- Immunosuppressant drugs

Содержание
- 2. INTRODUCTION OF IMMUNE SYSTEM Immunity : Ability of an organism to recognize and defensed itself against
- 3. THE IMMUNE SYSTEM IS THE THIRD LINE OF DEFENSE AGAINST INFECTION
- 4. IMMUNE SYSTEM Immune system include two main arms 1) Cell –mediated immunity. 2) Humoral (antibody –mediated
- 5. TYPES OF IMMUNITY Innate or genetic immunity : Immunity an organism is born with Genetically determined
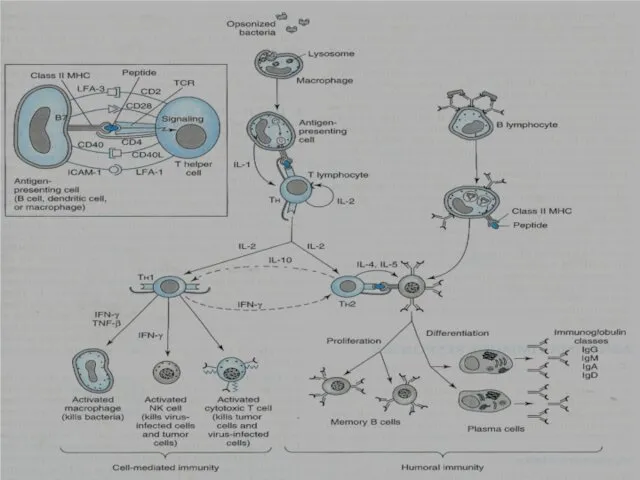
- 7. CYTOKINES Cytokines are soluble , antigen-nonspecific signaling proteins that bind to cell surface receptors on a
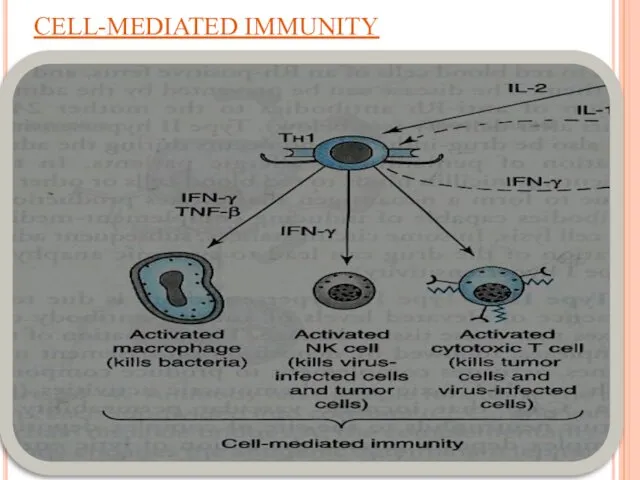
- 8. IL-2 stimulates the proliferation of antigen-primed (helper) T cells. Cell-mediated Immunity TH1 produce more IL-2, TNF-β
- 9. CELL-MEDIATED IMMUNITY
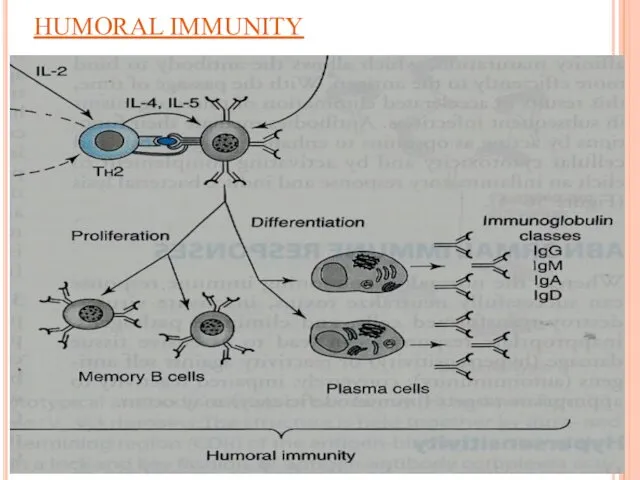
- 10. Humoral Immunity B-lymphocytes TH2 produces (interleukins) IL-4 & IL-5 which in turn causes: B cells proliferation
- 11. HUMORAL IMMUNITY
- 12. Mutual regulation of T helper lymphocytes TH1 interferon-γ: inhibits TH2 cell proliferation TH2 cells TH2 IL-10:
- 13. WHAT IS IMMUNOSUPRASSANT? Any of a variety of substance used to prevent production of antibodies. They
- 14. IMMUNOSUPPRESSANT DRUGS I. inhibitors of cytokine (IL-2) production or action: 1) Calcineurin inhibitors Cyclosporine Tacrolimus (FK506)
- 15. Cytotoxic drugs Inhibitors of purine or pyrimidine synthesis (Antimetabolites): Azathioprine Myclophenolate Mofetil Leflunomide Methotrexate Alkylating agents
- 16. IV. Immunosuppressive antibodies that block T cell surface molecules involved in signaling immunoglobulins antilymphocyte globulins (ALG).
