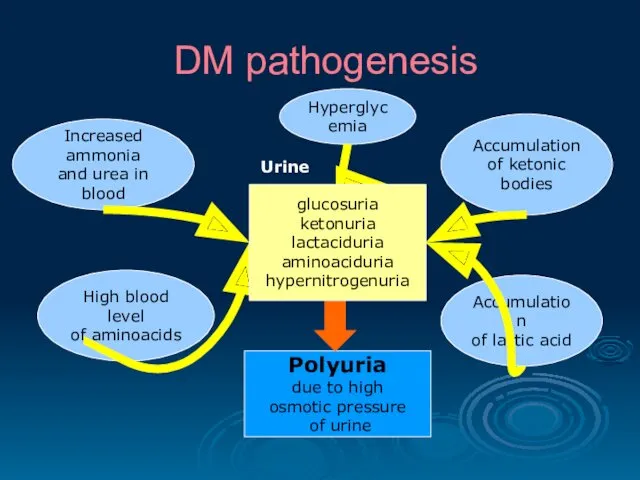
- 19. DM pathogenesis Accumulation of lactic acid High blood level of aminoacids Increased ammonia and urea in
- 20. DM pathogenesis Accumulation of lactic acid High blood level of aminoacids Increased ammonia and urea in
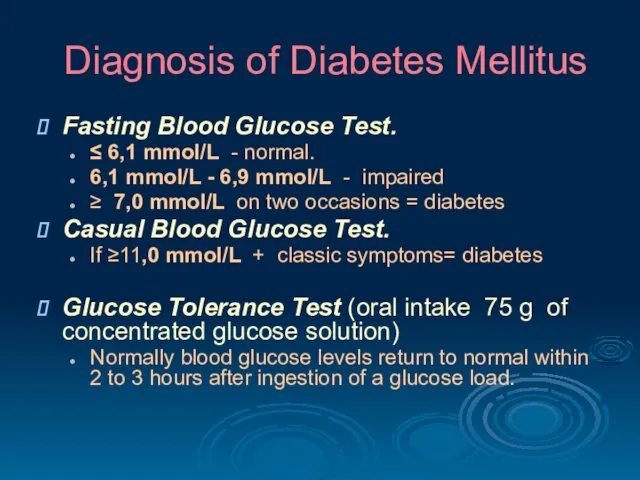
- 21. Diagnosis of Diabetes Mellitus Fasting Blood Glucose Test. ≤ 6,1 mmol/L - normal. 6,1 mmol/L -
- 22. Diagnosis of Diabetes Mellitus Glycated Hemoglobin Testing (hemoglobin A1C) provides an index of blood glucose levels
- 23. Clinical signs of DM hyperglycemia hyperketonemia glucosuria ketonuria polyuria hyperlipidemia polydipsia (thirst) hyperazotemia hyperphagia (hunger) hyperazoturia
- 24. Clinical signs of DM Absence of insulin Prevalence of catabolic processes Excessive hunger (hyperphagia) Usage of
- 25. Choose the characteristic feature of type 1 diabetes mellitus Middle age at onset Associated obesity Low
- 26. A patient with constant thirst and increased urination was done oral glucose tolerance test that proved
- 27. One of the diabetes mellitus clinical symptoms is hyperphagia. It is developed due to… lack of
- 28. Patient with diabetes mellitus has hyperglycemia 19 mmol/ l, which is clinically developed as glucosuria, polyuria,
- 29. Acute complications of DM Diabetic comas hyperglycemic hypoglycemic hyperosmolar hyperlactatacidemic
- 30. Acute complications of DM Hyperglycemic coma expressed hyperglycemia (>20 mmol/l); progressive dehydration of the organism; ketoacidosis
- 31. Acute complications of DM Hypoglycemic coma may develop if the glucose intake does not match the
- 32. Acute complications of DM Hyperosmolar coma high concentration of glucose, Na, Cl, bicarbonates, urea, ammonia in
- 33. Chronic complications of DM Microvascular disturbances Diabetic retinopathy - severe vision loss or blindness. Diabetic neuropathy
- 34. Chronic complications of DM Macrovascular disease Coronary artery disease, leading to myocardial infarction ("heart attack") or
- 35. Chronic complications of DM Diabetic cardiomyopathy results from many factors (atherosclerosis, hypertension, microvascular disease, endothelial and
- 36. Principles of treatment Control of hyperglycemia. Type 1 diabetics require insulin. Type 2 diabetics should be
- 37. Prevention of DM Early type 1 DM in some patients may be prevented by suppression of
- 38. Which coma often occurs in the patients with diabetes mellitus type 1 when diet is not
- 39. Patient R., 46 years old, has diabetic neuropathy. What is the main mechanism in nervous fibers
- 41. Скачать презентацию
General information
First reports – ancient times
‘diabetes’ – excessive urination
‘mellitus’ –honey.
