- Multi drug resistant tuberculosis. MDR-TB. (Lecture 6)

Содержание
- 2. An estimated 2 billion people – one-third of the global population – are infected with tuberculosis
- 3. Although TB is a global problem, its geographic distribution is drastically disproportionate. Ninety-five percent of all
- 4. TB is a major killer among women of reproductive age and the leading cause of death
- 5. The global resurgence of TB has been fueled by a combination of factors, including increasing rates
- 6. Multidrug-resistant tuberculosis ( MDR-TB) is a form of TB caused by bacteria that do not respond
- 7. Extensively drug-resistant TB (XDR-TB) is a rare type of MDR TB that is resistant to isoniazid
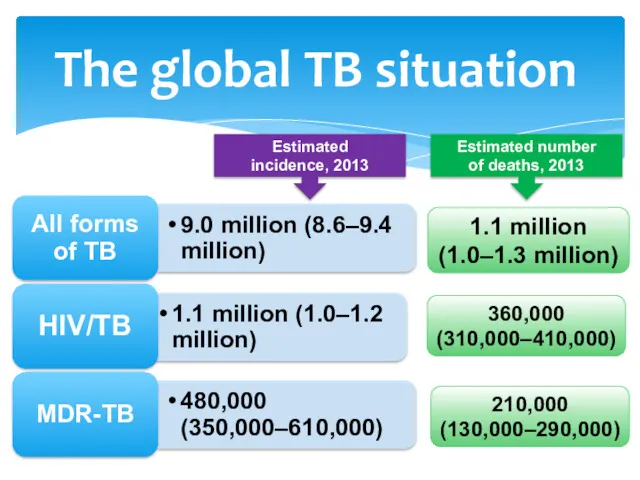
- 8. The global TB situation Estimated incidence, 2013 Estimated number of deaths, 2013 1.1 million (1.0–1.3 million)
- 9. Globally in 2013, an estimated 480 000 people developed MDR-TB and there were an estimated 210
- 10. A total of 97 000 patients were started on MDR-TB treatment in 2013, a three-fold increase
- 11. HIV/AIDS and TB co-infection present special challenges to the expansion and effectiveness of DOTS programs and
- 12. The dual epidemics of TB and HIV are particularly pervasive in Africa, where HIV has been
- 13. The dual epidemics are also of growing concern in Asia, where two-thirds of TB-infected people live
- 14. The overlap of TB-HIV co-infection with MDR-TB and extensively drug-resistant TB presents a tremendous challenge and
- 15. Individuals co-infected with HIV and TB are 30 times more likely to progress to active TB
- 16. In addition, clinical trials have shown that there are anti-TB regimens that can prevent or decrease
- 17. Global trends in estimated rates of TB incidence, prevalence and mortality Global trends in estimated incidence
- 18. 67th World Health Assembly, Geneva, May 2014
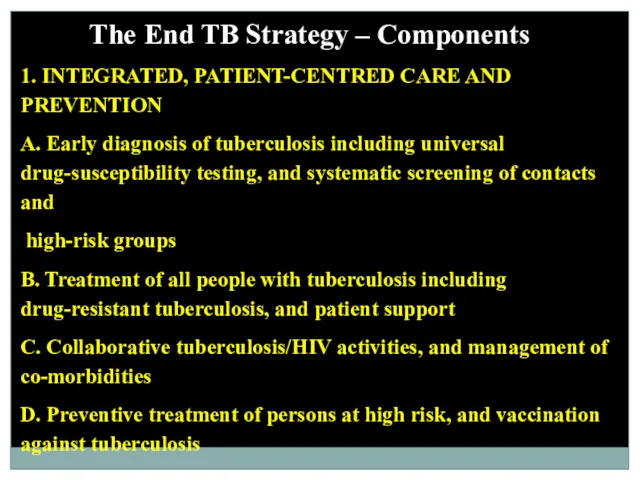
