- Lasik

Содержание
- 2. LASIK Indications Stable refraction (no change over a period of 2 years) Age ≥21 years Adequate
- 3. excimer laser ablation is carried out on the corneal stroma. usually takes less than 90 seconds.
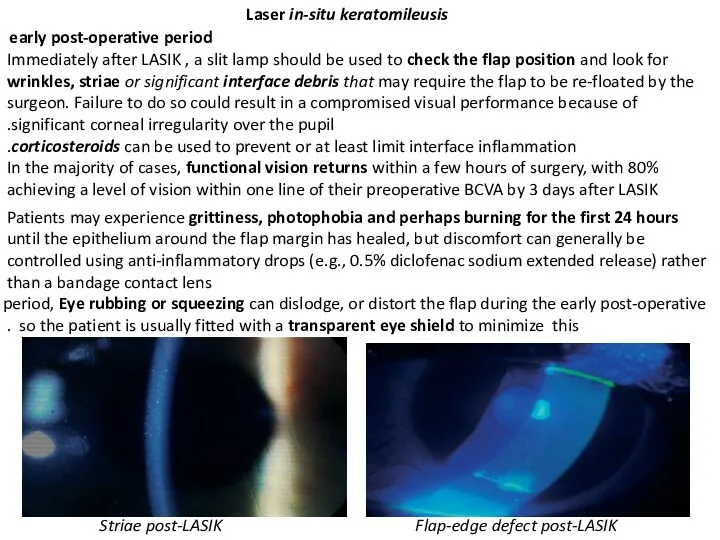
- 4. Laser in-situ keratomileusis early post-operative period Immediately after LASIK , a slit lamp should be used
- 5. The epithelium should fully cover the flap margin by 1 week post-LASIK. Epithelial defects should be
- 6. At 6 months and beyond 90–100% of eyes achieve±1.00D of emmetropia at 6 months post-LASIK for
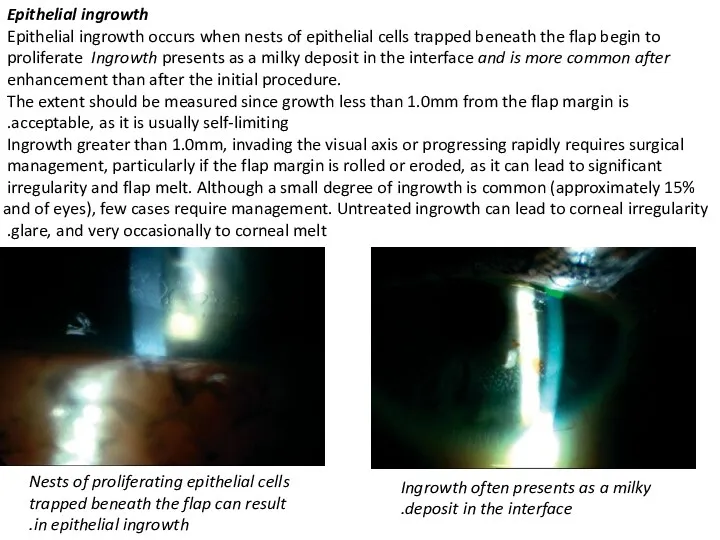
- 7. Epithelial ingrowth Epithelial ingrowth occurs when nests of epithelial cells trapped beneath the flap begin to
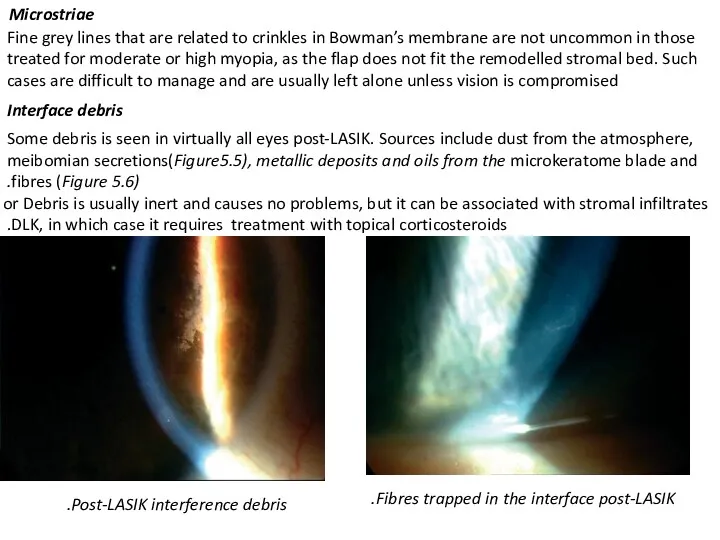
- 8. Fine grey lines that are related to crinkles in Bowman’s membrane are not uncommon in those
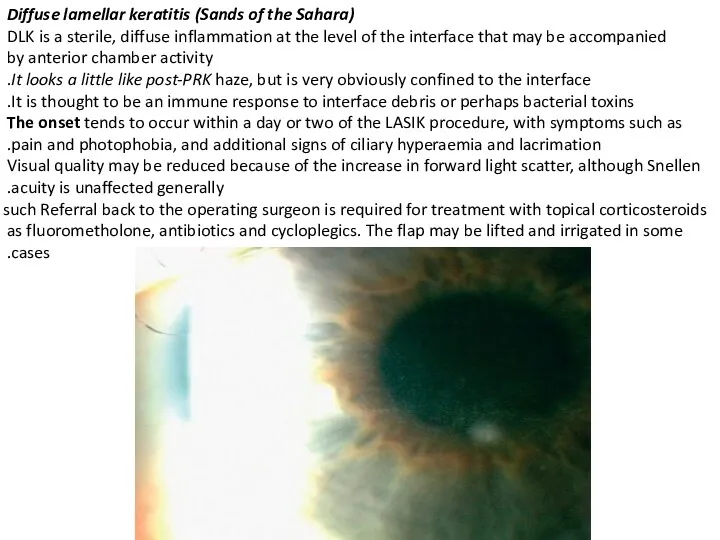
- 9. Diffuse lamellar keratitis (Sands of the Sahara) DLK is a sterile, diffuse inflammation at the level
- 10. A number of systems are used to grade DLK, including one that divides cases into one
- 11. Corneal integrity healing does not appear to lead to the growth of collagen fibres between the
- 12. A recent study of 2873 eyes reported ectasia in 0.66%. The authors noted that ectasia did
- 13. Undercorrection Residual myopia is usually the result of an inaccurate pre-operative refraction or an insufficient period
- 14. Intraocular pressure elevation If corticosteroids are used to treat the intense haze of DLK, for example,
- 15. Visual outcome Unaided vision PRK For low and medium degrees of myopia ( LASIK For eyes
