- Meningococcal infection

Содержание
- 2. Etiology the causative agent is meningococcus (Neisseria meningitidis). this microorganism has the form of a diplococcus,
- 3. Epidemiology the sources of infection are patient and carriers meningococcus expel the causative agent with the
- 4. Pathogenesis and Pathology The portal of the infection entry is the nasopharyngeal mucous The carrier state
- 5. Purulent meningitis develops due to the ingress of the meningococcus into the soft meninges of the
- 6. Acute swelling and edema of the brain can cause protrusion of the cerebellar tonsil into the
- 7. Classification Location form: Nasopharyngitis; Carriers. Generalized form Meningitis; Mingococcemia; Fulminating form; Meningitis+ mingococcemia. Atypical form: Iridocyclochorioiditis;
- 8. Nasopharyngitis headache, painful swallowing, subfebrile temperature hyperemia of the nasopharyngeal mucosa and hyperplasia of lymphoid nodes
- 9. Meningitis The onset of the disease is usually violent, and a considerable elevation of temperature; severe
- 10. Meningeal symptoms hyperesthesia of the skin and increased sensitivity to light and sound stiffness of the
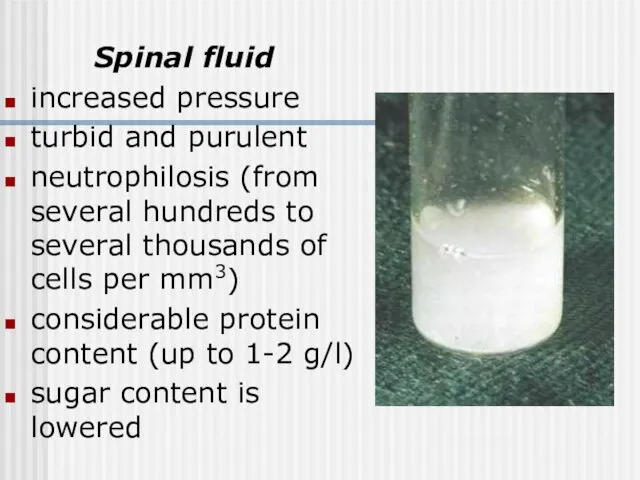
- 11. Spinal fluid increased pressure turbid and purulent neutrophilosis (from several hundreds to several thousands of cells
- 12. Blood leukocytosis (up to 20-40-109/1) neutrophilosis with a shift to the left aneosinophilia the ESR is
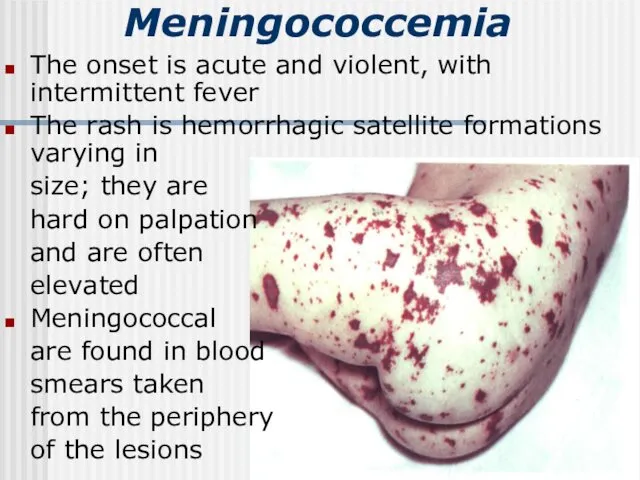
- 13. Meningococcemia The onset is acute and violent, with intermittent fever The rash is hemorrhagic satellite formations
- 15. Hypertoxic (fulminating) form A sudden turbulent onset Severe toxemia (uncontrollable vomiting, convulsions, mental confusion, cardiovascular weakness)
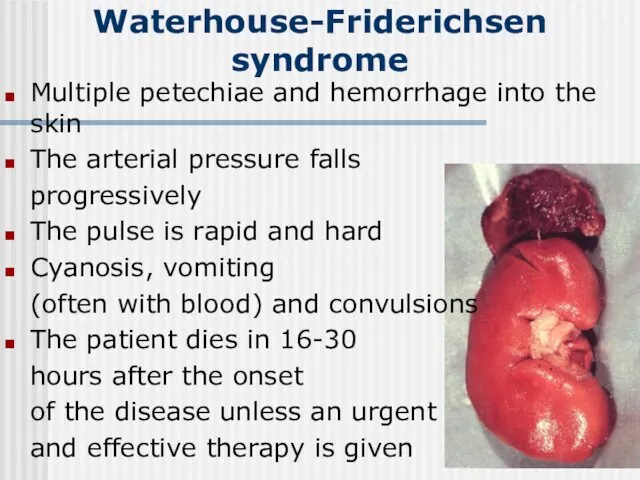
