- Hemostasis

Содержание
- 2. Hemostasis („hemo”=blood; sta=„remain”) is the stoppage of bleeding, which is vitally important when blood vessels are
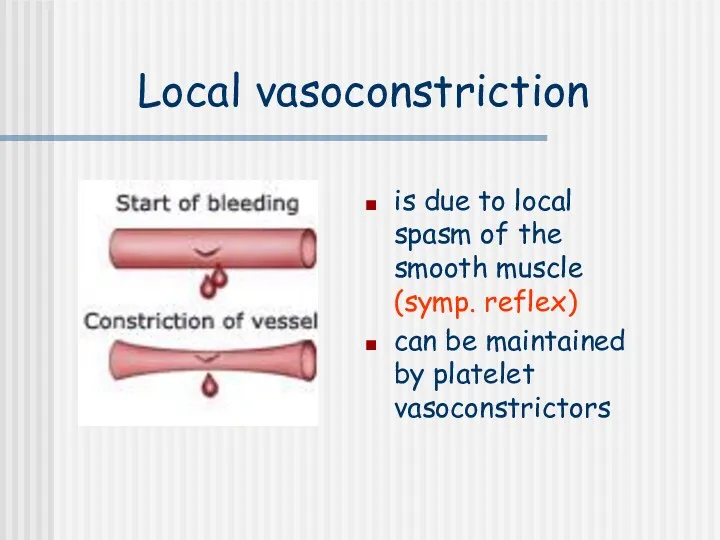
- 3. Local vasoconstriction is due to local spasm of the smooth muscle (symp. reflex) can be maintained
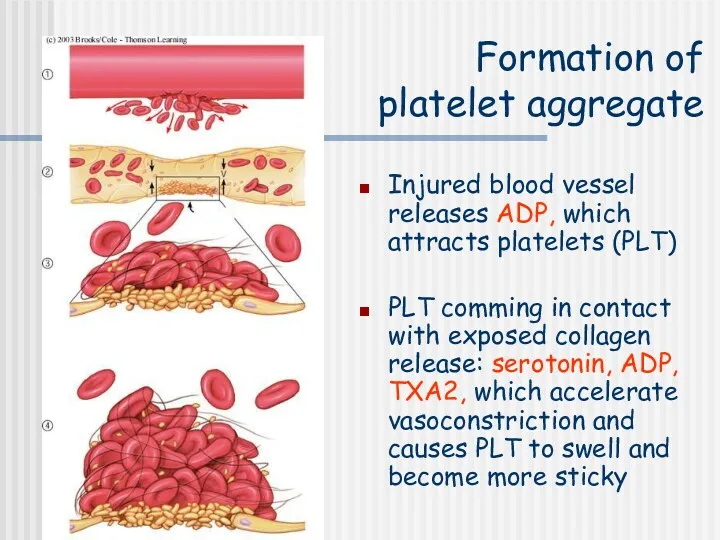
- 4. Formation of platelet aggregate Injured blood vessel releases ADP, which attracts platelets (PLT) PLT comming in
- 5. The micrograph shows activated platelets adhering to some damaged cells
- 6. Formation of blood clot In the formation of the clot, an enzyme called thrombin converts fibrinogen
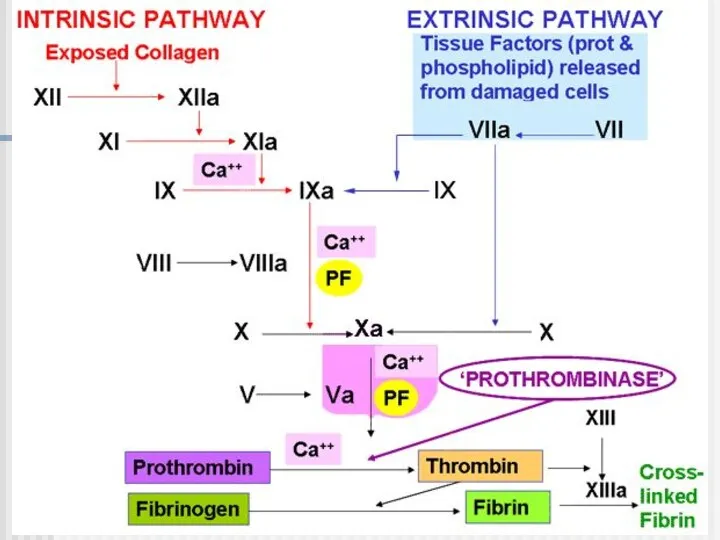
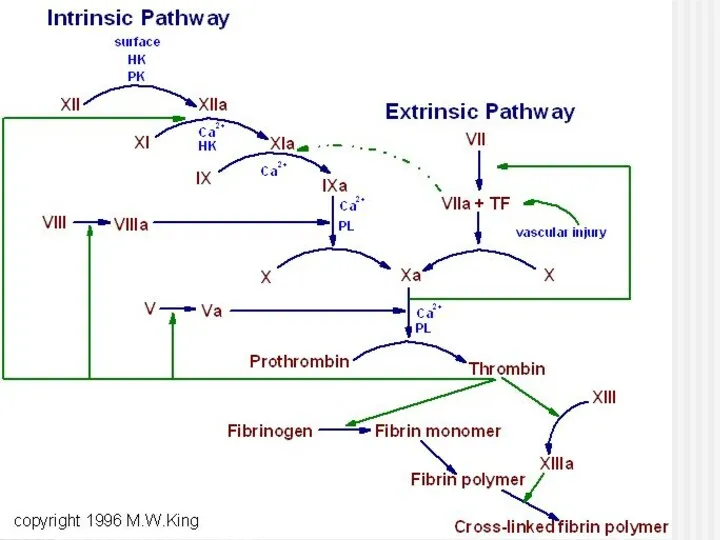
- 7. The intrinsic system is more complex and present only in „higher” life forms (e.g. birds and
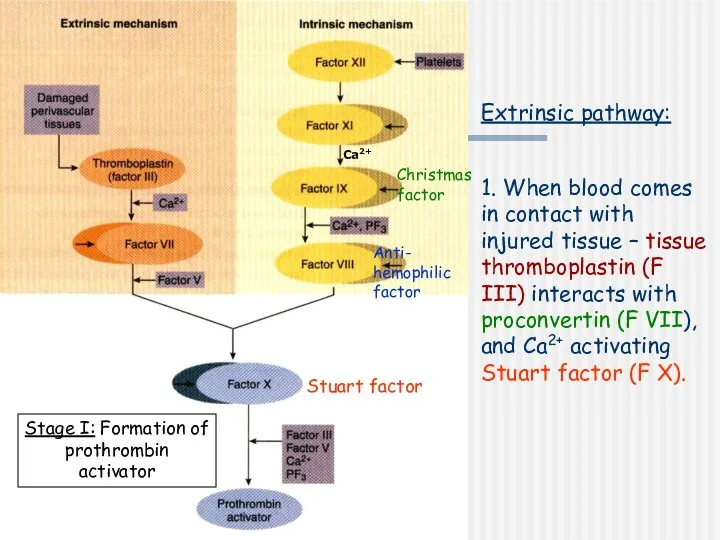
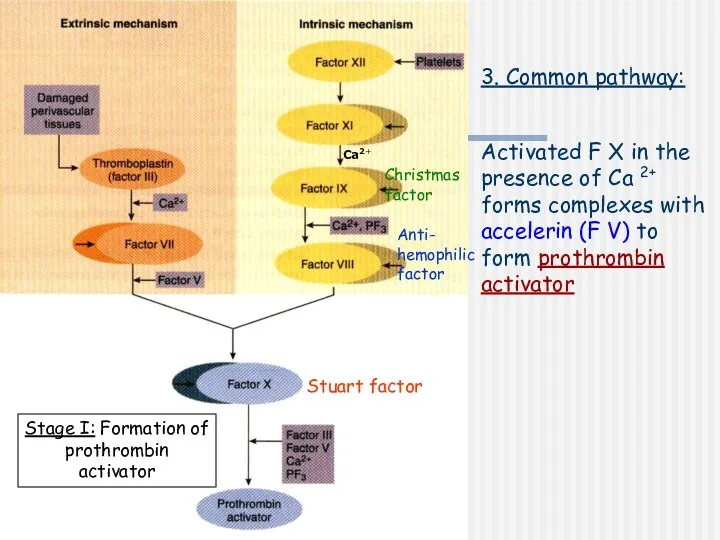
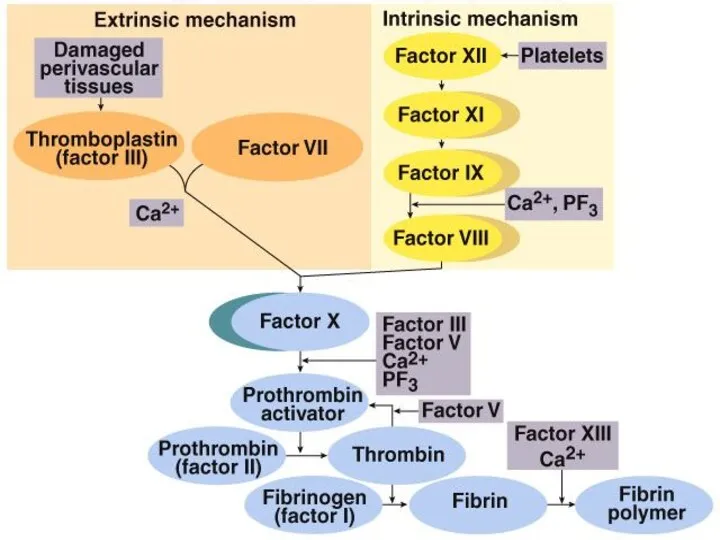
- 8. Extrinsic pathway: 1. When blood comes in contact with injured tissue – tissue thromboplastin (F III)
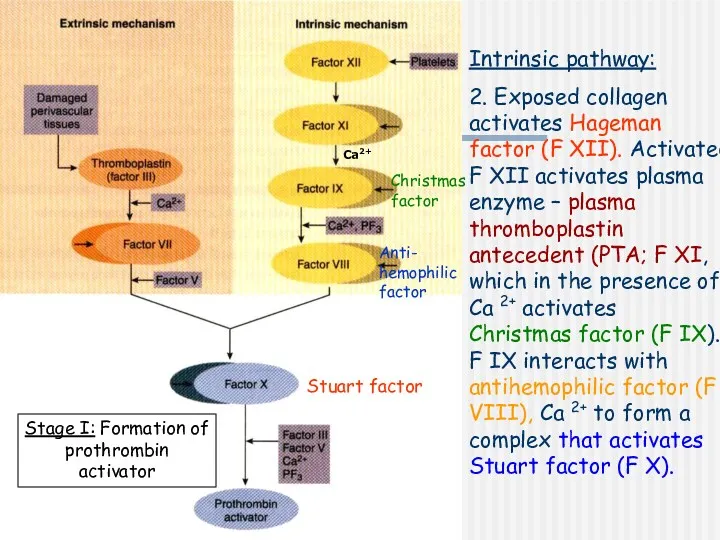
- 9. Intrinsic pathway: 2. Exposed collagen activates Hageman factor (F XII). Activated F XII activates plasma enzyme
- 10. Stage I: Formation of prothrombin activator 3. Common pathway: Activated F X in the presence of
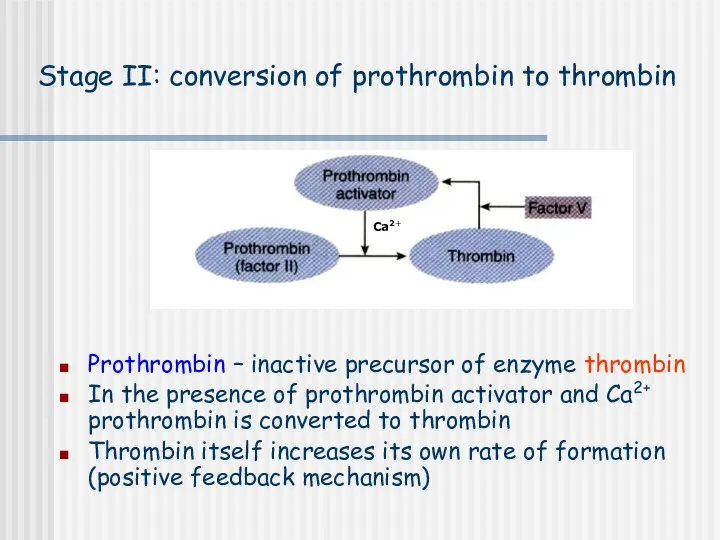
- 12. Stage II: conversion of prothrombin to thrombin Prothrombin – inactive precursor of enzyme thrombin In the
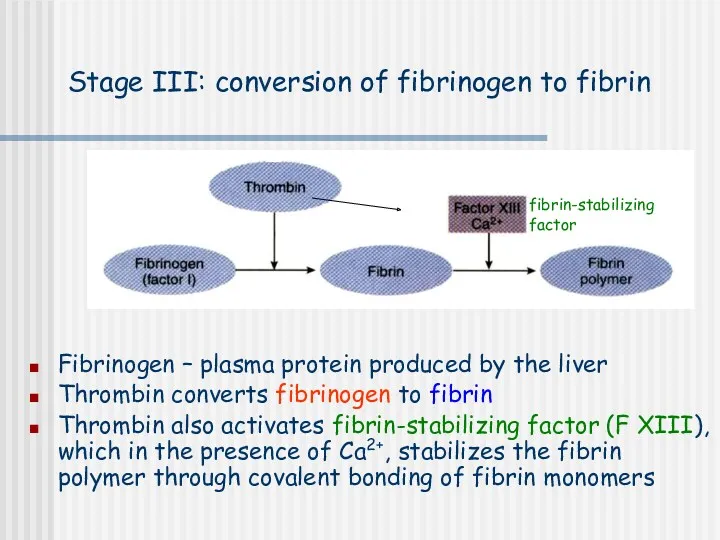
- 13. Stage III: conversion of fibrinogen to fibrin Fibrinogen – plasma protein produced by the liver Thrombin
