- Gastrointestinal functional diseases in children

Содержание
- 2. Plan of the lecture 1. Definition of gastrointestinal functional diseases in children 2. Etiologic factors 3.
- 3. Functional gastrointestinal Disorders: Definition Functional gastrointestinal disorders is combination of different gastrointestinal symptoms without structural or
- 4. Functional gastrointestinal Disorders: Definition According to conventional definition functional diseases are those ones when any morphological,
- 5. Functional gastrointestinal Disorders (FGD): Classification According to adopted FGD classification in children they were divided for
- 6. Functional gastrointestinal Disorders (FGD): Classification G. Functional gastrointestinal Disorders : Newborns/ Infants G1. Infant regurgitation G2.
- 7. Functional gastrointestinal Disorders (FGD): Classification Н. Child FGD :Children/Adolescents Н1. Vomiting and aerophagia. Н1а. Rumination syndrome
- 8. Functional gastrointestinal Disorders (FGD): Classification Н. Child FGD :Children/Adolescents Н2. Abdomen pain due to FGD. Н2а.
- 9. Functional gastrointestinal Disorders (FGD): reasons Anatomic and functional immaturity of gastro-intestinal system; Uncoordinated work of different
- 10. Functional gastrointestinal Disorders : Pathogenesis Conceptual model of FFGD Psychosocial factors Stress Ability of stress overcoming
- 11. Infant Regurgitation Morbidity in 20-50 % of first 6 mo old infants (after active questioning is
- 12. Infant Regurgitation Regurgitation is a passive involuntary food passge into oral cavity and outside Vomiting is
- 13. RUMINATION SYNDROME IN INFANTS: DEFINITION Rumination is constant regurgitation with recently consumed food when child chew
- 14. RUMINATION SYNDROME IN INFANTS: etiology and pathogenesis There is hypothesis that rumination syndrome is due to
- 15. RUMINATION SYNDROME IN INFANTS: symptoms Rumination syndrome is presented by periodic attacks of anterior abdomen musculature,
- 16. RUMINATION SYNDROME IN INFANTS: Rome criteria III Diagnosis is made when symptoms are present not less
- 17. RUMINATION SYNDROME IN INFANTS: treatment Provide favourable surrounding for child and calming regimen Behavioral therapy Food
- 18. AEROPHAGIA: Definition Aerophagia is sensation of epigastrium spreading due to excessive air swallowing that decreases after
- 19. AEROPHAGIA: Clinical presentation It appears with loud air eructation enhanced by psycho-emotional excitability Frequently this eructation
- 20. AEROPHAGIA: Rome criteria III Diagnosis is made if not less than 2 signs are present Air
- 21. AEROPHAGIA: Treatment To provide information Dietetic recommendations (prohibit candies, chewing gum and carbonate water, slow food
- 22. Cyclic vomiting syndrome: definition Cyclic vomiting syndrome (СVS) – is a disease predominantly of child period
- 23. Cyclic vomiting syndrome: Etiology More frequent provoked factors are Infection (41 %), especially chronic sinusitis; Psychological
- 24. Cyclic vomiting syndrome: Pathogenesis There are two mechanisms of nausea and vomiting First one: Is connected
- 25. Cyclic vomiting syndrome: Pathogenesis Second mechanism: Is connected with chemoreceptor trigger zone stimulation. From this zone
- 26. Cyclic vomiting syndrome:Clinical presentation Prodrome period is a time interval when patient feel cyclic vomiting syndrome
- 27. Cyclic vomiting syndrome: Clinical presentation Period of exacerbation is manifested with recurrent nausea and vomiting in
