- Hypoglycemia and insulinoma

Содержание
- 2. Glucose metabolism
- 3. Plasma glucose concentration in the fasting state(insulin low glucagon high) Dependent on net glucose influx –
- 4. Gluconeogenetic substrates and metabolism in prolonged fasting Lactate synthesized in muscle released into plasma and converted
- 5. Cori and alanine –pyruvate cycle
- 6. Plasma glucose in fed state(insuin high glucagon low) and exercise Fed state Dependent on net glucose
- 7. Hypoglycemia Imbalance between glucose production and utilization. Clinical hypoglycemia is a plasma glucose concentration low enough
- 8. Normal response to hypoglycemia
- 9. Symptoms of hypoglycemia Autonomic: Palpitation ,tremor, anxiety- adrenergic. Sweating , hunger and paresthesias-cholinergic. Neuroglycopenic: Cognitive, behavioral
- 10. Acute treatment PO 15 g carbohydrates with re-evalution after 15 minutes. Severe hypoglycemia (event requiring assistance
- 11. Evaluation(1) Reliable glucose test in plasma(not only by glucometer!) Whipple triade Fasting or reactive : postprandial
- 12. Evaluation(2) Cortisol and growth hormone deficiency. Autonomic failure. Autoimmune hypoglycemia. Reactive hypoglycemia : 1)In patients with
- 13. Gold standard:72 hours fast protocol Recommended to admit to the hospital and supervise. Stop all medications
- 14. Interpretation
- 15. Insulinoma 1:250.000 individuals. 90% benign. Usually sporadic and solitary ,may be part of MEN1. Evenly distributed
- 16. Insulinoma in the tail of pancreas on MRI
- 17. Malignant insulinoma with metastasis to liver on somatostatin scan
- 19. Скачать презентацию
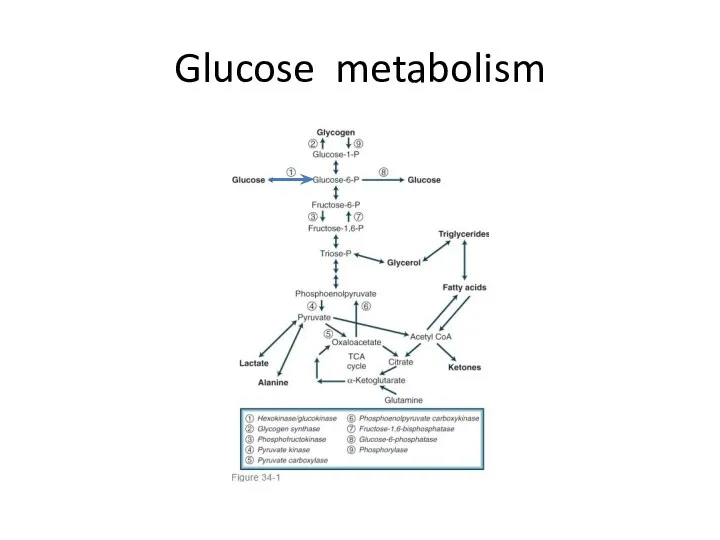
Glucose metabolism
Glucose metabolism
Plasma glucose concentration in the fasting state(insulin low glucagon high)
Dependent
Plasma glucose concentration in the fasting state(insulin low glucagon high)
Dependent
Gluconeogenetic substrates and metabolism in prolonged fasting
Lactate synthesized in muscle
Gluconeogenetic substrates and metabolism in prolonged fasting
Lactate synthesized in muscle
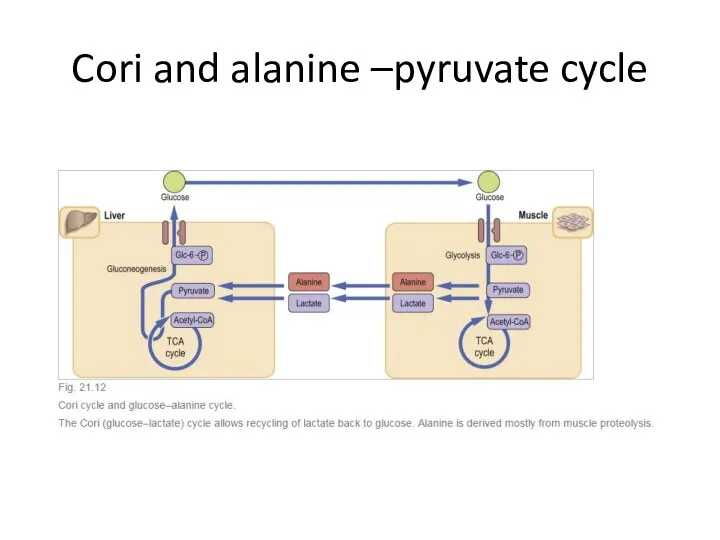
Cori and alanine –pyruvate cycle
Cori and alanine –pyruvate cycle
Plasma glucose in fed state(insuin high glucagon low) and exercise
Fed state
Dependent
Plasma glucose in fed state(insuin high glucagon low) and exercise
Fed state
Dependent
Hypoglycemia
Imbalance between glucose production and utilization.