- 14. Calcium ions Are required for promotion and acceleration of almost all blood clotting reactions Except: activation
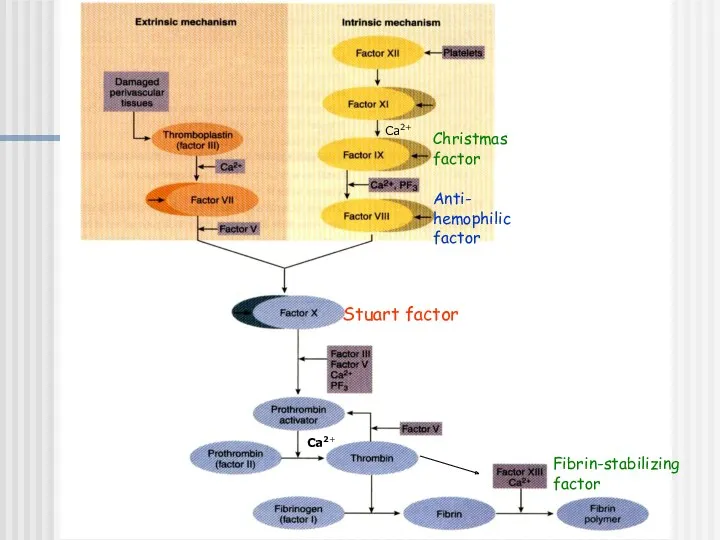
- 15. Ca2+ Ca2+ Christmas factor Anti- hemophilic factor Stuart factor Fibrin-stabilizing factor
- 18. Fibrinolysis
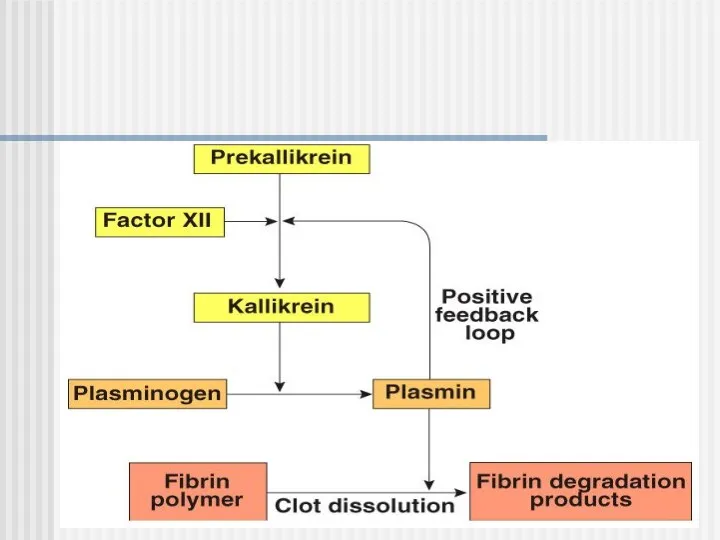
- 19. Clot Dissolution Plasmin is formed from plasminogen - enzyme called activator (e.g. enzymes from urine, tears,
- 21. Anticoagulants Hirudo medicinalis produce Hirudin that inhibits Thrombin
- 22. Anticoagulants Although tissue breakdown and platelets destruction are normal events in the absence of trauma, intravascular
- 23. Natural anticoagulants Antithrombin III – inhibits factor X and thrombin Heparin from basophils and mast cells
- 24. Abnormalities of hemostasis
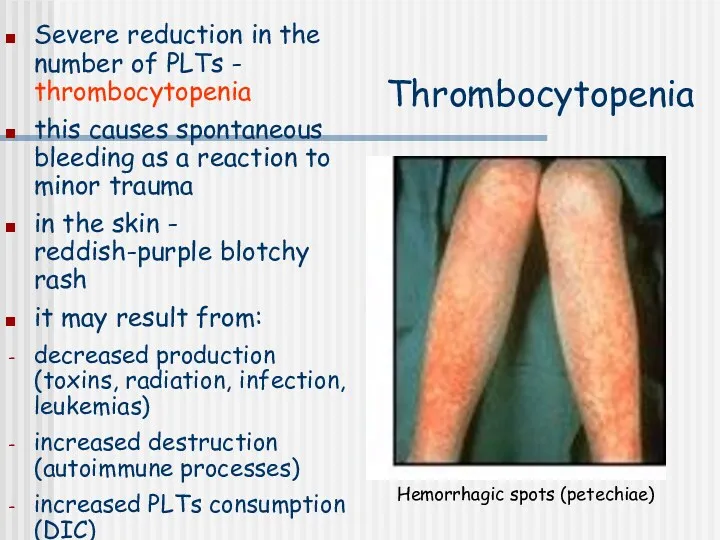
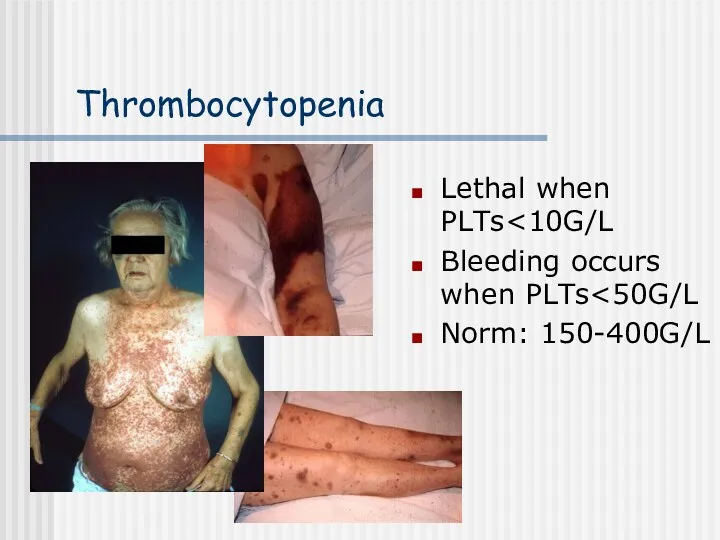
- 25. Thrombocytopenia Severe reduction in the number of PLTs - thrombocytopenia this causes spontaneous bleeding as a
- 26. Thrombocytopenia Lethal when PLTs Bleeding occurs when PLTs Norm: 150-400G/L
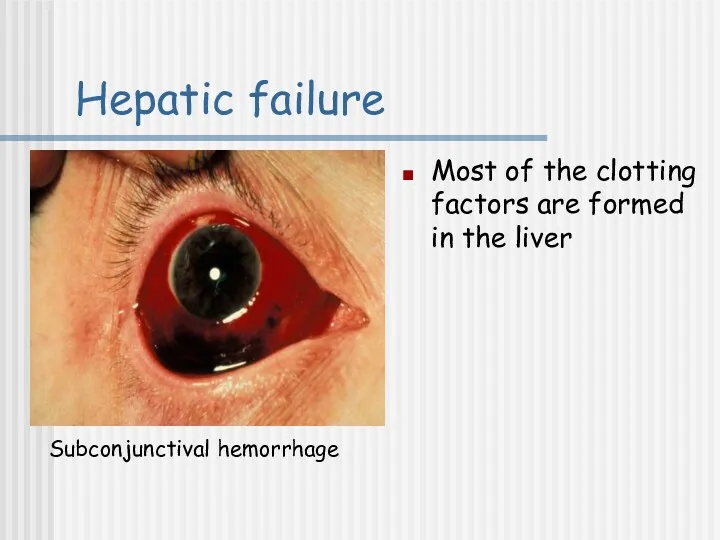
- 27. Hepatic failure Most of the clotting factors are formed in the liver Subconjunctival hemorrhage
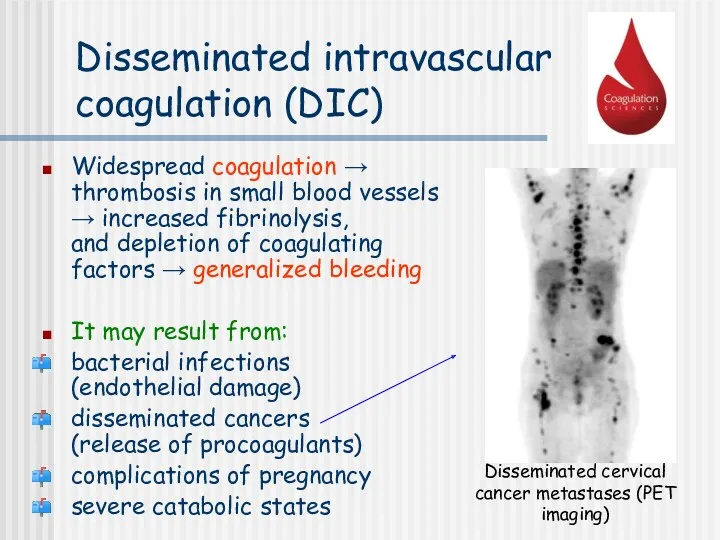
- 28. Disseminated intravascular coagulation (DIC) Widespread coagulation → thrombosis in small blood vessels → increased fibrinolysis, and
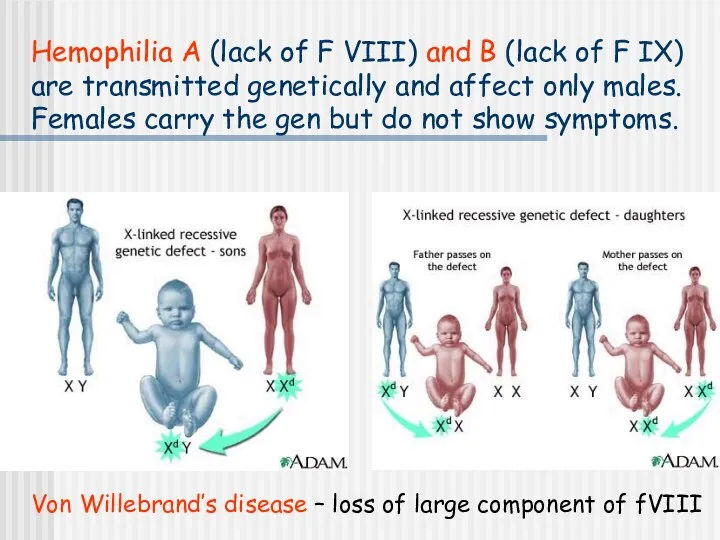
- 29. Hemophilia A (lack of F VIII) and B (lack of F IX) are transmitted genetically and
