Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy презентация
- Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy

Содержание
- 2. Adverse Drug Reactions (ADRs) include all unintended pharmacologic effects of a drug except: ● Therapeutic Failures,
- 3. Unpredictable reactions: ● Drug Intolerance ● Drug Idiosyncrasy ● Drug Allergy ● Pseudoallergic Reactions. Drug allergy
- 4. A. Humoral Type: Type I (Anaphylactic) reactions - Immediate hypersensitivity reactions are IgE mediated: Urticaria, Itching,
- 5. B. Cell Mediated: Type IV (Delayed hypersensitivity) reactions: several hours or days after exposure to the
- 6. The antigen reacts with reaginic IgE antibodies, bound to the surface of mast cells and basophils,
- 7. DRUG ALLERGY The most dangerous type of ADRs. 45% reports of AR/SE of drugs in town
- 8. Allergic Anamnesis Ignoring Analgin, Aspirin, Ampicillin were administered in patients with allergic anamnesis (sometimes with other
- 9. The various subtypes of T lymphocytes (Cytotoxic, Helper and Suppressor) and their responses constitute Cell Mediated
- 10. The spectrum of drug allergic reactions and syndromes DRESS: Drug Rash with Eosinophilia and Systemic Symptoms;
- 11. Atopic allergy and targets for therapy Allergen Avoid allergen ? IgE synthesis Desensitize ? Stabilize Mast
- 12. Aspirin and other NSAIDs are reported to account for 21-25% of all Adverse Drug Reactions Intake
- 13. Cyclo-oxygenase (COX) and Lipoxygenase (LO) are 2 main pathways of the metabolism of Arachidonic Acid The
- 14. ANTIALLERGIC DRUGS 1. Drugs Stabilizing Mast Cell Membrane: Glucocorticoids: Prednisolone, Hydrocortisone Antihistamine H1 : Ketotifen a
- 15. GLUCOCORTICOIDS (GCs) 1. Short-acting: Hydrocortisone acetate Cortisone 2. Intermediate-acting: Prednisolone Triamcinolone 3. Long-acting: Betametasone, Dexametasone OINTMENTS
- 16. Mechanism of Action of Glucocorticoids Steroid hormones are lipid soluble and cross cell membranes easily. Once
- 17. Action of GCs on mediators of inflammatory and immune response: GCs change Gene Expression: ? Production
- 18. Adverse effects of GCs: Cushing’s syndrome: Moon face, with red cheeks Thin arms and legs: muscle
- 19. Cromolyn sodium (caps. 20 mg for inhalation) and Nedocromil (aerosol: 2 mg/dose) stabilize mast cells and
- 20. Ketotifen (tab. 1 mg), a cromolyn analog, is an antihistaminic (H1) and mast cell stabilizer. ●
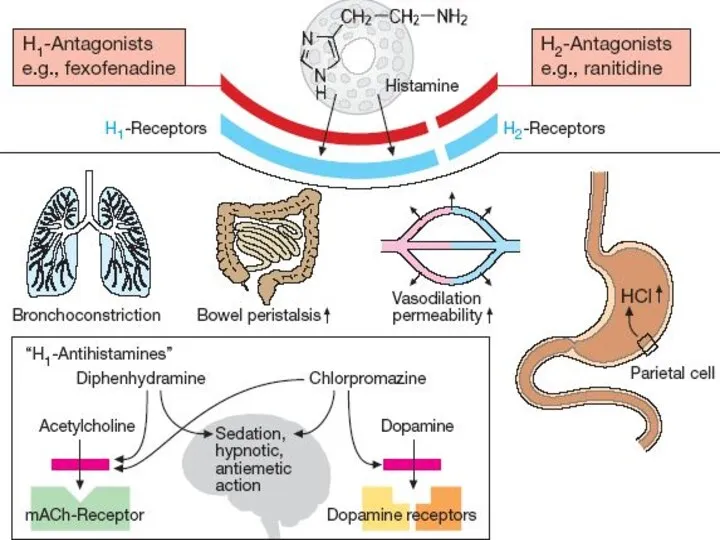
- 21. H1-Receptors: Exocrine excretion => ?Nasal and Bronchial mucus Bronchial smooth muscle constriction => bronchospasm Intestinal smooth
- 23. H1-Receptor Antagonists I GENERATION (SEDATIVE): Dimedrol (Diphenhydramine) Diprazine (Promethazine) Suprastine (Chloropyramine) Diazoline Tavegyl (Clemastin) II GENERATION
- 24. Pharmacodynamics of antihistamine H1 blockers ⮞ Block the actions of histamine by reversible competitive antagonism at
- 25. Dimedrol (Diphenhydramine)-Tab 0.05 g, amp 1%-1 ml competes to H1 receptors on the smooth muscle of
- 26. Terfenadine (Claritin)-. ● blocks cardiac K+ channels, prolongs Q-T and has occasionally produced Polymorphic Ventricular Tachycardia.