- 16. Waterhouse-Friderichsen syndrome Multiple petechiae and hemorrhage into the skin The arterial pressure falls progressively The pulse
- 17. Features peculiar to meningitis in infants The disease is accompanied with high temperature, general restlessness, vomiting,
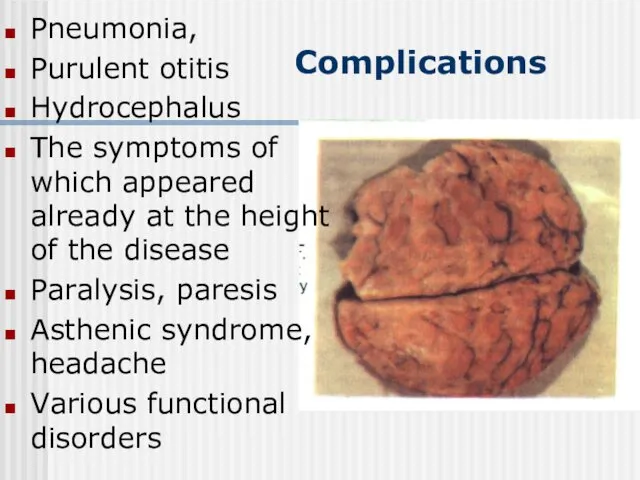
- 18. Complications Pneumonia, Purulent otitis Hydrocephalus The symptoms of which appeared already at the height of the
- 19. Diagnosis the clinical symptomatology and its course: acute onset and rapid development of meningeal symptoms The
- 20. Differential diagnosis Tuberculosis meningitis starts gradually and is accompanied with moderate pyrexia anamnesis and the results
- 21. Differential diagnosis Acute serous meningitis differs in the cerebrospinal fluid findings : complete transparency; moderately increased
- 22. Meningeal form of poliomyelitis The cerebrospinal fluid is transparent A slight or moderately increased cell count
- 23. Other purulent meningitis (staphylococcus, pneumococcus, Afanasyev-Pfeiffer bacillus, streptococcus ) develops secondarily to purulent otitis, pneumonia, sepsis
- 24. Meningococcemia of thrombopenic purpura and hemorrhagic vasculitis meningococcemia is characterized by high temperature, pronounced intoxication, marked
- 25. Prognosis Mortality from epidemic meningitis was very high (30 to 40 % on average) The worst
- 26. Etiotropic treatment Penicillin was first given dose of 300 000-400 000 units per kilogram of body
- 27. Toxicosis can be controlled by administration of large amounts of liquids electrolyte balance and osmotic pressure
- 28. Prophylaxis The following in an epidemic focus The patient is hospitalized and isolated to condition that
- 29. Acute Epidemic Poliomyelitis
- 30. Etiology the causative agent of polyomyelitis (Poliovirus hominis) a very small virus contains RNA is very
