- Diseases of the veins

Содержание
- 5. Venous return Muscle pump ( peripheral hearts) - ve intra thoracic pressure Arterial pulsation Vise at
- 8. Varicose Veins Dilated, elongated & tortuous vein of the LL problem comes from incompetent calve. 10
- 9. Causes of varicos veins in lower limbs. Secondary Obstruction of venous outflow. Pregnancy. Fibroids Ovarian cysts.
- 10. Varicose Veins (Etiology) Primary Hereditary Occupational Pregnancy obesity Secondary Venous obstruction Venous compression A/V fistula
- 11. Varicose Veins (Etiology) Obstruction of venous outflow. Pregnancy. Fibroids Ovarian cysts. Abdominal lymphadenopathy Pelvic cancer (cervical,
- 12. Varicose Veins Primary V V History: young and middle aged women most commonly affected.1:10 men :women
- 13. Varicose Veins (symptoms) Disfiguring effects of the veins usually principle complaint Pain, dull ache, and heaviness
- 14. Varicose Veins (signs) Dilated elongated tortuous veins Types of varices Tubular with dilated LSV or SSV
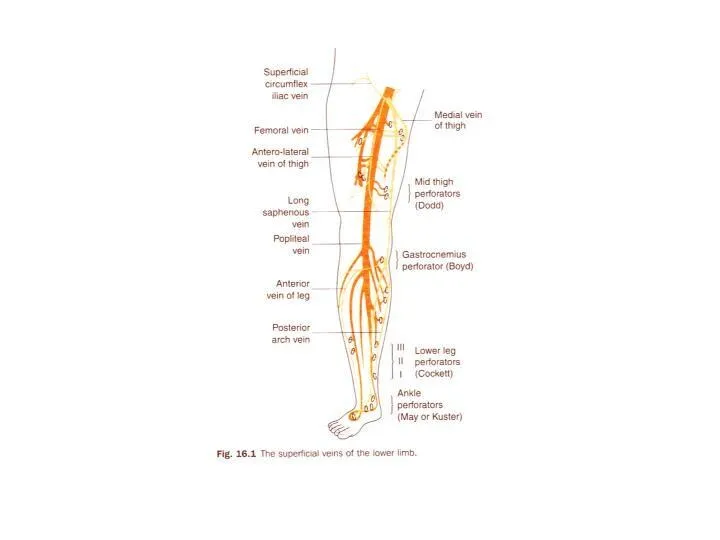
- 15. LSV LSV behind the knee Vein of Leonardo ( post arch vein ) LSV behind the
- 16. Communicator just below knee LSV Vein of Leonardo ( post arch vein ) LSV behind the
- 17. LSV starting at mid thigh Communicator and pass behind the knee Antromedial and calf Group of
- 18. Examination: Inspection: ask patient to stand up. look for abnormal visible subcutaneous veins. if dilated and
- 19. Examination: Palpation: feel along the course of the veins and feel the tension in the veins
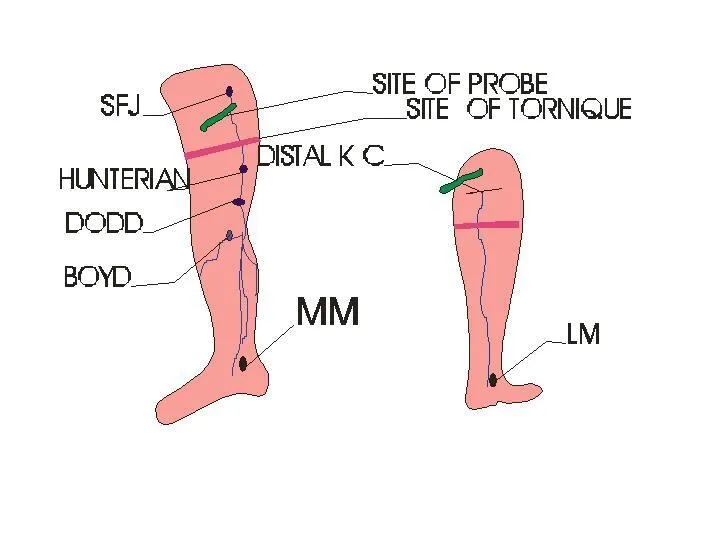
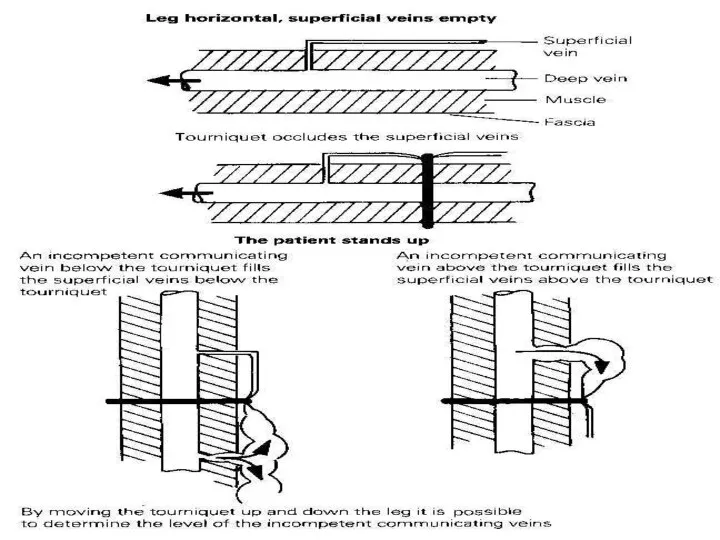
- 20. Examination Tourniquet tests. to check for the site of the incompetent valves. Lie patient flat and
- 22. Examination Percussion: transmission of percussion waves downward implies incompetent valves ( Shwartz test). Place fingers of
- 23. Examination General examination: examine abdomen, incl rectal and vaginal examination. men: palpate testes, testicular tumours can
- 24. Congenital A/V fistula with secondary V V
- 26. Traumatic A/V fistula with secondary V V
- 27. Investigation Routine Lab mainly BSL Hand held Doppler Continuous wave Doppler (CWD) (phono-angiography)
- 28. Investigation Doppler US
- 29. Investigation Duplex US gold standard (B mode ultrasound and a coupled doppler probe) allows direct visualiastion
- 30. Investigation Plethysmography and Venography are obsolete Venous pressure Radio-active isotope scanning Arteriograpgy if A/V fistula
- 31. Complications: Haemorrhage Oedema Skin pigmentation Lipodermatosclerosis Varicose eczema Venous ulceration Thrombophlebitis Atrophie blanche Marjolin ulcer Equinous
- 32. Thrombophelbitis Varicose eczema
- 33. Treatment A. Non- operative management. walking should be encouraged and prolonged sitting and standing should be
- 34. Treatment Compression sclerotherapy. permanent fibrotic occlusion of collapsed veins. patient is recumbent and veins collapsed, a
- 35. Compression sclerotherapy. continuous pressure is maintained for 1-2 weeks with elastic stockings. much less expensive than
- 36. Endo-venous laser Peri-venous LA 810 nm diode Time consuming Less painful
- 37. Radiofrequency ablation Peri-venous LA/ regional anaesthesia Pode expansion in CFV Cook at 85oC Time consuming
