- Giant cell arteritis

Содержание
- 3. Introduction Giant cell arteritis (GCA) is categorized as a vasculitis of large- and medium-sized vessels Systemic
- 5. Epidemiology GCA is the most common systemic vasculitis The lifetime risk of developing GCA is ~1%
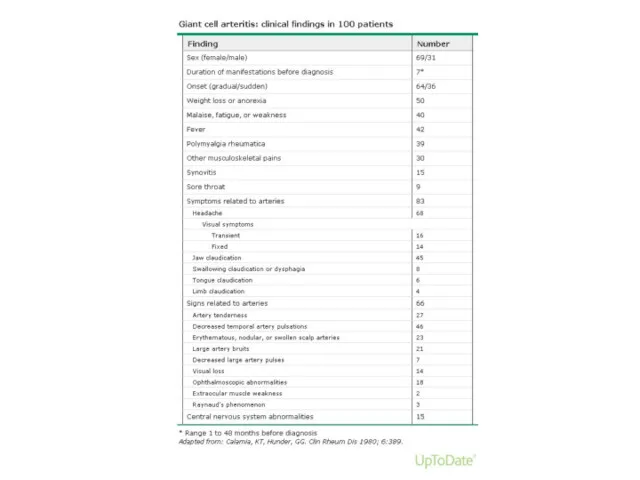
- 6. Clinical findings The onset of symptoms tends to be subacute Abrupt presentations occurs less frequently Systemic
- 8. Clinical findings - Headache Located over the temples, but can also be frontal or occipital or
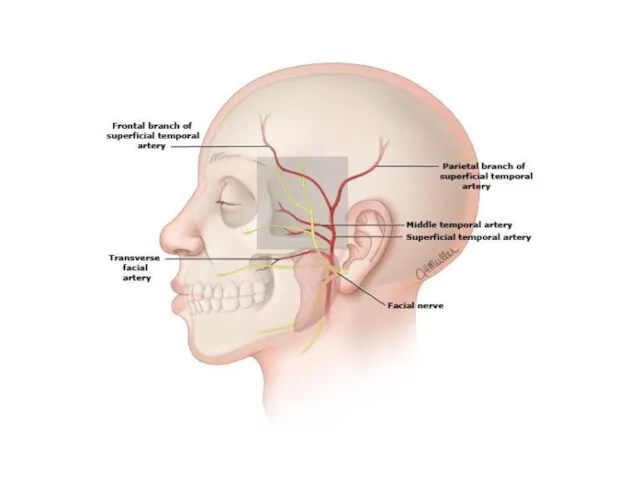
- 9. Temporal artery
- 10. Jaw Claudication Trismus-like symptoms Fatigue of the muscles of mastication Rapid onset after the start of
- 11. Vision Transient visual loss (amaurosis fugax) — Transient monocular (and, rarely, binocular) impairment of vision can
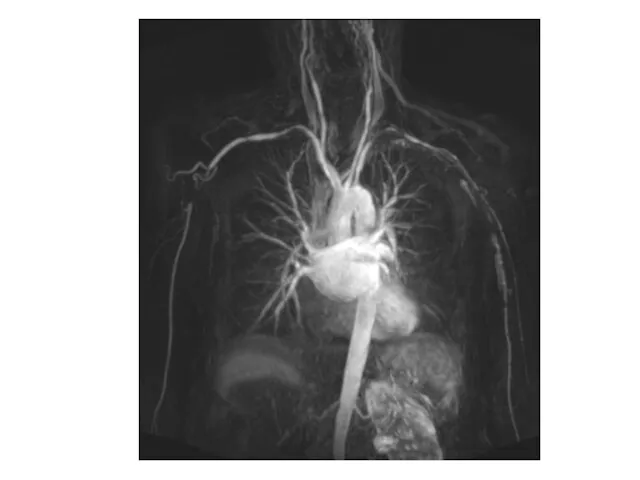
- 12. Large vessel GCA Involvement of the aorta and its major proximal branches - especially in the
- 14. External carotid artery- branches Maxillary and dental pain Facial swelling Throat pain Tongue pain
- 16. Physical examination Pulses – carotid, brachial, radial, femoral, pedal Blood pressure Bruits – carotid or supraclavicular
- 18. AION
- 19. Laboratory findings Normochromic anemia is often present prior to therapy and improves promptly after the institution
- 20. Diagnosis The diagnosis of giant cell arteritis (GCA) should be considered in a patient over the
- 21. Diagnosis Patient suspected of having GCA should undergo temporal artery biopsy ~85% sensitivity Other arteries can
- 22. Biopsy-negative GCA The patient may not have GCA. If the clinical story is equivocal, then alternative
- 23. Imaging MRI/MRA USD Angiography PET-CT
- 24. Treatment Uncomplicated GCA - 40 to 60 mg of prednisone in a single dose After achieving
- 26. Скачать презентацию

Introduction
Giant cell arteritis (GCA) is categorized as a vasculitis of large-
Introduction
Giant cell arteritis (GCA) is categorized as a vasculitis of large-
Epidemiology
GCA is the most common systemic vasculitis
The lifetime risk of developing
Epidemiology
GCA is the most common systemic vasculitis
The lifetime risk of developing
Clinical findings
The onset of symptoms tends to be subacute
Abrupt presentations occurs
Clinical findings
The onset of symptoms tends to be subacute
Abrupt presentations occurs
Clinical findings - Headache
Located over the temples, but can also be
Clinical findings - Headache
