- Morphine

Содержание
- 2. HISTORY Morphine was isolated from raw opium in 1805 by a German pharmacologist Friedrich Wilhelm Adam
- 3. HISTORY Barely eighteen years after morphine was discovered, it was used for homicide. In 1823, a
- 4. HISTORY In fact the name morphine comes from the Greek 'god of dreams Morpheus. Incidentally Morpheus
- 5. DEFINITION Morphine is a natural opium alkaloid. It is a dried extract obtained from the capsules
- 6. CLASSIFICATION
- 7. CLASSIFICATION Heroine Pholcodeine
- 8. MECHANISM OF ACTION Opioids exert their major effects by interacting with opioid receptors in the CNS
- 9. MECHANISM OF ACTION Opioids have an onset of action that depends on the route of administration
- 10. SCHEMATIC DIAGRAM ILLUSTRATING THE ROLE OF OPIOIDS IN ANALGESIA OF PERIPHERAL MECHANISM OF ACTION
- 11. PHARMACOKINETICS Absorption of morphine from Gl T is slow and incomplete Quick effect is produced on
- 12. PHARMACOLOGICAL ACTIONS 1. Analgesia - Morphine causes analgesia - Morphine relieves severe deep seated pain like
- 13. PHARMACOLOGICAL ACTIONS 2. CNS - Morphine produces euphoria in presence of pain - But in the
- 14. PHARMACOLOGICAL ACTIONS 4. Anti-tussive property - Morphine has anti-tussive property - Morphine depress the medularly cough
- 15. PHARMACOLOGICAL ACTIONS 6. Papillary constriction - Morphine produces constriction of pupil (miosis) - Miosis is induced
- 16. PHARMACOLOGICAL ACTIONS 7. Respiration - The action of morphine on the respiration is dose dependent -
- 17. PHARMACOLOGICAL ACTIONS 9. Gastro-intestinal tract - Morphine decreases peristaltic propulsive movements - It produces spasm of
- 18. PHARMACOLOGICAL ACTIONS 11. Cardiovascular system - Normal dose of morphine produces no effect on heart rate,
- 19. PHARMACOLOGICAL ACTIONS 12. Histamine release - Morphine releases histamine from mast cells, causing urticaria, sweating and
- 20. PHARMACOLOGICAL ACTIONS 14. Uterus - No significant effect. May prolong labor in high doses 15. On
- 21. ADVERSE REACTIONS Acute morphine poisoning characterized by respiratory depression, pin point pupil cyanosis, reduced body temperature,
- 22. ADVERSE REACTIONS Drug interactions - The depressant actions of morphine are enhanced by phenothiazines, monoamine oxidase
- 23. CONTRAINDICTIONS - Infants and elder people - Respiratory conditions such as bronchial asthma - Head injury
- 24. DOSAGE
- 25. USES 1. It is an analgesic for the relief of severe pain 2. Used as pre-anesthetic
- 27. Скачать презентацию
HISTORY
Morphine was isolated from raw opium in 1805 by a German
HISTORY
Morphine was isolated from raw opium in 1805 by a German
HISTORY
Barely eighteen years after morphine was discovered, it was used for
HISTORY
Barely eighteen years after morphine was discovered, it was used for
HISTORY
In fact the name morphine comes from the Greek 'god of
HISTORY
In fact the name morphine comes from the Greek 'god of
DEFINITION
Morphine is a natural opium alkaloid.
It is a dried extract obtained
DEFINITION
Morphine is a natural opium alkaloid.
