- HCV Case Study. Treat Now or Wait for New Therapies

Содержание
- 2. Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and
- 3. Learning Objectives Describe current data on approved and experimental DAA’s used in combination with Pegylated Interferon
- 4. Glenn: Patient Characteristics 55 year old male Shift worker History/risk factors BMI=34 Hypertension and dyslipidemia Moderate
- 5. Glenn: Baseline Labs Hemoglobin Neutrophils Platelets AST/ALT Albumin Bilirubin 15.6 g/dL 1400 cells/mm3 210,000 cells/mm3 55/75
- 6. Glenn: Disease Characteristics Treatment naïve Genotype IL28B METAVIR BL viral load 1a CC F3 1,300,000 IU/mL
- 7. Clinical Decision 1 How would you manage this patient? Continue to monitor patient but do not
- 8. Modeling of Liver Fibrosis in Chronic Hepatitis C n=1157 Patients 0 1 2 3 4 0
- 9. D’Amico G et al. J Hepatol. 2006;44:217-231. Proportion of Patients 1.00 0.75 0.50 0.25 0.00 Pts
- 10. 0% 20% 40% 60% 80% 100% Non-responders (n=1452) Relapsers (n=464) Sustained responders (n=1094) 36% 43% 86%
- 11. *T12PR = T+PR12 weeks, then PR12 or 36 weeks depending on eRVR status **T8PR = T+PR8
- 12. SVR Rates in F1/2 vs F3/4 Naïve Patients 100 90 80 70 60 50 40 30
- 13. OPTIMIZE Trial: Telaprevir BID vs TID PR + TVR 1125 mg BID versus 750 mg TID
- 14. OPTIMIZE Trial: Results 0 20 40 60 80 100 RVR SVR TVR 1125 mg BID TVR
- 15. Should Glenn Be Treated Now? F3 disease – risk of progression with waiting IL28B CC Potential
- 16. Multiple issues with current therapy Compliance – pill burden Co-morbidities Adverse effects New treatments on the
- 17. Pill Burden Food Requirement BOC = 18/d RBV 4-7/d TVR = 12/d RBV 4-7/d Compliance
- 18. Cardiac Risk Factors Hypertension, hyperlipidemia, smoker Pre Treatment DDI – Statin with TVR/BOC ? likely just
- 19. Drugs with the Potential to Interact with First Generation Protease Inhibitors are Commonly Used by HCV
- 20. No clinically significant interactions Boceprevir Prednisone (abstract #1896) Omeprazole (abstract #1808) Ethinyl estrodiol/norethidrone (abstract #1901) Simeprevir
- 21. 100 90 80 70 60 50 40 30 20 10 0 BOC PR 100 90 80
- 22. Future Options for Waiting? (Short-Term) x 12 wks + PR x 24-48 81 0 20 40
- 23. Anemia with Simeprevir + P/R1 Anemia with Faldaprevir + P/R2 2. Sulkowski et al, EASL 2011
- 24. Select Oral Directing Acting Antivirals in Development for the Treatment of Chronic Hepatitis C, 2012
- 25. Select Oral Directing Acting Antivirals in Development for the Treatment of Chronic Hepatitis C, 2012 (cont)
- 26. Should Glenn Delay Treatment? IL28B CC ? ~80% chance of shortened therapy - 80-90% chance of
- 27. Glenn: On Treatment Response Glenn was started on TVR/PEG/RBV TW4 and TW12 – HCV RNA undetectable
- 28. Clinical Decision 2 Which regimen should Glenn receive? 12 weeks TVR/PEG/RBV 12 weeks TVR/PEG/RBV + 12
- 29. Recommended Treatment Duration Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA. October, 2012.