- 31. Epidemiology Sources of infection - patients with clinically manifest poliomyelitis, persons suffering from atypical and abortive
- 32. Pathogenesis The most probable portal of entry of the infection - the pharyngeal lymphoid ring and
- 33. Clinical Manifestations The incubation period of poliomyelitis averages from 5 to 14 days; it may sometimes
- 34. Preparalytic stage The disease starts acutely with a marked rise of temperature Catarrh of the upper
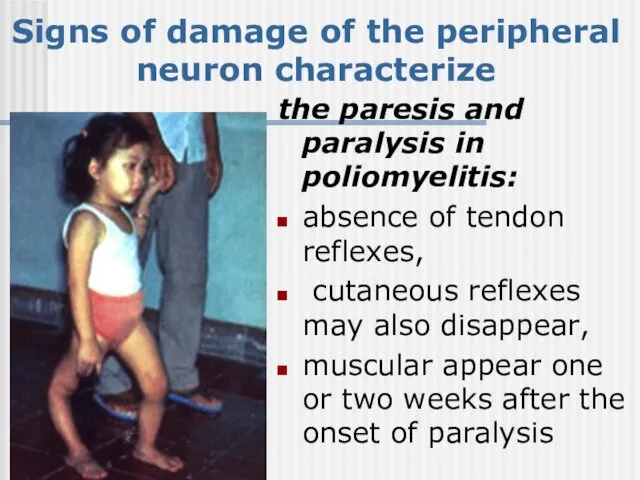
- 35. Paralytic stage The temperature falls at the end of the initial stage, and paresis and paralysis
- 36. Signs of damage of the peripheral neuron characterize the paresis and paralysis in poliomyelitis: absence of
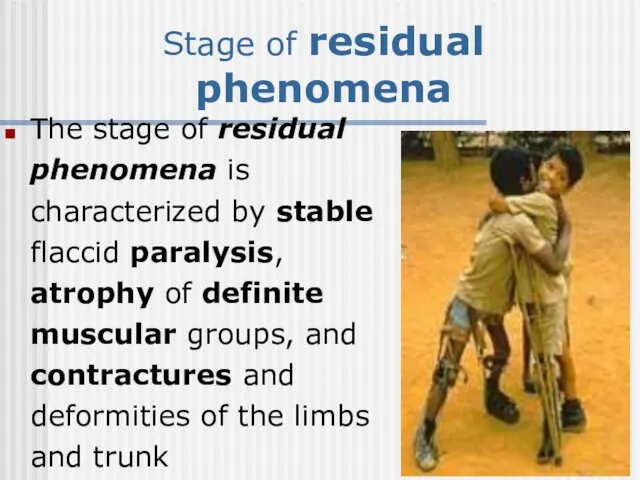
- 37. Stage of residual phenomena The stage of residual phenomena is characterized by stable flaccid paralysis, atrophy
- 38. Clinical forms of poliomyelitis paralytic poliomyelitis: a) spinal, b) bulbar, c) pontine, d) encephalitic aparalytic poliomyelitis:
- 39. Paralytic poliomyelitis The spinal form is characterized by flaccid paralysis of the limbs, trunk, neck and
- 40. Aparalytic poliomyelitis The visceral (or abortive) form shows symptoms of the initial stage of poliomyelitis. There
- 41. Diagnosis Rapid investigation suspected cases critical to identifying possible wild poliovirus transmission Clinical case definition Acute
- 42. Viral Isolation isolate wild polio virus from stool or pharynx; do genetic “finger printing” of virus
- 43. Treatment NO curative treatment Supportive care: aseptic meningitis- fluids, acetomenоphen, rest until fever improves, paralysis- pain
- 45. Скачать презентацию
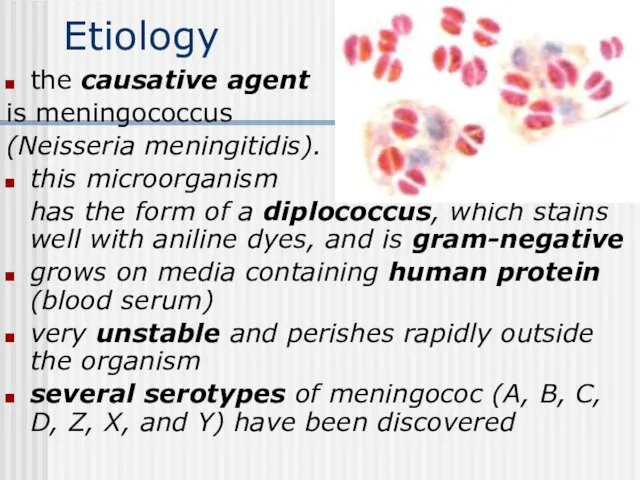
Etiology
the causative agent
is meningococcus
(Neisseria meningitidis).
this microorganism
has the
Etiology
the causative agent
is meningococcus
(Neisseria meningitidis).
