- Diabetic counceling

Содержание
- 2. Diabetes is a chronic, life long disease and could be controlled by insulin replacement therapy for
- 4. Lines of treatment of type Insulin therapy Nutrition Exercise Pychological aspect and health education Monitoring and
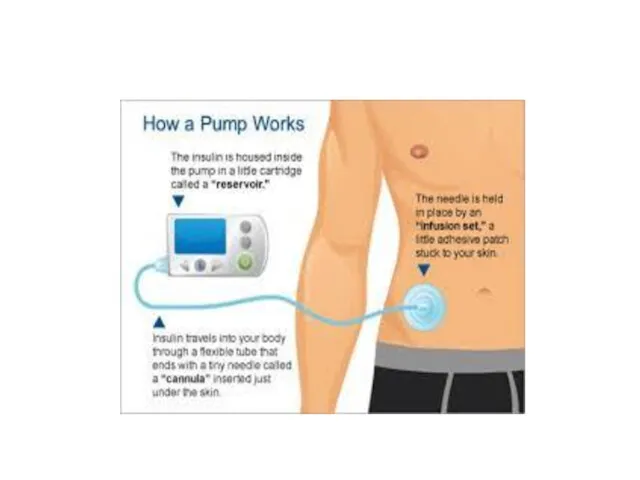
- 5. Insulin therapy Route: insulin is given by SC route
- 7. Injection sites and rotation
- 8. Insulin storage Insulin should be stored in room temperature in winter and in refrigerator in summer
- 9. Insulin regimen Insulin regimens: One of the following regimens be used: Four injections daily The most
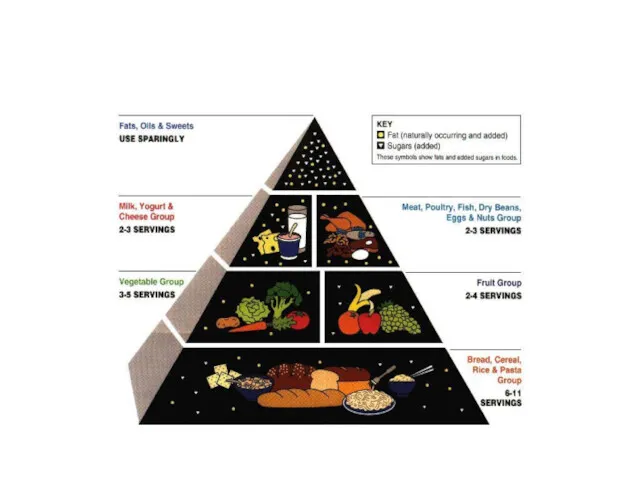
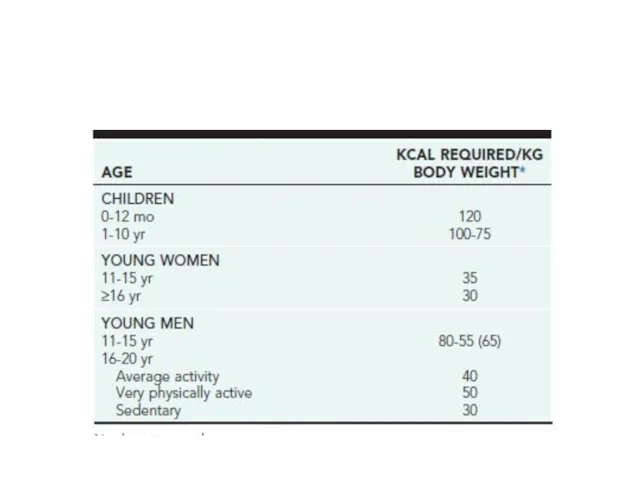
- 10. nutrition There are no special nutritional requirements for the diabetic child other than those for optimal
- 11. The caloric mixture should comprise approximately 55% carbohydrate, 30% fat, and 15% protein. 10% for each
- 12. Fiber: Diets with high fiber content are useful in improving control of blood glucose. Moderate amounts
- 13. Fat: Dietary fats derived from animal sources are, therefore, reduced and replaced by polyunsaturated fats from
- 16. exercise ∙ Exercise should be encouraged and never restricted unless indicated by other health problems. ∙
- 17. monitoring Every day :home glucose monitoring by glucometer4-6 times daily . Parents and patients should be
- 18. Every 3 months: glycosylated hemoglobin provides a useful index of control .its level reflects the blood
- 19. Pychological aspect Sharing responsibilities Camps for diabetic children Balance between love and limits
- 20. Health education In the acute phase, the family must learn the “basics,” which includes monitoring the
- 21. Hypoglycemic reactions Most children with T1DM can expect mild hypoglycemia each week, moderate hypoglycemia a few
- 22. Hypoglycemia can occur at any time of day or night. Early symptoms and signs (mild hypoglycemia)
- 23. glucose should be available at all times and places, including at school and during visits to
- 25. Скачать презентацию
Diabetes is a chronic, life long disease and could be controlled
Diabetes is a chronic, life long disease and could be controlled

Lines of treatment of type
Insulin therapy
Nutrition
Exercise
Pychological aspect and health education
Monitoring
Lines of treatment of type
Insulin therapy
Nutrition
Exercise
Pychological aspect and health education
Monitoring

Insulin therapy
Route: insulin is given by SC route
Insulin therapy
Route: insulin is given by SC route
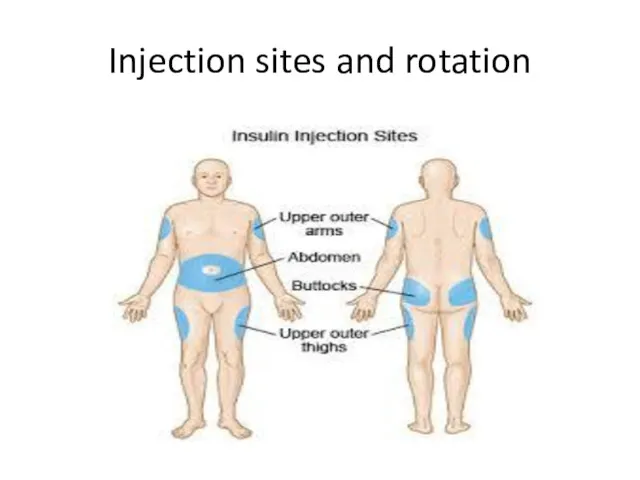
Injection sites and rotation
Injection sites and rotation
Insulin storage