- 38. Treatment Surgical therapy. Indications: severe symptoms very large varices attacks of superficial phlebitis haemorrhage from rupturd
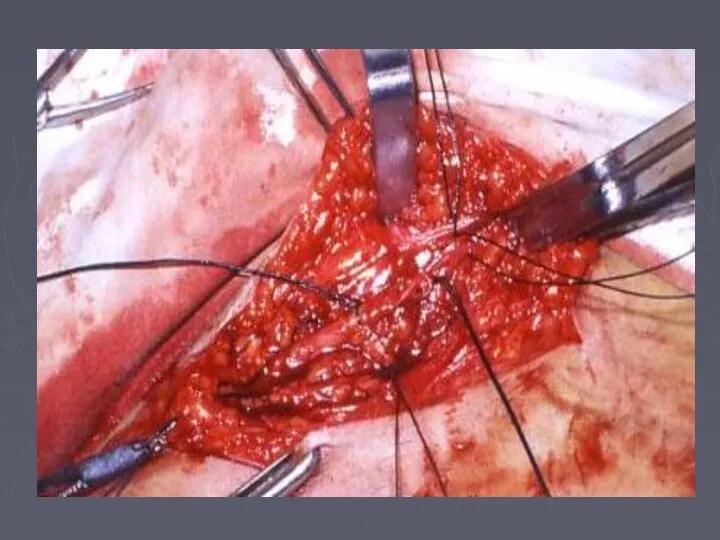
- 39. Treatment Surgical therapy. identify all perforating and superficial veins preoperatively and mark them. results depend on
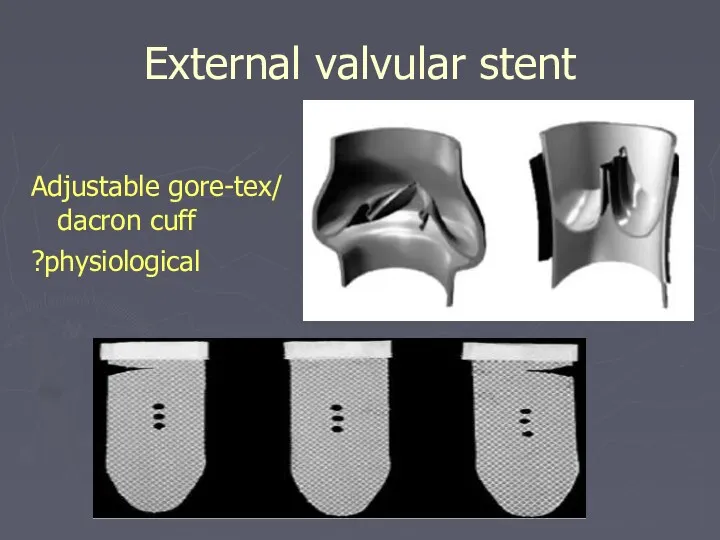
- 43. External valvular stent Adjustable gore-tex/ dacron cuff ?physiological
- 44. Deep Vein Thrombosis Only 1/3 of DVT's cause symptoms and signs. predisposition to thrombosis is predicted
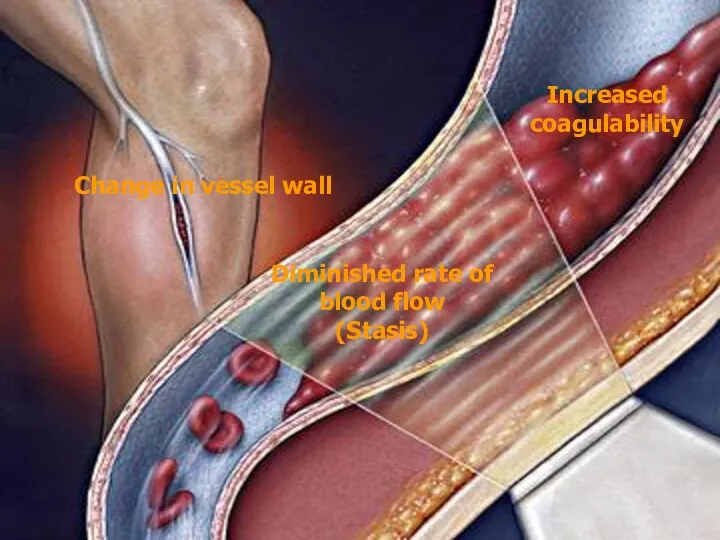
- 45. Increased coagulability Change in vessel wall Diminished rate of blood flow (Stasis)
- 46. Deep Vein Thrombosis History: pain and swelling in the calf or whole leg of sudden onset
- 47. Deep Vein Thrombosis Major criteria History of DVT or family history Malignancy Paralyzed or recent plaster
- 48. Deep Vein Thrombosis Minor criteria Trauma to the leg Hospitalization in last 6 months Unilateral oedema
- 49. Deep Vein Thrombosis High possibility 85 % > 3 major > 2 major > + 2
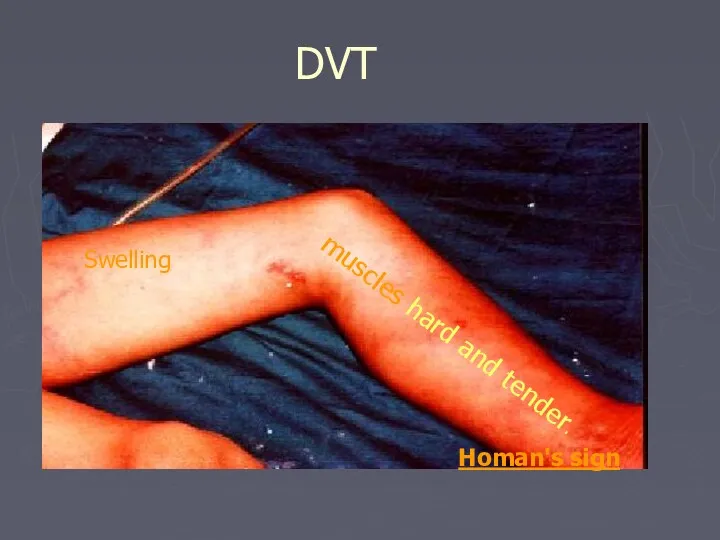
- 50. DVT Swelling muscles hard and tender. Homan's sign
- 51. Phlegmasia cerula Dolens
- 52. Common Iliac occlusion With phlegmasia Cerula dolens
- 53. IVC occlusion
- 54. Prevention of DVT Before operation: Stop pill ( if possible 6 weeks before), grossly overweight patients
- 55. Prevention of DVT Methods of prevention: Mechanical: assisting venous return by; Graduated static compression elastic stockings
- 56. accurate diagnosis using doppler ultrasound (or venography). Anticoagulation (Aim of treatment is to prevent proximal propagation
- 57. Heparin 5000 units IV as loading dose followed by initially 1250 units/hour then adjust according to
- 58. cease heparin when warfarin is established with a therapeutic INR 2 initial Warfarin 10mg orally, once
- 59. Treatment of DVT Thrombectomy; rarely indicated Fibrinolytic treatment: streptokinase, urokinase or combination of streptokinase with tissue
- 60. IVC filter
- 61. Chronic venous insufficiency
- 62. Chronic venous insufficiency Macro- circulation Changes Muscle dysfunction Obstruction Reflux Increase AVP Increase perforator incompetence Primary
- 63. Chronic venous insufficiency Micro- circulation Changes The two most popular current explanations for this process are
- 64. Chronic venous insufficiency Micro- circulation Changes Arterio-venous communications Some suggest the presence arteriovenous shunts further depriving
- 65. Chronic venous insufficiency Oedema Skin pigmentation Lipodermatosclerosis Varicose eczema Venous ulceration Thrombophlebitis Atrophie blanche Marjolin ulcer
- 66. Venous Ulcer The ulcer Gaiter area lower leg (medial lower 1/3) edge sloping and pale purple-blue
- 68. LSV CVI Ankle flare LSV CVI Ankle flare
- 73. DD of leg ulcer Infective Ulcer TB $ Ischemic ulcer Traumatic Malignant Epithelioma Malignant melanoma Trophic
- 74. DD of leg ulcer Traumatic ulcer Ecthyma
- 75. Symptomatic chronic venous insufficiency or Impending ulceration Hand held Doppler examination SVI only Superficial venous surgery
- 76. Symptomatic chronic venous insufficiency or Impending ulceration Compression therapy Functional assessment (venous pressure tracing or photoplethysmography)