- 16. Particular topographical features that may signal problems include central islands, decentred ablations and irregularities. A central
- 38. Скачать презентацию
LASIK
Indications
Stable refraction (no change over a period of 2 years)
Age
LASIK
Indications
Stable refraction (no change over a period of 2 years)
Age
excimer laser ablation is carried out on the corneal stroma. usually
excimer laser ablation is carried out on the corneal stroma. usually
Laser in-situ keratomileusis
early post-operative period
Immediately after LASIK , a slit lamp
Laser in-situ keratomileusis
early post-operative period
Immediately after LASIK , a slit lamp
The epithelium should fully cover the flap margin by 1
The epithelium should fully cover the flap margin by 1
At 6 months and beyond
90–100% of eyes achieve±1.00D of emmetropia
At 6 months and beyond
90–100% of eyes achieve±1.00D of emmetropia
Epithelial ingrowth
Epithelial ingrowth occurs when nests of epithelial cells trapped beneath
Epithelial ingrowth
Epithelial ingrowth occurs when nests of epithelial cells trapped beneath
Fine grey lines that are related to crinkles in Bowman’s
Fine grey lines that are related to crinkles in Bowman’s
Diffuse lamellar keratitis (Sands of the Sahara)
DLK is a sterile, diffuse
Diffuse lamellar keratitis (Sands of the Sahara)
DLK is a sterile, diffuse
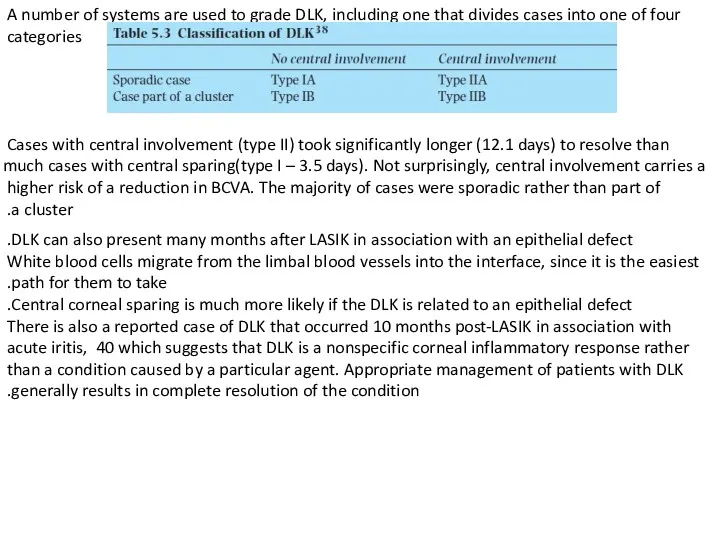
A number of systems are used to grade DLK, including one
A number of systems are used to grade DLK, including one
Corneal integrity
healing does not appear to lead to the growth
Corneal integrity
healing does not appear to lead to the growth
A recent study of 2873 eyes reported ectasia in 0.66%.