Clinical hypoglycemia is a plasma glucose
Hypoglycemia
Imbalance between glucose production and utilization.
Clinical hypoglycemia is a plasma glucose
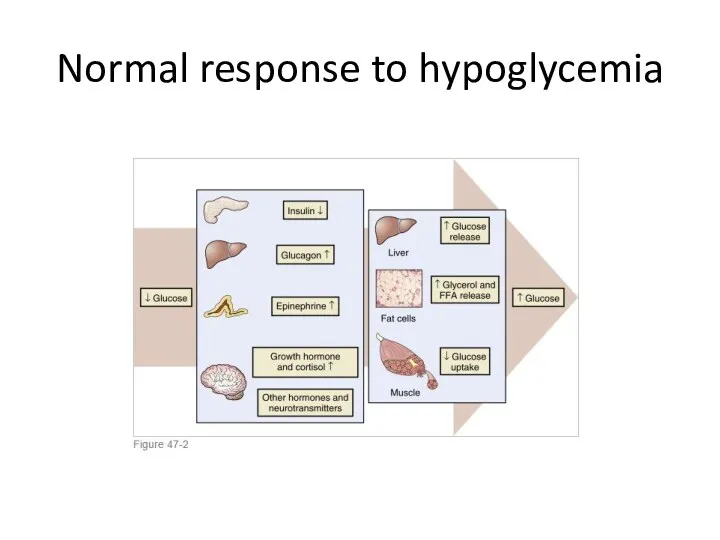
Normal response to hypoglycemia
Normal response to hypoglycemia
Symptoms of hypoglycemia
Autonomic:
Palpitation ,tremor, anxiety- adrenergic.
Sweating , hunger and paresthesias-cholinergic.
Neuroglycopenic:
Cognitive,
Symptoms of hypoglycemia
Autonomic:
Palpitation ,tremor, anxiety- adrenergic.
Sweating , hunger and paresthesias-cholinergic.
Neuroglycopenic:
Cognitive,
Acute treatment
PO 15 g carbohydrates with re-evalution after 15 minutes.
Severe
Acute treatment
PO 15 g carbohydrates with re-evalution after 15 minutes.
Severe
Evaluation(1)
Reliable glucose test in plasma(not only by glucometer!)
Whipple triade
Fasting or reactive
Evaluation(1)
Reliable glucose test in plasma(not only by glucometer!)
Whipple triade
Fasting or reactive
Evaluation(2)
Cortisol and growth hormone deficiency.
Autonomic failure.
Autoimmune hypoglycemia.
Reactive hypoglycemia :
Evaluation(2)
Cortisol and growth hormone deficiency.
Autonomic failure.
Autoimmune hypoglycemia.