- 30. Hemophilia A (lack of F VIII; 85%) Spontaneous or traumatic subcutaneous bleeding Blood in the urine
- 31. Son of the last Tsar of Russia – Aleksy Romanow suffered from Hemophilia A
- 32. Tests of coagulation
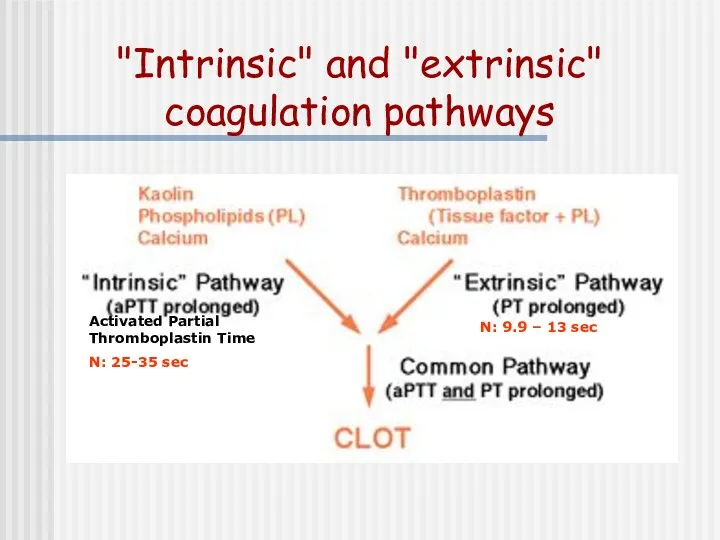
- 33. "Intrinsic" and "extrinsic" coagulation pathways N: 9.9 – 13 sec Activated Partial Thromboplastin Time N: 25-35
- 34. Prothrombin time (PT) test – norm 11 -15 sec evaluates extrinsic system (VII, X, V, II,
- 35. International Normalised Ratio (INR) The result for the PT is expressed as a ratio (prothrombin clotting
- 36. Activated Partial Thromboplastin Time test (aPTT) – norm: 25-35 s; evaluates intrinsic system (VIII, IX, XI,
- 37. Thrombin time (TT) – norm: 14-15 sec Prolonged TT: Heparin (much more sensitive to heparin than
- 38. Selected causes of abnormal coagulation tests
- 39. "Intrinsic" and "extrinsic" coagulation pathways N: 9.9 – 13 sec Activated Partial Thromboplastin Time N: 25-35
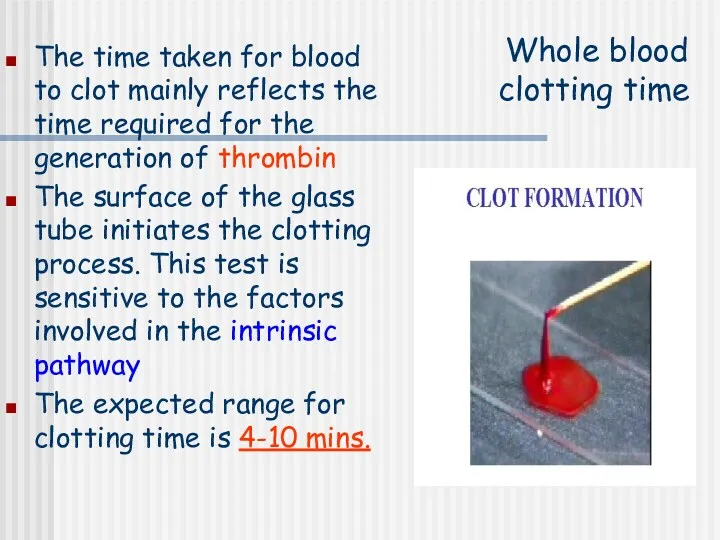
- 40. Whole blood clotting time The time taken for blood to clot mainly reflects the time required
- 41. Whole blood clotting time – procedure: Clean the tip of the finger with an alcohol Prick
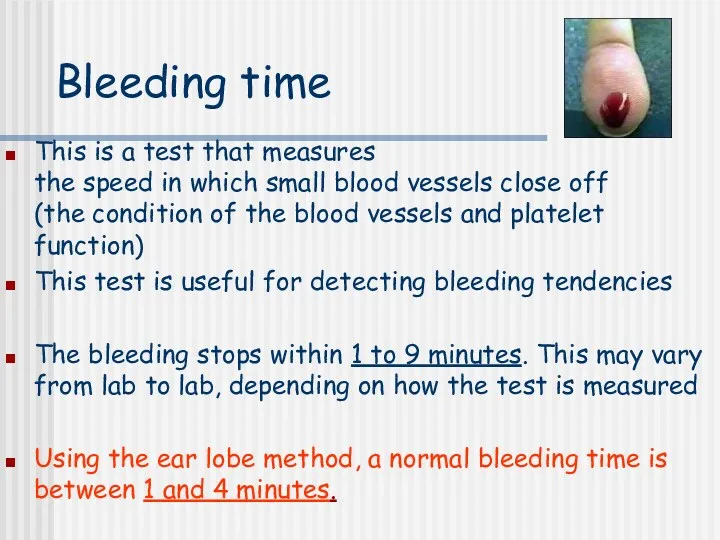
- 42. Bleeding time This is a test that measures the speed in which small blood vessels close
- 43. Bleeding time – procedure: Clean the earlobe with an alcohol Prick the earlobe with an automatic
- 44. Abnormal Bleeding Time Prolonged bleeding time may indicate: A vascular (blood vessel) defect A platelet function