- 17. I) Inhibitors of cytokines (IL-2) production or action Inhibitors of cytokines (IL-2) production Calcineurin inhibitors Cyclosporine
- 18. CYCLOSPORINE Chemistry Cyclosporine is a fungal polypeptide composed of 11 amino acids. Mechanism of action: Acts
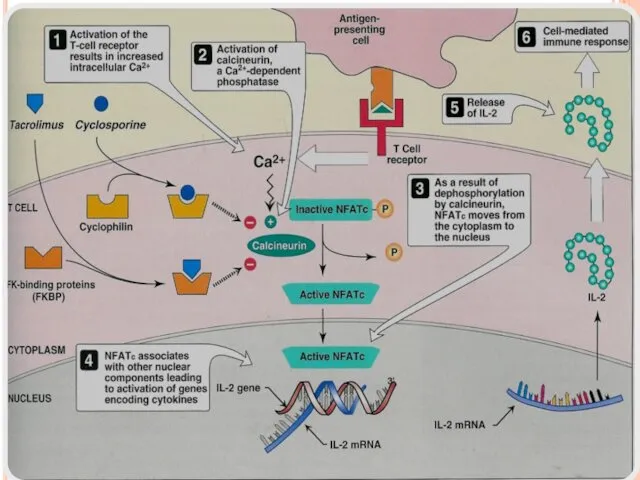
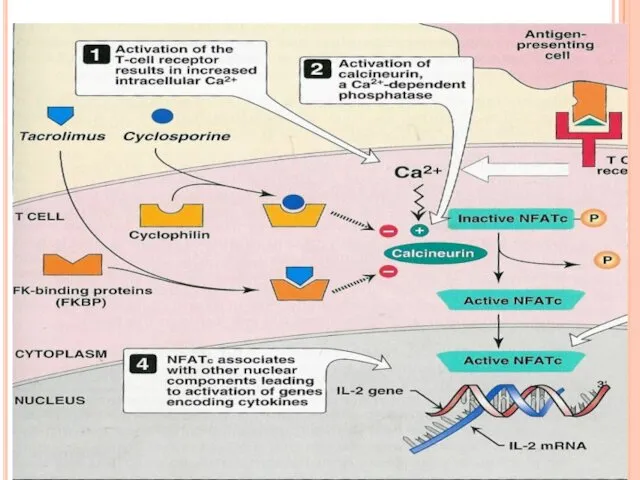
- 19. Cyclosporine binds to cyclophilin (immunophilin) intracellular protein receptors. Cyclosporine- immunophilin complex inhibits calcineurin, a phosphatase necessary
- 21. Pharmacokinetics: Can be given orally or i.v. infusion orally (25 or 100 mg) soft gelatin capsules,
- 22. 50 – 60% of cyclosporine accumulates in blood (erythrocytes – lymphocytes). metabolized by CYT-P450 system (CYP3A4).
- 23. Therapeutic Uses: Organ transplantation (kidney, liver, heart) either alone or with other immunosuppressive agents (Corticosteroids). Autoimmune
- 24. Adverse Effects (Dose-dependent) Therapeutic monitoring is essential Nephrotoxicity (increased by NSAIDs and aminoglycosides). Liver dysfunction. Hypertension,
- 25. Drug Interactions Clearance of cyclosporine is enhanced by co-administration of CYT p 450 inducers (Phenobarbitone, Phenytoin
- 26. TACROLIMUS (FK506) a fungal macrolide antibiotic. Chemically not related to cyclosporine both drugs have similar mechanism
- 28. Kinetics Given orally or i.v or topically (ointment). Oral absorption is variable and incomplete, reduced by
- 29. Toxic effects Nephrotoxicity (more than CsA) Neurotoxicity (more than CsA) Hyperglycemia ( require insulin). GIT disturbances
- 30. What are the differences between CsA and TAC ? TAC is more favorable than CsA due
- 31. Sirolimus (Rapamycin) SRL is macrolide antibiotic. SRL is derived from fungus origin. It binds to FKBP
- 33. Pharmakinetics Given orally and topically, reduced by fat meal. Extensively bound to plasma proteins metabolized by
- 34. USES Solid organ allograft Renal transplantation alone or combined with (CSA, tacrolimus, steroids, mycophenolate). Heart allografts
- 35. Toxic effects Hyperlipidaemia (cholesterol, triglycerides). Thrombocytopenia Leukopenia Hepatotoxicity Hypertension GIT dysfunction