this microorganism
has the
Epidemiology
the sources of infection are patient and carriers
meningococcus expel
Epidemiology
the sources of infection are patient and carriers
meningococcus expel
Pathogenesis and Pathology
The portal of the infection entry is the
Pathogenesis and Pathology
The portal of the infection entry is the
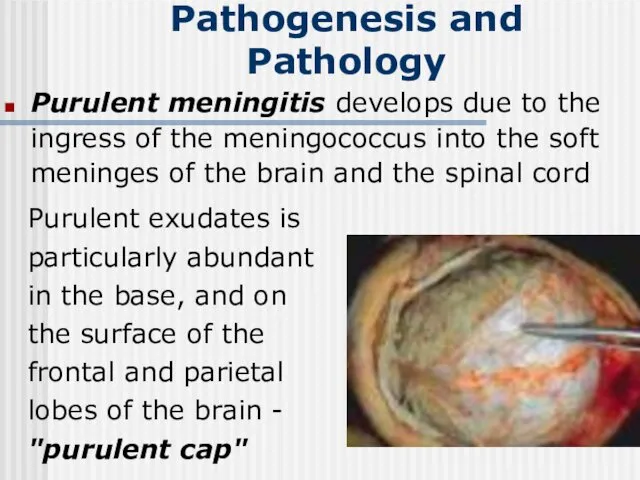
Purulent meningitis develops due to the ingress of the meningococcus into
Purulent meningitis develops due to the ingress of the meningococcus into
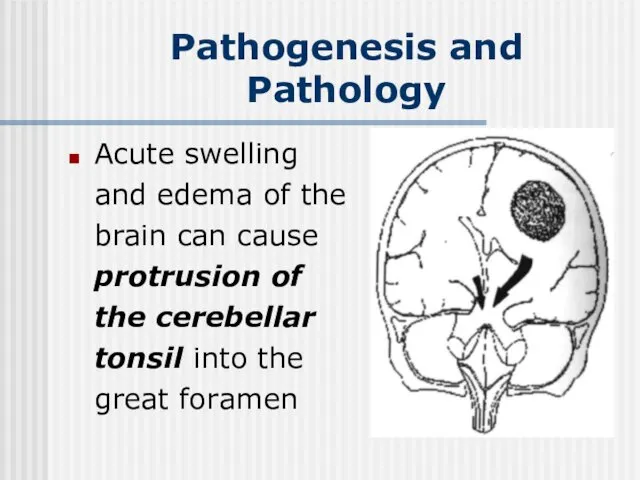
Acute swelling and edema of the brain can cause protrusion of
Acute swelling and edema of the brain can cause protrusion of
Classification
Location form:
Nasopharyngitis;
Carriers.
Generalized form
Meningitis;
Mingococcemia;
Fulminating form;
Meningitis+ mingococcemia.
Atypical form:
Iridocyclochorioiditis;
Pneumonia
Endocarditic.
Classification
Location form:
Nasopharyngitis;
Carriers.
Generalized form
Meningitis;
Mingococcemia;
Fulminating form;
Meningitis+ mingococcemia.
Atypical form:
Iridocyclochorioiditis;
Pneumonia
Endocarditic.