- 45. http://www.medicine.mcgill.ca/physio/vlab212D/bloodlab/images/clottime5.mpg
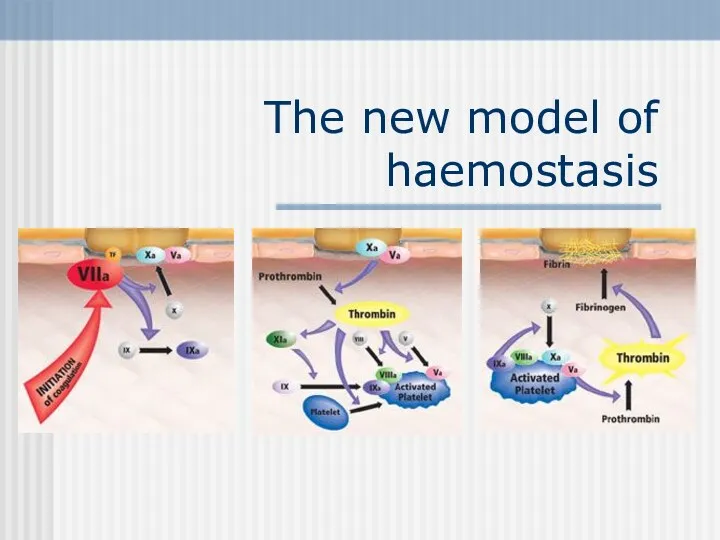
- 47. The new model of haemostasis
- 48. Injury of vessels wall leads to contact between blood and subendothelial cells FXa binds to FVa
- 49. 2. Amplification phase Activated platelets bind FVa, FVIIIa and FIXa
- 50. 3. Propagation phase The “thrombin burst” leads to the formation of a stable fibrin clot.
- 51. Summary: Haemostasis starts with the interaction between TF and FVIIa on the surface of subendothelial cells.
- 52. NovoSeven® Mode of Action Eptacog alfa (activated) The thrombin burst leads to the formation of a
- 53. Conclusion: • In high doses rFVIIa binds to the surface of the locally activated platelets where
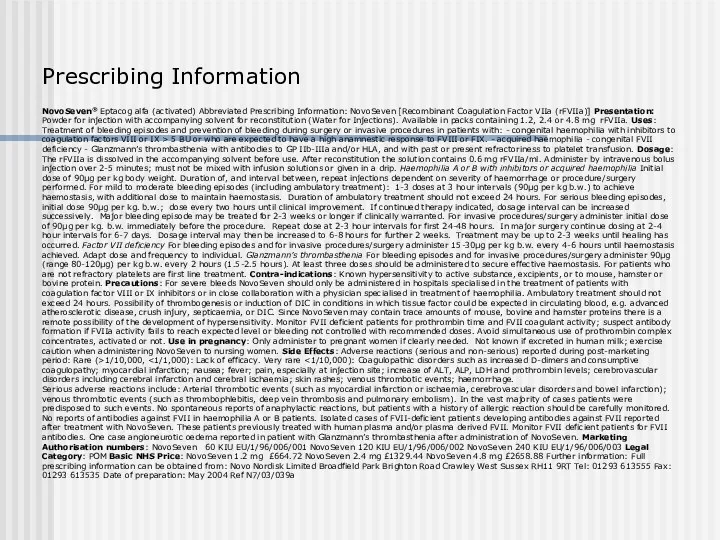
- 54. Prescribing Information NovoSeven® Eptacog alfa (activated) Abbreviated Prescribing Information: NovoSeven [Recombinant Coagulation Factor VIIa (rFVIIa)] Presentation:
- 55. A 35-year-old man complains of chronic physical fatigue, which began 3-4 weeks ago. He said he
- 56. Laboratory findings revealed the following:
- 57. Case history questions: What general medical condition is suggested by the person’s symptoms? What fundamental change
- 59. Скачать презентацию
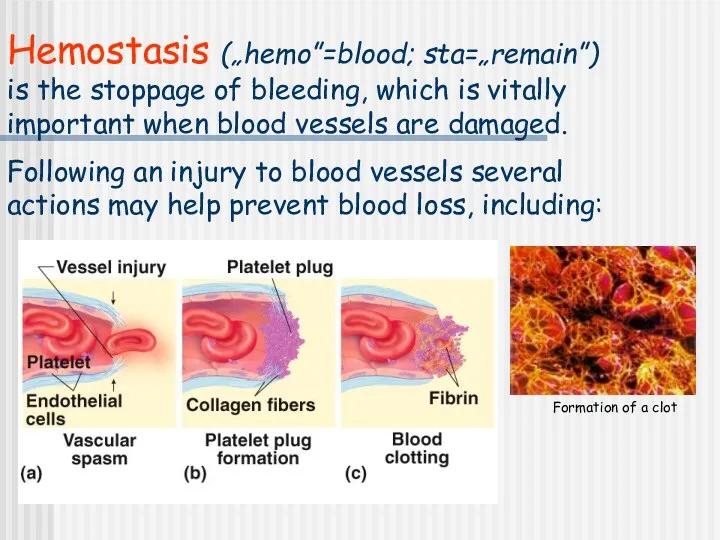
Hemostasis („hemo”=blood; sta=„remain”) is the stoppage of bleeding, which is vitally
Hemostasis („hemo”=blood; sta=„remain”) is the stoppage of bleeding, which is vitally
Local vasoconstriction
is due to local spasm of the smooth muscle (symp.