General information
First reports – ancient times
‘diabetes’ – excessive urination
‘mellitus’ –honey.
DM statistics (IDF)
382 millions diabetic patients worldwide (8,3%)
46% undiagnosed (in Sub-Saharan
DM statistics (IDF)
382 millions diabetic patients worldwide (8,3%)
46% undiagnosed (in Sub-Saharan
Insulin effects
Carbohydrate Metabolism
Insulin dependent tissues– muscles, adipose tissue, liver -
Insulin effects
Carbohydrate Metabolism
Insulin dependent tissues– muscles, adipose tissue, liver -
Insulin effects
Carbohydrate Metabolism
Increases glycogen synthesis in the liver.
↓ blood glucose
Insulin effects
Carbohydrate Metabolism
Increases glycogen synthesis in the liver.
↓ blood glucose
Insulin effects
Lipid metabolism
? synthesis of fatty acids in the liver.
?
Insulin effects
Lipid metabolism
? synthesis of fatty acids in the liver.
?
Biological effects of insulin
Very fast effect – ? glucose and ions
Biological effects of insulin
Very fast effect – ? glucose and ions
DIABETES -
is a complex metabolic disorder resulting from
absolute or
DIABETES -
is a complex metabolic disorder resulting from
absolute or
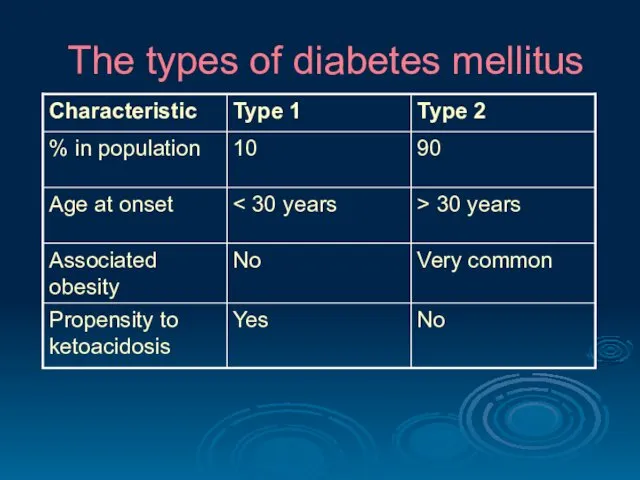
The types of diabetes mellitus
The types of diabetes mellitus
The types of diabetes mellitus
The types of diabetes mellitus
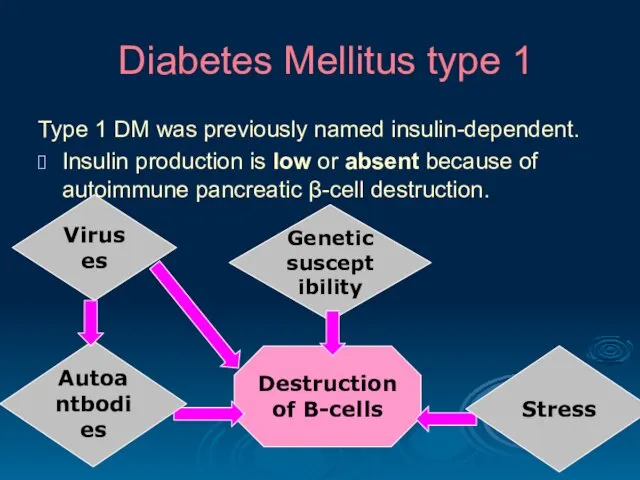
Diabetes Mellitus type 1
Type 1 DM was previously named insulin-dependent.
Insulin production
Diabetes Mellitus type 1
Type 1 DM was previously named insulin-dependent.