- 28. Cyclic vomiting syndrome: Clinical presentation Lethargy (pathologic condition manifested by suppressing of all life signs) can
- 29. Cyclic vomiting syndrome: Clinical presentation Lot of patients with СVS have neurologic disturbancies which can connect
- 30. Cyclic vomiting syndrome: treatment
- 31. Functional constipation Diagnostic criteria: Elongation of intervals between defecation more than 32-36 h Long period of
- 32. Risk factors Early artificial feeding Perinatal CNS affection Prematurity Morpho-functional newborn immaturity Food intolerance Dysbacteriosis Gastro-intestinal
- 33. Treatment Diet Improvement of mother’s diet (decreasing of fats and subsiding it by oils, include into
- 34. Gastro-esophageal Reflux disease (GERD) Disease is manifested with inflammation in esophagus distal part mucous membranes or/and
- 35. Classification Endoscopy-negative HERD or not erosive (60-65%) Reflux-esophagitis (30-35%) – is damaging of esophagus mucous membrane,
- 36. Predisposing factors for HERD Diaphragm hernia Smoking Medication intake that decrease pressure in lower esophagus sphyncter
- 37. Clinical symptoms Esophagus symptoms Burning (retrasternum or epigastrium sensation of burning) , enhanced after meal, carbonate
- 38. Another symptoms: Respiratory – cough, dyspnea attacks Otholaryngologic –voice mutation, dryness of throat, sinusitis, pharyngytis Stomatologic
- 39. Diagnostic methods Necessary instrumental examining: Fibrogastroduodenoscopy Esophagus mucous membrane biopsy in complicated cases Radiologic methods of
- 40. Additional methods 24-h intraesophagus pH –metry is a “gold standard”: elongation of reflux time (рН less
- 41. Treatment Main aim: Stop symptoms To heal erosions To prevent complications To improve life quality Prophylaxis
- 42. Medications Prokineticsо (stimulate food passage through GI tract) domperidon (motilium), methoclopromide Antisecretory medications: lasnprosol, rabeprasol, esomeprasol.
- 44. Скачать презентацию
Plan of the lecture
1. Definition of gastrointestinal functional diseases in
Plan of the lecture
1. Definition of gastrointestinal functional diseases in
Functional gastrointestinal Disorders: Definition
Functional gastrointestinal disorders is combination of different gastrointestinal
Functional gastrointestinal Disorders: Definition
Functional gastrointestinal disorders is combination of different gastrointestinal
Functional gastrointestinal Disorders: Definition
According to conventional definition functional diseases are those
Functional gastrointestinal Disorders: Definition
According to conventional definition functional diseases are those
Functional gastrointestinal Disorders (FGD): Classification
According to adopted FGD classification in children
Functional gastrointestinal Disorders (FGD): Classification
According to adopted FGD classification in children
Functional gastrointestinal Disorders (FGD): Classification
G. Functional gastrointestinal Disorders : Newborns/ Infants
G1.
Functional gastrointestinal Disorders (FGD): Classification
G. Functional gastrointestinal Disorders : Newborns/ Infants
G1.
Functional gastrointestinal Disorders (FGD): Classification
Н. Child FGD :Children/Adolescents
Н1. Vomiting and aerophagia.
Н1а.
Functional gastrointestinal Disorders (FGD): Classification
Н. Child FGD :Children/Adolescents
Н1. Vomiting and aerophagia.
Н1а.