Local vasoconstriction
is due to local spasm of the smooth muscle (symp.
Formation of
platelet aggregate
Injured blood vessel releases ADP, which attracts platelets
Formation of
platelet aggregate
Injured blood vessel releases ADP, which attracts platelets
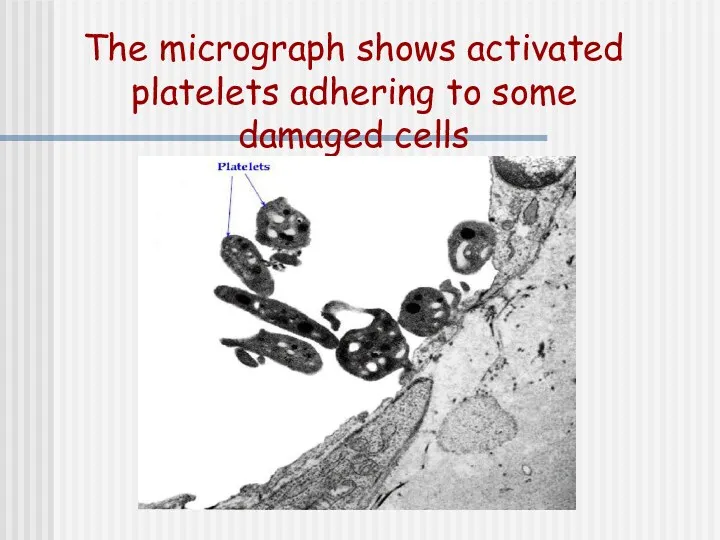
The micrograph shows activated platelets adhering to some damaged cells
The micrograph shows activated platelets adhering to some damaged cells
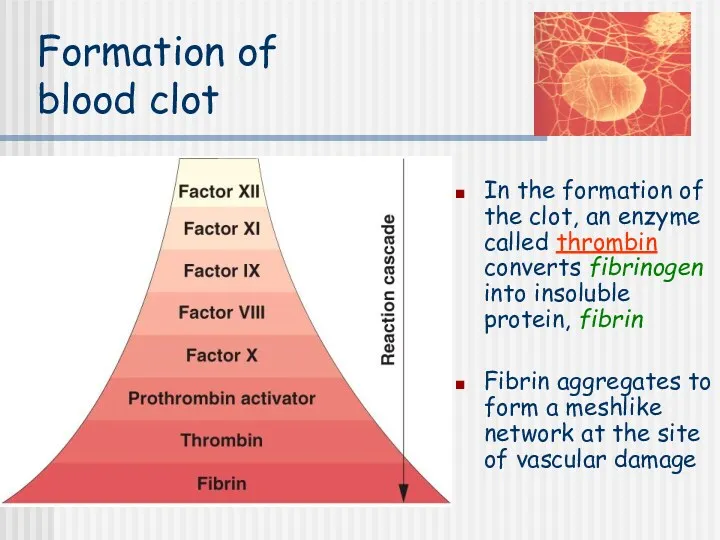
Formation of blood clot
In the formation of the clot, an enzyme
Formation of blood clot
In the formation of the clot, an enzyme
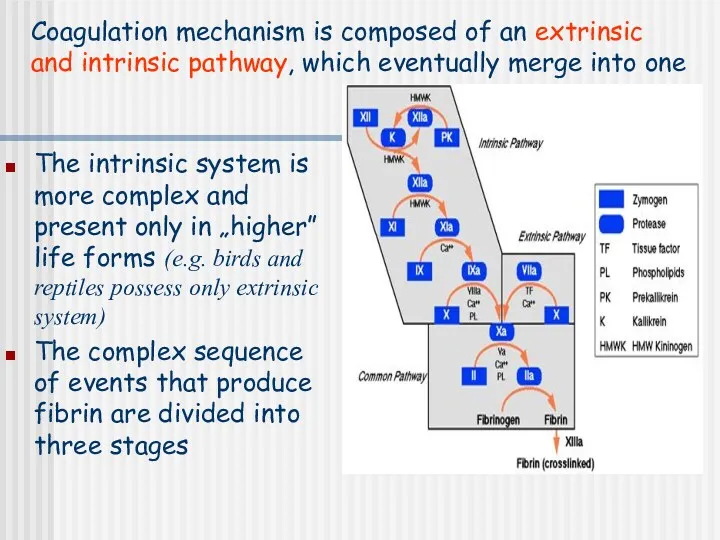
The intrinsic system is more complex and present only in „higher”
Extrinsic pathway:
1. When blood comes in contact with injured tissue –
Extrinsic pathway:
1. When blood comes in contact with injured tissue –
Intrinsic pathway:
2. Exposed collagen activates Hageman factor (F XII). Activated F
Intrinsic pathway:
2. Exposed collagen activates Hageman factor (F XII). Activated F
Stage I: Formation of prothrombin activator
3. Common pathway:
Activated F X in
Stage I: Formation of prothrombin activator
3. Common pathway:
Activated F X in
Stage II: conversion of prothrombin to thrombin
Prothrombin – inactive precursor of
Stage II: conversion of prothrombin to thrombin
Prothrombin – inactive precursor of
Stage III: conversion of fibrinogen to fibrin
Fibrinogen – plasma protein produced
Stage III: conversion of fibrinogen to fibrin
Fibrinogen – plasma protein produced
Calcium ions
Are required for promotion and acceleration of almost all blood
Calcium ions
Are required for promotion and acceleration of almost all blood
Ca2+
Ca2+
Christmas factor
Anti- hemophilic factor
Stuart factor
Fibrin-stabilizing factor
Ca2+
Ca2+
Christmas factor
Anti- hemophilic factor
Stuart factor
Fibrin-stabilizing factor
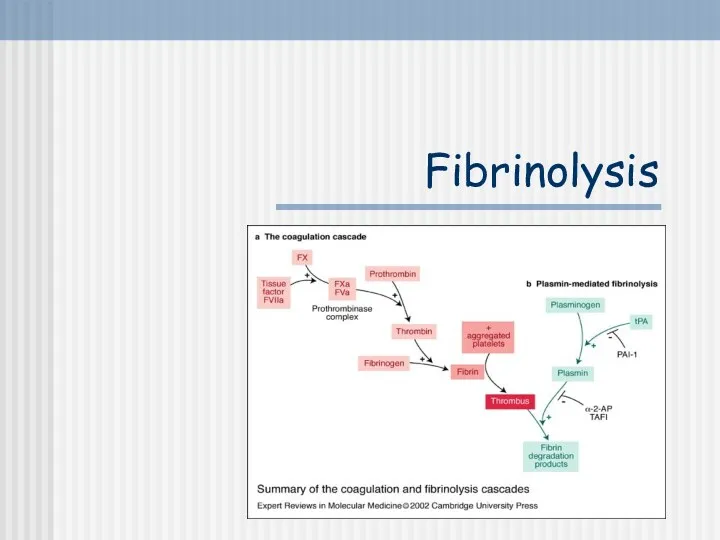
Fibrinolysis
Fibrinolysis
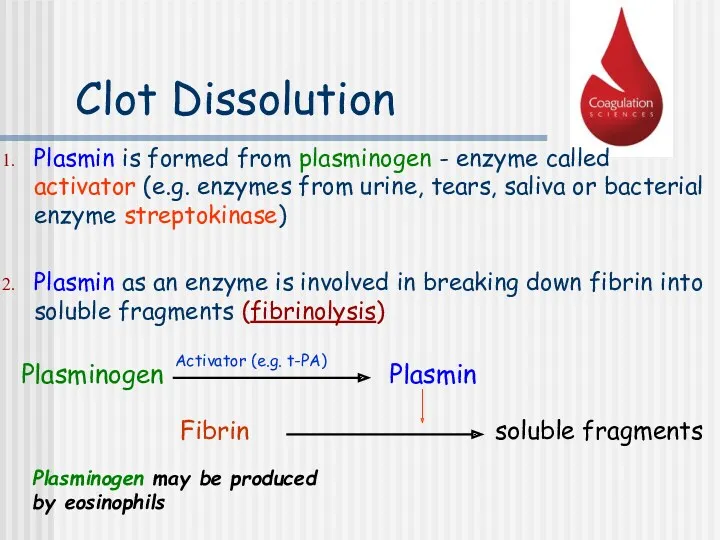
Clot Dissolution
Plasmin is formed from plasminogen - enzyme called activator (e.g.
