- Malaria

Содержание
- 2. MALARIA Infection with pathogenic protozoa exacts an enormous toll of human suffering, notably, but not exclusively,
- 3. Four species are encountered in human disease: P. vivax and P. ovale, both of which cause
- 4. Parasitology The female mosquito becomes infected after taking a blood meal containing gametocytes, the sexual form
- 5. Parasitology Here they multiply inside hepatocytes as merozoites: this is pre-erythrocytic (or hepatic) sporogeny. After a
- 6. Parasitology Inside the red cells the parasites again multiply, changing from merozoite, to trophozoite, to schizont,
- 7. Parasitology A few merozoites develop not into trophozoites but into gametocytes. These are not released from
- 8. Pathogenesis The pathology of malaria is related to: anaemia, cytokine release, in the case of P.
- 9. Pathogenesis The female anopheline mosquito becomes infected when it feeds on human blood containing gametocytes, the
- 10. Pathogenesis P. vivax and P. ovale may persist in liver cells as dormant forms, hypozoites, capable
- 11. Pathogenesis P. falciparum and P. malariae have no persistent exoerythrocytic phase but recrudescences of fever may
- 12. Effect on red blood cells and capillaries Malaria is always accompanied by haemolysis and in a
- 13. Pathogenesis Haemolysis is most severe with P. falciparum, which invades red cells of all ages but
- 14. Pathogenesis In P. falciparum malaria, red cells containing schizonts adhere to the lining of capillaries in
- 15. Pathogenesis After repeated infections partial immunity develops, allowing the host to tolerate parasitaemia with minimal ill
- 16. Pathogenesis Certain genetic traits also confer some immunity to malaria. People who lack the Duffy antigen
- 17. Clinical features Typical malaria is seen in non-immune individuals. This includes children in any area, adults
- 18. P. vivax and P. ovale malaria In many cases the illness starts with a period of
- 19. P. malariae infection This usually associated with mild symptoms and bouts of fever every third day.
- 20. P. falciparum infection These are more dangerous than other forms of malaria. The onset, especially of
- 21. P. falciparum infection A patient with falciparum malaria, apparently not seriously ill, may develop serious complications.
- 22. Complications of malaria due to P. falciparum: I. Severe anaemia. II. Organ damage due to anoxia:
- 23. Complications of malaria due to P. falciparum: III. Intravascular haemolysis. Blackwater fever is associated with chronic
- 24. Clinical features In hyperendemic and in holoendemic areas malaria may kill up to 15-20 % of
- 25. Diagnosis Malaria should be considered in the differential diagnosis of anyone who presents with a febrile
- 26. Laboratory diagnosis To establish the diagnosis, a drop of peripheral blood is spread on a glass
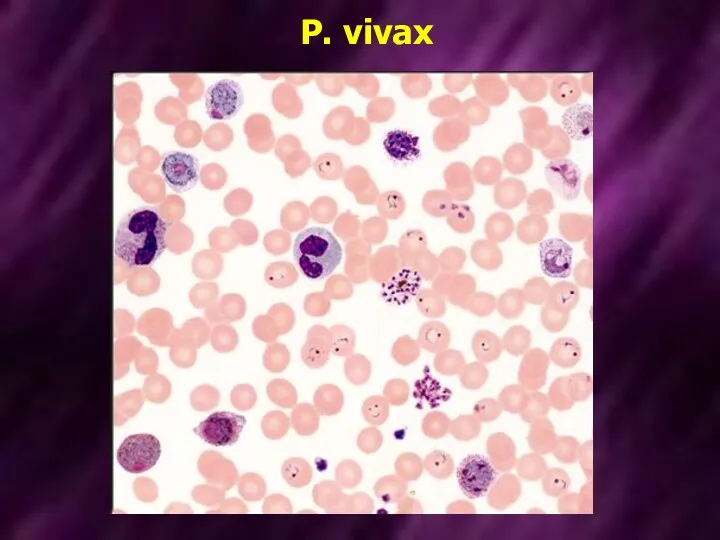
- 27. P. vivax
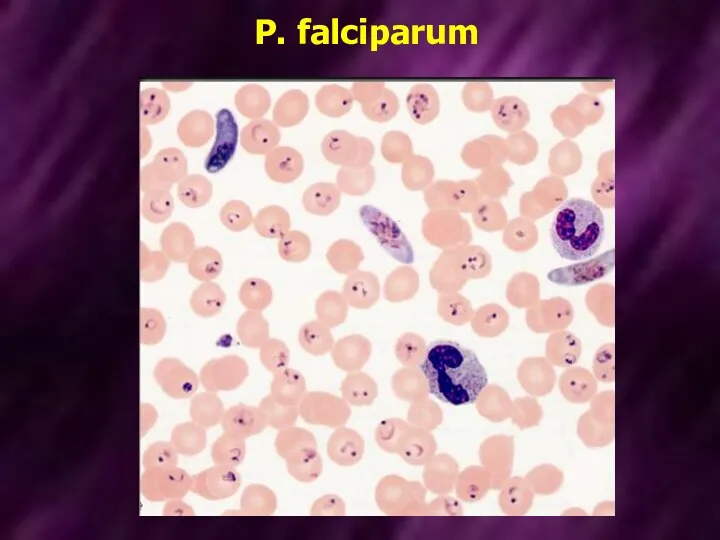
- 28. P. falciparum
- 29. Treatment For many years the standard treatment for acute malaria was chloroquine. Howewer, resistance to that
- 30. Treatment Alternative agents include mefloquine and halofantrine. These drugs are active against chloroquine-resistant strains, but resistance
- 31. Treatment Treatment of acute malaria with chloroquine, quinine or other antimalarials will not eliminate parasites in
- 32. Prevention Clinical attacks of malaria may be preventable by drugs such as proguanil which attack the
- 33. Chemoprophylaxis of malaria
- 34. Chemoprophylaxis of malaria Chemoprophylaxis is begun 1 week before entering the malarious area and is continued
- 36. Скачать презентацию
MALARIA
Infection with pathogenic protozoa exacts an enormous toll of human suffering,
MALARIA
Infection with pathogenic protozoa exacts an enormous toll of human suffering,
Four species are encountered in human disease:
P. vivax and P.
Four species are encountered in human disease:
P. vivax and P.
Parasitology
The female mosquito becomes infected after taking a blood meal containing
Parasitology
The female mosquito becomes infected after taking a blood meal containing
Parasitology
Here they multiply inside hepatocytes as merozoites: this is pre-erythrocytic (or
Parasitology
Here they multiply inside hepatocytes as merozoites: this is pre-erythrocytic (or
Parasitology
Inside the red cells the parasites again multiply, changing from merozoite,
Parasitology
Inside the red cells the parasites again multiply, changing from merozoite,
Parasitology
A few merozoites develop not into trophozoites but into gametocytes. These
Parasitology
A few merozoites develop not into trophozoites but into gametocytes. These
Pathogenesis
The pathology of malaria is related to:
anaemia,
cytokine release,
in the
Pathogenesis
The pathology of malaria is related to:
anaemia,
cytokine release,
in the
Pathogenesis
The female anopheline mosquito becomes infected when it feeds on human
Pathogenesis
The female anopheline mosquito becomes infected when it feeds on human
Pathogenesis
P. vivax and P. ovale may persist in liver cells as
Pathogenesis
P. vivax and P. ovale may persist in liver cells as
Pathogenesis
P. falciparum and P. malariae have no persistent exoerythrocytic phase but
Pathogenesis
P. falciparum and P. malariae have no persistent exoerythrocytic phase but
Effect on red blood cells and capillaries
Malaria is always accompanied by
Effect on red blood cells and capillaries
Malaria is always accompanied by
Pathogenesis
Haemolysis is most severe with P. falciparum, which invades red cells
Pathogenesis
Haemolysis is most severe with P. falciparum, which invades red cells
Pathogenesis
In P. falciparum malaria, red cells containing schizonts adhere to the
Pathogenesis
In P. falciparum malaria, red cells containing schizonts adhere to the
Pathogenesis
After repeated infections partial immunity develops, allowing the host to tolerate
Pathogenesis
After repeated infections partial immunity develops, allowing the host to tolerate
Pathogenesis
Certain genetic traits also confer some immunity to malaria. People who
Pathogenesis
Certain genetic traits also confer some immunity to malaria. People who
Clinical features
Typical malaria is seen in non-immune individuals. This includes children
Clinical features
Typical malaria is seen in non-immune individuals. This includes children
P. vivax and P. ovale malaria
In many cases the illness starts
P. vivax and P. ovale malaria
In many cases the illness starts
P. malariae infection
This usually associated with mild symptoms and bouts of
P. malariae infection
This usually associated with mild symptoms and bouts of
P. falciparum infection
These are more dangerous than other forms of malaria.
P. falciparum infection
These are more dangerous than other forms of malaria.
P. falciparum infection
A patient with falciparum malaria, apparently not seriously ill,
P. falciparum infection
A patient with falciparum malaria, apparently not seriously ill,
Complications of malaria due to P. falciparum:
I. Severe anaemia.
Complications of malaria due to P. falciparum:
I. Severe anaemia.
Complications of malaria due to P. falciparum:
III. Intravascular haemolysis. Blackwater fever
Complications of malaria due to P. falciparum:
III. Intravascular haemolysis. Blackwater fever
Clinical features
In hyperendemic and in holoendemic areas malaria may kill up
Clinical features
In hyperendemic and in holoendemic areas malaria may kill up
Diagnosis
Malaria should be considered in the differential diagnosis of anyone who
Diagnosis
Malaria should be considered in the differential diagnosis of anyone who
Laboratory diagnosis
To establish the diagnosis, a drop of peripheral blood is
Laboratory diagnosis
To establish the diagnosis, a drop of peripheral blood is
P. vivax
P. vivax
P. falciparum
P. falciparum
Treatment
For many years the standard treatment for acute malaria was chloroquine.
Treatment
For many years the standard treatment for acute malaria was chloroquine.