- 36. Inhibitors of cytokine gene expression Corticosteroids Prednisone Prednisolone Methylprednisolone Dexamethasone They have both anti-inflammatory action and
- 37. Mechanism of action bind to glucocorticoid receptors and the complex interacts with DNA to inhibit gene
- 38. Kinetics Can be given orally or parenterally. Dynamics 1. Suppression of response to infection 2. anti-inflammatory
- 39. Adverse Effects Adrenal suppression Osteoporosis Hypercholesterolemia Hyperglycemia Hypertension Cataract Infection
- 40. Cytotoxic drugs Inhibitors of purine or pyrimidine synthesis (Antimetabolites): Azathioprine Myclophenolate Mofetil Leflunomide Methotrexate Alkylating agents
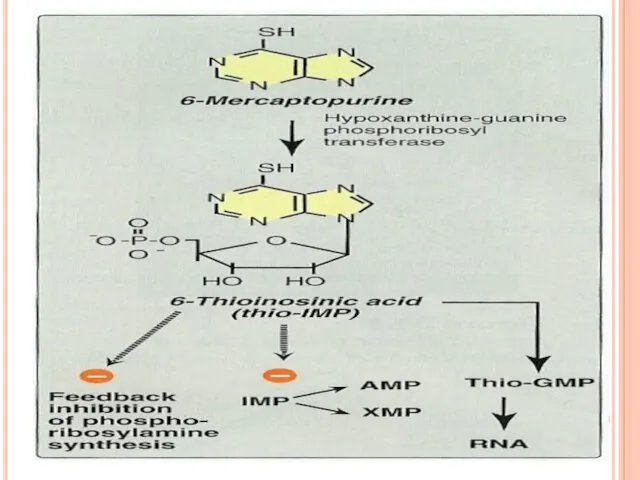
- 41. AZATHIOPRINE CHEMISTRY: Derivative of mercaptopurine. Prodrug. Cleaved to 6-mercaptopurine then to 6-mercaptopurine nucleotide, thioinosinic acid (nucleotide
- 43. Pharmacokinetics orally or intravenously. Widely distributed but does not cross BBB. Metabolized in the liver to
- 44. Adverse Effects Bone marrow depression: leukopenia, thrombocytopenia. Gastrointestinal toxicity. Hepatotoxicity. Increased risk of infections.
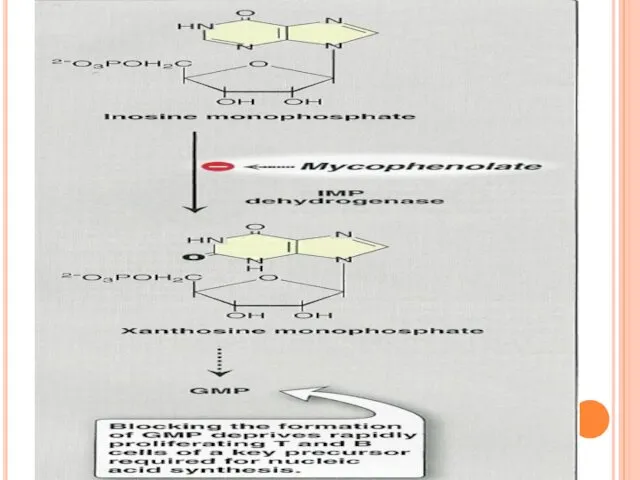
- 45. MYCOPHENOLATE MOFETIL Is a semisynthetic derivative of mycophenolic acid from fungus source. Prodrug; is hydrolyzed to
- 47. Pharmacokinetics: Given orally, i.v. or i.m. rapidly and completely absorbed after oral administration. It undergoes first-pass
- 48. CLINICAL USE: Solid organ transplants for refractory rejection. Steroid-refractory hematopoietic stem cell transplant patients. Combined with
- 49. LEFLUNOMIDE A prodrug Active metabolite undergoes enterohepatic circulation. Has long duration of action. Can be given
- 50. Adverse effects Elevation of liver enzymes Renal impairment Teratogenicity Cardiovascular effects (tachycardia).
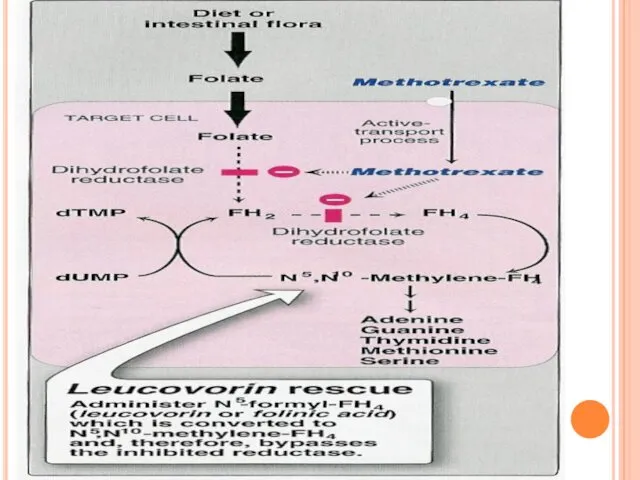
- 51. Methotrexate a folic acid antagonist Orally, parenterally (I.V., I.M). Excreted in urine. Inhibits dihydrofolate reductase required
- 53. Cyclophosphamide Alkylating agent to DNA. Prodrug, activated into phosphamide. Is given orally& intravenously Destroy proliferating lymphoid
- 54. Antibodies block T cell surface molecules involved in signaling immunoglobulins antilymphocyte globulins (ALG). antithymocyte globulins (ATG).