Insulin production
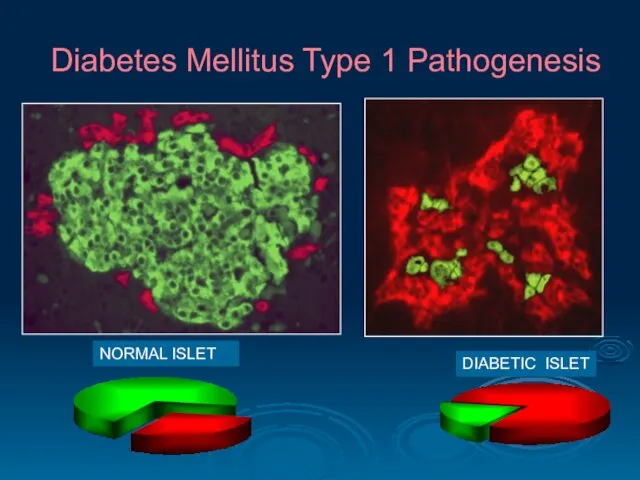
Diabetes Mellitus Type 1 Pathogenesis
NORMAL ISLET
DIABETIC ISLET
Diabetes Mellitus Type 1 Pathogenesis
NORMAL ISLET
DIABETIC ISLET
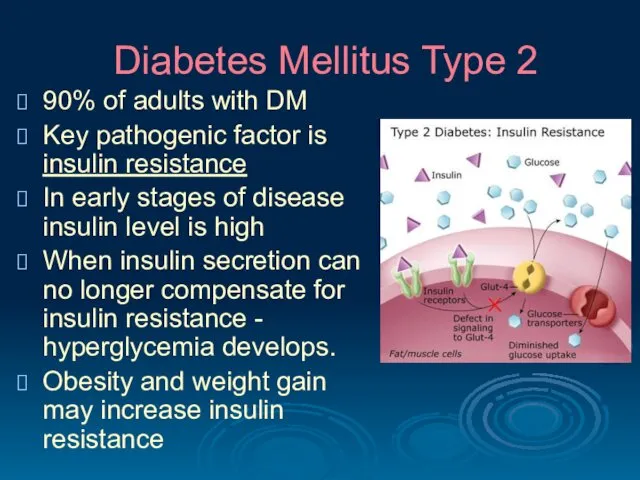
Diabetes Mellitus Type 2
90% of adults with DM
Key pathogenic factor
Diabetes Mellitus Type 2
90% of adults with DM
Key pathogenic factor
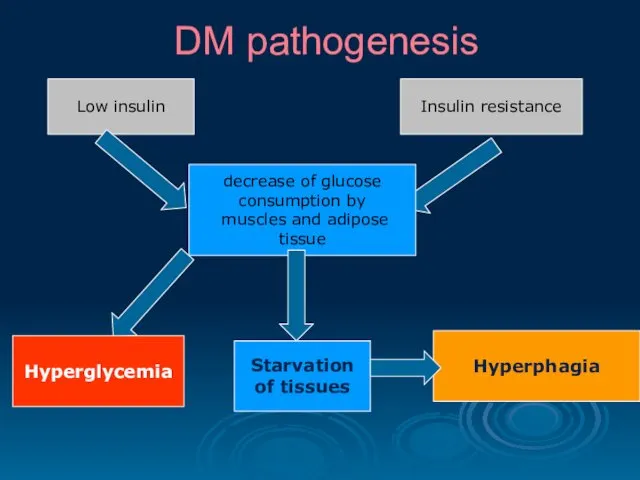
DM pathogenesis
Hyperglycemia
Low insulin
Insulin resistance
decrease of glucose
consumption by
muscles and
DM pathogenesis
Hyperglycemia
Low insulin
Insulin resistance
decrease of glucose
consumption by
muscles and
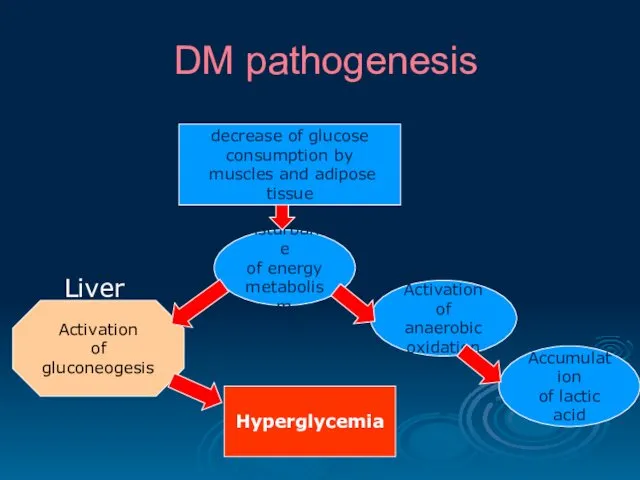
DM pathogenesis
decrease of glucose
consumption by
muscles and adipose tissue
Disturbance
DM pathogenesis
decrease of glucose
consumption by
muscles and adipose tissue
Disturbance
DM pathogenesis
Disturbance of protein metabolism
Protein-rich food
Inability
to uptake
aminoacids
Absence of insulin
DM pathogenesis
Disturbance of protein metabolism
Protein-rich food
Inability
to uptake
aminoacids
Absence of insulin
DM pathogenesis
Disturbance of lipid metabolism
Fatty food
Inability
of fatty acids
uptake
Absence of
DM pathogenesis
Disturbance of lipid metabolism
Fatty food
Inability
of fatty acids
uptake
Absence of
DM pathogenesis
Absence of insulin
or insulin-resistance
Activation
of gluconeogenesis
from aminoacids
Activation
of gluconeogenesis
from
DM pathogenesis
Absence of insulin
or insulin-resistance
Activation
of gluconeogenesis
from aminoacids
Activation
of gluconeogenesis
from
DM pathogenesis
Accumulation
of lactic acid
High blood level
of aminoacids
Increased ammonia
DM pathogenesis
Accumulation
of lactic acid
High blood level
of aminoacids
Increased ammonia
DM pathogenesis
Accumulation
of lactic acid
High blood level
of aminoacids
Increased ammonia
DM pathogenesis
Accumulation
of lactic acid
High blood level
of aminoacids
Increased ammonia
Diagnosis of Diabetes Mellitus
Fasting Blood Glucose Test.
≤ 6,1 mmol/L -
Diagnosis of Diabetes Mellitus
Fasting Blood Glucose Test.
≤ 6,1 mmol/L -
Diagnosis of Diabetes Mellitus
Glycated Hemoglobin Testing (hemoglobin A1C) provides an index
Diagnosis of Diabetes Mellitus
Glycated Hemoglobin Testing (hemoglobin A1C) provides an index
Clinical signs of DM
hyperglycemia hyperketonemia
glucosuria ketonuria
polyuria hyperlipidemia
polydipsia (thirst) hyperazotemia