It is a dried extract obtained
CLASSIFICATION
CLASSIFICATION
CLASSIFICATION
Heroine
Pholcodeine
CLASSIFICATION
Heroine
Pholcodeine
MECHANISM OF ACTION
Opioids exert their major effects by interacting with opioid
MECHANISM OF ACTION
Opioids exert their major effects by interacting with opioid
MECHANISM OF ACTION
Opioids have an onset of action that depends on
MECHANISM OF ACTION
Opioids have an onset of action that depends on
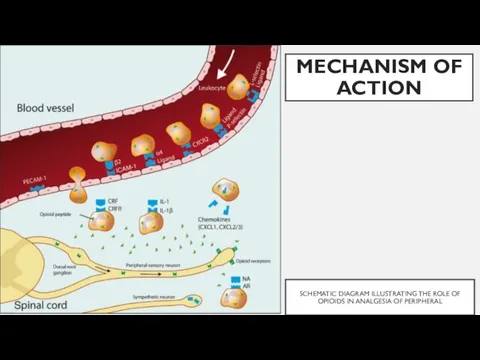
SCHEMATIC DIAGRAM ILLUSTRATING THE ROLE OF OPIOIDS IN ANALGESIA OF PERIPHERAL
MECHANISM
SCHEMATIC DIAGRAM ILLUSTRATING THE ROLE OF OPIOIDS IN ANALGESIA OF PERIPHERAL
MECHANISM
PHARMACOKINETICS
Absorption of morphine from Gl T is slow and incomplete
Quick effect
PHARMACOKINETICS
Absorption of morphine from Gl T is slow and incomplete
Quick effect
PHARMACOLOGICAL ACTIONS
1. Analgesia
- Morphine causes analgesia
- Morphine relieves severe deep seated
PHARMACOLOGICAL ACTIONS
1. Analgesia
- Morphine causes analgesia
- Morphine relieves severe deep seated
PHARMACOLOGICAL ACTIONS
2. CNS
- Morphine produces euphoria in presence of pain
- But
PHARMACOLOGICAL ACTIONS
2. CNS
- Morphine produces euphoria in presence of pain
- But
PHARMACOLOGICAL ACTIONS
4. Anti-tussive property
- Morphine has anti-tussive property
- Morphine depress the
PHARMACOLOGICAL ACTIONS
4. Anti-tussive property
- Morphine has anti-tussive property
- Morphine depress the
PHARMACOLOGICAL ACTIONS
6. Papillary constriction
- Morphine produces constriction of pupil (miosis)
- Miosis
PHARMACOLOGICAL ACTIONS
6. Papillary constriction
- Morphine produces constriction of pupil (miosis)
- Miosis
PHARMACOLOGICAL ACTIONS
7. Respiration
- The action of morphine on the respiration is
PHARMACOLOGICAL ACTIONS
7. Respiration
- The action of morphine on the respiration is
PHARMACOLOGICAL ACTIONS
9. Gastro-intestinal tract
- Morphine decreases peristaltic propulsive movements
- It produces
PHARMACOLOGICAL ACTIONS
9. Gastro-intestinal tract
- Morphine decreases peristaltic propulsive movements
- It produces
PHARMACOLOGICAL ACTIONS
11. Cardiovascular system
- Normal dose of morphine produces no effect
PHARMACOLOGICAL ACTIONS
11. Cardiovascular system
- Normal dose of morphine produces no effect
PHARMACOLOGICAL ACTIONS
12. Histamine release
- Morphine releases histamine from mast cells, causing
PHARMACOLOGICAL ACTIONS
12. Histamine release
- Morphine releases histamine from mast cells, causing
PHARMACOLOGICAL ACTIONS
14. Uterus
- No significant effect. May prolong labor in high
PHARMACOLOGICAL ACTIONS
14. Uterus
- No significant effect. May prolong labor in high
ADVERSE REACTIONS
Acute morphine poisoning characterized by respiratory depression, pin point pupil
ADVERSE REACTIONS
Acute morphine poisoning characterized by respiratory depression, pin point pupil
ADVERSE REACTIONS
Drug interactions
- The depressant actions of morphine are enhanced by
ADVERSE REACTIONS
Drug interactions
- The depressant actions of morphine are enhanced by
CONTRAINDICTIONS
- Infants and elder people
- Respiratory conditions such as bronchial asthma
-
CONTRAINDICTIONS