- 30. HCV-RNA Levels and Lab Assays LLOQ Values for Various Assays* “Undetectable” (or “target not detected”) result
- 32. Скачать презентацию
Program Disclosure
This activity has been planned and implemented in accordance with
Program Disclosure
This activity has been planned and implemented in accordance with
Learning Objectives
Describe current data on approved and experimental DAA’s used in
Learning Objectives
Describe current data on approved and experimental DAA’s used in
Glenn: Patient Characteristics
55 year old male
Shift worker
History/risk factors
BMI=34
Hypertension and dyslipidemia
Moderate drinker/cigarette
Glenn: Patient Characteristics
55 year old male
Shift worker
History/risk factors
BMI=34
Hypertension and dyslipidemia
Moderate drinker/cigarette
Glenn: Baseline Labs
Hemoglobin
Neutrophils
Platelets
AST/ALT
Albumin
Bilirubin
15.6 g/dL
1400 cells/mm3
210,000 cells/mm3 55/75 IU/L
4.1 g/dL
0.7 mg/dL
Glenn: Baseline Labs
Hemoglobin
Neutrophils
Platelets
AST/ALT
Albumin
Bilirubin
15.6 g/dL
1400 cells/mm3
210,000 cells/mm3 55/75 IU/L
4.1 g/dL
0.7 mg/dL
Glenn: Disease Characteristics
Treatment naïve
Genotype
IL28B
METAVIR
BL viral load
1a CC F3
1,300,000 IU/mL
Glenn: Disease Characteristics
Treatment naïve
Genotype
IL28B
METAVIR
BL viral load
1a CC F3
1,300,000 IU/mL
Clinical Decision 1
How would you manage this patient?
Continue to monitor patient
Clinical Decision 1
How would you manage this patient?
Continue to monitor patient
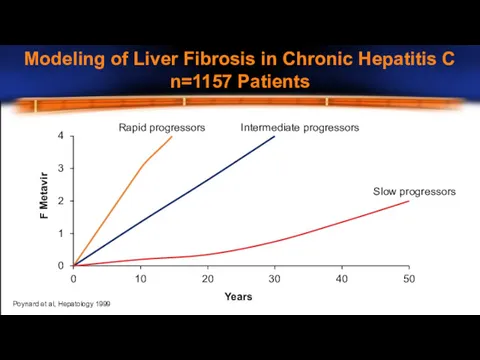
Modeling of Liver Fibrosis in Chronic Hepatitis C
n=1157 Patients
0
1
2
3
4
0
10
20
30
40
50
F Metavir
Years
Rapid progressors
Intermediate
Modeling of Liver Fibrosis in Chronic Hepatitis C
n=1157 Patients
0
1
2
3
4
0
10
20
30
40
50
F Metavir
Years
Rapid progressors
Intermediate
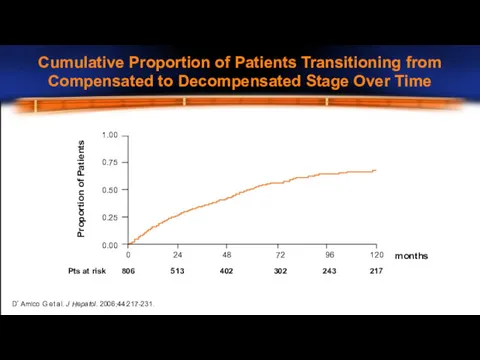
D’Amico G et al. J Hepatol. 2006;44:217-231.
Proportion of Patients
1.00
0.75
0.50
0.25
0.00
Pts at risk
months
0
806
24
513
48
402
72
302
96
243
120
217
Cumulative
D’Amico G et al. J Hepatol. 2006;44:217-231.
Proportion of Patients
1.00
0.75
0.50
0.25
0.00
Pts at risk
months
0
806
24
513
48
402
72
302
96
243
120
217
Cumulative
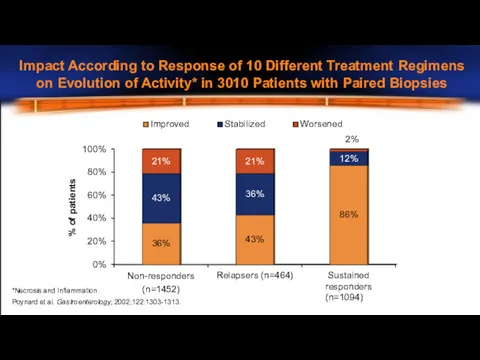
0%
20%
40%
60%
80%
100%
Non-responders (n=1452)
Relapsers (n=464)
Sustained responders (n=1094)
36%
43%
86%
43%
36%
12%
21%
21%
2%
% of patients
Improved
Stabilized
Worsened
*Necrosis and Inflammation.