Clot Dissolution
Plasmin is formed from plasminogen - enzyme called activator (e.g.
Anticoagulants
Hirudo medicinalis produce Hirudin that inhibits Thrombin
Anticoagulants
Hirudo medicinalis produce Hirudin that inhibits Thrombin
Anticoagulants
Although tissue breakdown and platelets destruction are normal events in the
Anticoagulants
Although tissue breakdown and platelets destruction are normal events in the
Natural anticoagulants
Antithrombin III – inhibits factor X and thrombin
Heparin from
Natural anticoagulants
Antithrombin III – inhibits factor X and thrombin
Heparin from
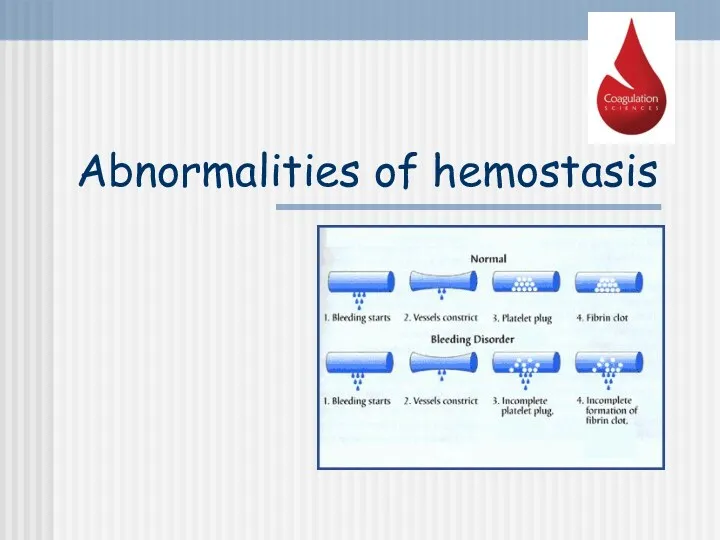
Abnormalities of hemostasis
Abnormalities of hemostasis
Thrombocytopenia
Severe reduction in the number of PLTs - thrombocytopenia
this causes spontaneous
Thrombocytopenia
Severe reduction in the number of PLTs - thrombocytopenia
this causes spontaneous
Thrombocytopenia
Lethal when PLTs<10G/L
Bleeding occurs when PLTs<50G/L
Norm: 150-400G/L
Thrombocytopenia
Lethal when PLTs<10G/L
Bleeding occurs when PLTs<50G/L
Norm: 150-400G/L
Hepatic failure
Most of the clotting factors are formed in the liver
Subconjunctival
Hepatic failure
Most of the clotting factors are formed in the liver
Subconjunctival
Disseminated intravascular coagulation (DIC)
Widespread coagulation → thrombosis in small blood vessels
Disseminated intravascular coagulation (DIC)
Widespread coagulation → thrombosis in small blood vessels
Hemophilia A (lack of F VIII) and B (lack of F
Hemophilia A (lack of F VIII) and B (lack of F
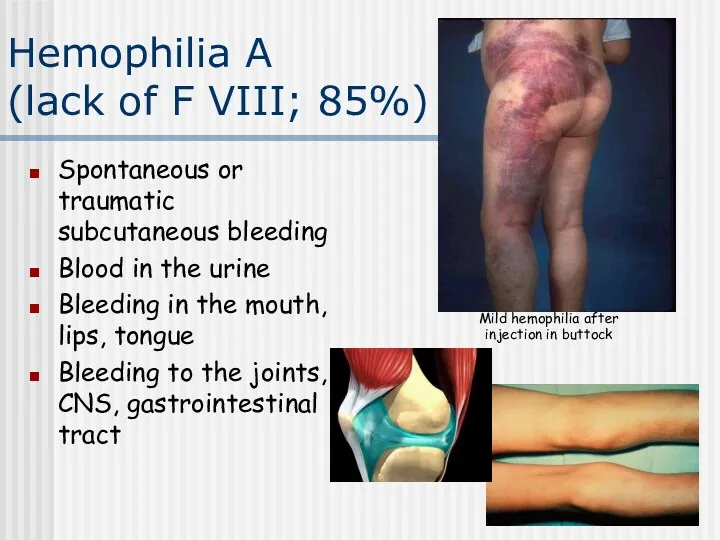
Hemophilia A
(lack of F VIII; 85%)
Spontaneous or traumatic subcutaneous bleeding
Blood
Hemophilia A
(lack of F VIII; 85%)
Spontaneous or traumatic subcutaneous bleeding
Blood

Son of the last Tsar of Russia – Aleksy Romanow suffered
Son of the last Tsar of Russia – Aleksy Romanow suffered
Tests of coagulation
Tests of coagulation
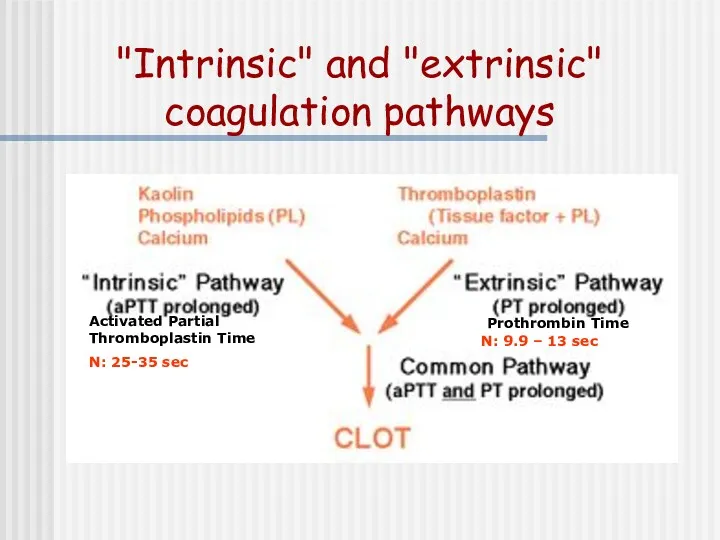
"Intrinsic" and "extrinsic" coagulation pathways
N: 9.9 – 13 sec
Activated Partial Thromboplastin
"Intrinsic" and "extrinsic" coagulation pathways
N: 9.9 – 13 sec
Activated Partial Thromboplastin
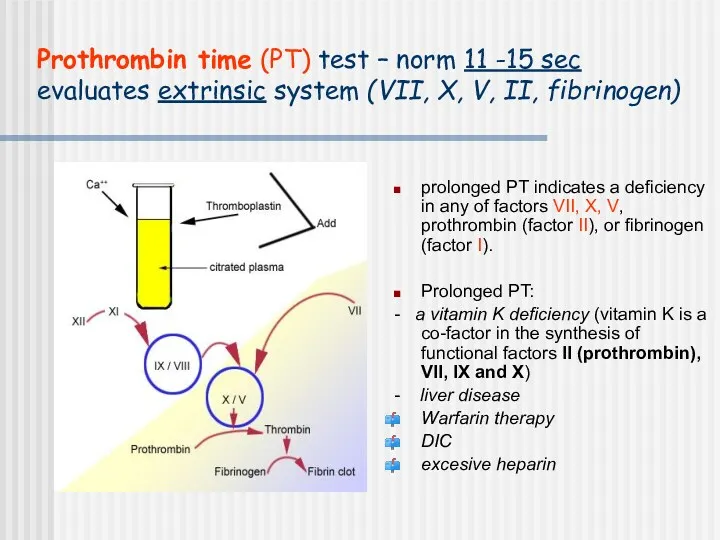
Prothrombin time (PT) test – norm 11 -15 sec
evaluates extrinsic system
Prothrombin time (PT) test – norm 11 -15 sec evaluates extrinsic system
International Normalised Ratio (INR)
The result for the PT is expressed as
International Normalised Ratio (INR)
The result for the PT is expressed as
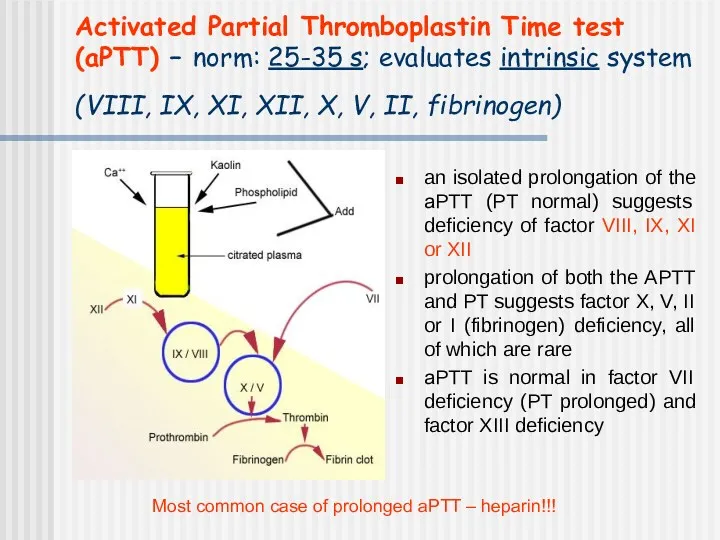
Activated Partial Thromboplastin Time test (aPTT) – norm: 25-35 s; evaluates
Activated Partial Thromboplastin Time test (aPTT) – norm: 25-35 s; evaluates
Thrombin time (TT) – norm: 14-15 sec
Prolonged TT:
Heparin (much more sensitive
Thrombin time (TT) – norm: 14-15 sec
Prolonged TT:
Heparin (much more sensitive
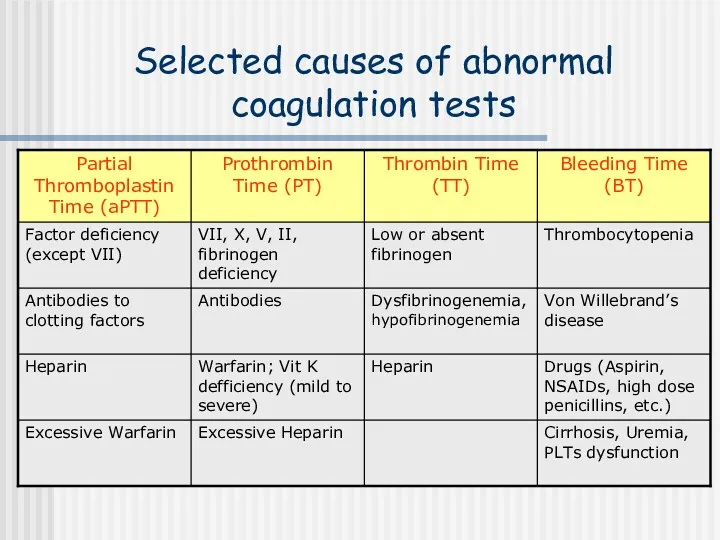
Selected causes of abnormal coagulation tests