- 77. Conservative Treatment Bisgaar method: Elevation, bandaging, exercises and massage. Compression bandaging: multilayer bandaging for several weeks
- 78. Surgical Treatment Ligation and division of incompetent perforating veins to prevent hydrodynamic forces generated in the
- 79. Perforator sub facial ligation
- 80. Endoscopic perforator surgery Active or healed ulcers Contra-indicated in Deep venous occlusion Infected ulcer
- 81. Treatment Deep venous reconstruction Not yet standard treatment Can correct primary deep veins reflux but not
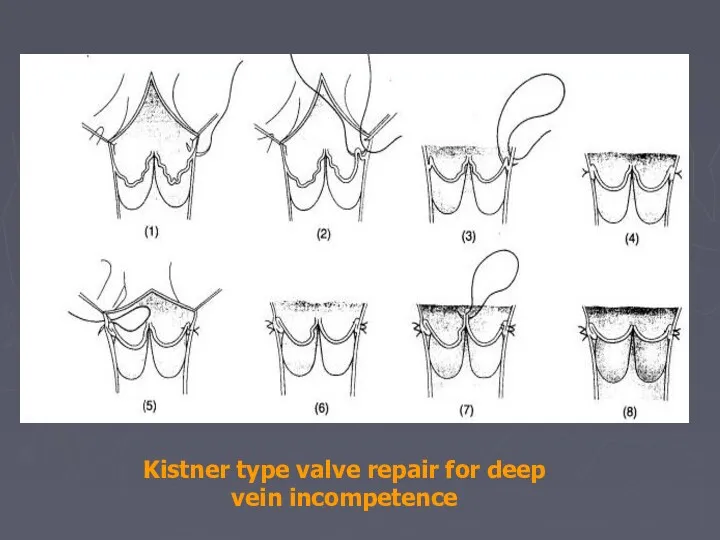
- 82. Kistner type valve repair for deep vein incompetence
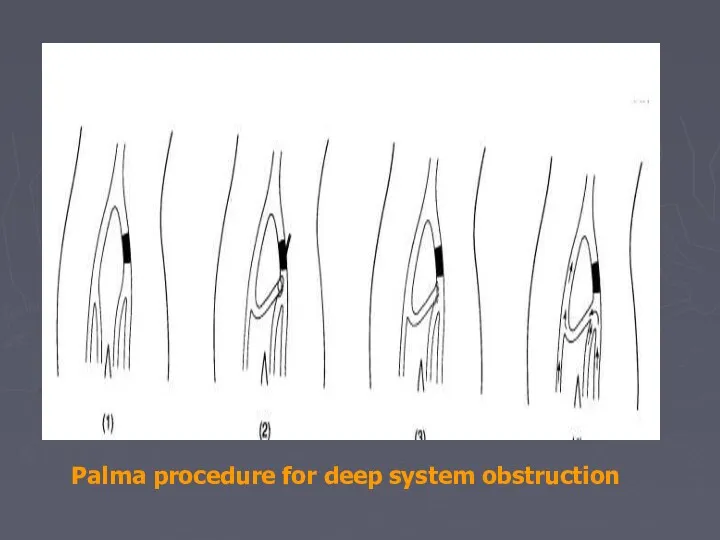
- 83. Palma procedure for deep system obstruction
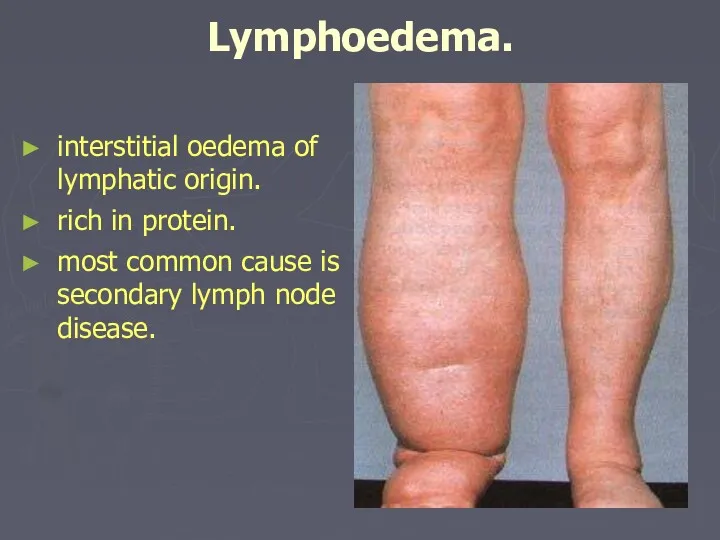
- 84. Lymphoedema. interstitial oedema of lymphatic origin. rich in protein. most common cause is secondary lymph node
- 85. Causes Primary: Congenital or acquired deficiency of the lymphatics ( aplasia or Hypoplasia) Dilation and incompetence
- 86. Causes Secondary: Neoplastic infiltration of lymph nodes. secondary carcinoma Primary reticuloses. Infection Filariasis (parasite Wuchereria bancrofti)
- 87. Clinical Classification Sub clinical with histological abnormalities of LN and lymphatic Grade I Oedema pit on
- 88. Lymphoedema. History. females>males. slowly progressive swelling of the limb or genitelia. lower limb most often affected
- 89. Examination. oedema all oedema pits (clasically sayed to be non-pitting). lymphoedema of the lower limb affect
- 90. Examination. In advanced cases Chronic eczema Fungal skin infection ( Dermatophtosis) Fungal nail infection ( Dermatomycosis)
- 92. Investigation Laboratory Pathology Radiology Contrast lymphangiography Isotope lymphangiography CT scan MRI
- 93. Management: goals of treatment is to control the oedema and to prevent recurrent infection. early treatment
- 94. Management: Non-operative Management: Physical methods reduce lymph formation; elevation of the limb. external compression; custom fitted,
- 95. Management: Surgical Treatment: Only needed in a small number of patients.(16%) Indications for surgery. impaired function.
- 96. Management Bypass Microsurgery: axial pattern and mycocutaneous flaps and lymphatic-lymphatic and lymphatico-venous anastomoses. some procedures try
- 98. Скачать презентацию
Venous return
Muscle pump ( peripheral hearts)
- ve intra thoracic pressure
Arterial pulsation
Vise
Venous return
Muscle pump ( peripheral hearts)
- ve intra thoracic pressure
Arterial pulsation
Vise
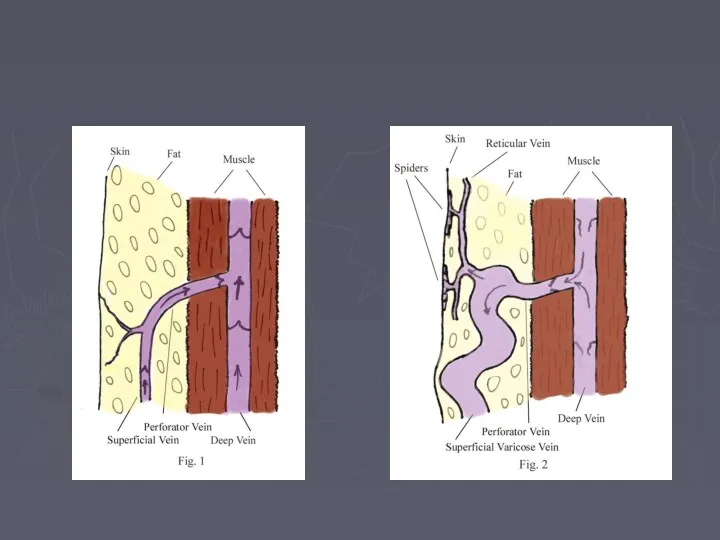
Varicose Veins
Dilated, elongated & tortuous vein of the LL
problem comes from
Varicose Veins
Dilated, elongated & tortuous vein of the LL
problem comes from
Causes of varicos veins in lower limbs.
Secondary
Obstruction of venous outflow.
Causes of varicos veins in lower limbs.
Secondary
Obstruction of venous outflow.
Varicose Veins (Etiology)
Primary
Hereditary
Occupational
Pregnancy
obesity
Secondary
Venous obstruction
Venous compression
A/V fistula
Varicose Veins (Etiology)
Primary
Hereditary
Occupational
Pregnancy
obesity
Secondary
Venous obstruction
Venous compression
A/V fistula
Varicose Veins (Etiology)
Obstruction of venous outflow.
Pregnancy.
Fibroids
Ovarian cysts.
Abdominal
Varicose Veins (Etiology)
Obstruction of venous outflow.
Pregnancy.
Fibroids
Ovarian cysts.