Poynard et al.
0%
20%
40%
60%
80%
100%
Non-responders (n=1452)
Relapsers (n=464)
Sustained responders (n=1094)
36%
43%
86%
43%
36%
12%
21%
21%
2%
% of patients
Improved
Stabilized
Worsened
*Necrosis and Inflammation.
Poynard et al.
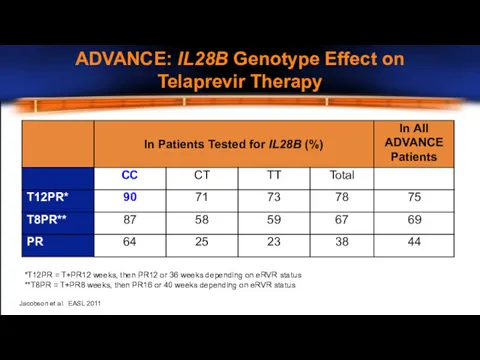
*T12PR = T+PR12 weeks, then PR12 or 36 weeks depending on
*T12PR = T+PR12 weeks, then PR12 or 36 weeks depending on
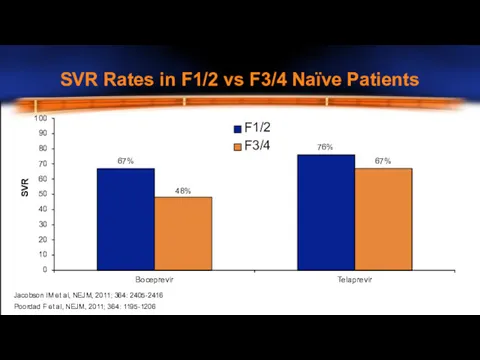
SVR Rates in F1/2 vs F3/4 Naïve Patients
100
90
80
70
60
50
40
30
20
10
0
Telaprevir
F1/2 F3/4
76%
67%
67%
48%
SVR
Boceprevir
Jacobson IM et
SVR Rates in F1/2 vs F3/4 Naïve Patients
100
90
80
70
60
50
40
30
20
10
0
Telaprevir
F1/2 F3/4
76%
67%
67%
48%
SVR
Boceprevir
Jacobson IM et
OPTIMIZE Trial: Telaprevir BID vs TID
PR + TVR 1125 mg BID
OPTIMIZE Trial: Telaprevir BID vs TID
PR + TVR 1125 mg BID
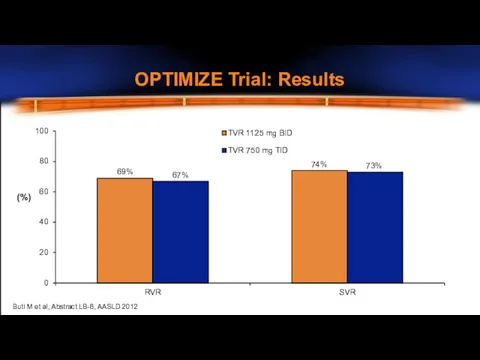
OPTIMIZE Trial: Results
0
20
40
60
80
100
RVR
SVR
TVR 1125 mg BID
TVR 750 mg TID
(%)
69%
67%
74%
73%
Buti M et
OPTIMIZE Trial: Results
0
20
40
60
80
100
RVR
SVR
TVR 1125 mg BID
TVR 750 mg TID
(%)
69%
67%
74%
73%
Buti M et
Should Glenn Be Treated Now?
F3 disease – risk of progression with
Should Glenn Be Treated Now?