- 55. 2. Hybridoma technology produce antigen-specific, monoclonal antibody (homogenous, specific). produced by fusing mouse antibody-producing cells with
- 56. Antilymphocyte globulins (ALG) &Antithymocyte globulins (ATG) Polyclonal antibodies obtained from plasma or serum of horses hyper-immunized
- 57. Adverse Effects: Antigenicity. Leukopenia, thrombocytopenia. Risk of viral infection. Anaphylactic and serum sickness reactions (Fever, Chills,
- 58. Muromonab-CD3 Is a murine monoclonal antibody Prepared by hybridoma technology Directed against glycoprotein CD3 antigen of
- 59. Uses Used for treatment of acute renal allograft rejection & steroid-resistant acute allograft To deplete T
- 60. Rho (D) immune globulin Rho (D) is a concentrated solution of human IgG containing higher titer
- 61. Mechanism of action IL-2 receptor antagonists Are Anti-CD25 Bind to CD25 (α-subunit chain of IL-2 receptor
- 62. Monoclonal antibodies Infliximab a chimeric human-mouse IgG Directed against TNF-α Is approved for ulcerative colitis, Crohn’s
- 63. INTERFERONS Three families: Type I IFNs ( IFN-α, β ): acid-stable proteins; act on same target
- 64. Interferon Effects: IFN- γ : Immune Enhancing increased antigen presentations with macrophage, natural killer cell, cytotoxic
- 65. VI. INTERFERONS Recombinant DNA cloning technology. Antiproliferative activity. Antiviral action Immunomodulatory effect. USES: Treatment of certain
- 66. THAMLIDOMIDE A sedative drug. Teratogenic (Class-X). Can be given orally. Has immunomodulatory actions Inhibits TNF-α Reduces
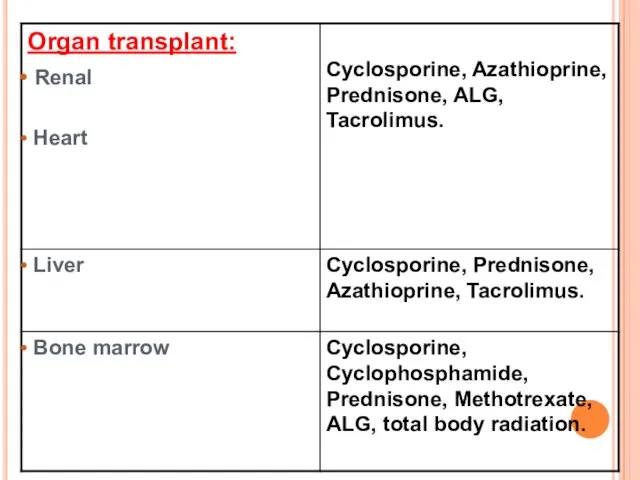
- 68. CLINICAL USES OF IMMUNOSUPPRESSIVE AGENTS
- 71. Скачать презентацию
INTRODUCTION OF IMMUNE SYSTEM
Immunity : Ability of an organism to recognize
INTRODUCTION OF IMMUNE SYSTEM
Immunity : Ability of an organism to recognize
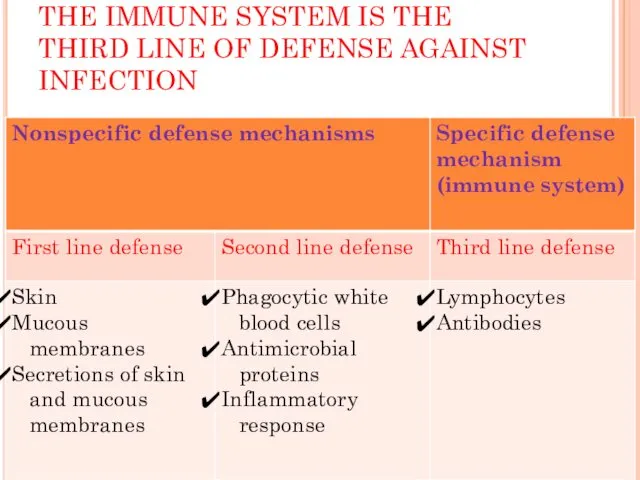
THE IMMUNE SYSTEM IS THE THIRD LINE OF DEFENSE AGAINST INFECTION
THE IMMUNE SYSTEM IS THE THIRD LINE OF DEFENSE AGAINST INFECTION
IMMUNE SYSTEM
Immune system include two main arms
1) Cell –mediated immunity.