Nasopharyngitis
headache, painful swallowing, subfebrile temperature
hyperemia of the nasopharyngeal mucosa
Nasopharyngitis
headache, painful swallowing, subfebrile temperature
hyperemia of the nasopharyngeal mucosa
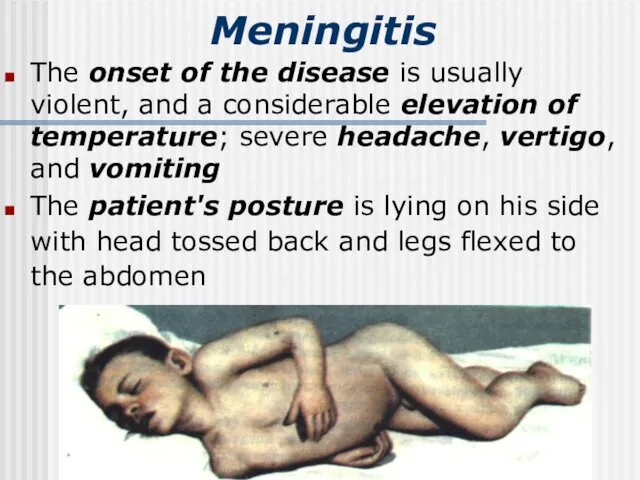
Meningitis
The onset of the disease is usually violent, and a
Meningitis
The onset of the disease is usually violent, and a
Meningeal symptoms
hyperesthesia of the skin and increased sensitivity to light
Meningeal symptoms
hyperesthesia of the skin and increased sensitivity to light
Spinal fluid
increased pressure
turbid and purulent
neutrophilosis (from several hundreds
Spinal fluid
increased pressure
turbid and purulent
neutrophilosis (from several hundreds
Blood
leukocytosis (up to 20-40-109/1)
neutrophilosis with a shift to the
Blood
leukocytosis (up to 20-40-109/1)
neutrophilosis with a shift to the
Meningococcemia
The onset is acute and violent, with intermittent fever
The
Meningococcemia
The onset is acute and violent, with intermittent fever
The


Hypertoxic (fulminating) form
A sudden turbulent onset
Severe toxemia (uncontrollable vomiting,
Hypertoxic (fulminating) form
A sudden turbulent onset
Severe toxemia (uncontrollable vomiting,
Waterhouse-Friderichsen syndrome
Multiple petechiae and hemorrhage into the skin
The arterial
Waterhouse-Friderichsen syndrome
Multiple petechiae and hemorrhage into the skin
The arterial
Features peculiar to meningitis in infants
The disease is accompanied with
Features peculiar to meningitis in infants
The disease is accompanied with
Complications
Pneumonia,
Purulent otitis
Hydrocephalus
The symptoms of which appeared already at
Complications
Pneumonia,
Purulent otitis
Hydrocephalus
The symptoms of which appeared already at
Diagnosis
the clinical symptomatology and its course: acute onset and rapid
Diagnosis
the clinical symptomatology and its course: acute onset and rapid
Differential diagnosis
Tuberculosis meningitis
starts gradually and is accompanied with moderate pyrexia
Differential diagnosis
Tuberculosis meningitis
starts gradually and is accompanied with moderate pyrexia
Differential diagnosis
Acute serous meningitis
differs in the cerebrospinal fluid findings :
Differential diagnosis
Acute serous meningitis
differs in the cerebrospinal fluid findings :
Meningeal form of poliomyelitis
The cerebrospinal fluid is transparent
A slight
Meningeal form of poliomyelitis
The cerebrospinal fluid is transparent
A slight
Other purulent meningitis (staphylococcus, pneumococcus, Afanasyev-Pfeiffer bacillus, streptococcus )
develops secondarily to
Other purulent meningitis (staphylococcus, pneumococcus, Afanasyev-Pfeiffer bacillus, streptococcus )
develops secondarily to
Meningococcemia of thrombopenic purpura and hemorrhagic vasculitis
meningococcemia is characterized by
Meningococcemia of thrombopenic purpura and hemorrhagic vasculitis
meningococcemia is characterized by
Prognosis
Mortality from epidemic meningitis was very high (30 to 40
Prognosis
Mortality from epidemic meningitis was very high (30 to 40
Etiotropic treatment
Penicillin was first given dose of 300 000-400 000
Etiotropic treatment
Penicillin was first given dose of 300 000-400 000
Toxicosis can be controlled by administration of large amounts of liquids
Toxicosis can be controlled by administration of large amounts of liquids
Prophylaxis
The following in an epidemic focus
The patient is hospitalized
Prophylaxis
The following in an epidemic focus
The patient is hospitalized
Acute Epidemic Poliomyelitis
Acute Epidemic Poliomyelitis
Etiology
the causative agent of polyomyelitis (Poliovirus hominis)
a very small virus
contains RNA
is
Etiology
the causative agent of polyomyelitis (Poliovirus hominis)
a very small virus
contains RNA
is
Epidemiology
Sources of infection - patients with clinically manifest poliomyelitis, persons suffering
Epidemiology
Sources of infection - patients with clinically manifest poliomyelitis, persons suffering
Pathogenesis
The most probable portal of entry of the infection - the
Pathogenesis
The most probable portal of entry of the infection - the
Clinical Manifestations
The incubation period of poliomyelitis averages from 5 to 14