- Infants and elder people
- Respiratory conditions such as bronchial asthma
-
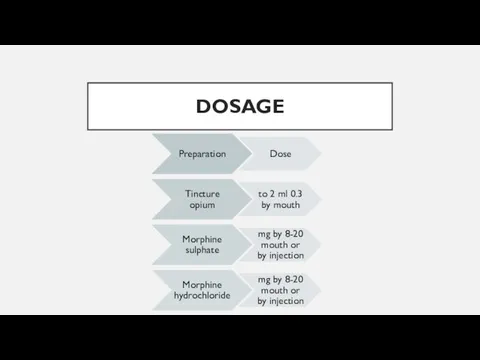
DOSAGE
DOSAGE
USES
1. It is an analgesic for the relief of severe pain
USES
1. It is an analgesic for the relief of severe pain
 Терминальное состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного
Терминальное состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного Абдомінальний ішемічний синдром. Тема 05
Абдомінальний ішемічний синдром. Тема 05 Нутритивная поддержка в хирургии. Обзор современных клинических рекомендаций
Нутритивная поддержка в хирургии. Обзор современных клинических рекомендаций История изучения сердечно-сосудистой системы
История изучения сердечно-сосудистой системы Учение о биосфере. Ноосфера. (Лекция 18)
Учение о биосфере. Ноосфера. (Лекция 18) Клинические рекомендации пациенту с заболеванием мочеполовой системы. Тактика ведения пациента на уровне ПМСП
Клинические рекомендации пациенту с заболеванием мочеполовой системы. Тактика ведения пациента на уровне ПМСП Кроветворение (гемопоэз) – образование клеток крови в красном костном мозге
Кроветворение (гемопоэз) – образование клеток крови в красном костном мозге Обмороження та його періоди. Класифікація обмороження. Домедична допомога при обмороженнях
Обмороження та його періоди. Класифікація обмороження. Домедична допомога при обмороженнях ХТА пестицидов ФОС
ХТА пестицидов ФОС Атомная медицина и медицинская физика
Атомная медицина и медицинская физика Внематочная беременность
Внематочная беременность История сестринского дела
История сестринского дела Гирсутизм. Вирилизация. Гипертрихоз
Гирсутизм. Вирилизация. Гипертрихоз Коронавирус 2019, профилактика, санитарно-просветительская работа
Коронавирус 2019, профилактика, санитарно-просветительская работа Қарыншалар гипертрофиясының ЭКГ белгілері
Қарыншалар гипертрофиясының ЭКГ белгілері Багатоплідна вагітність
Багатоплідна вагітність Фізіологічні основи оздоровчої фізичної культури
Фізіологічні основи оздоровчої фізичної культури Больные с заболеваниями крови и органов кроветворения
Больные с заболеваниями крови и органов кроветворения Возрастные особенности строения уха
Возрастные особенности строения уха Раны. Классификация ран. Лечение чистой раны
Раны. Классификация ран. Лечение чистой раны Обмен нуклеотидов. Матричные биосинтезы
Обмен нуклеотидов. Матричные биосинтезы Переломы скуловых костей и дуг
Переломы скуловых костей и дуг Бейспецификалық жаралы колит
Бейспецификалық жаралы колит Травма позвоночника
Травма позвоночника Фенотипические особенности наследственных синдромов рака молочной железы и яичников среди татарского этноса
Фенотипические особенности наследственных синдромов рака молочной железы и яичников среди татарского этноса Профессиональное здоровье педагогов по результатам социологического опроса
Профессиональное здоровье педагогов по результатам социологического опроса בן 45עם כאבי פרקים סימטרים עם נפיחויות ,קשיון בוקר מעל שעה חודשיים
בן 45עם כאבי פרקים סימטרים עם נפיחויות ,קשיון בוקר מעל שעה חודשיים Демография. Медицинская демография
Демография. Медицинская демография