hyperphagia (hunger)
Clinical signs of DM
hyperglycemia hyperketonemia
glucosuria ketonuria
polyuria hyperlipidemia
polydipsia (thirst) hyperazotemia
hyperphagia (hunger)
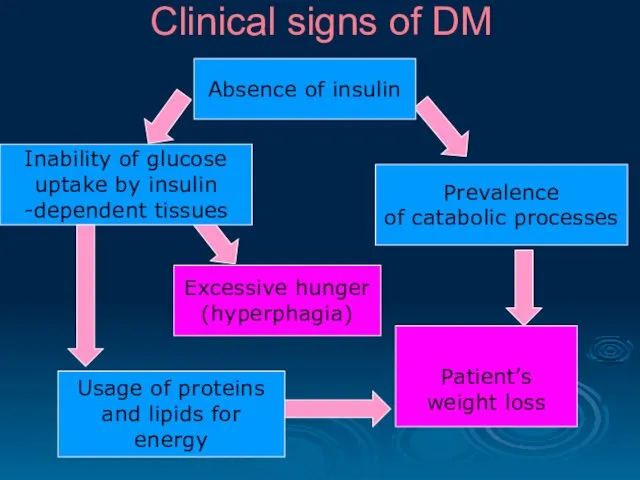
Clinical signs of DM
Absence of insulin
Prevalence
of catabolic processes
Excessive hunger
Clinical signs of DM
Absence of insulin
Prevalence
of catabolic processes
Excessive hunger
Choose the characteristic feature of type 1 diabetes mellitus
Middle age at
Choose the characteristic feature of type 1 diabetes mellitus
Middle age at
A patient with constant thirst and increased urination was done oral
A patient with constant thirst and increased urination was done oral
One of the diabetes mellitus clinical symptoms is hyperphagia. It is
One of the diabetes mellitus clinical symptoms is hyperphagia. It is
Patient with diabetes mellitus has hyperglycemia 19 mmol/ l, which is
Patient with diabetes mellitus has hyperglycemia 19 mmol/ l, which is
Acute complications of DM
Diabetic comas
hyperglycemic
hypoglycemic
hyperosmolar
hyperlactatacidemic
Acute complications of DM
Diabetic comas
hyperglycemic
hypoglycemic
hyperosmolar
hyperlactatacidemic
Acute complications of DM
Hyperglycemic coma
expressed hyperglycemia (>20 mmol/l);
progressive dehydration
Acute complications of DM
Hyperglycemic coma
expressed hyperglycemia (>20 mmol/l);
progressive dehydration
Acute complications of DM
Hypoglycemic coma may develop if the glucose intake
Acute complications of DM
Hypoglycemic coma may develop if the glucose intake
Acute complications of DM
Hyperosmolar coma high concentration of glucose, Na, Cl,
Acute complications of DM
Hyperosmolar coma high concentration of glucose, Na, Cl,
Chronic complications of DM
Microvascular disturbances
Diabetic retinopathy - severe vision loss or
Chronic complications of DM
Microvascular disturbances
Diabetic retinopathy - severe vision loss or
Chronic complications of DM
Macrovascular disease
Coronary artery disease, leading to myocardial infarction
Chronic complications of DM
Macrovascular disease
Coronary artery disease, leading to myocardial infarction
Chronic complications of DM
Diabetic cardiomyopathy results from many factors (atherosclerosis, hypertension,
Chronic complications of DM
Diabetic cardiomyopathy results from many factors (atherosclerosis, hypertension,
Principles of treatment
Control of hyperglycemia.