Functional gastrointestinal Disorders (FGD): Classification
Н. Child FGD :Children/Adolescents
Н2. Abdomen pain
Functional gastrointestinal Disorders (FGD): Classification
Н. Child FGD :Children/Adolescents
Н2. Abdomen pain
Functional gastrointestinal Disorders (FGD): reasons
Anatomic and functional immaturity of gastro-intestinal system;
Uncoordinated
Functional gastrointestinal Disorders (FGD): reasons
Anatomic and functional immaturity of gastro-intestinal system;
Uncoordinated
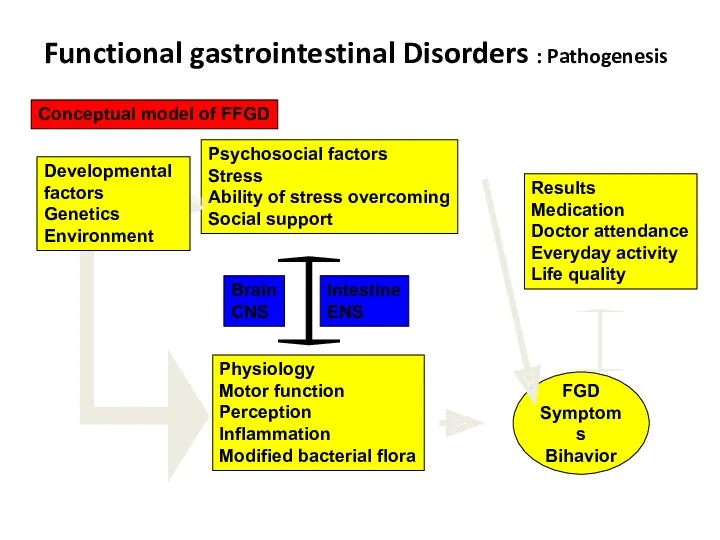
Functional gastrointestinal Disorders : Pathogenesis
Conceptual model of FFGD
Psychosocial factors
Stress
Ability of stress
Functional gastrointestinal Disorders : Pathogenesis
Conceptual model of FFGD
Psychosocial factors
Stress
Ability of stress
Infant Regurgitation
Morbidity in 20-50 % of first 6 mo old infants
Infant Regurgitation
Morbidity in 20-50 % of first 6 mo old infants
Infant Regurgitation
Regurgitation is a passive involuntary food passge into oral
Infant Regurgitation
Regurgitation is a passive involuntary food passge into oral
RUMINATION SYNDROME IN INFANTS: DEFINITION
Rumination is constant regurgitation with recently consumed
RUMINATION SYNDROME IN INFANTS: DEFINITION
Rumination is constant regurgitation with recently consumed
RUMINATION SYNDROME IN INFANTS: etiology and pathogenesis
There is hypothesis that rumination
RUMINATION SYNDROME IN INFANTS: etiology and pathogenesis
There is hypothesis that rumination
RUMINATION SYNDROME IN INFANTS: symptoms
Rumination syndrome is presented by periodic attacks
RUMINATION SYNDROME IN INFANTS: symptoms
Rumination syndrome is presented by periodic attacks
RUMINATION SYNDROME IN INFANTS: Rome criteria III
Diagnosis is made when symptoms
RUMINATION SYNDROME IN INFANTS: Rome criteria III
Diagnosis is made when symptoms
RUMINATION SYNDROME IN INFANTS: treatment
Provide favourable surrounding for child and calming
RUMINATION SYNDROME IN INFANTS: treatment
Provide favourable surrounding for child and calming
AEROPHAGIA: Definition
Aerophagia is sensation of epigastrium spreading due to excessive air
AEROPHAGIA: Definition
Aerophagia is sensation of epigastrium spreading due to excessive air
AEROPHAGIA: Clinical presentation
It appears with loud air eructation enhanced by psycho-emotional
AEROPHAGIA: Clinical presentation
It appears with loud air eructation enhanced by psycho-emotional
AEROPHAGIA: Rome criteria III
Diagnosis is made if not less than 2
AEROPHAGIA: Rome criteria III
Diagnosis is made if not less than 2
AEROPHAGIA: Treatment
To provide information
Dietetic recommendations (prohibit candies, chewing gum and carbonate
AEROPHAGIA: Treatment
To provide information
Dietetic recommendations (prohibit candies, chewing gum and carbonate
Cyclic vomiting syndrome: definition
Cyclic vomiting syndrome (СVS) – is a disease
Cyclic vomiting syndrome: definition
Cyclic vomiting syndrome (СVS) – is a disease
Cyclic vomiting syndrome: Etiology
More frequent provoked factors are
Infection (41 %), especially
Cyclic vomiting syndrome: Etiology
More frequent provoked factors are
Infection (41 %), especially
Cyclic vomiting syndrome: Pathogenesis
There are two mechanisms of nausea and vomiting
First
Cyclic vomiting syndrome: Pathogenesis
There are two mechanisms of nausea and vomiting
First
Cyclic vomiting syndrome: Pathogenesis
Second mechanism:
Is connected with chemoreceptor trigger zone stimulation.