- 19. The End TB Strategy – Components 1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION A. Early diagnosis of
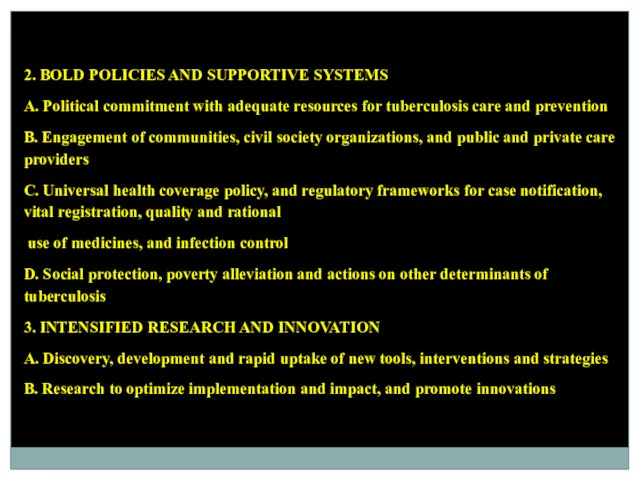
- 20. 2. BOLD POLICIES AND SUPPORTIVE SYSTEMS A. Political commitment with adequate resources for tuberculosis care and
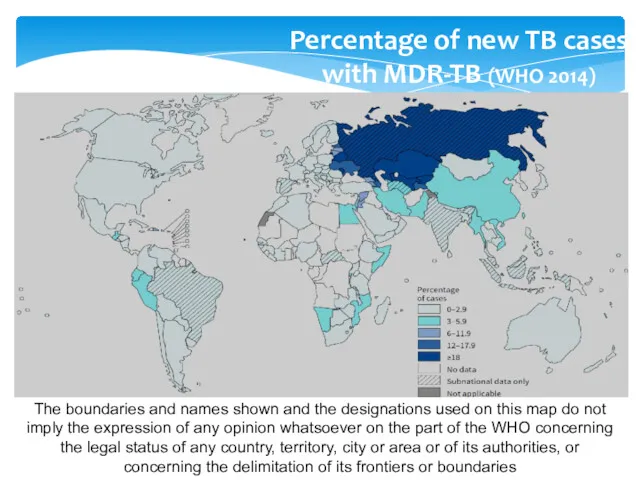
- 21. Percentage of new TB cases with MDR-TB (WHO 2014) The boundaries and names shown and the
- 22. Five priority actions to address the global MDR-TB crisis
- 23. Diagnosing drug-resistant TB Since there are no specific clinical or radiographic features to distinguish HIV-infected patients
- 24. Sputum and other clinical specimens – such as pleural or bronchoalveolar lavage fluid and tissue from
- 25. At present, the rapid DST of choice in individuals suspected of MDR-TB is the Xpert MTB/RIF
- 27. The test is based on real-time polymerase chain reaction (PCR) technology targeting specific nucleic acid sequences
- 28. 1. For TB detection, Xpert MTB/RIF is substantially more sensitive than microscopy. Sensitivity is close to
- 29. 1. Diagnosing XDR-TB is done through conventional phenotypic DST for the injectable drugs (kanamycin/amikacin and capreomycin)
- 30. Diagnosis of MDR-TB in people living with HIV Xpert MTB/RIF is the recommended test for drug
- 31. Laboratory confirmation of MDR-TB may be difficult or impossible (e.g., extrapulmonary TB) for many coinfected patients,
- 32. Immune reconstitution inflammatory syndrome (IRIS) is an exaggerated immune response to a previously undiagnosed opportunistic infection
- 33. Mild to moderate TB-IRIS is relatively common, especially in severely immunosuppressed patients (CD4 count TB-IRIS can
- 34. Principles of MDR-TB treatment The intensive phase should include at least four core second-line anti-TB drugs
- 35. Each dose is given under directly observed therapy (DOT) throughout the treatment. A treatment card is
- 36. Empiric refers to the initiation of treatment prior to determination of a firm diagnosis of DR-TB.