Selected causes of abnormal coagulation tests
"Intrinsic" and "extrinsic" coagulation pathways
N: 9.9 – 13 sec
Activated Partial Thromboplastin
"Intrinsic" and "extrinsic" coagulation pathways
N: 9.9 – 13 sec
Activated Partial Thromboplastin
Whole blood
clotting time
The time taken for blood to clot mainly
Whole blood
clotting time
The time taken for blood to clot mainly
Whole blood clotting time – procedure:
Clean the tip of the finger
Whole blood clotting time – procedure:
Clean the tip of the finger
Bleeding time
This is a test that measures the speed in
Bleeding time
This is a test that measures the speed in
Bleeding time – procedure:
Clean the earlobe with an alcohol
Prick
Bleeding time – procedure:
Clean the earlobe with an alcohol
Prick
Abnormal Bleeding Time
Prolonged bleeding time may indicate:
A vascular (blood vessel)
Abnormal Bleeding Time
Prolonged bleeding time may indicate:
A vascular (blood vessel)

http://www.medicine.mcgill.ca/physio/vlab212D/bloodlab/images/clottime5.mpg
http://www.medicine.mcgill.ca/physio/vlab212D/bloodlab/images/clottime5.mpg
The new model of haemostasis
The new model of haemostasis
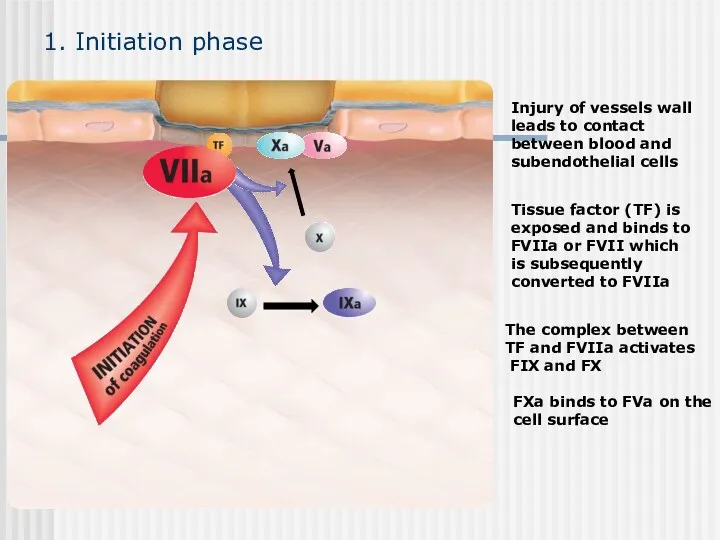
Injury of vessels wall
leads to contact
between blood and
subendothelial cells
FXa
Injury of vessels wall
leads to contact
between blood and
subendothelial cells
FXa
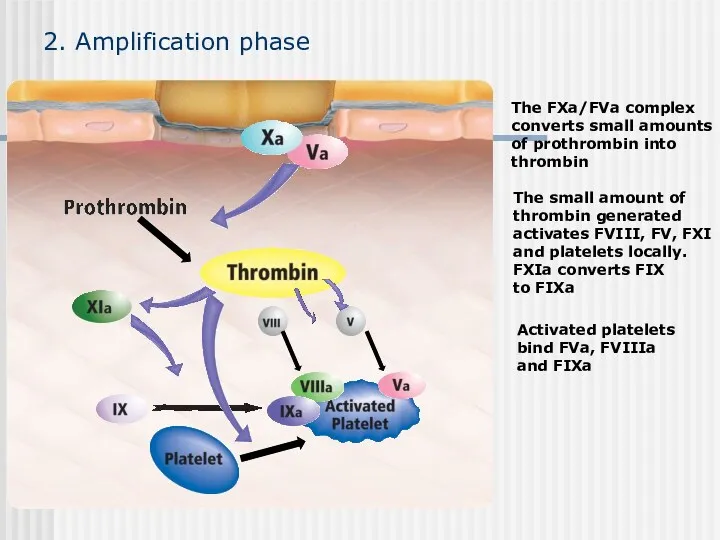
2. Amplification phase
Activated platelets
bind FVa, FVIIIa
and FIXa
2. Amplification phase
Activated platelets
bind FVa, FVIIIa
and FIXa
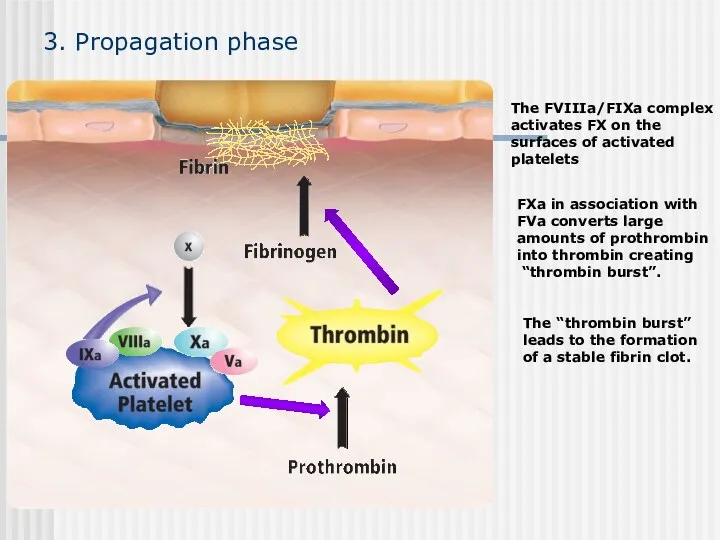
3. Propagation phase
The “thrombin burst”
leads to the formation
of a stable fibrin
3. Propagation phase
The “thrombin burst” leads to the formation of a stable fibrin
Summary:
Haemostasis starts with the interaction between TF and FVIIa on
Summary:
Haemostasis starts with the interaction between TF and FVIIa on
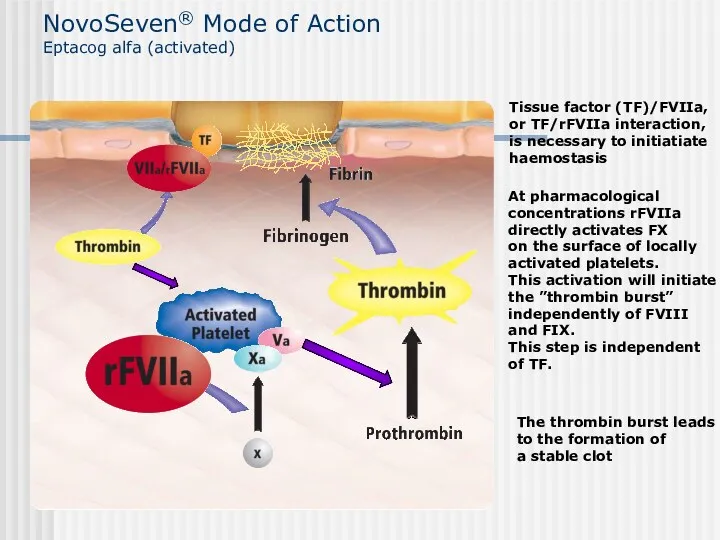
NovoSeven® Mode of Action
Eptacog alfa (activated)
The thrombin burst leads
to the
NovoSeven® Mode of Action
Eptacog alfa (activated)
The thrombin burst leads to the
Conclusion:
• In high doses rFVIIa binds to the surface of the
Conclusion:
• In high doses rFVIIa binds to the surface of the
Prescribing Information
NovoSeven® Eptacog alfa (activated) Abbreviated Prescribing Information: NovoSeven [Recombinant Coagulation
Prescribing Information
NovoSeven® Eptacog alfa (activated) Abbreviated Prescribing Information: NovoSeven [Recombinant Coagulation
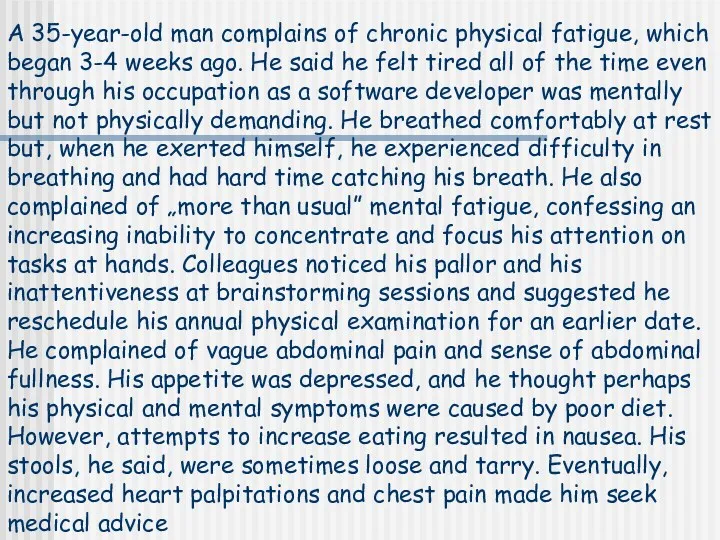
A 35-year-old man complains of chronic physical fatigue, which began 3-4
A 35-year-old man complains of chronic physical fatigue, which began 3-4
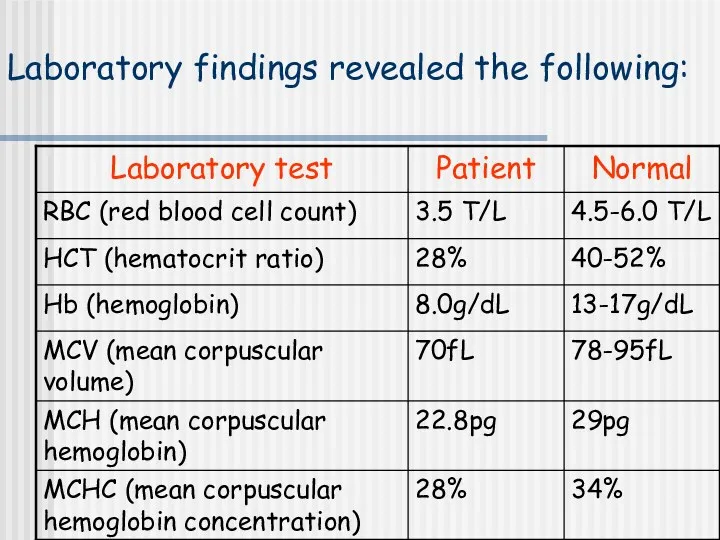
Laboratory findings revealed the following:
Laboratory findings revealed the following:
Case history questions:
What general medical condition is suggested by the person’s
Case history questions:
What general medical condition is suggested by the person’s
 Плевральный выпот
Плевральный выпот Заболевания органов дыхания у детей
Заболевания органов дыхания у детей Пневмония. Этиология. Принципы лечения
Пневмония. Этиология. Принципы лечения Тактика наружной терапии атопического дерматита: современный взгляд
Тактика наружной терапии атопического дерматита: современный взгляд Мерез. Мерез ауруының өзектілігі
Мерез. Мерез ауруының өзектілігі Дәлелді медицина – дәрілік заттарды қолдану құралы түрінде. Дәрілік заттарды қате жарнамалаудың белгілері
Дәлелді медицина – дәрілік заттарды қолдану құралы түрінде. Дәрілік заттарды қате жарнамалаудың белгілері Диагностика и малоинвазивные методы лечения жидкостных образований брюшной полости
Диагностика и малоинвазивные методы лечения жидкостных образований брюшной полости Ортодонтическое лечение
Ортодонтическое лечение Современные аспекты комплексного сестринского ухода за пациентами с хроническим гастритом
Современные аспекты комплексного сестринского ухода за пациентами с хроническим гастритом Наркоз (общее обезболивание, общая анестезия)
Наркоз (общее обезболивание, общая анестезия) Современные алгоритмы лечения сахарного диабета 2 типа
Современные алгоритмы лечения сахарного диабета 2 типа Иммунопатология и аллергия
Иммунопатология и аллергия Лучевая диагностика заболеваний пищеварительного тракта
Лучевая диагностика заболеваний пищеварительного тракта Анафилактический шок
Анафилактический шок Психолого-медико-педагогическая комиссия
Психолого-медико-педагогическая комиссия Выделительная система
Выделительная система Заболевания органов мочевыводящей системы
Заболевания органов мочевыводящей системы Хронический холецистит. Классификация. Диагностика и лечение некалькулезного и калькулезного холецистита
Хронический холецистит. Классификация. Диагностика и лечение некалькулезного и калькулезного холецистита Омыртқаның зақымдалуы.Жіктемесі. диагностикасы.емі
Омыртқаның зақымдалуы.Жіктемесі. диагностикасы.емі Кора полушарий головного мозга. Расстройства высших корковых функций
Кора полушарий головного мозга. Расстройства высших корковых функций Об утверждении санитарных норм СанПин противоэпидемических мероприятий в том числе и работе с медицинскими отходами
Об утверждении санитарных норм СанПин противоэпидемических мероприятий в том числе и работе с медицинскими отходами Предмет и задачи токсикологии
Предмет и задачи токсикологии Доброкачественные и злокачественные новообразования вульвы
Доброкачественные и злокачественные новообразования вульвы Железодефицитные анемии у новорожденных современные возможности профилактики и лечения
Железодефицитные анемии у новорожденных современные возможности профилактики и лечения Геморрагиялық шок
Геморрагиялық шок Спадкові хвороби
Спадкові хвороби Организация медицинского обеспечения населения в чрезвычайных ситуациях
Организация медицинского обеспечения населения в чрезвычайных ситуациях СӨЖ. Глаукома
СӨЖ. Глаукома