Abdominal
Varicose Veins
Primary V V
History:
young and middle aged women most commonly
Varicose Veins
Primary V V
History:
young and middle aged women most commonly
Varicose Veins (symptoms)
Disfiguring effects of the veins usually principle complaint
Pain,
Varicose Veins (symptoms)
Disfiguring effects of the veins usually principle complaint
Pain,
Varicose Veins (signs)
Dilated elongated tortuous veins
Types of varices
Tubular with dilated LSV
Varicose Veins (signs)
Dilated elongated tortuous veins
Types of varices
Tubular with dilated LSV
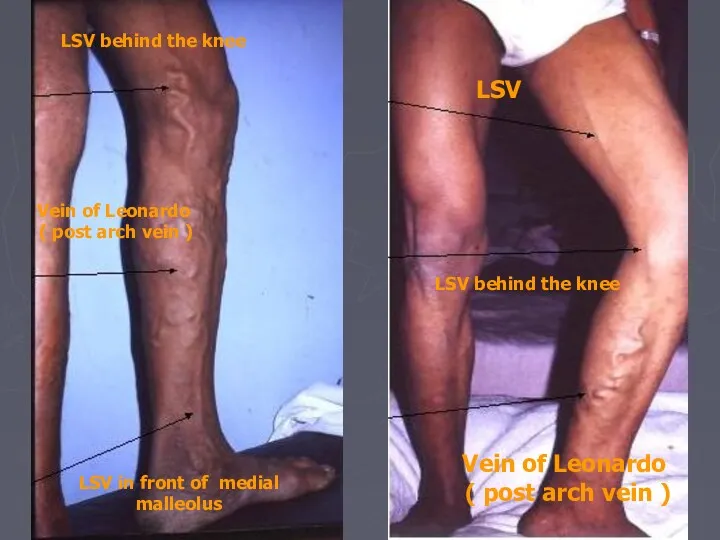
LSV
LSV behind the knee
Vein of Leonardo
( post arch vein )
LSV
LSV
LSV behind the knee
Vein of Leonardo
( post arch vein )
LSV
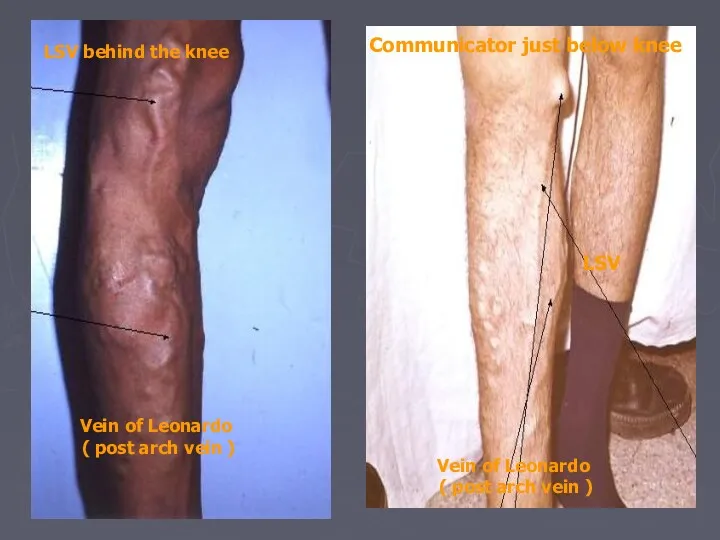
Communicator just below knee
LSV
Vein of Leonardo
( post arch vein )
LSV
Communicator just below knee
LSV
Vein of Leonardo
( post arch vein )
LSV
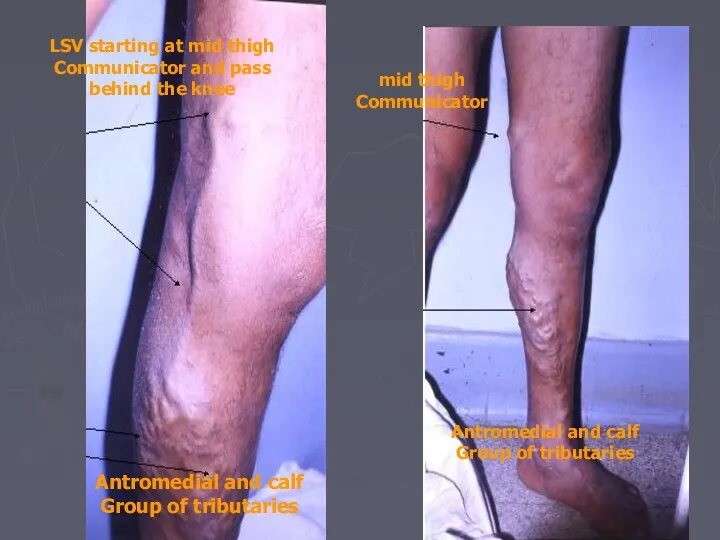
LSV starting at mid thigh
Communicator and pass
behind the knee
Antromedial and calf
Group
LSV starting at mid thigh
Communicator and pass
behind the knee
Antromedial and calf
Group
Examination:
Inspection:
ask patient to stand up.
look for abnormal visible subcutaneous
Examination:
Inspection:
ask patient to stand up.
look for abnormal visible subcutaneous
Examination:
Palpation:
feel along the course of the veins and feel the
Examination:
Palpation:
feel along the course of the veins and feel the
Examination
Tourniquet tests.
to check for the site of the incompetent valves.
Examination
Tourniquet tests.
to check for the site of the incompetent valves.
Examination
Percussion:
transmission of percussion waves downward implies incompetent valves ( Shwartz
Examination
Percussion:
transmission of percussion waves downward implies incompetent valves ( Shwartz
Examination
General examination:
examine abdomen, incl rectal and vaginal examination.
men: palpate
Examination
General examination:
examine abdomen, incl rectal and vaginal examination.
men: palpate
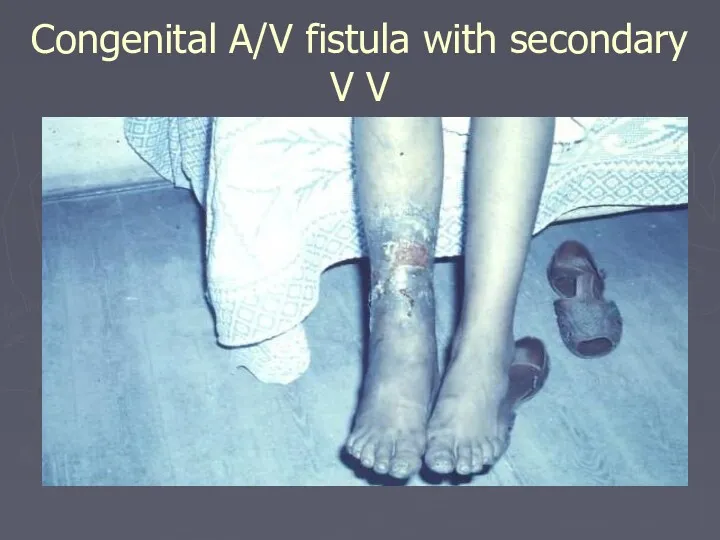
Congenital A/V fistula with secondary V V
Congenital A/V fistula with secondary V V
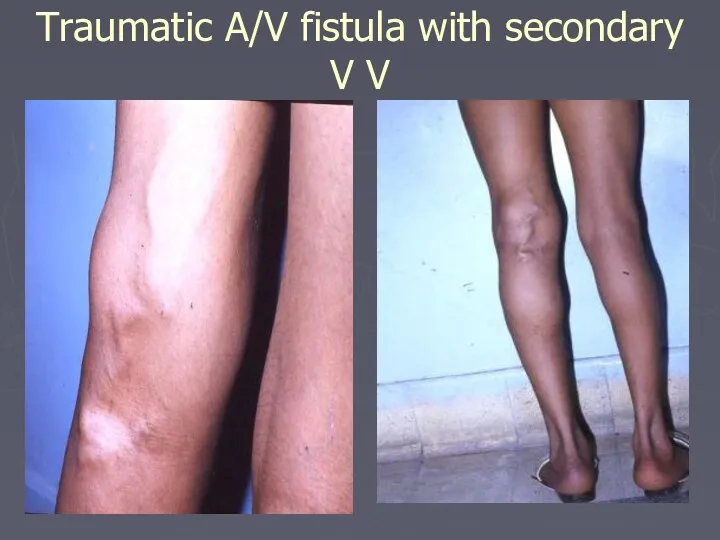
Traumatic A/V fistula with secondary V V
Traumatic A/V fistula with secondary V V
Investigation
Routine Lab mainly BSL
Hand held Doppler
Continuous wave Doppler (CWD)
(phono-angiography)
Investigation
Routine Lab mainly BSL
Hand held Doppler
Continuous wave Doppler (CWD)
(phono-angiography)
Investigation
Doppler US
Investigation
Doppler US
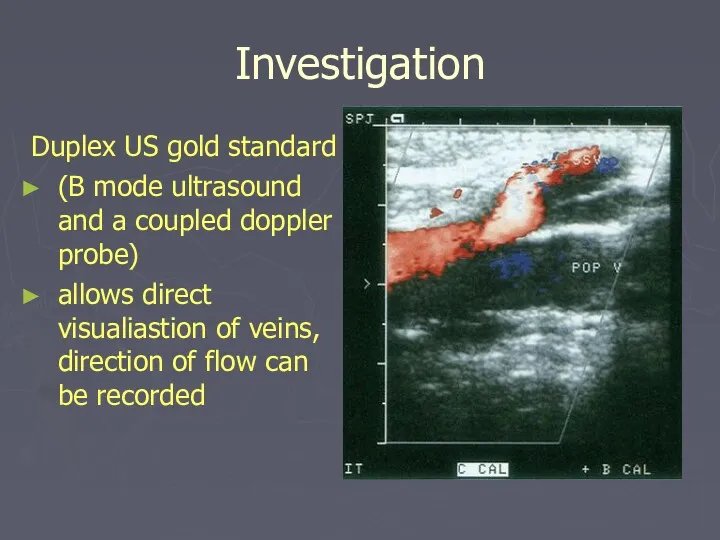
Investigation
Duplex US gold standard
(B mode ultrasound and a coupled doppler
Investigation
Duplex US gold standard
(B mode ultrasound and a coupled doppler
Investigation
Plethysmography and Venography are obsolete
Venous pressure
Radio-active isotope scanning
Arteriograpgy if A/V fistula
Investigation
Plethysmography and Venography are obsolete
Venous pressure
Radio-active isotope scanning
Arteriograpgy if A/V fistula
Complications:
Haemorrhage
Oedema
Skin pigmentation
Lipodermatosclerosis
Varicose eczema
Venous ulceration
Thrombophlebitis
Atrophie blanche
Marjolin ulcer
Equinous deformity
Complications:
Haemorrhage
Oedema
Skin pigmentation
Lipodermatosclerosis
Varicose eczema
Venous ulceration
Thrombophlebitis
Atrophie blanche
Marjolin ulcer
Equinous deformity