- 27. Sympathomimetics: Adrenaline h/ch - 0.1% sol. 0.3-0,5-1 ml in 2-3 ml of 0.9% NCl solution SC
- 28. Drugs used to treat Delayed Type Hypersensitivity Reactions: I. IMMUNOSUPRESSANTS - suppressing mainly cell-mediated immunity: 1.Inhibitors
- 29. Drugs used to treat Delayed Type Hypersensitivity Reactions: II. Drugs decreasing tissue damage – 1. Glucocorticoids
- 31. Скачать презентацию
Adverse Drug Reactions (ADRs) include all unintended pharmacologic effects of a
Adverse Drug Reactions (ADRs) include all unintended pharmacologic effects of a
Unpredictable reactions:
● Drug Intolerance
● Drug Idiosyncrasy
● Drug
Unpredictable reactions:
● Drug Intolerance
● Drug Idiosyncrasy
● Drug
A. Humoral Type:
Type I (Anaphylactic) reactions - Immediate hypersensitivity reactions are
A. Humoral Type:
Type I (Anaphylactic) reactions - Immediate hypersensitivity reactions are
B. Cell Mediated:
Type IV (Delayed hypersensitivity) reactions:
several hours or days
B. Cell Mediated:
Type IV (Delayed hypersensitivity) reactions:
several hours or days
The antigen reacts with reaginic IgE antibodies, bound to the surface
The antigen reacts with reaginic IgE antibodies, bound to the surface