Insulin should be stored in room temperature in winter and
Insulin storage
Insulin should be stored in room temperature in winter and
Insulin regimen
Insulin regimens:
One of the following regimens be used:
Four injections
Insulin regimen
Insulin regimens:
One of the following regimens be used:
Four injections
nutrition
There are no special nutritional requirements for the diabetic child other
nutrition
There are no special nutritional requirements for the diabetic child other
The caloric mixture should comprise approximately 55% carbohydrate,
30% fat, and 15%
30% fat, and 15%
Fiber: Diets with high fiber content are useful in improving control
Fiber: Diets with high fiber content are useful in improving control
Fat:
Dietary fats derived from animal sources
are, therefore, reduced and replaced by
Fat:
Dietary fats derived from animal sources
are, therefore, reduced and replaced by
exercise
∙ Exercise should be encouraged and never restricted unless indicated by
exercise
∙ Exercise should be encouraged and never restricted unless indicated by
monitoring
Every day :home glucose monitoring by glucometer4-6 times daily . Parents
monitoring
Every day :home glucose monitoring by glucometer4-6 times daily . Parents
Every 3 months: glycosylated hemoglobin provides a useful index of control
Every 3 months: glycosylated hemoglobin provides a useful index of control
Pychological aspect
Sharing responsibilities
Camps for diabetic children
Balance between love and limits
Pychological aspect
Sharing responsibilities
Camps for diabetic children
Balance between love and limits
Health education
In the acute phase, the family must learn the “basics,”
Health education
In the acute phase, the family must learn the “basics,”
Hypoglycemic reactions
Most children with T1DM can expect mild hypoglycemia
each week, moderate
Hypoglycemic reactions
Most children with T1DM can expect mild hypoglycemia
each week, moderate
Hypoglycemia can occur at any time of day or night. Early
Hypoglycemia can occur at any time of day or night. Early
 Алкоголизм, наркомания, токсикомания
Алкоголизм, наркомания, токсикомания Сенильді психоздың дамуына әкелетін факторлар. Кәрі жастағы психикалық бұзылыстары бар науқастардың реабилитациясы
Сенильді психоздың дамуына әкелетін факторлар. Кәрі жастағы психикалық бұзылыстары бар науқастардың реабилитациясы Клиническая фармакология антитромботических средств
Клиническая фармакология антитромботических средств Острая печеночная недостаточность
Острая печеночная недостаточность Нормативно-правовая основа деятельности участковой медицинской сестры
Нормативно-правовая основа деятельности участковой медицинской сестры Туляремия у детей