F3 disease – risk of progression with
Multiple issues with current therapy
Compliance – pill burden
Co-morbidities
Adverse effects
New treatments on
Multiple issues with current therapy
Compliance – pill burden
Co-morbidities
Adverse effects
New treatments on
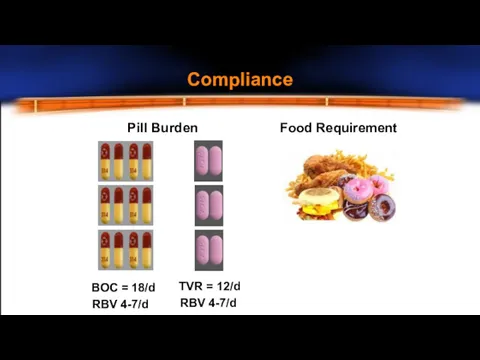
Pill Burden
Food Requirement
BOC = 18/d RBV 4-7/d
TVR = 12/d
RBV 4-7/d
Compliance
Pill Burden
Food Requirement
BOC = 18/d RBV 4-7/d
TVR = 12/d
RBV 4-7/d
Compliance
Cardiac Risk Factors
Hypertension, hyperlipidemia, smoker
Pre Treatment
DDI – Statin with TVR/BOC ?
Cardiac Risk Factors
Hypertension, hyperlipidemia, smoker
Pre Treatment
DDI – Statin with TVR/BOC ?
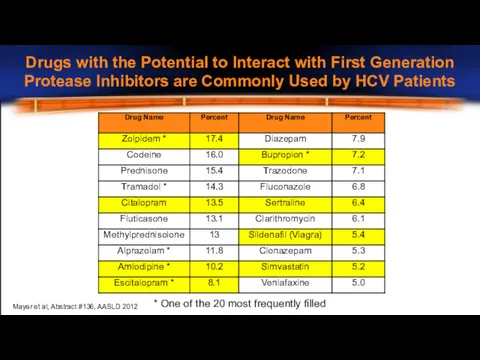
Drugs with the Potential to Interact with First Generation
Protease Inhibitors are
Drugs with the Potential to Interact with First Generation
Protease Inhibitors are
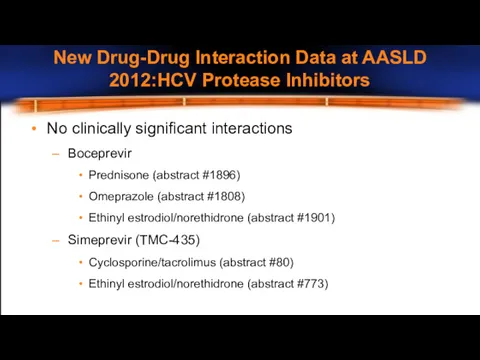
No clinically significant interactions
Boceprevir
Prednisone (abstract #1896)
Omeprazole (abstract #1808)
Ethinyl estrodiol/norethidrone (abstract #1901)
Simeprevir
No clinically significant interactions
Boceprevir
Prednisone (abstract #1896)
Omeprazole (abstract #1808)
Ethinyl estrodiol/norethidrone (abstract #1901)
Simeprevir
100
90
80
70
60
50
40
30
20
10
0
BOC
PR
100
90
80
70
60
50
40
30
20
10
0
TVR PR
% of patients
36%
17%
14%
5%
49%
28%
7%
3%
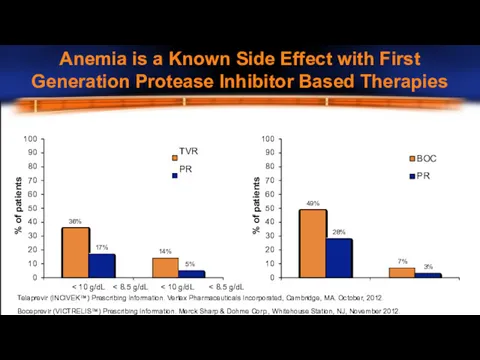
Anemia is a Known Side Effect with First
Generation
100
90
80
70
60
50
40
30
20
10
0
BOC
PR
100
90
80
70
60
50
40
30
20
10
0
TVR PR
% of patients
36%
17%
14%