Thrombophelbitis
Varicose eczema
Thrombophelbitis
Varicose eczema
Treatment
A. Non- operative management.
walking should be encouraged and prolonged
Treatment
A. Non- operative management.
walking should be encouraged and prolonged
Treatment
Compression sclerotherapy.
permanent fibrotic occlusion of collapsed veins.
patient is
Treatment
Compression sclerotherapy.
permanent fibrotic occlusion of collapsed veins.
patient is
Compression sclerotherapy.
continuous pressure is maintained for 1-2 weeks with elastic
Compression sclerotherapy.
continuous pressure is maintained for 1-2 weeks with elastic
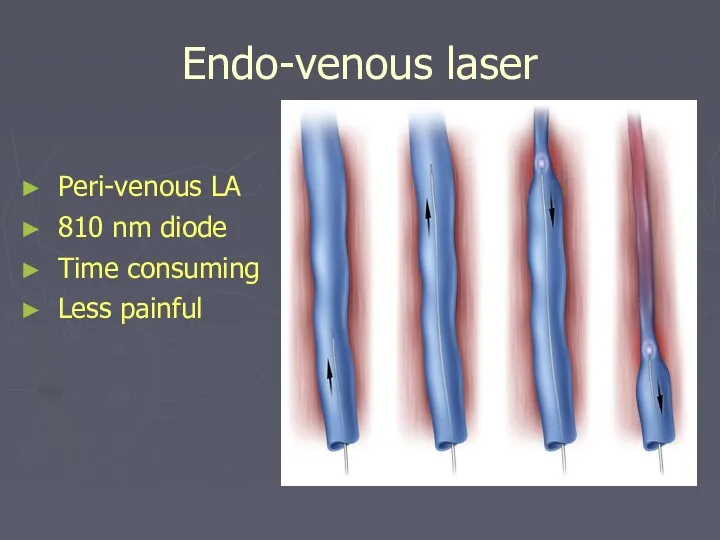
Endo-venous laser
Peri-venous LA
810 nm diode
Time consuming
Less painful
Endo-venous laser
Peri-venous LA
810 nm diode
Time consuming
Less painful
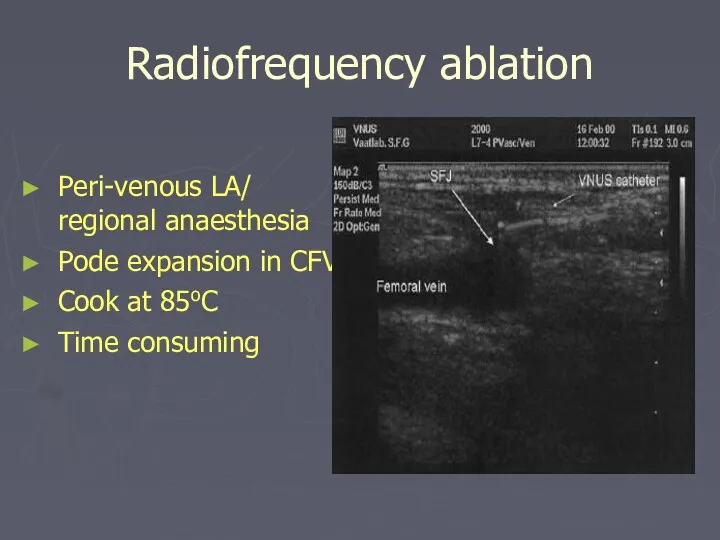
Radiofrequency ablation
Peri-venous LA/ regional anaesthesia
Pode expansion in CFV
Cook at 85oC
Time consuming
Radiofrequency ablation
Peri-venous LA/ regional anaesthesia
Pode expansion in CFV
Cook at 85oC
Time consuming
Treatment
Surgical therapy.
Indications:
severe symptoms
very large varices
attacks of superficial
Treatment
Surgical therapy.
Indications:
severe symptoms
very large varices
attacks of superficial
Treatment
Surgical therapy.
identify all perforating and superficial veins preoperatively and mark
Treatment
Surgical therapy.
identify all perforating and superficial veins preoperatively and mark
External valvular stent
Adjustable gore-tex/ dacron cuff
?physiological
External valvular stent
Adjustable gore-tex/ dacron cuff
?physiological
Deep Vein Thrombosis
Only 1/3 of DVT's cause symptoms and signs.
Deep Vein Thrombosis
Only 1/3 of DVT's cause symptoms and signs.
Increased coagulability
Change in vessel wall
Diminished rate of blood flow (Stasis)
Increased coagulability
Change in vessel wall
Diminished rate of blood flow (Stasis)
Deep Vein Thrombosis
History:
pain and swelling in the calf or whole
Deep Vein Thrombosis
History:
pain and swelling in the calf or whole
Deep Vein Thrombosis
Major criteria
History of DVT or family history
Malignancy
Paralyzed or recent
Deep Vein Thrombosis
Major criteria
History of DVT or family history
Malignancy
Paralyzed or recent
Deep Vein Thrombosis
Minor criteria
Trauma to the leg < 60 day
Hospitalization in
Deep Vein Thrombosis
Minor criteria
Trauma to the leg < 60 day
Hospitalization in
Deep Vein Thrombosis
High possibility 85 %
> 3 major
> 2 major >
Deep Vein Thrombosis
High possibility 85 %
> 3 major
> 2 major >
DVT
Swelling
muscles hard and tender.
Homan's sign
DVT
Swelling
muscles hard and tender.