Located over the temples, but can also be
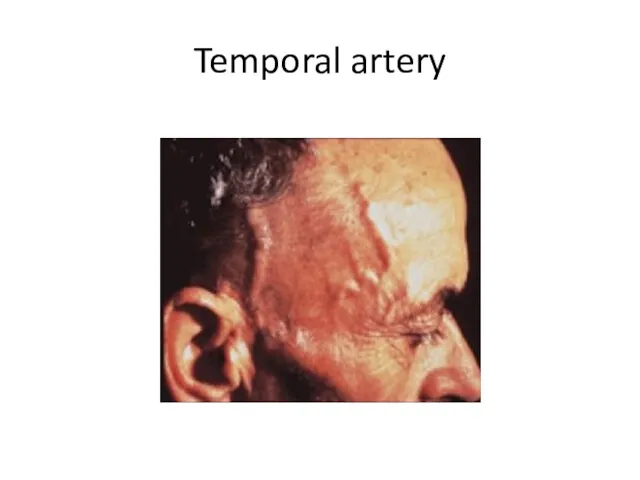
Temporal artery
Temporal artery
Jaw Claudication
Trismus-like symptoms
Fatigue of the muscles of mastication
Rapid onset after the
Jaw Claudication
Trismus-like symptoms
Fatigue of the muscles of mastication
Rapid onset after the
Vision
Transient visual loss (amaurosis fugax) — Transient monocular (and, rarely, binocular) impairment of
Vision
Transient visual loss (amaurosis fugax) — Transient monocular (and, rarely, binocular) impairment of
Large vessel GCA
Involvement of the aorta and its major proximal branches
Large vessel GCA
Involvement of the aorta and its major proximal branches
External carotid artery- branches
Maxillary and dental pain
Facial swelling
Throat pain
Tongue pain
External carotid artery- branches
Maxillary and dental pain
Facial swelling
Throat pain
Tongue pain
Physical examination
Pulses – carotid, brachial, radial, femoral, pedal
Blood pressure
Bruits – carotid
Physical examination
Pulses – carotid, brachial, radial, femoral, pedal
Blood pressure
Bruits – carotid

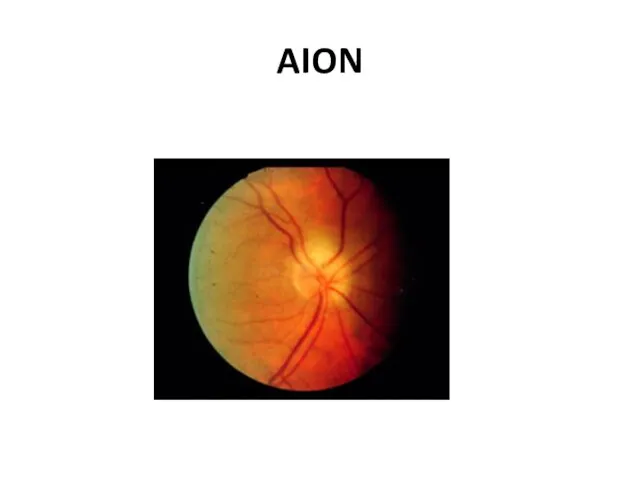
AION
AION
Laboratory findings
Normochromic anemia is often present prior to therapy and improves
Laboratory findings
Normochromic anemia is often present prior to therapy and improves
Diagnosis
The diagnosis of giant cell arteritis (GCA) should be considered in
Diagnosis
The diagnosis of giant cell arteritis (GCA) should be considered in
Diagnosis
Patient suspected of having GCA should undergo temporal artery biopsy
~85% sensitivity
Other
Diagnosis
Patient suspected of having GCA should undergo temporal artery biopsy
~85% sensitivity
Other
Biopsy-negative GCA
The patient may not have GCA. If the clinical story
Biopsy-negative GCA
The patient may not have GCA. If the clinical story
Imaging
MRI/MRA
USD
Angiography
PET-CT
Imaging
MRI/MRA
USD
Angiography
PET-CT
Treatment
Uncomplicated GCA - 40 to 60 mg of prednisone in a single dose
After
Treatment
Uncomplicated GCA - 40 to 60 mg of prednisone in a single dose
After
 Дұрыс тамақтану
Дұрыс тамақтану Прогностические шкалы. Классификация, актуальность
Прогностические шкалы. Классификация, актуальность Лечебно –диагностические вмешательства и сестринский уход при заболеваниях глотки
Лечебно –диагностические вмешательства и сестринский уход при заболеваниях глотки Лікарські засоби, що діють на кровотворення, систему згортання крові та фібриноліз