5%
49%
28%
7%
3%
Anemia is a Known Side Effect with First
Generation
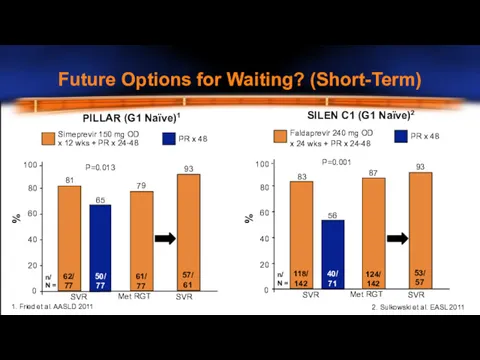
Future Options for Waiting? (Short-Term)
x 12 wks + PR x 24-48
81
0
20
40
60
80
100
%
n/
Future Options for Waiting? (Short-Term)
x 12 wks + PR x 24-48
81
0
20
40
60
80
100
%
n/
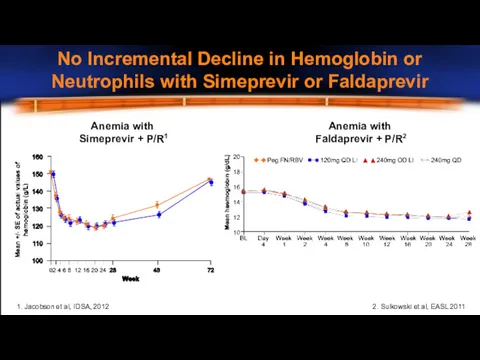
Anemia with
Simeprevir + P/R1
Anemia with
Faldaprevir + P/R2
2. Sulkowski et al, EASL
Anemia with
Simeprevir + P/R1
Anemia with
Faldaprevir + P/R2
2. Sulkowski et al, EASL
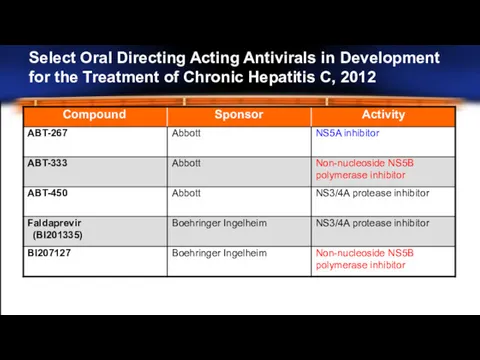
Select Oral Directing Acting Antivirals in Development
for the Treatment of Chronic
Select Oral Directing Acting Antivirals in Development
for the Treatment of Chronic
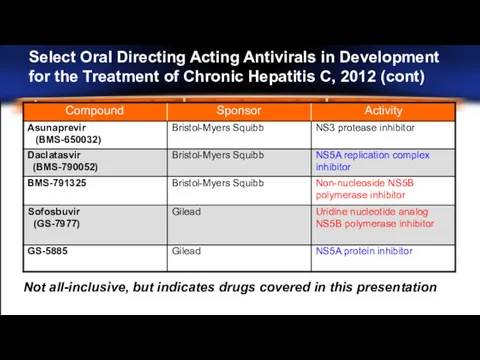
Select Oral Directing Acting Antivirals in Development
for the Treatment of Chronic
Select Oral Directing Acting Antivirals in Development
for the Treatment of Chronic
Should Glenn Delay Treatment?
IL28B CC ? ~80% chance of shortened therapy
-
Should Glenn Delay Treatment?
IL28B CC ? ~80% chance of shortened therapy
-
Glenn: On Treatment Response
Glenn was started on TVR/PEG/RBV
TW4 and TW12
– HCV RNA
Glenn: On Treatment Response
Glenn was started on TVR/PEG/RBV
TW4 and TW12
– HCV RNA
Clinical Decision 2
Which regimen should Glenn receive?
12 weeks TVR/PEG/RBV
12 weeks TVR/PEG/RBV
Clinical Decision 2
Which regimen should Glenn receive?
12 weeks TVR/PEG/RBV
12 weeks TVR/PEG/RBV
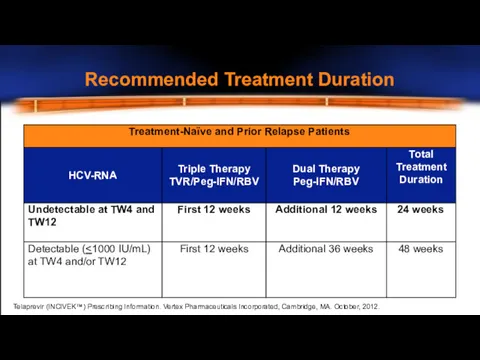
Recommended Treatment Duration
Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA.