DRUG ALLERGY
The most dangerous type of ADRs.
45% reports of AR/SE of
DRUG ALLERGY
The most dangerous type of ADRs.
45% reports of AR/SE of
Allergic Anamnesis Ignoring
Analgin, Aspirin, Ampicillin were administered in patients with
Allergic Anamnesis Ignoring
Analgin, Aspirin, Ampicillin were administered in patients with
The various subtypes of T lymphocytes
(Cytotoxic, Helper and Suppressor) and
The various subtypes of T lymphocytes
(Cytotoxic, Helper and Suppressor) and
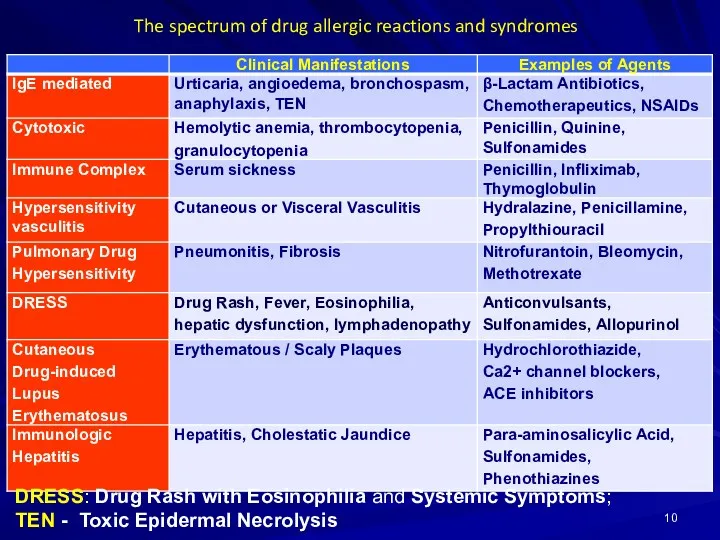
The spectrum of drug allergic reactions and syndromes
DRESS: Drug Rash with
The spectrum of drug allergic reactions and syndromes
DRESS: Drug Rash with
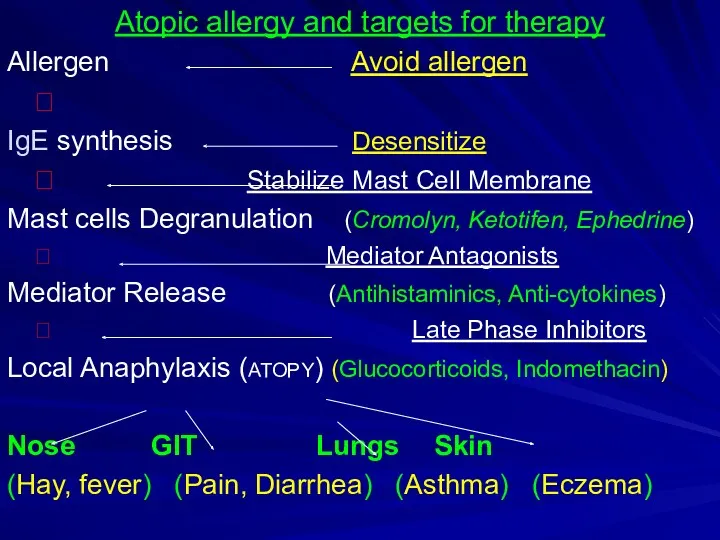
Atopic allergy and targets for therapy
Allergen Avoid allergen
?
IgE synthesis Desensitize
Atopic allergy and targets for therapy
Allergen Avoid allergen
?
IgE synthesis Desensitize
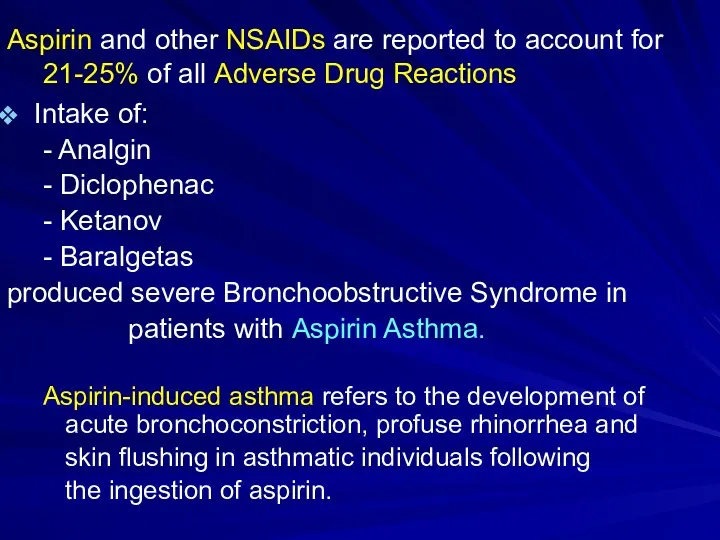
Aspirin and other NSAIDs are reported to account for 21-25% of
Aspirin and other NSAIDs are reported to account for 21-25% of
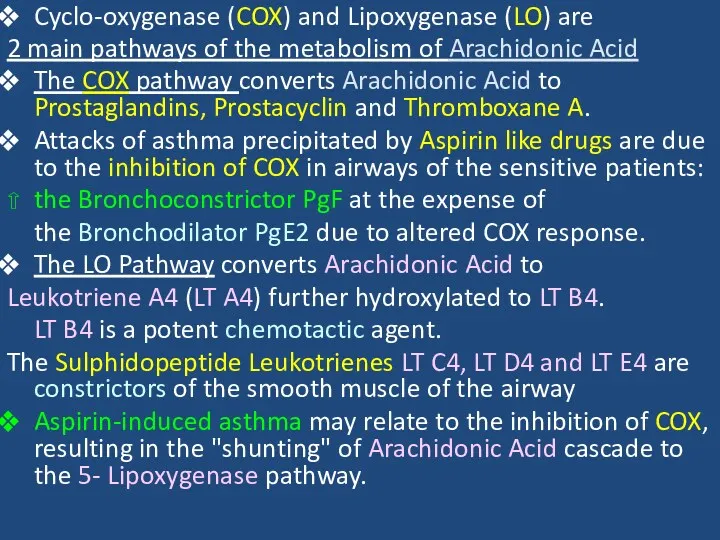
Cyclo-oxygenase (COX) and Lipoxygenase (LO) are
2 main pathways of the
