- Multiple Sclerois

Содержание
- 2. Topic outlines Incidence Definition of MS Etiology pathophysiology Classification of MS Clinical manifestation Risk factors Diagnosis
- 3. -MS was first describe in 1868 Jean-Martin Charcot. -The name multiple sclerosis refer to the numerous
- 4. Incidence 2.5 million people are affected with MS worldwide . High prevalence rates (over 30 per
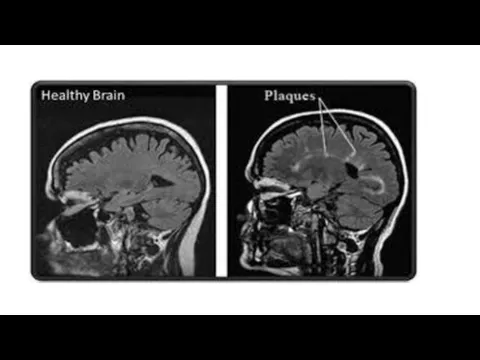
- 5. Definition -MS : Is a chronic , progressive , degenerative disorder of the CNS, characterized by
- 6. MS-Etiology The cause of MS unknown although research findings suggest that MS is related to infectious
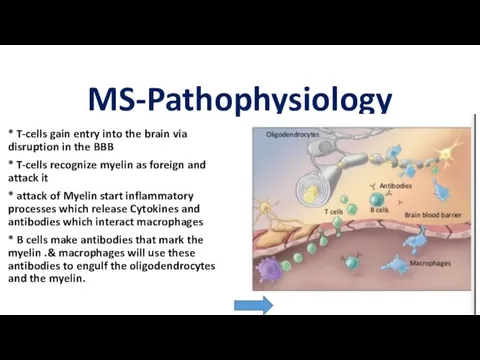
- 7. MS-Pathophysiology * T-cells gain entry into the brain via disruption in the BBB * T-cells recognize
- 8. * Without Oligodendrocytes there's no more remyelination to the axon. * In MS immune attack happen
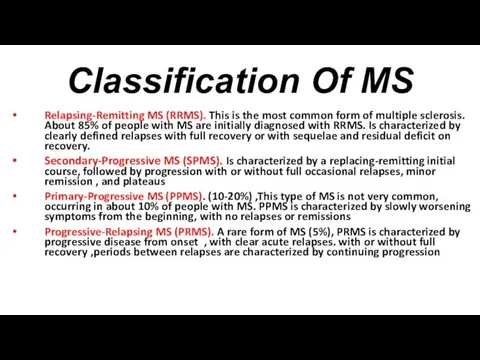
- 11. Classification Of MS Relapsing-Remitting MS (RRMS). This is the most common form of multiple sclerosis. About
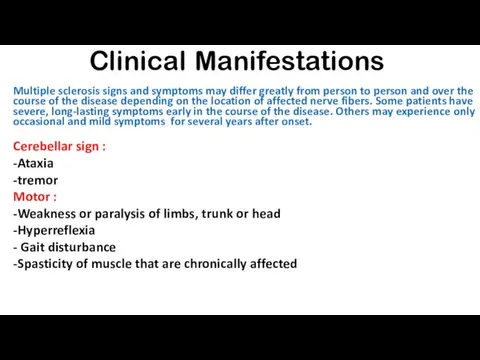
- 13. Clinical Manifestations Multiple sclerosis signs and symptoms may differ greatly from person to person and over
- 14. Sensory -Numbness, tingling and other parasthesias -Radicular (nerve root) pain in lower thoracic abdominal region. -Lhermitte'
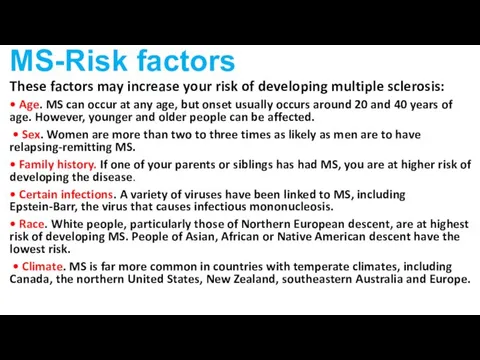
- 15. MS-Risk factors These factors may increase your risk of developing multiple sclerosis: • Age. MS can
- 16. • Vitamin D. Having low levels of vitamin D and low exposure to sunlight is associated
- 17. MS-Diagnosis Because there is no definitive diagnostic test for MS, diagnosis is based primarily on history
- 18. MS-Complications Epilepsy Mental changes such as forgetfulness or mood swing Problem with bladder, bowel or sexual
- 19. MS- Management Drug therapy : the treatment falls in 3 categories Treatment of acute relapse :
- 20. 2. Treat exacerbation: Interferon-Beta 1b Betaseron:, given subcutaneously Interferon Beta 1a : Avonex Glatiramer acetate :
- 21. Surgical therapy : Thalamotomy (unmanageable tremor ) Neurectomy , rhizotomy, Occupational therapy : Can help people
- 22. Nutritional therapy : Various nutritional measures that have been advocated in the management of MS include
- 23. Nursing management • Observe motor strength, coordination, and gait • Perform cranial nerve assessment Evaluate elimination
- 24. Patient Teaching Review the disease process, emphasizing the need for optimizing the patient's potential and avoiding
- 25. Nursing Diagnosis 1. Impaired physical mobility related to muscle weakness or paralysis and muscle spasticity as
- 26. summary
- 27. Reference Medical-surgical nursing assessment and management of clinical problem :( LWEIS , Dirksen, Heitkemper ) https://mymsaa.org/
- 29. Скачать презентацию
Topic outlines
Incidence
Definition of MS
Etiology
pathophysiology
Classification of MS
Clinical manifestation
Risk factors
Diagnosis
Complications
Medical
Topic outlines
Incidence
Definition of MS
Etiology
pathophysiology
Classification of MS
Clinical manifestation
Risk factors
Diagnosis
Complications
Medical
-MS was first describe in 1868 Jean-Martin Charcot.