Туляремия у детей Diagnostyka i leczenie chłoniaków złośliwych
Diagnostyka i leczenie chłoniaków złośliwych Организация наблюдения за новорожденными на педиатрическом участке
Организация наблюдения за новорожденными на педиатрическом участке Уход за больными в хирургической клинике
Уход за больными в хирургической клинике Психология, патопсихология и психопатология ощущений и восприятий
Психология, патопсихология и психопатология ощущений и восприятий Вред, причиняемый алкоголем. Тест
Вред, причиняемый алкоголем. Тест Туберкулез бронхов
Туберкулез бронхов Белок. Правильное питание как необходимое условие здоровья и долголетия
Белок. Правильное питание как необходимое условие здоровья и долголетия Танымал қоғам қайраткерлерінің және орыстың профессор-энциклопедисттерінің гигиенаның дамуындағы рөлі
Танымал қоғам қайраткерлерінің және орыстың профессор-энциклопедисттерінің гигиенаның дамуындағы рөлі Психосоматические расстройства
Психосоматические расстройства Корь
Корь Состав и свойства ротовой жидкости, ее роль в процессах созревания эмали, ре- и деминерализации
Состав и свойства ротовой жидкости, ее роль в процессах созревания эмали, ре- и деминерализации Респираторная поддержка при межгоспитальной транспортировке больных с тяжелой сочетанной травмой и нарушением витальных функций
Респираторная поддержка при межгоспитальной транспортировке больных с тяжелой сочетанной травмой и нарушением витальных функций Обструктивный синдром у детей раннего возраста. Лечение
Обструктивный синдром у детей раннего возраста. Лечение Лекарственные средства, регулирующие функции ЦНС Средства для наркоза. Спирт этиловый. Снотворные средства
Лекарственные средства, регулирующие функции ЦНС Средства для наркоза. Спирт этиловый. Снотворные средства Кожа и её производные. Гистология
Кожа и её производные. Гистология Патофизиология пищеварения. Нарушения аппетита.. Язвенная болезнь желудка и ДП
Патофизиология пищеварения. Нарушения аппетита.. Язвенная болезнь желудка и ДП Применение Конусно-лучевой компьютерной томографии(КЛКТ) в амбулаторной стоматологической практике
Применение Конусно-лучевой компьютерной томографии(КЛКТ) в амбулаторной стоматологической практике Основы здорового питания
Основы здорового питания Отоларингология. Неотложные состояния
Отоларингология. Неотложные состояния Методи лікування хворих на туберкульоз. Антимікобактеріальні препарати, механізми їх дії. (Лекція 3)
Методи лікування хворих на туберкульоз. Антимікобактеріальні препарати, механізми їх дії. (Лекція 3) Комы при сахарном диабете
Комы при сахарном диабете Нарушения обмена углеводов
Нарушения обмена углеводов