Cyclo-oxygenase (COX) and Lipoxygenase (LO) are
2 main pathways of the
ANTIALLERGIC DRUGS
1. Drugs Stabilizing Mast Cell Membrane:
Glucocorticoids: Prednisolone, Hydrocortisone
Antihistamine H1
ANTIALLERGIC DRUGS
1. Drugs Stabilizing Mast Cell Membrane:
Glucocorticoids: Prednisolone, Hydrocortisone
Antihistamine H1
GLUCOCORTICOIDS (GCs)
1. Short-acting: Hydrocortisone acetate Cortisone
2. Intermediate-acting:
Prednisolone
Triamcinolone
3. Long-acting:
GLUCOCORTICOIDS (GCs)
1. Short-acting: Hydrocortisone acetate Cortisone
2. Intermediate-acting:
Prednisolone
Triamcinolone
3. Long-acting:
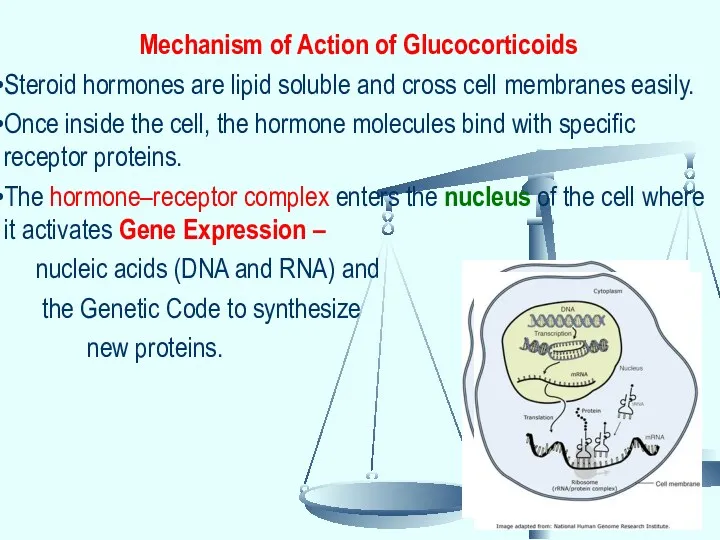
Mechanism of Action of Glucocorticoids
Steroid hormones are lipid soluble and cross
Mechanism of Action of Glucocorticoids
Steroid hormones are lipid soluble and cross
Action of GCs on mediators of inflammatory
and immune response:
GCs change
Action of GCs on mediators of inflammatory
and immune response:
GCs change
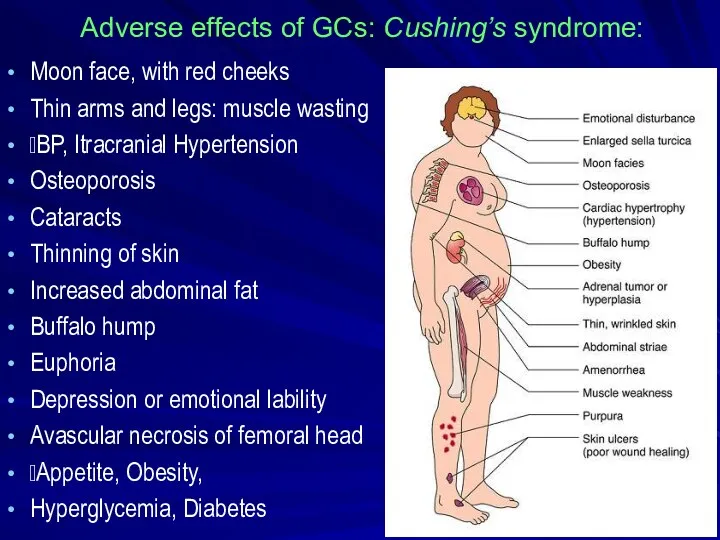
Adverse effects of GCs: Cushing’s syndrome:
Moon face, with red cheeks
Thin
Adverse effects of GCs: Cushing’s syndrome:
Moon face, with red cheeks
Thin
Cromolyn sodium (caps. 20 mg for inhalation) and