Reactive hypoglycemia :
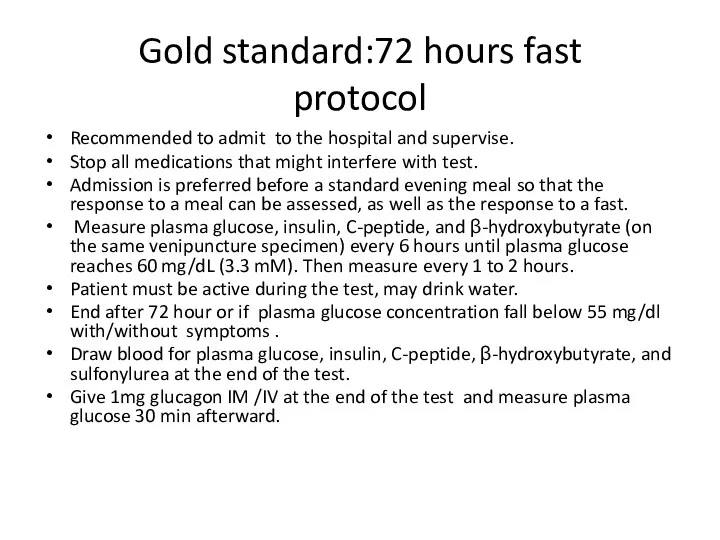
Gold standard:72 hours fast
protocol
Recommended to admit to the hospital and
Gold standard:72 hours fast
protocol
Recommended to admit to the hospital and
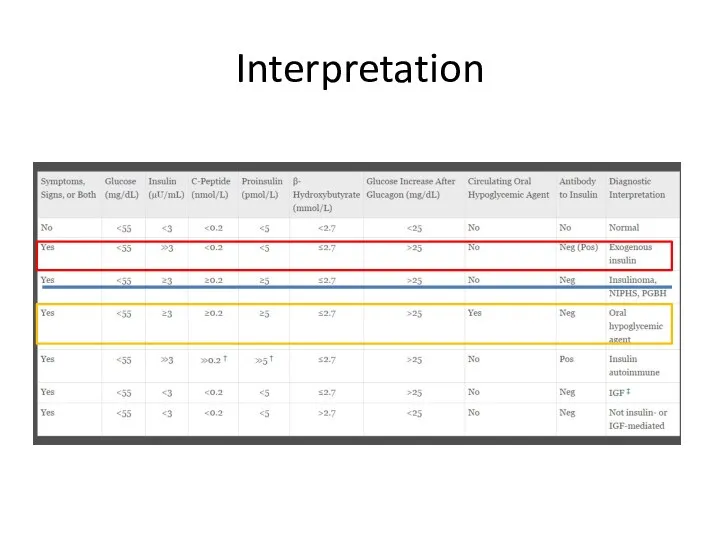
Interpretation
Interpretation
Insulinoma
1:250.000 individuals.
90% benign.
Usually sporadic and solitary ,may be part of
Insulinoma
1:250.000 individuals.
90% benign.
Usually sporadic and solitary ,may be part of
Insulinoma in the tail of pancreas on MRI
Insulinoma in the tail of pancreas on MRI
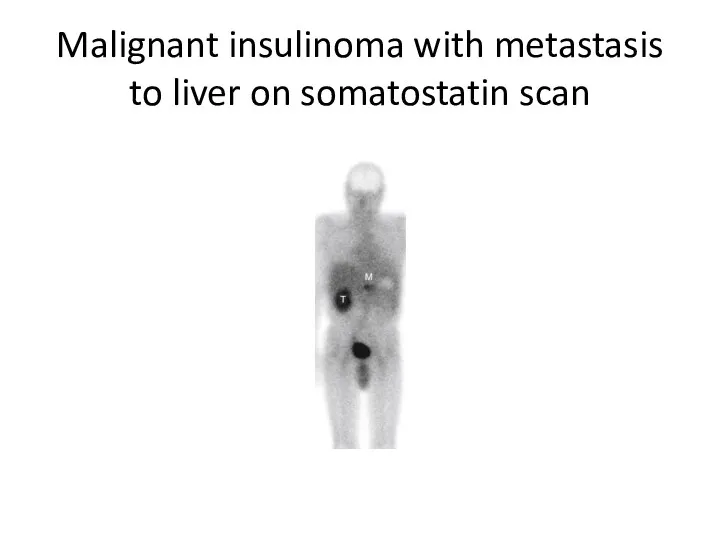
Malignant insulinoma with metastasis to liver on somatostatin scan
Malignant insulinoma with metastasis to liver on somatostatin scan
 Жас балалардағы тырнақ және шаш ерекшіліктері
Жас балалардағы тырнақ және шаш ерекшіліктері Профилактика стоматологических заболеваний в раннем детском возрасте
Профилактика стоматологических заболеваний в раннем детском возрасте Геморрагический васкули
Геморрагический васкули Болевые синдромы. Сенсорные расстройства
Болевые синдромы. Сенсорные расстройства Патологическая стираемость генерализованного типа
Патологическая стираемость генерализованного типа Медицина Московского государства (XV – XVII вв.)