- 37. People living with HIV are vulnerable to MDR-TB infection and are at high risk of developing
- 38. MDR-TB patients who are already on ART should continue it. WHO recommends that MDR-TB patients who
- 39. A first-line ART regimen should include two nucleoside reverse-transcriptase inhibitors (NRTIs) plus a non-nucleoside reverse-transcriptase inhibitor
- 40. AZT (azt, retrovir) – a drug that suppresses the replication (reproduction) of HIV EPIVIR 3TC –
- 41. Infection control for MDR-TB
- 42. Administrative controls Outpatient settings Patients should be screened for cough as they enter into the health
- 43. Inpatient settings The circulation of visitors, patients, and their attendants in the hospital needs to be
- 44. TB wards must be well-ventilated and separated from the other wards in the health structure compound:
- 45. Environmental controls Ventilation Ventilation is the most effective means for reducing the concentration of M. tuberculosis
- 46. TB infection control should be considered during the planning stages of new health structures and those
- 47. Ultraviolet germicidal irradiation (UVGI) M. tuberculosis is sensitive to germicidal radiation of UV found in the
- 48. Personal protection Respirators Respirators (also known as high-filtration masks, N95 masks, or FFP2 masks) provide a
- 50. Attendants and visitors must wear a high-filtration mask (like those worn by staff) when entering a
- 51. Simple cloth masks and surgical masks Contagious patients must wear a simple cloth, surgical, or face
- 52. Waste management In wards, where patients are coughing regularly, sputum containers should be about 200 mL,
- 54. Скачать презентацию
An estimated 2 billion people – one-third of the global population
An estimated 2 billion people – one-third of the global population
Although TB is a global problem, its geographic distribution is drastically
Although TB is a global problem, its geographic distribution is drastically
TB is a major killer among women of reproductive age and
TB is a major killer among women of reproductive age and
The global resurgence of TB has been fueled by a combination
The global resurgence of TB has been fueled by a combination
Multidrug-resistant tuberculosis ( MDR-TB) is a form of TB caused by
Multidrug-resistant tuberculosis ( MDR-TB) is a form of TB caused by
Extensively drug-resistant TB (XDR-TB)
is a rare type of MDR TB
Extensively drug-resistant TB (XDR-TB)
is a rare type of MDR TB
The global TB situation
Estimated
incidence, 2013
Estimated number
of deaths, 2013
1.1 million
(1.0–1.3 million)
360,000
(310,000–410,000)
210,000
(130,000–290,000)
The global TB situation
Estimated
incidence, 2013
Estimated number
of deaths, 2013
1.1 million
(1.0–1.3 million)
360,000
(310,000–410,000)
210,000
(130,000–290,000)
Globally in 2013, an estimated 480 000 people developed MDR-TB and
Globally in 2013, an estimated 480 000 people developed MDR-TB and
A total of 97 000 patients were started on MDR-TB treatment
A total of 97 000 patients were started on MDR-TB treatment
HIV/AIDS and TB co-infection present special challenges to the expansion and
HIV/AIDS and TB co-infection present special challenges to the expansion and
The dual epidemics of TB and HIV are particularly pervasive in
The dual epidemics of TB and HIV are particularly pervasive in
The dual epidemics are also of growing concern in Asia, where
The dual epidemics are also of growing concern in Asia, where
The overlap of TB-HIV co-infection with MDR-TB and extensively drug-resistant TB
The overlap of TB-HIV co-infection with MDR-TB and extensively drug-resistant TB
Individuals co-infected with HIV and TB are 30 times more likely
Individuals co-infected with HIV and TB are 30 times more likely
In addition, clinical trials have shown that there are anti-TB regimens
In addition, clinical trials have shown that there are anti-TB regimens
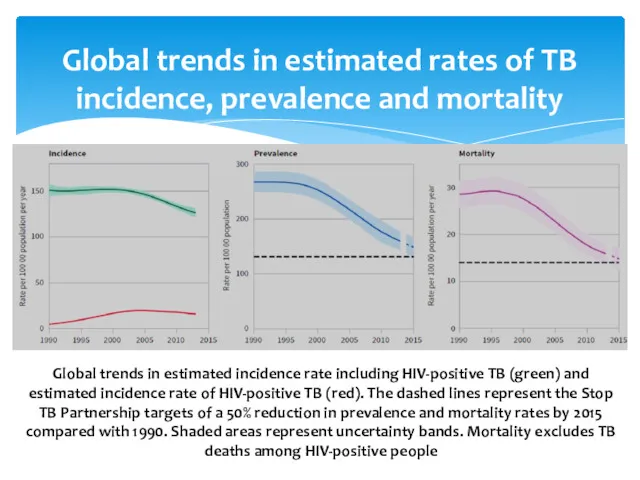
Global trends in estimated rates of TB incidence, prevalence and mortality
Global trends in estimated rates of TB incidence, prevalence and mortality
67th World Health Assembly, Geneva, May 2014
67th World Health Assembly, Geneva, May 2014
The End TB Strategy – Components
1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION
A.