Homan's sign
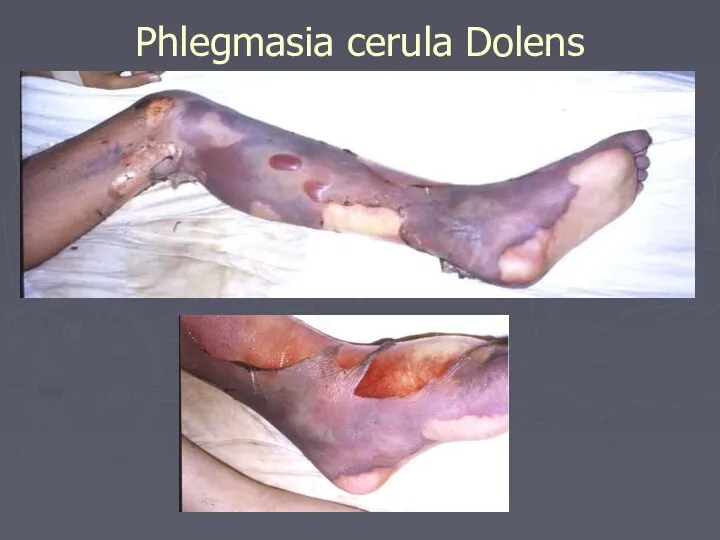
Phlegmasia cerula Dolens
Phlegmasia cerula Dolens
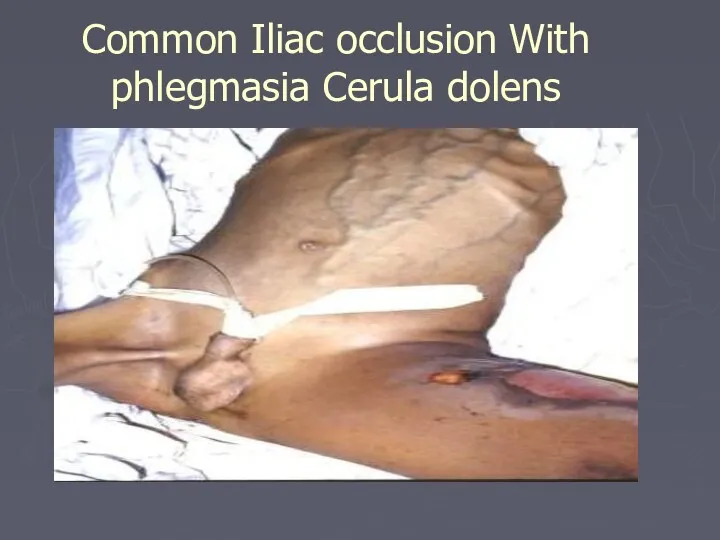
Common Iliac occlusion With phlegmasia Cerula dolens
Common Iliac occlusion With phlegmasia Cerula dolens
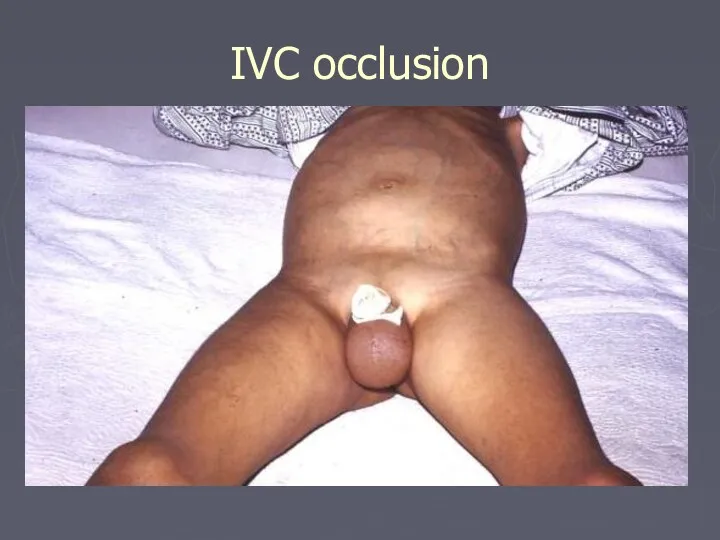
IVC occlusion
IVC occlusion
Prevention of DVT
Before operation: Stop pill ( if possible 6 weeks
Prevention of DVT
Before operation: Stop pill ( if possible 6 weeks
Prevention of DVT
Methods of prevention:
Mechanical: assisting venous return by; Graduated
Prevention of DVT
Methods of prevention:
Mechanical: assisting venous return by; Graduated
accurate diagnosis using doppler ultrasound (or venography).
Anticoagulation
(Aim of treatment
accurate diagnosis using doppler ultrasound (or venography).
Anticoagulation
(Aim of treatment
Heparin
5000 units IV as loading dose
followed by initially 1250
Heparin
5000 units IV as loading dose
followed by initially 1250
cease heparin when warfarin is established with a therapeutic INR 2<
cease heparin when warfarin is established with a therapeutic INR 2<
Treatment of DVT
Thrombectomy; rarely indicated
Fibrinolytic treatment:
streptokinase, urokinase or combination
Treatment of DVT
Thrombectomy; rarely indicated
Fibrinolytic treatment:
streptokinase, urokinase or combination
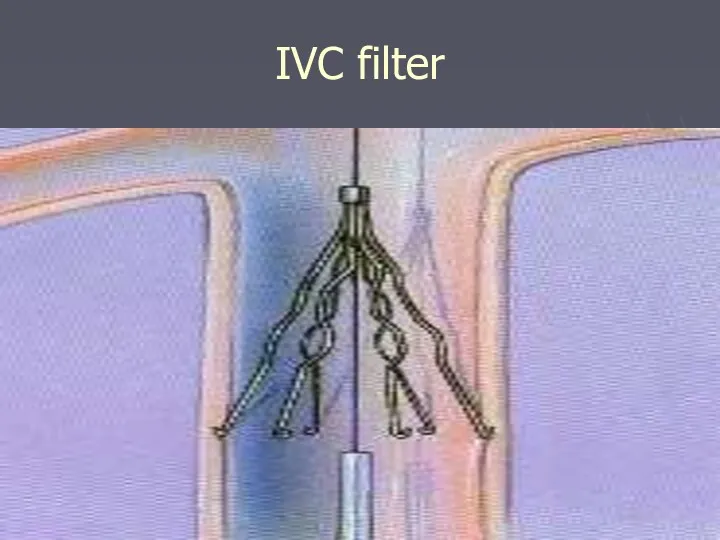
IVC filter
IVC filter
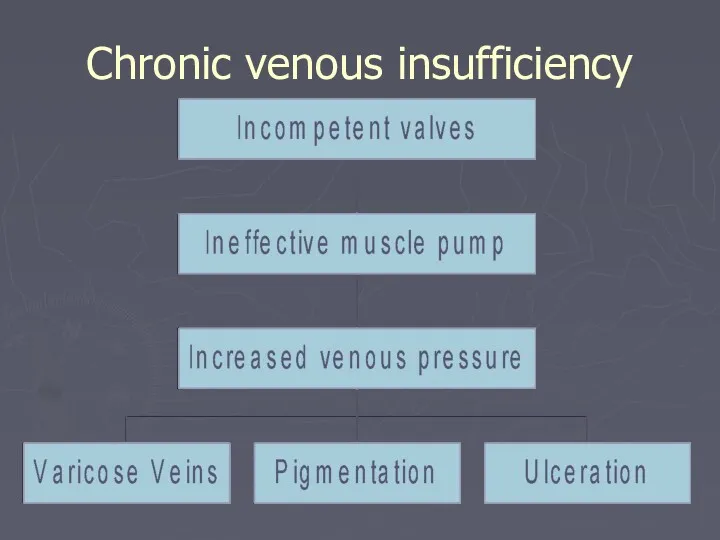
Chronic venous insufficiency
Chronic venous insufficiency
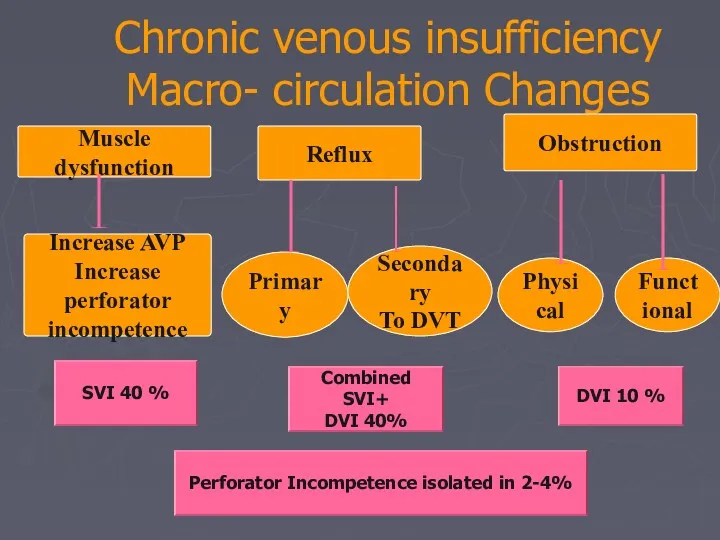
Chronic venous insufficiency
Macro- circulation Changes
Muscle dysfunction
Obstruction
Reflux
Increase AVP
Increase perforator
incompetence
Primary
Physical
Secondary
To DVT
Functional
SVI 40
Chronic venous insufficiency
Macro- circulation Changes
Muscle dysfunction
Obstruction
Reflux
Increase AVP
Increase perforator
incompetence
Primary
Physical
Secondary
To DVT
Functional
SVI 40
Chronic venous insufficiency
Micro- circulation Changes
The two most popular current explanations for