2) Humoral
IMMUNE SYSTEM
Immune system include two main arms
1) Cell –mediated immunity.
2) Humoral
TYPES OF IMMUNITY
Innate or genetic immunity :
Immunity an organism is
TYPES OF IMMUNITY
Innate or genetic immunity :
Immunity an organism is
CYTOKINES
Cytokines are soluble , antigen-nonspecific signaling proteins that
bind to
CYTOKINES
Cytokines are soluble , antigen-nonspecific signaling proteins that
bind to
IL-2 stimulates the proliferation of antigen-primed (helper) T cells.
Cell-mediated Immunity
TH1
IL-2 stimulates the proliferation of antigen-primed (helper) T cells.
Cell-mediated Immunity
TH1
CELL-MEDIATED IMMUNITY
CELL-MEDIATED IMMUNITY
Humoral Immunity
B-lymphocytes TH2 produces (interleukins) IL-4 & IL-5 which in
Humoral Immunity
B-lymphocytes TH2 produces (interleukins) IL-4 & IL-5 which in
HUMORAL IMMUNITY
HUMORAL IMMUNITY
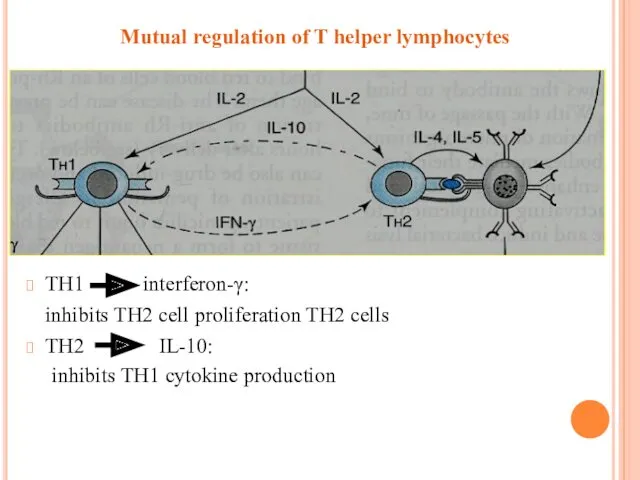
Mutual regulation of T helper lymphocytes
TH1 interferon-γ:
inhibits TH2 cell proliferation
Mutual regulation of T helper lymphocytes
TH1 interferon-γ:
inhibits TH2 cell proliferation
WHAT IS IMMUNOSUPRASSANT?
Any of a variety of substance used to prevent
WHAT IS IMMUNOSUPRASSANT?
Any of a variety of substance used to prevent
IMMUNOSUPPRESSANT DRUGS
I. inhibitors of cytokine (IL-2) production or action:
1) Calcineurin inhibitors
Cyclosporine
Tacrolimus
IMMUNOSUPPRESSANT DRUGS
I. inhibitors of cytokine (IL-2) production or action:
1) Calcineurin inhibitors
Cyclosporine
Tacrolimus
Cytotoxic drugs
Inhibitors of purine or pyrimidine synthesis
(Antimetabolites):
Azathioprine
Myclophenolate Mofetil
Leflunomide
Methotrexate
Alkylating agents
Cyclophosphamide
Cytotoxic drugs
Inhibitors of purine or pyrimidine synthesis
(Antimetabolites):
Azathioprine
Myclophenolate Mofetil
Leflunomide
Methotrexate
Alkylating agents
Cyclophosphamide
IV. Immunosuppressive antibodies
that block T cell surface molecules involved
IV. Immunosuppressive antibodies
that block T cell surface molecules involved
I) Inhibitors of cytokines (IL-2) production or action
Inhibitors of cytokines (IL-2)
I) Inhibitors of cytokines (IL-2) production or action
Inhibitors of cytokines (IL-2)
CYCLOSPORINE
Chemistry
Cyclosporine is a fungal polypeptide composed of 11 amino
CYCLOSPORINE
Chemistry
Cyclosporine is a fungal polypeptide composed of 11 amino
Cyclosporine binds to cyclophilin (immunophilin) intracellular protein receptors.
Cyclosporine- immunophilin complex inhibits
Cyclosporine binds to cyclophilin (immunophilin) intracellular protein receptors.
Cyclosporine- immunophilin complex inhibits
Pharmacokinetics:
Can be given orally or i.v. infusion
orally (25 or 100
Pharmacokinetics:
Can be given orally or i.v. infusion
orally (25 or 100
50 – 60% of cyclosporine accumulates in blood (erythrocytes – lymphocytes).
metabolized
metabolized
Therapeutic Uses:
Organ transplantation (kidney, liver, heart) either alone or with other
Therapeutic Uses:
Organ transplantation (kidney, liver, heart) either alone or with other
Adverse Effects (Dose-dependent)
Therapeutic monitoring is essential
Nephrotoxicity
(increased by NSAIDs and aminoglycosides).