-The name multiple sclerosis
-MS was first describe in 1868 Jean-Martin Charcot.
-The name multiple sclerosis
Incidence
2.5 million people are affected with MS worldwide .
High prevalence
Incidence
2.5 million people are affected with MS worldwide .
High prevalence
Definition
-MS : Is a chronic , progressive , degenerative disorder
Definition
-MS : Is a chronic , progressive , degenerative disorder
MS-Etiology
The cause of MS unknown although research findings suggest that
MS-Etiology
The cause of MS unknown although research findings suggest that
MS-Pathophysiology
* T-cells gain entry into the brain via disruption in
MS-Pathophysiology
* T-cells gain entry into the brain via disruption in
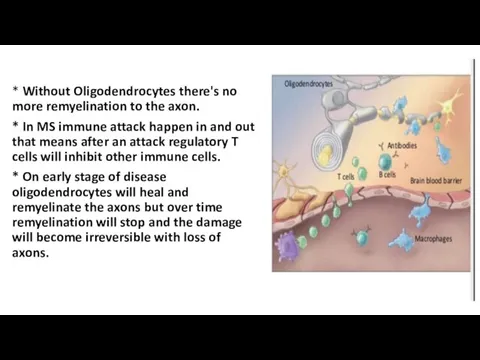
* Without Oligodendrocytes there's no more remyelination to the axon.
* In
* Without Oligodendrocytes there's no more remyelination to the axon.
* In
Classification Of MS
Relapsing-Remitting MS (RRMS). This is the most common form
Classification Of MS
Relapsing-Remitting MS (RRMS). This is the most common form

Clinical Manifestations
Multiple sclerosis signs and symptoms may differ greatly from
Clinical Manifestations
Multiple sclerosis signs and symptoms may differ greatly from

Sensory
-Numbness, tingling and other parasthesias
-Radicular (nerve root) pain in
Sensory
-Numbness, tingling and other parasthesias
-Radicular (nerve root) pain in
MS-Risk factors
These factors may increase your risk of developing multiple
MS-Risk factors
These factors may increase your risk of developing multiple
• Vitamin D. Having low levels of vitamin D and
• Vitamin D. Having low levels of vitamin D and
MS-Diagnosis
Because there is no definitive diagnostic test for MS, diagnosis
MS-Diagnosis
Because there is no definitive diagnostic test for MS, diagnosis
MS-Complications
Epilepsy
Mental changes such as forgetfulness or mood swing
Problem
MS-Complications
Epilepsy
Mental changes such as forgetfulness or mood swing
Problem
MS- Management
Drug therapy : the treatment falls in 3 categories
MS- Management
Drug therapy : the treatment falls in 3 categories
2. Treat exacerbation:
Interferon-Beta 1b
Betaseron:, given subcutaneously
Interferon Beta 1a :
2. Treat exacerbation:
Interferon-Beta 1b
Betaseron:, given subcutaneously
Interferon Beta 1a :
Surgical therapy :
Thalamotomy (unmanageable tremor )
Neurectomy , rhizotomy,
Occupational therapy :
Can
Surgical therapy :
Thalamotomy (unmanageable tremor )
Neurectomy , rhizotomy,
Occupational therapy :
Can
Nutritional therapy :
Various nutritional measures that have been advocated in
Nutritional therapy :
Various nutritional measures that have been advocated in
Nursing management
• Observe motor strength, coordination, and gait
•
Nursing management
• Observe motor strength, coordination, and gait
•
Patient Teaching
Review the disease process, emphasizing the need for optimizing
Patient Teaching
Review the disease process, emphasizing the need for optimizing
Nursing Diagnosis
1. Impaired physical mobility related to muscle weakness or
Nursing Diagnosis
1. Impaired physical mobility related to muscle weakness or
summary
summary
Reference
Medical-surgical nursing assessment and management of clinical problem :( LWEIS
Reference