Nedocromil (aerosol: 2
Cromolyn sodium (caps. 20 mg for inhalation) and
Nedocromil (aerosol: 2
Ketotifen (tab. 1 mg), a cromolyn analog, is an antihistaminic (H1)
Ketotifen (tab. 1 mg), a cromolyn analog, is an antihistaminic (H1)
H1-Receptors:
Exocrine excretion => ?Nasal and Bronchial mucus
Bronchial smooth
H1-Receptors:
Exocrine excretion => ?Nasal and Bronchial mucus
Bronchial smooth
H1-Receptor Antagonists
I GENERATION (SEDATIVE):
Dimedrol (Diphenhydramine)
Diprazine (Promethazine)
Suprastine (Chloropyramine)
Diazoline
Tavegyl (Clemastin)
II GENERATION
H1-Receptor Antagonists
I GENERATION (SEDATIVE):
Dimedrol (Diphenhydramine)
Diprazine (Promethazine)
Suprastine (Chloropyramine)
Diazoline
Tavegyl (Clemastin)
II GENERATION
Pharmacodynamics of antihistamine H1 blockers
⮞ Block the actions of histamine
Pharmacodynamics of antihistamine H1 blockers
⮞ Block the actions of histamine
Dimedrol (Diphenhydramine)-Tab 0.05 g, amp 1%-1 ml
competes to H1 receptors
Dimedrol (Diphenhydramine)-Tab 0.05 g, amp 1%-1 ml
competes to H1 receptors
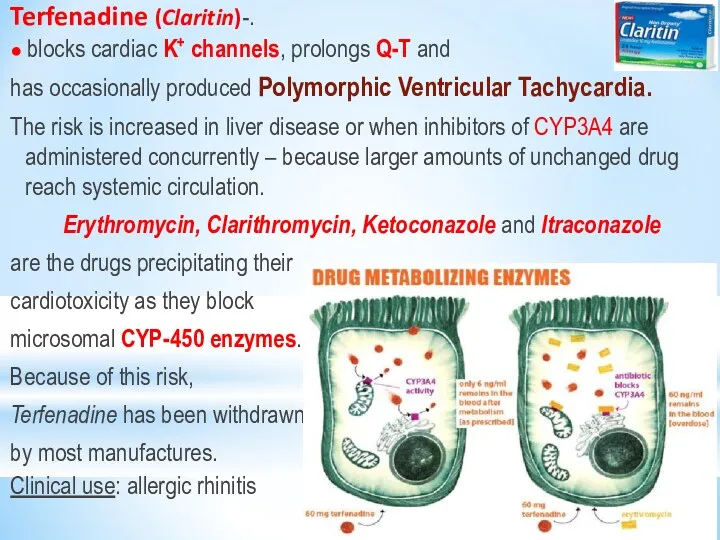
Terfenadine (Claritin)-.
● blocks cardiac K+ channels, prolongs Q-T and
has
Terfenadine (Claritin)-.