The End TB Strategy – Components
1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION
A.
2. BOLD POLICIES AND SUPPORTIVE SYSTEMS
A. Political commitment with adequate resources
2. BOLD POLICIES AND SUPPORTIVE SYSTEMS
A. Political commitment with adequate resources
Percentage of new TB cases
with MDR-TB (WHO 2014)
The boundaries and
Percentage of new TB cases
with MDR-TB (WHO 2014)
The boundaries and
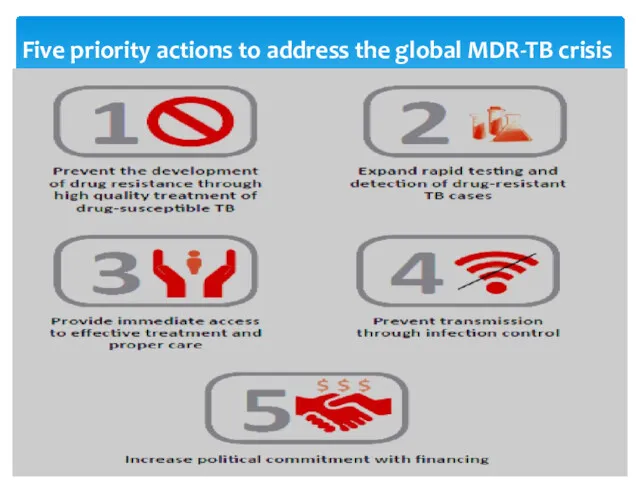
Five priority actions to address the global MDR-TB crisis
Five priority actions to address the global MDR-TB crisis
Diagnosing drug-resistant TB
Since there are no specific clinical or radiographic features
Diagnosing drug-resistant TB
Since there are no specific clinical or radiographic features
Sputum and other clinical specimens – such as pleural or bronchoalveolar
Sputum and other clinical specimens – such as pleural or bronchoalveolar
At present, the rapid DST of choice in individuals suspected of
At present, the rapid DST of choice in individuals suspected of
The test is based on real-time polymerase chain reaction (PCR) technology
The test is based on real-time polymerase chain reaction (PCR) technology
1. For TB detection, Xpert MTB/RIF is substantially more sensitive than
1. For TB detection, Xpert MTB/RIF is substantially more sensitive than
1. Diagnosing XDR-TB is done through conventional phenotypic DST for the
1. Diagnosing XDR-TB is done through conventional phenotypic DST for the
Diagnosis of MDR-TB in people living with HIV
Xpert MTB/RIF is the
Diagnosis of MDR-TB in people living with HIV
Xpert MTB/RIF is the
Laboratory confirmation of MDR-TB may be difficult or impossible (e.g., extrapulmonary
Laboratory confirmation of MDR-TB may be difficult or impossible (e.g., extrapulmonary
Immune reconstitution inflammatory syndrome (IRIS) is an exaggerated immune response to
Immune reconstitution inflammatory syndrome (IRIS) is an exaggerated immune response to
Mild to moderate TB-IRIS is relatively common, especially in severely immunosuppressed
Mild to moderate TB-IRIS is relatively common, especially in severely immunosuppressed
Principles of MDR-TB treatment
The intensive phase should include at least four
Principles of MDR-TB treatment
The intensive phase should include at least four
Each dose is given under directly observed therapy (DOT) throughout the
Each dose is given under directly observed therapy (DOT) throughout the
Empiric refers to the initiation of treatment prior to determination of
Empiric refers to the initiation of treatment prior to determination of
People living with HIV are vulnerable to MDR-TB infection and are
People living with HIV are vulnerable to MDR-TB infection and are
MDR-TB patients who are already on ART should continue it.
WHO recommends
MDR-TB patients who are already on ART should continue it.