Type 1 diabetics require insulin.
Principles of treatment
Control of hyperglycemia.
Type 1 diabetics require insulin.
Prevention of DM
Early type 1 DM in some patients may be
Prevention of DM
Early type 1 DM in some patients may be
Which coma often occurs in the patients with diabetes mellitus type
Which coma often occurs in the patients with diabetes mellitus type
Patient R., 46 years old, has diabetic neuropathy. What is the
Patient R., 46 years old, has diabetic neuropathy. What is the
 Жалпы практика дәрігерінің жұмысын ұйымдастыру. Дәрігерлік амбулатория жұмысының менеджмент негіздері
Жалпы практика дәрігерінің жұмысын ұйымдастыру. Дәрігерлік амбулатория жұмысының менеджмент негіздері Жергілікті жансызданудың асқынулары
Жергілікті жансызданудың асқынулары Гигиена аптечных заведений
Гигиена аптечных заведений Женское бесплодие. Современные технологии в диагностике и лечении
Женское бесплодие. Современные технологии в диагностике и лечении :Пародонтоз аурулары. Патогенез. Алдын алу және емдеу
:Пародонтоз аурулары. Патогенез. Алдын алу және емдеу Рентгенологические признаки заболеваний легких: как читать рентгенограммы и КТ органов грудной клетки
Рентгенологические признаки заболеваний легких: как читать рентгенограммы и КТ органов грудной клетки Неспецифические заболевания тонкого и толстого кишечника
Неспецифические заболевания тонкого и толстого кишечника Балалардағы герпестік және цитомегаловирустық
Балалардағы герпестік және цитомегаловирустық Легочная гипертензия
Легочная гипертензия Медицина и первая помощь
Медицина и первая помощь Валидация очистки помещения и оборудования
Валидация очистки помещения и оборудования Дисплазия коленного сустава
Дисплазия коленного сустава Синдромы поражения плевры
Синдромы поражения плевры Лікарські помилки, моральна та правова відповідальність лікаря
Лікарські помилки, моральна та правова відповідальність лікаря Ожоги органа зрения
Ожоги органа зрения ЛП, влияющие на функции органов дыхания
ЛП, влияющие на функции органов дыхания Пневмония. Внебольничные и внутрибольничные пневмонии
Пневмония. Внебольничные и внутрибольничные пневмонии Обеспечение безопасности при неблагоприятной экологической обстановке
Обеспечение безопасности при неблагоприятной экологической обстановке Страховая система здравоохранения США
Страховая система здравоохранения США Нейродиетология тиков и гиперкинезов
Нейродиетология тиков и гиперкинезов Pathophysiology of loco-motor system
Pathophysiology of loco-motor system Гемопоэз. Теория кроветворения
Гемопоэз. Теория кроветворения Кровотечение. Методы остановки кровотечений
Кровотечение. Методы остановки кровотечений Пластические операции в маммологии
Пластические операции в маммологии Ультразвуковое исследование тазобедренного сустава
Ультразвуковое исследование тазобедренного сустава Микробиологическая диагностика спирохетозов
Микробиологическая диагностика спирохетозов Реабилитация пациентов при инфекционных и паразитарных заболеваниях
Реабилитация пациентов при инфекционных и паразитарных заболеваниях Эшерихии. Классификация эшерихий
Эшерихии. Классификация эшерихий