Медицина Московского государства (XV – XVII вв.) Туберкулез почек, мочевыводящей системы и мужских половых органов
Туберкулез почек, мочевыводящей системы и мужских половых органов Воспалительные заболевания глазного яблока и зрительного нерва
Воспалительные заболевания глазного яблока и зрительного нерва Язвенная болезнь желудка и 12-перстной кишки у детей
Язвенная болезнь желудка и 12-перстной кишки у детей Шкода алкоголю, куріння та наркотиків
Шкода алкоголю, куріння та наркотиків Первая медицинская помощь при травмах опорнодвигательного аппарата
Первая медицинская помощь при травмах опорнодвигательного аппарата Организация здравоохранения в зарубежных странах. Страховая, бюджетная и частная системы здравоохранения
Организация здравоохранения в зарубежных странах. Страховая, бюджетная и частная системы здравоохранения Гипоксия и дыхательная недостаточность
Гипоксия и дыхательная недостаточность Медицинский отряд специального назначения
Медицинский отряд специального назначения Сенсорные и гностические нарушения при поражении зрительного и слухового анализаторов
Сенсорные и гностические нарушения при поражении зрительного и слухового анализаторов Современные методы исследования в офтальмологии
Современные методы исследования в офтальмологии Стоматологическое просвещение населения. (Лекция 17)
Стоматологическое просвещение населения. (Лекция 17) Цитомегаловирусты инфекция
Цитомегаловирусты инфекция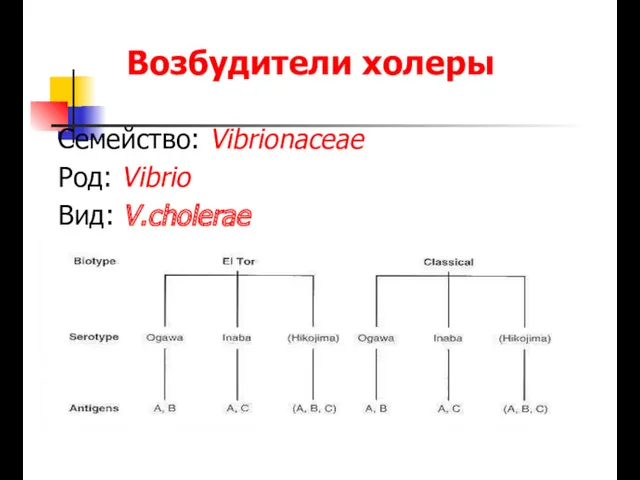 Возбудители холеры
Возбудители холеры Профилактика ВИЧ-инфекции
Профилактика ВИЧ-инфекции Зәр шығару жүйесі
Зәр шығару жүйесі Бүйрек туберкулезі
Бүйрек туберкулезі Выделение. Мочевыделительная система
Выделение. Мочевыделительная система Амбулаториялық-емханалық көмек көрсететін денсаулық сақтау ұйымдарының қызметі туралы ережені бекіту туралы
Амбулаториялық-емханалық көмек көрсететін денсаулық сақтау ұйымдарының қызметі туралы ережені бекіту туралы ЭХО-КГ в норме у детей
ЭХО-КГ в норме у детей Работники медицинских учреждений
Работники медицинских учреждений Балалардың іш қатуы
Балалардың іш қатуы Лекция №23. Острые гнойные заболевания мягких тканей
Лекция №23. Острые гнойные заболевания мягких тканей