Clinical Manifestations
The incubation period of poliomyelitis averages from 5 to 14
Preparalytic stage
The disease starts acutely with a marked rise of temperature
Catarrh
Preparalytic stage
The disease starts acutely with a marked rise of temperature
Catarrh
Paralytic stage
The temperature falls at the end of the initial stage,
Paralytic stage
The temperature falls at the end of the initial stage,
Signs of damage of the peripheral neuron characterize
the paresis and paralysis
Signs of damage of the peripheral neuron characterize
the paresis and paralysis
Stage of residual phenomena
The stage of residual phenomena is characterized
Stage of residual phenomena
The stage of residual phenomena is characterized
Clinical forms of poliomyelitis
paralytic poliomyelitis:
a) spinal,
b) bulbar,
c) pontine,
Clinical forms of poliomyelitis
paralytic poliomyelitis:
a) spinal,
b) bulbar,
c) pontine,
Paralytic poliomyelitis
The spinal form is characterized by flaccid paralysis of the
Paralytic poliomyelitis
The spinal form is characterized by flaccid paralysis of the
Aparalytic poliomyelitis
The visceral (or abortive) form shows symptoms of the initial
Aparalytic poliomyelitis
The visceral (or abortive) form shows symptoms of the initial
Diagnosis
Rapid investigation suspected cases
critical to identifying possible wild
Diagnosis
Rapid investigation suspected cases
critical to identifying possible wild
Viral Isolation
isolate wild polio virus from stool or pharynx;
Viral Isolation
isolate wild polio virus from stool or pharynx;
Treatment
NO curative treatment
Supportive care:
aseptic meningitis- fluids, acetomenоphen,
rest until fever
Treatment
NO curative treatment
Supportive care:
aseptic meningitis- fluids, acetomenоphen,
rest until fever
 Андреас Везалий
Андреас Везалий Бронхиальная астма
Бронхиальная астма Өкпенің инфильтратты туберкулезі
Өкпенің инфильтратты туберкулезі Травма живота
Травма живота Патологические роды у мелких домашних животных. Кесарево сечение
Патологические роды у мелких домашних животных. Кесарево сечение Оборудование группы среднего возраста
Оборудование группы среднего возраста Дифтерия у детей
Дифтерия у детей Методы определения центрального соотношения челюстей в стоматологии
Методы определения центрального соотношения челюстей в стоматологии Группа природных фенольных соединений - антраценпроизводные
Группа природных фенольных соединений - антраценпроизводные Нейротропные средства
Нейротропные средства Тамақтан улану кезіндегі алғашқы . Шұғыл әрекеттер
Тамақтан улану кезіндегі алғашқы . Шұғыл әрекеттер Адаптация человека к условиям среды обитания
Адаптация человека к условиям среды обитания Гипоксия плода и асфиксия новорожденного
Гипоксия плода и асфиксия новорожденного Психические расстройства при эпилепсии
Психические расстройства при эпилепсии Формулярлық жүйенің рөлі. Дәрілік формулярды құрастыру. Қазақстандық ұлттық формулярдың рөлі
Формулярлық жүйенің рөлі. Дәрілік формулярды құрастыру. Қазақстандық ұлттық формулярдың рөлі Основы физической реабилитации: медицинские группы для занятий физической культурой
Основы физической реабилитации: медицинские группы для занятий физической культурой Визначення чинників розвитку безпліддя у пацієнтів та аналіз факторів, які його викликають
Визначення чинників розвитку безпліддя у пацієнтів та аналіз факторів, які його викликають Ревматоидный артрит
Ревматоидный артрит Ультразвуковое исследование поджелудочной железы
Ультразвуковое исследование поджелудочной железы Офтальмология. АФО органа зрения
Офтальмология. АФО органа зрения Культура общения медсестры с пациентом
Культура общения медсестры с пациентом Дыхательная недостаточность у детей
Дыхательная недостаточность у детей Основные мышцы человека и их функции
Основные мышцы человека и их функции Өкпенің жедел диссеминирлі туберкулезі
Өкпенің жедел диссеминирлі туберкулезі Опыт использования системной гипотермии у новорожденных, родившихся в тяжелой асфиксии
Опыт использования системной гипотермии у новорожденных, родившихся в тяжелой асфиксии Острый коронарный синдром
Острый коронарный синдром Chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease Новые пероральные антикоагулянты
Новые пероральные антикоагулянты