Cyclic vomiting syndrome: Pathogenesis
Second mechanism:
Is connected with chemoreceptor trigger zone stimulation.
Cyclic vomiting syndrome:Clinical presentation
Prodrome period is a time interval when patient
Cyclic vomiting syndrome:Clinical presentation
Prodrome period is a time interval when patient
Cyclic vomiting syndrome: Clinical presentation
Period of exacerbation is manifested with recurrent
Cyclic vomiting syndrome: Clinical presentation
Period of exacerbation is manifested with recurrent
Cyclic vomiting syndrome: Clinical presentation
Lethargy (pathologic condition manifested by suppressing of
Cyclic vomiting syndrome: Clinical presentation
Lethargy (pathologic condition manifested by suppressing of
Cyclic vomiting syndrome: Clinical presentation
Lot of patients with СVS have neurologic
Cyclic vomiting syndrome: Clinical presentation
Lot of patients with СVS have neurologic
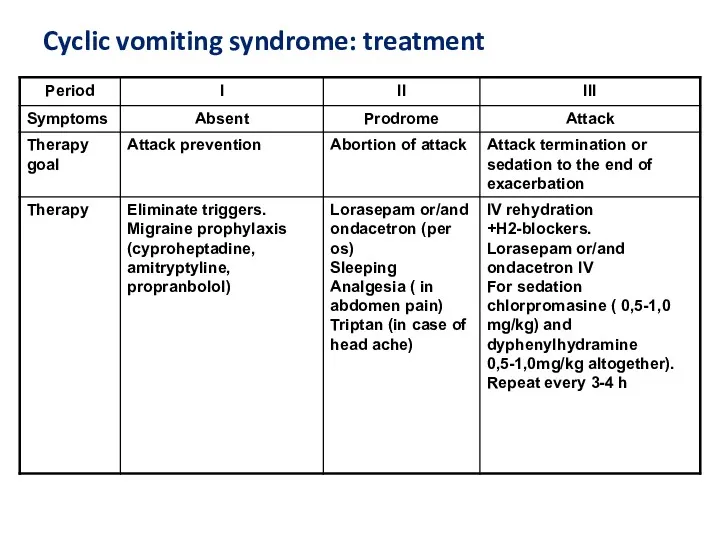
Cyclic vomiting syndrome: treatment
Cyclic vomiting syndrome: treatment
Functional constipation
Diagnostic criteria:
Elongation of intervals between defecation more than 32-36
Functional constipation
Diagnostic criteria:
Elongation of intervals between defecation more than 32-36
Risk factors
Early artificial feeding
Perinatal CNS affection
Prematurity
Morpho-functional newborn immaturity
Food intolerance
Dysbacteriosis
Gastro-intestinal diseases abnormal
Risk factors
Early artificial feeding
Perinatal CNS affection
Prematurity
Morpho-functional newborn immaturity
Food intolerance
Dysbacteriosis
Gastro-intestinal diseases abnormal
Treatment
Diet
Improvement of mother’s diet (decreasing of fats and subsiding it by
Treatment
Diet
Improvement of mother’s diet (decreasing of fats and subsiding it by
Gastro-esophageal Reflux disease (GERD)
Disease is manifested with inflammation in esophagus
Gastro-esophageal Reflux disease (GERD)
Disease is manifested with inflammation in esophagus
Classification
Endoscopy-negative HERD or not erosive (60-65%)
Reflux-esophagitis (30-35%) – is damaging of
Classification
Endoscopy-negative HERD or not erosive (60-65%)
Reflux-esophagitis (30-35%) – is damaging of
Predisposing factors for HERD
Diaphragm hernia
Smoking
Medication intake that decrease pressure in lower
Predisposing factors for HERD
Diaphragm hernia
Smoking
Medication intake that decrease pressure in lower
Clinical symptoms
Esophagus symptoms
Burning (retrasternum or epigastrium sensation of burning) , enhanced
Clinical symptoms
Esophagus symptoms
Burning (retrasternum or epigastrium sensation of burning) , enhanced
Another symptoms:
Respiratory – cough, dyspnea attacks
Otholaryngologic –voice mutation, dryness of throat,
Another symptoms:
Respiratory – cough, dyspnea attacks
Otholaryngologic –voice mutation, dryness of throat,
Diagnostic methods
Necessary instrumental examining:
Fibrogastroduodenoscopy
Esophagus mucous membrane biopsy in complicated cases
Radiologic methods
Diagnostic methods