The
A recent study of 2873 eyes reported ectasia in 0.66%.
The
Undercorrection
Residual myopia is usually the result of an inaccurate pre-operative refraction
Residual myopia is usually the result of an inaccurate pre-operative refraction
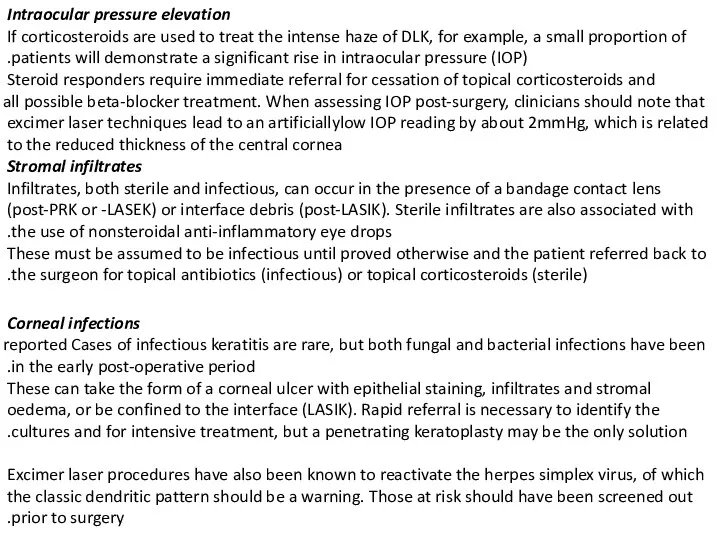
Intraocular pressure elevation
If corticosteroids are used to treat the intense haze
Intraocular pressure elevation
If corticosteroids are used to treat the intense haze
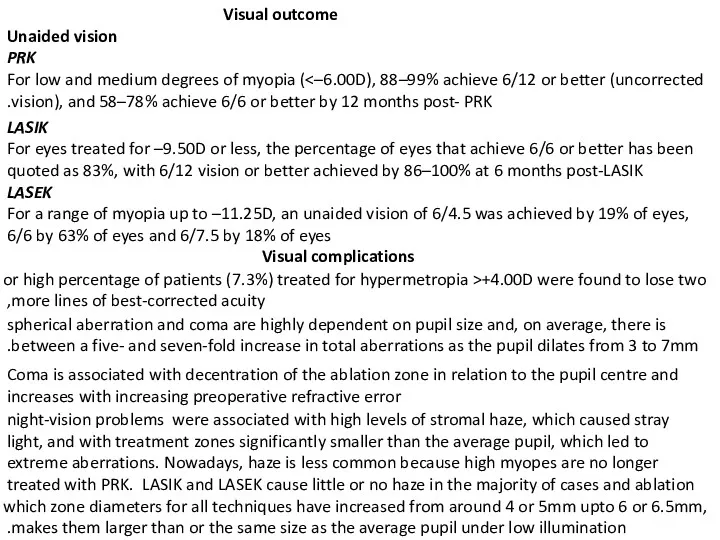
Visual outcome
Unaided vision
PRK
For low and medium degrees of myopia
Visual outcome
Unaided vision
PRK
For low and medium degrees of myopia
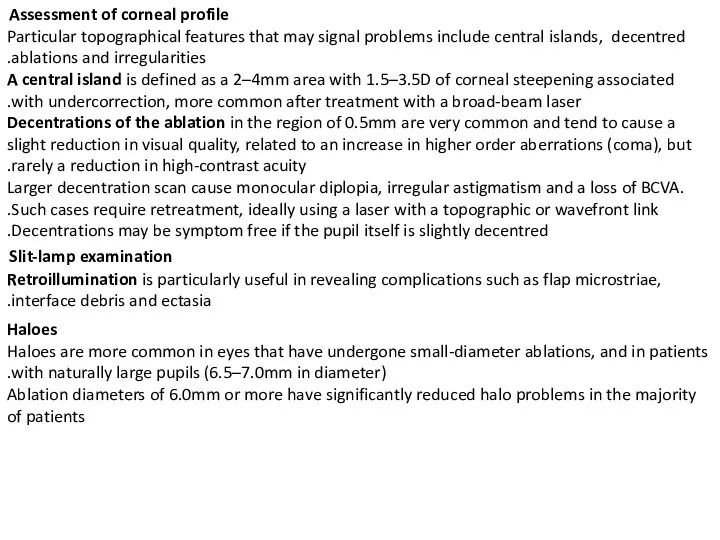
Particular topographical features that may signal problems include central islands,
Particular topographical features that may signal problems include central islands,




















 Тыныс алудың маңызы. Тыныс алу мүшелері көмей бронхылар кеңірдек
Тыныс алудың маңызы. Тыныс алу мүшелері көмей бронхылар кеңірдек Металды қалыпталған сауытты дайындауда қолданылатын болат маркасы
Металды қалыпталған сауытты дайындауда қолданылатын болат маркасы Средства, влияющие на Н-холинорецепторы. Н-холиномиметики. Ганглиоблокаторы. Миорелаксанты периферического действия (Лекция 5)
Средства, влияющие на Н-холинорецепторы. Н-холиномиметики. Ганглиоблокаторы. Миорелаксанты периферического действия (Лекция 5) Особенности фармакокинетики и фармакотерапии в неонатальном периоде
Особенности фармакокинетики и фармакотерапии в неонатальном периоде Острые промиелоцитарные лейкозы
Острые промиелоцитарные лейкозы Журектiн аускультациясы патологияда
Журектiн аускультациясы патологияда Промывание желудка