Treatment
Alternative agents include mefloquine and halofantrine. These drugs are active against
Treatment
Alternative agents include mefloquine and halofantrine. These drugs are active against
Treatment
Treatment of acute malaria with chloroquine, quinine or other antimalarials will
Treatment
Treatment of acute malaria with chloroquine, quinine or other antimalarials will
Prevention
Clinical attacks of malaria may be preventable by drugs such as
Prevention
Clinical attacks of malaria may be preventable by drugs such as
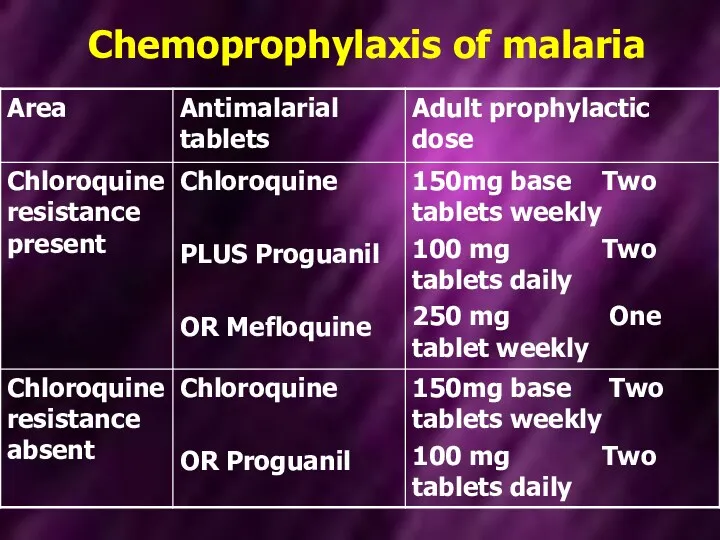
Chemoprophylaxis of malaria
Chemoprophylaxis of malaria
Chemoprophylaxis of malaria
Chemoprophylaxis is begun 1 week before entering the malarious
Chemoprophylaxis of malaria
Chemoprophylaxis is begun 1 week before entering the malarious
 Центральные анальгетики
Центральные анальгетики Анатомия носа и околоносовых пазух. Наружный нос. Хрящи, вид спереди
Анатомия носа и околоносовых пазух. Наружный нос. Хрящи, вид спереди Организация медицинского обеспечения мотострелкового батальона
Организация медицинского обеспечения мотострелкового батальона Ангиогенин – естественное восстановление красоты и здоровья
Ангиогенин – естественное восстановление красоты и здоровья COVID-19. Профилактика
COVID-19. Профилактика Эякуляцияның физиологиясы
Эякуляцияның физиологиясы Полтавченко СИ 71310 Рентгенография
Полтавченко СИ 71310 Рентгенография Ортодонтиядағы рентгенологиялық диагностикалау әдістері, ортопантомография, 3Д, панорамды, ауызішілік
Ортодонтиядағы рентгенологиялық диагностикалау әдістері, ортопантомография, 3Д, панорамды, ауызішілік Маркировка лекарственных средств
Маркировка лекарственных средств Гигиена и правила ухода за кожей
Гигиена и правила ухода за кожей Основы физической реабилитации: лечебная физическая культура
Основы физической реабилитации: лечебная физическая культура Зондовые манипуляции
Зондовые манипуляции Пограничное расстройство личности
Пограничное расстройство личности Пиодермии. Определение
Пиодермии. Определение Роль среднего медицинского работника в пропаганде грамотного использования устройств сотовой связи
Роль среднего медицинского работника в пропаганде грамотного использования устройств сотовой связи Основные методологические подходы к оценке качества медицинской помощи
Основные методологические подходы к оценке качества медицинской помощи Недоношенные дети
Недоношенные дети Атеросклероз коронарной артерии
Атеросклероз коронарной артерии ГЭРБ и бронхиальная астма
ГЭРБ и бронхиальная астма Инородные тела уха
Инородные тела уха Врожденная косолапость
Врожденная косолапость Развитие координационных способностей мужчин с нарушением слуха на занятиях футболом
Развитие координационных способностей мужчин с нарушением слуха на занятиях футболом Экология микроорганизмов. Микрофлора воздуха, почвы, воды. Нормальная микрофлора организма человека, ее значение. Дисбактериоз
Экология микроорганизмов. Микрофлора воздуха, почвы, воды. Нормальная микрофлора организма человека, ее значение. Дисбактериоз Этиология и патогенез. Опухолевого роста. Лихорадка. Лекция 5
Этиология и патогенез. Опухолевого роста. Лихорадка. Лекция 5 Pirmās palīdzības apmācība
Pirmās palīdzības apmācība I.Introduction. Contact transmission mechanism. Prevention of contact infection
I.Introduction. Contact transmission mechanism. Prevention of contact infection Общая рецептура. Твердые лекарственные формы
Общая рецептура. Твердые лекарственные формы Қартаюдың молекулалықгенетикалық механизмдері
Қартаюдың молекулалықгенетикалық механизмдері