Chronic venous insufficiency
Micro- circulation Changes
The two most popular current explanations for
Chronic venous insufficiency
Micro- circulation Changes
Arterio-venous communications
Some suggest the presence arteriovenous
Chronic venous insufficiency
Micro- circulation Changes
Arterio-venous communications
Some suggest the presence arteriovenous
Chronic venous insufficiency
Oedema
Skin pigmentation
Lipodermatosclerosis
Varicose eczema
Venous ulceration
Thrombophlebitis
Atrophie blanche
Marjolin ulcer
Equinous deformity
Chronic venous insufficiency
Oedema
Skin pigmentation
Lipodermatosclerosis
Varicose eczema
Venous ulceration
Thrombophlebitis
Atrophie blanche
Marjolin ulcer
Equinous deformity
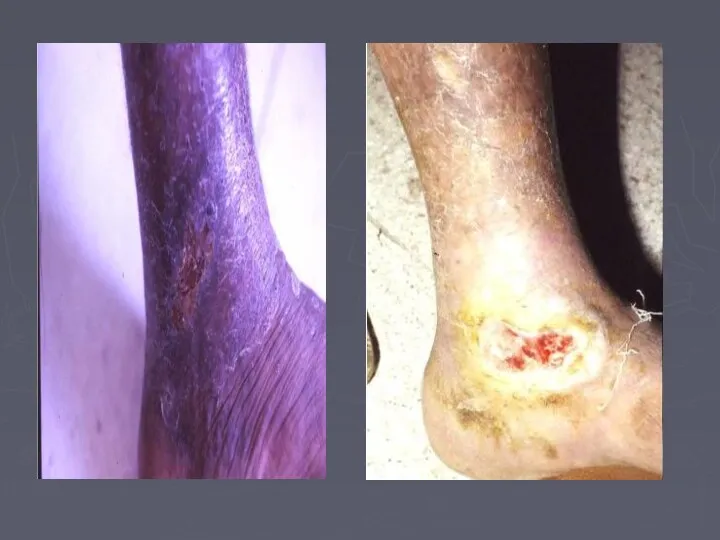
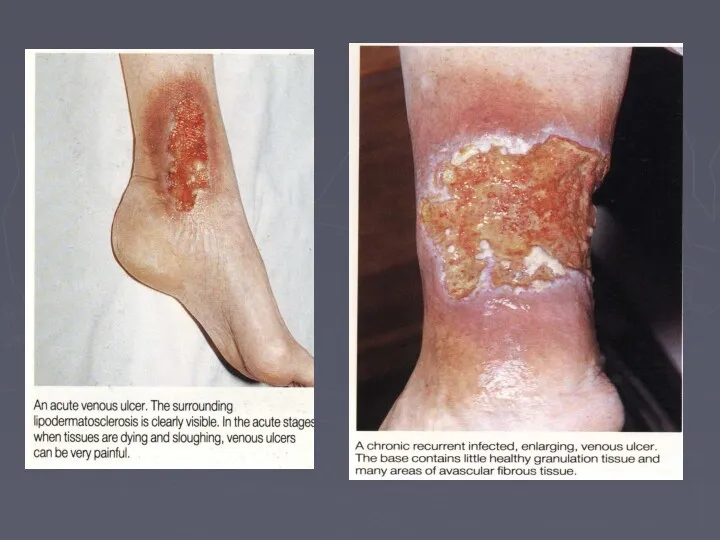
Venous Ulcer
The ulcer
Gaiter area lower leg (medial lower 1/3)
Venous Ulcer
The ulcer
Gaiter area lower leg (medial lower 1/3)


LSV
CVI
Ankle flare
LSV
CVI
Ankle flare
LSV
CVI
Ankle flare
LSV
CVI
Ankle flare


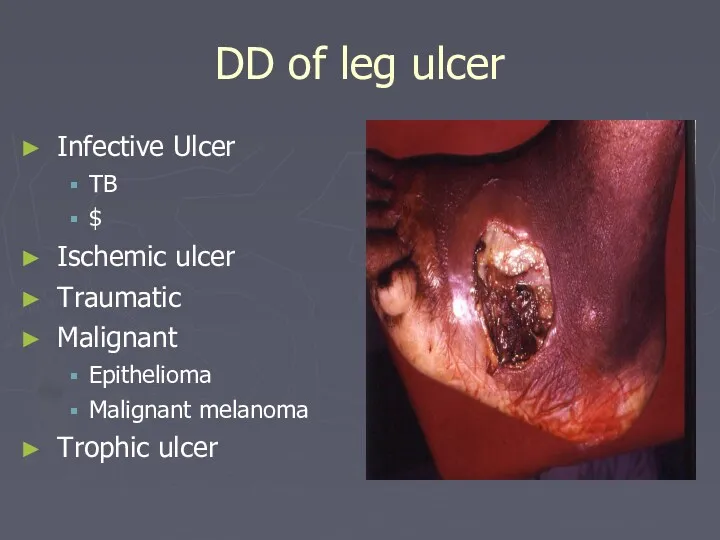
DD of leg ulcer
Infective Ulcer
TB
$
Ischemic ulcer
Traumatic
Malignant
Epithelioma
Malignant melanoma
Trophic ulcer
DD of leg ulcer
Infective Ulcer
TB
$
Ischemic ulcer
Traumatic
Malignant
Epithelioma
Malignant melanoma
Trophic ulcer
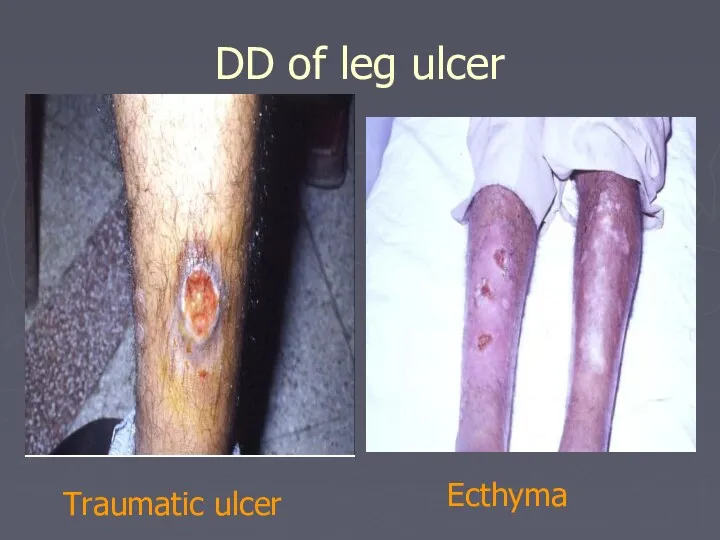
DD of leg ulcer
Traumatic ulcer
Ecthyma
DD of leg ulcer
Traumatic ulcer
Ecthyma
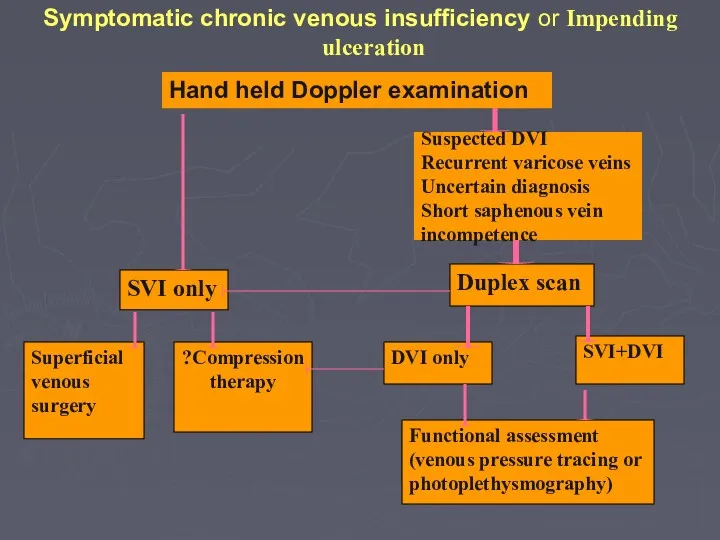
Symptomatic chronic venous insufficiency or Impending ulceration
Hand held Doppler examination
SVI
Symptomatic chronic venous insufficiency or Impending ulceration
Hand held Doppler examination
SVI
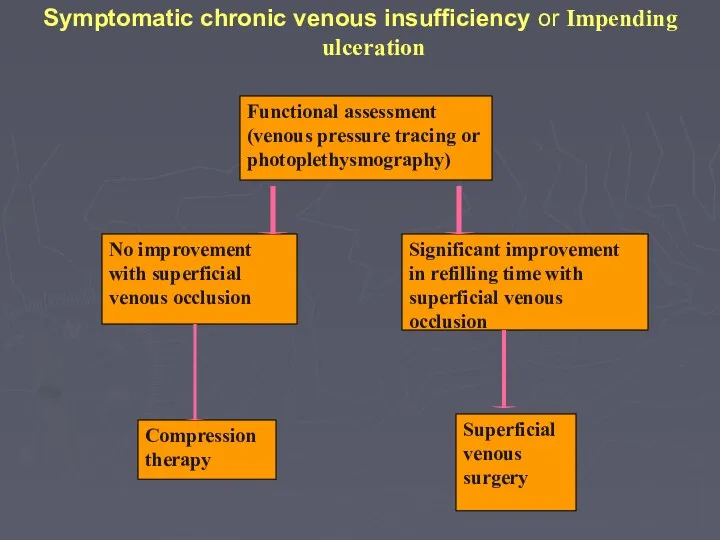
Symptomatic chronic venous insufficiency or Impending ulceration
Compression therapy
Functional assessment
(venous pressure
Symptomatic chronic venous insufficiency or Impending ulceration
Compression therapy
Functional assessment
(venous pressure

Conservative Treatment
Bisgaar method: Elevation, bandaging, exercises and massage.