Recommended Treatment Duration
Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA.
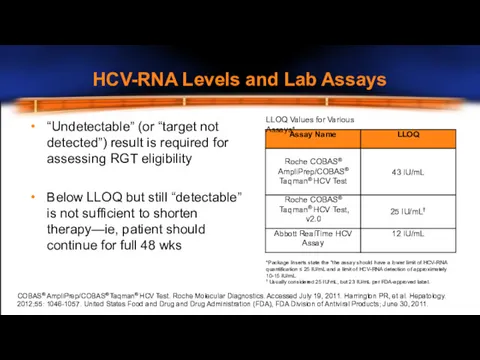
HCV-RNA Levels and Lab Assays
LLOQ Values for Various Assays*
“Undetectable” (or “target
HCV-RNA Levels and Lab Assays
LLOQ Values for Various Assays*
“Undetectable” (or “target
 Остеомиелит. Острый гематогенный остеомиелит
Остеомиелит. Острый гематогенный остеомиелит Воздушно - капельные инфекции: Скарлатина
Воздушно - капельные инфекции: Скарлатина Виды Сухожильных швов
Виды Сухожильных швов Укусы насекомых
Укусы насекомых Инфекции, передаваемые половым путем. Уголовная ответственность за заражение этими болезнями
Инфекции, передаваемые половым путем. Уголовная ответственность за заражение этими болезнями Травмы. Травматический шок
Травмы. Травматический шок Защитные функции антител
Защитные функции антител Использование КТ для диагностики травм у мелких домашних животных
Использование КТ для диагностики травм у мелких домашних животных Факторы риска и профилактика болезней пародонта, зубочелюстных аномалий у детей. (Лекция 15)
Факторы риска и профилактика болезней пародонта, зубочелюстных аномалий у детей. (Лекция 15) Синдром Ретта
Синдром Ретта Жүрек ишемия ауруы. Стенокардия
Жүрек ишемия ауруы. Стенокардия Асқазанның және ас қорыту бездерінің топографиялық анатомиясы және балалардағы ерекшеліктері
Асқазанның және ас қорыту бездерінің топографиялық анатомиясы және балалардағы ерекшеліктері Морфологические особенности крови крупного рогатого скота
Морфологические особенности крови крупного рогатого скота Беременность при туберкулезе
Беременность при туберкулезе Остановка наружного кровотечения
Остановка наружного кровотечения Управління якістю у фармацевтичній галузі. Державна система забезпечення якості лікарських засобів в Україні
Управління якістю у фармацевтичній галузі. Державна система забезпечення якості лікарських засобів в Україні Остеобластокластома челюстей. Фиброзная дисплазия челюстей
Остеобластокластома челюстей. Фиброзная дисплазия челюстей Патология пищеварительной системы
Патология пищеварительной системы Диагностика и лечение черепно–мозговой травмы
Диагностика и лечение черепно–мозговой травмы Ротавирусная инфекция
Ротавирусная инфекция Операции в области живота. Абдоминальная хирургия
Операции в области живота. Абдоминальная хирургия Перелом лодыжек
Перелом лодыжек Schizophrenia is a mental illness
Schizophrenia is a mental illness Недостаточность кровообращения: принципы фармакотерапии. Кардиотонические средства
Недостаточность кровообращения: принципы фармакотерапии. Кардиотонические средства Система методов лечебных воздействий
Система методов лечебных воздействий Динамикалык қатар. Медициналық ұйымдардағы динамикалық көрсеткішін сраптау есептеу
Динамикалык қатар. Медициналық ұйымдардағы динамикалық көрсеткішін сраптау есептеу Несеп шығару жүйесінің балалардағы ерекшеліктері
Несеп шығару жүйесінің балалардағы ерекшеліктері Общая гигиена. Климат. (Лекция 12-13)
Общая гигиена. Климат. (Лекция 12-13)