● blocks cardiac K+ channels, prolongs Q-T and
has
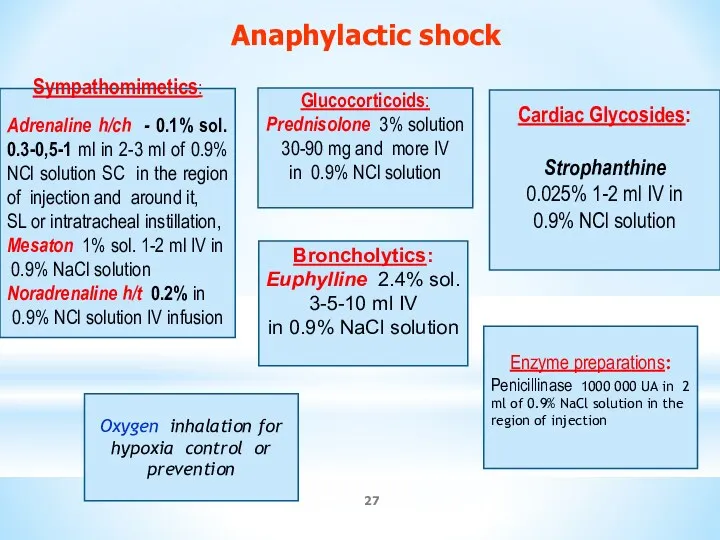
Sympathomimetics:
Adrenaline h/ch - 0.1% sol. 0.3-0,5-1 ml in 2-3 ml of
Sympathomimetics:
Adrenaline h/ch - 0.1% sol. 0.3-0,5-1 ml in 2-3 ml of
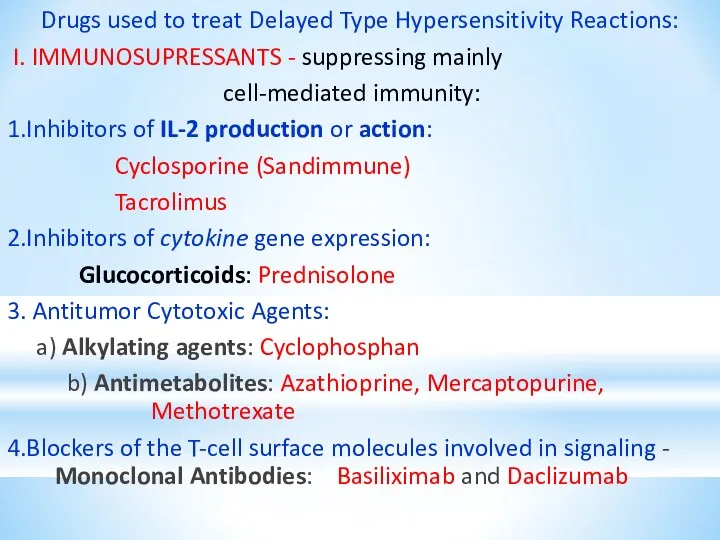
Drugs used to treat Delayed Type Hypersensitivity Reactions:
I. IMMUNOSUPRESSANTS
Drugs used to treat Delayed Type Hypersensitivity Reactions:
I. IMMUNOSUPRESSANTS
Drugs used to treat
Delayed Type Hypersensitivity Reactions:
II. Drugs decreasing
Drugs used to treat
Delayed Type Hypersensitivity Reactions:
II. Drugs decreasing
 Aims and Rationale
Aims and Rationale Рекуррентные ОРВИ в практике педиатра
Рекуррентные ОРВИ в практике педиатра Лечение шизофрении
Лечение шизофрении Международной классификации болезней (МКБ-10)
Международной классификации болезней (МКБ-10) Энергозатраты организма
Энергозатраты организма Острые эндогенные психозы
Острые эндогенные психозы Эпидемиологическая ситуация по ТБ в мире и Украине
Эпидемиологическая ситуация по ТБ в мире и Украине Острый нелимфобластный лейкоз. Клинический случай
Острый нелимфобластный лейкоз. Клинический случай Неправильные положения плода. Разгибательные предлежания головки плода. Тема 6
Неправильные положения плода. Разгибательные предлежания головки плода. Тема 6 Применение левосимендана в практике кардиологической и кардиохирургической реанимации – голос За
Применение левосимендана в практике кардиологической и кардиохирургической реанимации – голос За Возбудители инфекций верхних дыхательных путей, характеризующихся специфичностью патогенеза и клинической картины
Возбудители инфекций верхних дыхательных путей, характеризующихся специфичностью патогенеза и клинической картины Электрокардиограмма при гипертрофии различных отделов миокарда