Промывание желудка Осложнения желудочно-кишечного тракта внутриутробного развития
Осложнения желудочно-кишечного тракта внутриутробного развития Продуктивное воспаление
Продуктивное воспаление 05. медичне страхування
05. медичне страхування Рестриктивные кардиомиопатии. Формы РКМП
Рестриктивные кардиомиопатии. Формы РКМП Опухоли слюнных желез
Опухоли слюнных желез Изосерологическая несовместимость крови матери и плода
Изосерологическая несовместимость крови матери и плода Болезнь Лайма
Болезнь Лайма Рак яичников
Рак яичников Введение в доказательную медицину
Введение в доказательную медицину Вплив алкоголю на дітей та підлітків
Вплив алкоголю на дітей та підлітків Дерматомиозит
Дерматомиозит Кавказские Минеральные Воды
Кавказские Минеральные Воды Профессиональная гигиена полости рта
Профессиональная гигиена полости рта Т-20С.31 янв
Т-20С.31 янв Дифференциально-диагностический поиск у пациентов с гипогликемическим синдромом
Дифференциально-диагностический поиск у пациентов с гипогликемическим синдромом Сердце, аорта, кровь, вены, капилляры
Сердце, аорта, кровь, вены, капилляры Ларингит
Ларингит Проблемы нормативного обеспечения в сфере информатизации здравоохранения
Проблемы нормативного обеспечения в сфере информатизации здравоохранения Қан айналымды зерттеу әдістері. Интегралдық және регионарлық реография. Реография
Қан айналымды зерттеу әдістері. Интегралдық және регионарлық реография. Реография Анемия у детей
Анемия у детей Клиническая характеристика больных и оказание неотложной помощи при почечной колике
Клиническая характеристика больных и оказание неотложной помощи при почечной колике