Liver
Adverse Effects (Dose-dependent)
Therapeutic monitoring is essential
Nephrotoxicity
(increased by NSAIDs and aminoglycosides).
Liver
Drug Interactions
Clearance of cyclosporine is enhanced by co-administration of CYT p
Drug Interactions
Clearance of cyclosporine is enhanced by co-administration of CYT p
TACROLIMUS (FK506)
a fungal macrolide antibiotic.
Chemically not related to cyclosporine
both drugs
TACROLIMUS (FK506)
a fungal macrolide antibiotic.
Chemically not related to cyclosporine
both drugs
Kinetics
Given orally or i.v or topically (ointment).
Oral absorption is variable and
Kinetics
Given orally or i.v or topically (ointment).
Oral absorption is variable and
Toxic effects
Nephrotoxicity (more than CsA)
Neurotoxicity (more than CsA)
Hyperglycemia ( require
Toxic effects
Nephrotoxicity (more than CsA)
Neurotoxicity (more than CsA)
Hyperglycemia ( require
What are the differences between CsA and TAC ?
TAC is more
What are the differences between CsA and TAC ?
TAC is more
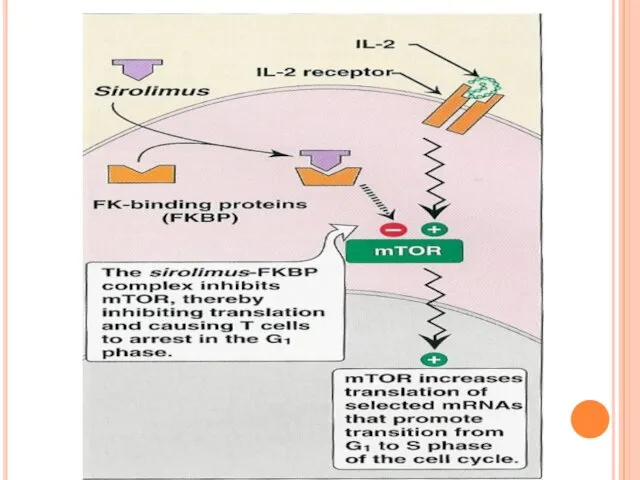
Sirolimus (Rapamycin)
SRL is macrolide antibiotic.
SRL is derived from fungus origin.
It
Sirolimus (Rapamycin)
SRL is macrolide antibiotic.
SRL is derived from fungus origin.
It
Pharmakinetics
Given orally and topically, reduced by fat meal.
Extensively bound to plasma
Pharmakinetics
Given orally and topically, reduced by fat meal.
Extensively bound to plasma
USES
Solid organ allograft
Renal transplantation alone or combined with (CSA, tacrolimus, steroids,
USES
Solid organ allograft
Renal transplantation alone or combined with (CSA, tacrolimus, steroids,
Toxic effects
Hyperlipidaemia (cholesterol, triglycerides).
Thrombocytopenia
Leukopenia
Hepatotoxicity
Hypertension
GIT dysfunction
Toxic effects
Hyperlipidaemia (cholesterol, triglycerides).
Thrombocytopenia
Leukopenia
Hepatotoxicity
Hypertension
GIT dysfunction
Inhibitors of cytokine gene expression
Corticosteroids
Prednisone
Prednisolone
Methylprednisolone
Dexamethasone
They have both anti-inflammatory action and
Inhibitors of cytokine gene expression
Corticosteroids
Prednisone
Prednisolone
Methylprednisolone
Dexamethasone
They have both anti-inflammatory action and
Mechanism of action
bind to glucocorticoid receptors and the complex interacts with
Mechanism of action
bind to glucocorticoid receptors and the complex interacts with
Kinetics
Can be given orally or parenterally.
Dynamics
1. Suppression of response to infection
2.
Kinetics
Can be given orally or parenterally.
Dynamics
1. Suppression of response to infection
2.
Adverse Effects
Adrenal suppression
Osteoporosis
Hypercholesterolemia
Hyperglycemia
Hypertension
Cataract
Infection
Adverse Effects
Adrenal suppression
Osteoporosis
Hypercholesterolemia
Hyperglycemia
Hypertension
Cataract
Infection
Cytotoxic drugs
Inhibitors of purine or pyrimidine synthesis
(Antimetabolites):
Azathioprine
Myclophenolate Mofetil
Leflunomide
Methotrexate
Alkylating agents
Cyclophosphamide
Cytotoxic drugs
Inhibitors of purine or pyrimidine synthesis
(Antimetabolites):
Azathioprine
Myclophenolate Mofetil
Leflunomide
Methotrexate
Alkylating agents
Cyclophosphamide
AZATHIOPRINE
CHEMISTRY:
Derivative of mercaptopurine.
Prodrug.
Cleaved to 6-mercaptopurine then to
6-mercaptopurine nucleotide,
AZATHIOPRINE
CHEMISTRY:
Derivative of mercaptopurine.