Necessary instrumental examining:
Fibrogastroduodenoscopy
Esophagus mucous membrane biopsy in complicated cases
Radiologic methods
Additional methods
24-h intraesophagus pH –metry is a “gold standard”: elongation of
Additional methods
24-h intraesophagus pH –metry is a “gold standard”: elongation of
Treatment
Main aim:
Stop symptoms
To heal erosions
To prevent complications
To improve life quality
Prophylaxis of
Treatment
Main aim:
Stop symptoms
To heal erosions
To prevent complications
To improve life quality
Prophylaxis of
Medications
Prokineticsо (stimulate food passage through GI tract) domperidon (motilium), methoclopromide
Antisecretory medications:
Medications
Prokineticsо (stimulate food passage through GI tract) domperidon (motilium), methoclopromide
Antisecretory medications:
 Перикардиты. Анатомия перикарда
Перикардиты. Анатомия перикарда Спадкові захворювання нервової системи
Спадкові захворювання нервової системи ВИЧ: вопросы и ответы
ВИЧ: вопросы и ответы Нейтропении у детей
Нейтропении у детей Николай Иванович Пирогов Русский хирург и анатом
Николай Иванович Пирогов Русский хирург и анатом Информационные технологии для фармацевтов
Информационные технологии для фармацевтов Периоды детства
Периоды детства Антипсихотики (нейролептики)
Антипсихотики (нейролептики) Глобальные риски и новейшие медицинские технологии
Глобальные риски и новейшие медицинские технологии Компрессионные синдромы шейного отдела позвоночника
Компрессионные синдромы шейного отдела позвоночника Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау
Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау Інсульт. Причини, симптоми інсульту, перша допомога, поради
Інсульт. Причини, симптоми інсульту, перша допомога, поради Крон ауруы
Крон ауруы Pancreatic Cancer
Pancreatic Cancer Особенности фармакокинетики и фармакодинамики при лечении аллергий
Особенности фармакокинетики и фармакодинамики при лечении аллергий ИБС. Стенокардия
ИБС. Стенокардия Нәрестелердің асфиксиясы
Нәрестелердің асфиксиясы Опухолевый рост
Опухолевый рост Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы
Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы Нарушения сна у младенцев и детей раннего возраста
Нарушения сна у младенцев и детей раннего возраста Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову
Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову Токсикология фосфорорганических соединений (ФОС)
Токсикология фосфорорганических соединений (ФОС) Анатомо-фізіологічні особливості сечовидільної системи у дітей
Анатомо-фізіологічні особливості сечовидільної системи у дітей Өлім, өлім белгілері
Өлім, өлім белгілері Ми қыртысының анатомиялық-гистологиялық құрылымы
Ми қыртысының анатомиялық-гистологиялық құрылымы Воспалительные процессы органов женской половой системы специфической этиологии
Воспалительные процессы органов женской половой системы специфической этиологии Болезнь Крона
Болезнь Крона Respiratory system
Respiratory system