Compression bandaging:
multilayer
Conservative Treatment
Bisgaar method: Elevation, bandaging, exercises and massage.
Compression bandaging:
multilayer
Surgical Treatment
Ligation and division of incompetent perforating veins
to prevent hydrodynamic
Surgical Treatment
Ligation and division of incompetent perforating veins
to prevent hydrodynamic

Perforator sub facial ligation
Perforator sub facial ligation
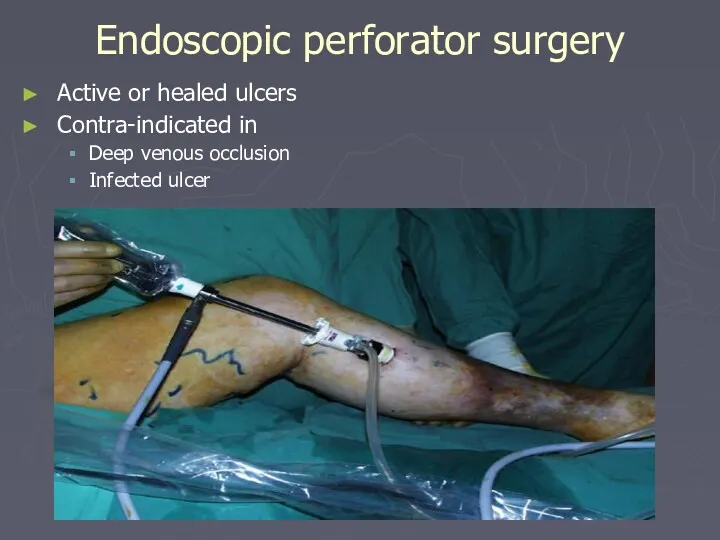
Endoscopic perforator surgery
Active or healed ulcers
Contra-indicated in
Deep venous occlusion
Infected ulcer
Endoscopic perforator surgery
Active or healed ulcers
Contra-indicated in
Deep venous occlusion
Infected ulcer
Treatment
Deep venous reconstruction
Not yet standard treatment
Can correct primary deep veins reflux
Treatment
Deep venous reconstruction
Not yet standard treatment
Can correct primary deep veins reflux
Kistner type valve repair for deep vein incompetence
Kistner type valve repair for deep vein incompetence
Palma procedure for deep system obstruction
Palma procedure for deep system obstruction
Lymphoedema.
interstitial oedema of lymphatic origin.
rich in protein.
most common cause
Lymphoedema.
interstitial oedema of lymphatic origin.
rich in protein.
most common cause
Causes
Primary:
Congenital or acquired deficiency of the lymphatics ( aplasia or
Causes
Primary:
Congenital or acquired deficiency of the lymphatics ( aplasia or
Causes
Secondary:
Neoplastic infiltration of lymph nodes.
secondary carcinoma
Primary reticuloses.
Infection
Causes
Secondary:
Neoplastic infiltration of lymph nodes.
secondary carcinoma
Primary reticuloses.
Infection
Clinical Classification
Sub clinical with histological abnormalities of LN and lymphatic
Grade I
Oedema
Clinical Classification
Sub clinical with histological abnormalities of LN and lymphatic
Grade I
Oedema
Lymphoedema.
History.
females>males.
slowly progressive swelling of the limb or genitelia.
lower
Lymphoedema.
History.
females>males.
slowly progressive swelling of the limb or genitelia.
lower
Examination.
oedema
all oedema pits (clasically sayed to be non-pitting).
lymphoedema of
Examination.
oedema
all oedema pits (clasically sayed to be non-pitting).
lymphoedema of
Examination.
In advanced cases
Chronic eczema
Fungal skin infection ( Dermatophtosis)
Fungal nail infection
Examination.
In advanced cases
Chronic eczema
Fungal skin infection ( Dermatophtosis)
Fungal nail infection

Investigation
Laboratory
Pathology
Radiology
Contrast lymphangiography
Isotope lymphangiography
CT scan
MRI
Investigation
Laboratory
Pathology
Radiology
Contrast lymphangiography
Isotope lymphangiography
CT scan
MRI
Management:
goals of treatment is to control the oedema and to
Management:
goals of treatment is to control the oedema and to
Management:
Non-operative Management:
Physical methods
reduce lymph formation; elevation of the limb.
Management:
Non-operative Management:
Physical methods
reduce lymph formation; elevation of the limb.
Management:
Surgical Treatment:
Only needed in a small number of patients.(16%)
Indications
Management:
Surgical Treatment:
Only needed in a small number of patients.(16%)
Indications
Management
Bypass
Microsurgery: axial pattern and mycocutaneous flaps and lymphatic-lymphatic and lymphatico-venous anastomoses.
Management
Bypass
Microsurgery: axial pattern and mycocutaneous flaps and lymphatic-lymphatic and lymphatico-venous anastomoses.
 Тыныс алудың маңызы. Тыныс алу мүшелері көмей бронхылар кеңірдек
Тыныс алудың маңызы. Тыныс алу мүшелері көмей бронхылар кеңірдек Металды қалыпталған сауытты дайындауда қолданылатын болат маркасы
Металды қалыпталған сауытты дайындауда қолданылатын болат маркасы Средства, влияющие на Н-холинорецепторы. Н-холиномиметики. Ганглиоблокаторы. Миорелаксанты периферического действия (Лекция 5)
Средства, влияющие на Н-холинорецепторы. Н-холиномиметики. Ганглиоблокаторы. Миорелаксанты периферического действия (Лекция 5) Особенности фармакокинетики и фармакотерапии в неонатальном периоде
Особенности фармакокинетики и фармакотерапии в неонатальном периоде Острые промиелоцитарные лейкозы
Острые промиелоцитарные лейкозы Журектiн аускультациясы патологияда
Журектiн аускультациясы патологияда Промывание желудка
Промывание желудка Осложнения желудочно-кишечного тракта внутриутробного развития
Осложнения желудочно-кишечного тракта внутриутробного развития Продуктивное воспаление
Продуктивное воспаление 05. медичне страхування
05. медичне страхування Рестриктивные кардиомиопатии. Формы РКМП
Рестриктивные кардиомиопатии. Формы РКМП Опухоли слюнных желез
Опухоли слюнных желез Изосерологическая несовместимость крови матери и плода
Изосерологическая несовместимость крови матери и плода Болезнь Лайма
Болезнь Лайма Рак яичников
Рак яичников Введение в доказательную медицину
Введение в доказательную медицину Вплив алкоголю на дітей та підлітків
Вплив алкоголю на дітей та підлітків Дерматомиозит
Дерматомиозит Кавказские Минеральные Воды
Кавказские Минеральные Воды Профессиональная гигиена полости рта
Профессиональная гигиена полости рта Т-20С.31 янв
Т-20С.31 янв Дифференциально-диагностический поиск у пациентов с гипогликемическим синдромом
Дифференциально-диагностический поиск у пациентов с гипогликемическим синдромом Сердце, аорта, кровь, вены, капилляры
Сердце, аорта, кровь, вены, капилляры Ларингит
Ларингит Проблемы нормативного обеспечения в сфере информатизации здравоохранения
Проблемы нормативного обеспечения в сфере информатизации здравоохранения Қан айналымды зерттеу әдістері. Интегралдық және регионарлық реография. Реография
Қан айналымды зерттеу әдістері. Интегралдық және регионарлық реография. Реография Анемия у детей
Анемия у детей Клиническая характеристика больных и оказание неотложной помощи при почечной колике
Клиническая характеристика больных и оказание неотложной помощи при почечной колике