Электрокардиограмма при гипертрофии различных отделов миокарда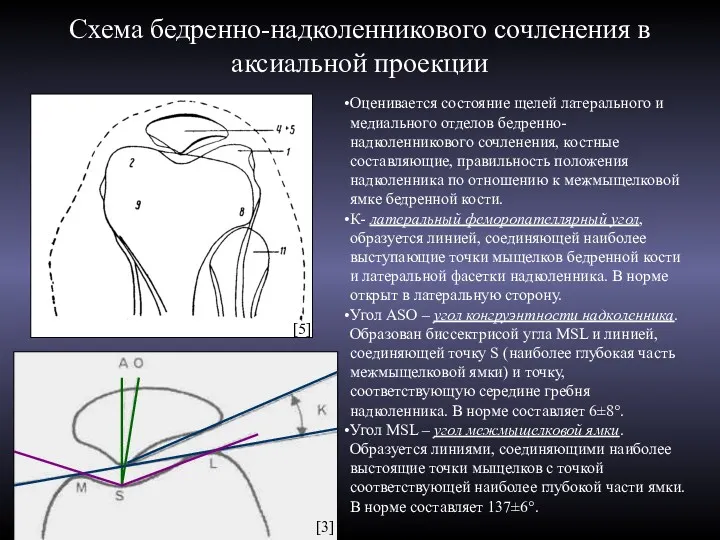 Схема бедренно-надколенникового сочленения в аксиальной проекции
Схема бедренно-надколенникового сочленения в аксиальной проекции Медицинская демография. (Лекция 4)
Медицинская демография. (Лекция 4) Профилактика врожденной патологии лица
Профилактика врожденной патологии лица Причины интеллектуальных нарушений и слабовыраженных отклонений. Классификация нарушения по степени тяжести
Причины интеллектуальных нарушений и слабовыраженных отклонений. Классификация нарушения по степени тяжести Гомеопатия
Гомеопатия Гематология анализаторлар тобы
Гематология анализаторлар тобы Медициналық аспаптарды стерилизациялау
Медициналық аспаптарды стерилизациялау Питание пациентов терапевтического профиля
Питание пациентов терапевтического профиля Медицинские приборнокомпьютерные системы (МПКС)
Медицинские приборнокомпьютерные системы (МПКС) Общая хирургическая техника. Хирургический инструментарий. Принципы местной анестезии
Общая хирургическая техника. Хирургический инструментарий. Принципы местной анестезии Жасушалық иммунитет жүйесінің негізгі қызметтері. Иммунологиялық төзімділік
Жасушалық иммунитет жүйесінің негізгі қызметтері. Иммунологиялық төзімділік Адаптаційні зміни в організмі жінки під час вагітності. Лабораторна діагностика при вагітності. Методи обстеження вагітних
Адаптаційні зміни в організмі жінки під час вагітності. Лабораторна діагностика при вагітності. Методи обстеження вагітних Адам эмбриогенезі. Дамудың қауіпті кезеңдері
Адам эмбриогенезі. Дамудың қауіпті кезеңдері Интенсивная терапия острых отравлений
Интенсивная терапия острых отравлений Заикание. Особенности течения заикания
Заикание. Особенности течения заикания Клещевой энцефалит, болезнь Лайма
Клещевой энцефалит, болезнь Лайма