Prodrug.
Cleaved to 6-mercaptopurine then to
6-mercaptopurine nucleotide,
Pharmacokinetics
orally or intravenously.
Widely distributed but does not cross BBB.
Metabolized in the
Pharmacokinetics
orally or intravenously.
Widely distributed but does not cross BBB.
Metabolized in the
Adverse Effects
Bone marrow depression: leukopenia,
thrombocytopenia.
Gastrointestinal toxicity.
Adverse Effects
Bone marrow depression: leukopenia,
thrombocytopenia.
Gastrointestinal toxicity.
MYCOPHENOLATE MOFETIL
Is a semisynthetic derivative of mycophenolic acid from fungus source.
Prodrug;
MYCOPHENOLATE MOFETIL
Is a semisynthetic derivative of mycophenolic acid from fungus source.
Prodrug;
Pharmacokinetics:
Given orally, i.v. or i.m.
rapidly and completely absorbed after oral administration.
It
Pharmacokinetics:
Given orally, i.v. or i.m.
rapidly and completely absorbed after oral administration.
It
CLINICAL USE:
Solid organ transplants for refractory rejection.
Steroid-refractory hematopoietic stem cell transplant
CLINICAL USE:
Solid organ transplants for refractory rejection.
Steroid-refractory hematopoietic stem cell transplant
LEFLUNOMIDE
A prodrug
Active metabolite undergoes enterohepatic circulation.
Has long duration of action.
Can be
LEFLUNOMIDE
A prodrug
Active metabolite undergoes enterohepatic circulation.
Has long duration of action.
Can be
Adverse effects
Elevation of liver enzymes
Renal impairment
Teratogenicity
Cardiovascular effects
Elevation of liver enzymes
Renal impairment
Teratogenicity
Cardiovascular effects
Methotrexate
a folic acid antagonist
Orally, parenterally (I.V., I.M).
Excreted in urine.
Inhibits
Methotrexate
a folic acid antagonist
Orally, parenterally (I.V., I.M).
Excreted in urine.
Inhibits
Cyclophosphamide
Alkylating agent to DNA.
Prodrug, activated into phosphamide.
Is given orally& intravenously
Destroy proliferating
Cyclophosphamide
Alkylating agent to DNA.
Prodrug, activated into phosphamide.
Is given orally& intravenously
Destroy proliferating
Antibodies
block T cell surface molecules involved in signaling immunoglobulins
antilymphocyte
Antibodies
block T cell surface molecules involved in signaling immunoglobulins
antilymphocyte
2. Hybridoma technology
produce antigen-specific, monoclonal antibody (homogenous, specific).
produced by fusing
2. Hybridoma technology
produce antigen-specific, monoclonal antibody (homogenous, specific).
produced by fusing
Antilymphocyte globulins (ALG) &Antithymocyte globulins (ATG)
Polyclonal antibodies obtained from plasma
Antilymphocyte globulins (ALG) &Antithymocyte globulins (ATG)
Polyclonal antibodies obtained from plasma
Adverse Effects:
Antigenicity.
Leukopenia, thrombocytopenia.
Risk of viral infection.
Anaphylactic and serum sickness reactions (Fever,
Adverse Effects:
Antigenicity.
Leukopenia, thrombocytopenia.
Risk of viral infection.
Anaphylactic and serum sickness reactions (Fever,
Muromonab-CD3
Is a murine monoclonal antibody
Prepared by hybridoma technology
Directed against
Muromonab-CD3
Is a murine monoclonal antibody
Prepared by hybridoma technology
Directed against
Uses
Used for treatment of acute renal allograft rejection & steroid-resistant acute
Uses
Used for treatment of acute renal allograft rejection & steroid-resistant acute
Rho (D) immune globulin
Rho (D) is a concentrated solution of
Rho (D) immune globulin
Rho (D) is a concentrated solution of
Mechanism of action
IL-2 receptor antagonists
Are Anti-CD25
Bind to CD25 (α-subunit chain of
Mechanism of action
IL-2 receptor antagonists
Are Anti-CD25
Bind to CD25 (α-subunit chain of
Monoclonal antibodies
Infliximab
a chimeric human-mouse IgG
Directed against TNF-α
Is approved for ulcerative
Monoclonal antibodies
Infliximab
a chimeric human-mouse IgG
Directed against TNF-α
Is approved for ulcerative
INTERFERONS
Three families:
Type I IFNs ( IFN-α, β ):
INTERFERONS
Three families:
Type I IFNs ( IFN-α, β ):
Interferon Effects:
IFN- γ : Immune Enhancing
increased antigen presentations with
Interferon Effects:
IFN- γ : Immune Enhancing
increased antigen presentations with
VI. INTERFERONS
Recombinant DNA cloning technology.
Antiproliferative activity.
Antiviral action
Immunomodulatory effect.