Medical-surgical nursing assessment and management of clinical problem :( LWEIS
 Гомеопатия и ноотропные препараты от головокружения
Гомеопатия и ноотропные препараты от головокружения Балалардың тыныс алу жүйесінің ауруларын емдеу, денсаулығын нығайту алдын алу
Балалардың тыныс алу жүйесінің ауруларын емдеу, денсаулығын нығайту алдын алу Специфическая иммунопрофилактика. Основы дезинфекционного дела. Внутрибольничные инфекции
Специфическая иммунопрофилактика. Основы дезинфекционного дела. Внутрибольничные инфекции Использование тестов и функциональных проб для оценки состояния сердечнососудистой и дыхательной систем
Использование тестов и функциональных проб для оценки состояния сердечнососудистой и дыхательной систем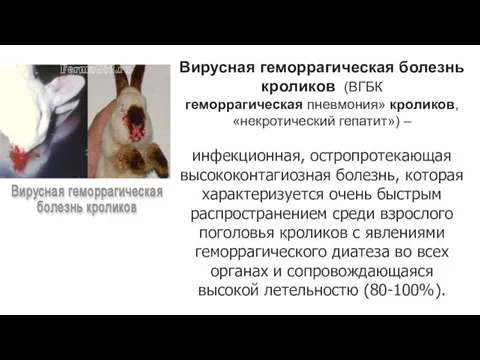 Вирусная геморрагическая болезнь кроликов
Вирусная геморрагическая болезнь кроликов Түбірлік периодонтиттің этиологиясы және патогенезі. Патологиялық анатомиясы. Периодонтиттің жіктелуі. Клиникасы,диагностикасы
Түбірлік периодонтиттің этиологиясы және патогенезі. Патологиялық анатомиясы. Периодонтиттің жіктелуі. Клиникасы,диагностикасы Наркотические (опиоидные) анальгетики
Наркотические (опиоидные) анальгетики Показание и противопоказание к операции при расщелинах нёба (уранопластика). Ребилитация и диспанцериазия
Показание и противопоказание к операции при расщелинах нёба (уранопластика). Ребилитация и диспанцериазия Первая доврачебная помощь при острой сердечной недостаточности и инсульте. 11 класс
Первая доврачебная помощь при острой сердечной недостаточности и инсульте. 11 класс Патронаж здорового новорожденного на дому с оформлением учебной амбулаторной карты
Патронаж здорового новорожденного на дому с оформлением учебной амбулаторной карты Повреждения груди и органов грудной полости
Повреждения груди и органов грудной полости Эпидемиологические исследования
Эпидемиологические исследования Нарушения внимания при локальных поражениях мозга
Нарушения внимания при локальных поражениях мозга Туберкулез бронхов
Туберкулез бронхов Исследование больных с заболеваниями сердца и сосудов
Исследование больных с заболеваниями сердца и сосудов Основы хирургии пороков развития
Основы хирургии пороков развития Ситуационные задачи. Болезни носа и околоносовых пазух
Ситуационные задачи. Болезни носа и околоносовых пазух Физиология мышечной ткани и нервно-мышечные рефлексы. Постизометрическая релаксация (ПИР)
Физиология мышечной ткани и нервно-мышечные рефлексы. Постизометрическая релаксация (ПИР) Рак легкого. Онкология
Рак легкого. Онкология Врачебный контроль за женщинами, занимающимися физкультурой и спортом
Врачебный контроль за женщинами, занимающимися физкультурой и спортом The history of the discovery of antibiotics
The history of the discovery of antibiotics Медицинская защита населения и спасателей в ЧС
Медицинская защита населения и спасателей в ЧС Лечение аллергии в санаториях Армении
Лечение аллергии в санаториях Армении prezentatsiya_sibirskaya_yazva
prezentatsiya_sibirskaya_yazva Слайд-лекция №16. Противоаритмические средства
Слайд-лекция №16. Противоаритмические средства Antimicrobial drugs
Antimicrobial drugs Тірі адамға сараптама жасау
Тірі адамға сараптама жасау Печінкові та ниркові коліки
Печінкові та ниркові коліки