WHO recommends
A first-line ART regimen should include two nucleoside reverse-transcriptase inhibitors (NRTIs)
A first-line ART regimen should include two nucleoside reverse-transcriptase inhibitors (NRTIs)
AZT (azt, retrovir) – a drug that suppresses the replication (reproduction)
AZT (azt, retrovir) – a drug that suppresses the replication (reproduction)

Infection control for MDR-TB
Infection control for MDR-TB
Administrative controls
Outpatient settings
Patients should be screened for cough as they enter
Administrative controls
Outpatient settings
Patients should be screened for cough as they enter
Inpatient settings
The circulation of visitors, patients, and their attendants in the
Inpatient settings
The circulation of visitors, patients, and their attendants in the
TB wards must be well-ventilated and separated from the other wards
TB wards must be well-ventilated and separated from the other wards
Environmental controls
Ventilation
Ventilation is the most effective means for reducing the concentration
Environmental controls
Ventilation
Ventilation is the most effective means for reducing the concentration
TB infection control should be considered during the planning stages of
TB infection control should be considered during the planning stages of
Ultraviolet germicidal irradiation (UVGI)
M. tuberculosis is sensitive to germicidal radiation of
Ultraviolet germicidal irradiation (UVGI)
M. tuberculosis is sensitive to germicidal radiation of
Personal protection
Respirators
Respirators (also known as high-filtration masks, N95 masks, or FFP2
Personal protection
Respirators
Respirators (also known as high-filtration masks, N95 masks, or FFP2
Attendants and visitors must wear a high-filtration mask (like those worn
Attendants and visitors must wear a high-filtration mask (like those worn
Simple cloth masks and surgical masks
Contagious patients must wear a simple
Simple cloth masks and surgical masks
Contagious patients must wear a simple
Waste management
In wards, where patients are coughing regularly, sputum containers should
Waste management
In wards, where patients are coughing regularly, sputum containers should
 Трансплантация почки
Трансплантация почки Дифференциальная диагностика синдрома крупа у детей
Дифференциальная диагностика синдрома крупа у детей Мочекаменная болезнь
Мочекаменная болезнь Абсцессы и флегмоны скуловой области
Абсцессы и флегмоны скуловой области Основы здорового образа жизни студента. Физическая культура в обеспечении здоровья
Основы здорового образа жизни студента. Физическая культура в обеспечении здоровья Наркомании и токсикомании
Наркомании и токсикомании Тиісті фармацевтикалық практика GPP
Тиісті фармацевтикалық практика GPP Инсульт. Бас ми қан айналым жүйесінің жедел бұзылулары
Инсульт. Бас ми қан айналым жүйесінің жедел бұзылулары Тунельные синдромы срединного нерва
Тунельные синдромы срединного нерва Лекарственные средства, подлежащие предметно-количественному учету
Лекарственные средства, подлежащие предметно-количественному учету Период школьного, подросткового и юношеского возраста
Период школьного, подросткового и юношеского возраста Физическое развитие и функциональное состояние организма. Медицинский контроль
Физическое развитие и функциональное состояние организма. Медицинский контроль Lingua latina. Receptum
Lingua latina. Receptum Актиномицеты сем. Actinomycetaceae
Актиномицеты сем. Actinomycetaceae Генетика пола. Наследование, сцепленное с полом
Генетика пола. Наследование, сцепленное с полом Пароксизмдік тахикардия. АВ блокада
Пароксизмдік тахикардия. АВ блокада Гігієнічні вимоги до персоналу. Перечень рекомендуемых стандартных операционных процедур для построения системы фармаконадзора
Гігієнічні вимоги до персоналу. Перечень рекомендуемых стандартных операционных процедур для построения системы фармаконадзора Сосудистая хирургия
Сосудистая хирургия Мойын, кеуде, бел, сегізкөз және құйымшақ омыртқаларының құрылыс ерекшеліктері
Мойын, кеуде, бел, сегізкөз және құйымшақ омыртқаларының құрылыс ерекшеліктері Гален. О частях человеческого тела
Гален. О частях человеческого тела Некоторые вопросы гигиены детей и подростков
Некоторые вопросы гигиены детей и подростков Лечение в раннем восстановительном периоде перинатального поражения мозга
Лечение в раннем восстановительном периоде перинатального поражения мозга Көпір тәрізді протез
Көпір тәрізді протез Chemistry, food & health
Chemistry, food & health Медицинская служба Вооруженных сил РФ в ЧС
Медицинская служба Вооруженных сил РФ в ЧС Дисплазия тазобедренного сустава
Дисплазия тазобедренного сустава Геморрагические лихорадки
Геморрагические лихорадки Заболевания,подлежащие мониторингу. Программы управления заболеваниями
Заболевания,подлежащие мониторингу. Программы управления заболеваниями