USES:
Treatment of certain
VI. INTERFERONS
Recombinant DNA cloning technology.
Antiproliferative activity.
Antiviral action
Immunomodulatory effect.
USES:
Treatment of certain
THAMLIDOMIDE
A sedative drug.
Teratogenic (Class-X).
Can be given orally.
Has immunomodulatory actions
Inhibits
THAMLIDOMIDE
A sedative drug.
Teratogenic (Class-X).
Can be given orally.
Has immunomodulatory actions
Inhibits
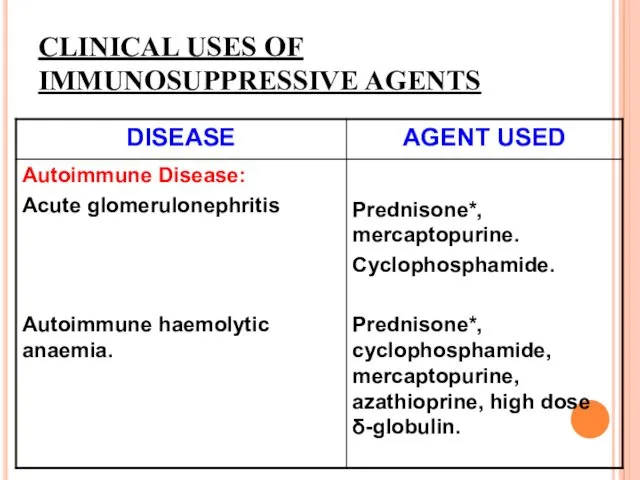
CLINICAL USES OF IMMUNOSUPPRESSIVE AGENTS
CLINICAL USES OF IMMUNOSUPPRESSIVE AGENTS
 Развитие клинической медицины в XIX веке в России. Лекция 10
Развитие клинической медицины в XIX веке в России. Лекция 10 Основные задачи и направления развития гигиены
Основные задачи и направления развития гигиены Жизнеугрожающие состояния при синоатриальной, атриовентрикулярной блокадах вісокой степени и дисфункции синусового узла
Жизнеугрожающие состояния при синоатриальной, атриовентрикулярной блокадах вісокой степени и дисфункции синусового узла Medical-preventive faculty
Medical-preventive faculty Болезнь Паркинсона
Болезнь Паркинсона Гистофизиология органов дыхательной системы
Гистофизиология органов дыхательной системы Занятие 4. Кожа и подкожно-жировая клетчатка
Занятие 4. Кожа и подкожно-жировая клетчатка Печеночная кома. Интенсивная терапия
Печеночная кома. Интенсивная терапия Диабеттік ретинопатия
Диабеттік ретинопатия Виды нарушений опорно-двигательного аппарата
Виды нарушений опорно-двигательного аппарата Жыныстық ажыратылу физиологиясы және жыныс бездері функциясының жас ерекшелігіне қатысты өзгерістері
Жыныстық ажыратылу физиологиясы және жыныс бездері функциясының жас ерекшелігіне қатысты өзгерістері Communication 25
Communication 25 Медикаментозная обработка корневых каналов
Медикаментозная обработка корневых каналов Раковые стволовые клетки
Раковые стволовые клетки Психология терминальных больных. Концепция Е. Кюблер-Росс “смерть как стадия роста”. Право на правду о последнем диагнозе
Психология терминальных больных. Концепция Е. Кюблер-Росс “смерть как стадия роста”. Право на правду о последнем диагнозе Топографическая анатомия и операции на голове
Топографическая анатомия и операции на голове Основні методи дослідження пацієнтів при травмах та захворюваннях опорно-рухового апарату (ОРА). Об’єктивне обстеження
Основні методи дослідження пацієнтів при травмах та захворюваннях опорно-рухового апарату (ОРА). Об’єктивне обстеження Патология восприятия
Патология восприятия pril1
pril1 Уход за ребенком первого года жизни
Уход за ребенком первого года жизни Наркомания. Есть выбор: жизнь без наркотиков
Наркомания. Есть выбор: жизнь без наркотиков Шовный материал в хирургии
Шовный материал в хирургии Салмонеллалар. Морфологиясы мен тинкториалдық қасиеттері
Салмонеллалар. Морфологиясы мен тинкториалдық қасиеттері Профилактика остеохондроза
Профилактика остеохондроза Teva Pharmaceutical Industries Ltd. - один из лидеров мировой фармацевтической отрасли
Teva Pharmaceutical Industries Ltd. - один из лидеров мировой фармацевтической отрасли Тазовое дно. Дисфункция тазового дна
Тазовое дно. Дисфункция тазового дна Общие вопросы наркологии
Общие вопросы наркологии Зубні відкладення. Неминерализованные та карієсогенна ситуація в порожнині рота. Механізм утворення та видалення
Зубні відкладення. Неминерализованные та карієсогенна ситуація в порожнині рота. Механізм утворення та видалення