Лікарські засоби, що діють на кровотворення, систему згортання крові та фібриноліз Диагностика цервикальных неоплазий у женщин репродуктивного возраста
Диагностика цервикальных неоплазий у женщин репродуктивного возраста Экстрапирамидные гиперкинезы
Экстрапирамидные гиперкинезы Асқазан және 12 елі ішектің ойық жарасы аурулары, асқынулары
Асқазан және 12 елі ішектің ойық жарасы аурулары, асқынулары Факторы риска возникновения парадонта и их устранение
Факторы риска возникновения парадонта и их устранение Фармаконимика. Номенклатура
Фармаконимика. Номенклатура Лечения боли у детей
Лечения боли у детей Предоперационная подготовка гинекологических больных
Предоперационная подготовка гинекологических больных Изменения в организме женщины и дискомфортные ощущения во время беременности
Изменения в организме женщины и дискомфортные ощущения во время беременности Диагностика кожных высыпаний у детей
Диагностика кожных высыпаний у детей Экспертиза и регистрация изделий медицинского назначения
Экспертиза и регистрация изделий медицинского назначения История фельдшерского колледжа
История фельдшерского колледжа Туберкулездің емі
Туберкулездің емі Физическая реабилитация при заболеваниях сердечно-сосудистой системы, органов дыхания и пищеварения
Физическая реабилитация при заболеваниях сердечно-сосудистой системы, органов дыхания и пищеварения Дерматомиозит
Дерматомиозит Неотложная помощь при эпилептическом припадке, эпилептическом статусе
Неотложная помощь при эпилептическом припадке, эпилептическом статусе Алкоголь и его влияние на здоровье человека
Алкоголь и его влияние на здоровье человека Пиодермии. Определение
Пиодермии. Определение Антибиотики. Определение
Антибиотики. Определение ДариТал клиникасының бизнес-жоспары
ДариТал клиникасының бизнес-жоспары Современная клинико-диагностическая лаборатория. Лабораторные информационные системы
Современная клинико-диагностическая лаборатория. Лабораторные информационные системы Доброкачественные и злокачественные опухоли эндокринной системы
Доброкачественные и злокачественные опухоли эндокринной системы Клиника, диагностика и терапия предменструального синдрома в современных условиях
Клиника, диагностика и терапия предменструального синдрома в современных условиях Side effects of drugs affecting cardiovascular system
Side effects of drugs affecting cardiovascular system Диагностика, лечение и профилактика сифилиса: первичный, вторичный, третичный
Диагностика, лечение и профилактика сифилиса: первичный, вторичный, третичный