- Antimicrobial drugs

Содержание
- 2. Antimicrobial drugs have antimicrobial properties. They are divided into 2 groups: Disinfectants and Antiseptics (drugs are
- 4. Disinfectants and Antiseptics Disinfection denotes the inactivation or killing of pathogens (protozoa, bacteria, fungi, viruses) in
- 5. Phenol was the first antiseptics. Phenol coefficient (the ratio between the concentration of phenol and the
- 6. Antisepsis refers to the reduction by chemical agents of germ numbers on skin and mucosal surfaces.
- 7. Disinfectants come from various chemical classes, including oxidants, halogens or halogen-releasing agents, alcohols, aldehydes, organic acids,
- 8. Applications Skin “disinfection.” (Reduction of germs before injections or surgical procedures). Useful agents include: alcohols (ethanol)
- 10. Wound disinfection can be achieved with hydrogen peroxide or with potassium permanganate, as well as PVP
- 12. Disinfection of instruments: Instruments that cannot be heat- or steam sterilized can be precleaned and then
- 13. Chemotherapeutic drugs inhibit/kill the infecting organism and have no/minimal effect on the recipient. They can be
- 14. Basic principles of chemotherapy Early start of treatment. Determination of the causative agent, its sensitivity to
- 15. SULFONAMIDES Sulfonamides were the first antimicrobial agents (AMAs) effective against pyogenic bacterial infections. All sulfonamides are
- 17. Sulfonamides are primarily bacteriostatic against many gram-positive and gram-negative bacteria. However, bactericidal concentrations may be attained
- 18. 1. Preparations used for their systemic action: Short acting (4–8 hr): Sulfadiazine, sulfadimidine Intermediate acting (8–12
- 19. The mechanism is connected with their competitive antagonism with para-aminobenzoic acid (PABA). Sulfonamides block dihydropteroate synthetase
- 20. Sulfonamides are rapidly and nearly completely absorbed from G.I.T. Extent of plasma protein binding differs considerably
- 21. Sulfonamides are excreted mainly by the kidney through glomerular filtration. Both renal tubular secretion and reabsorption
- 22. Side effects: Nausea, vomiting and epigastric pain. Crystalluria . Precipitation in urine can be minimized by
- 23. USES: suppressive therapy of chronic urinary tract infection; ear, throat, nose infections; gum infection; malaria and
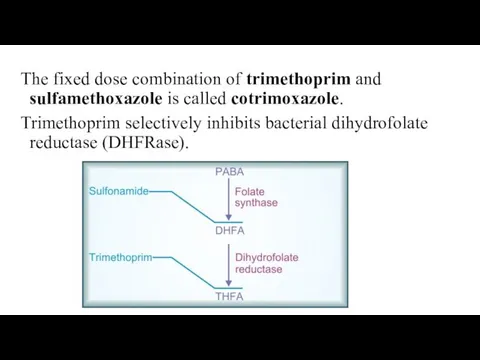
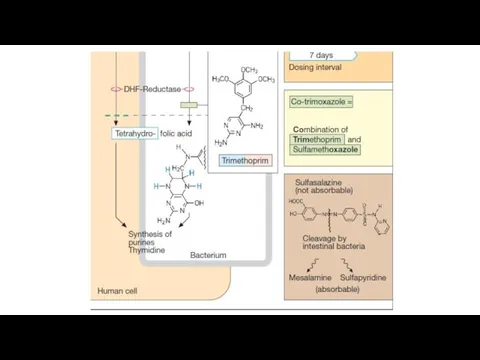
- 24. The fixed dose combination of trimethoprim and sulfamethoxazole is called cotrimoxazole. Trimethoprim selectively inhibits bacterial dihydrofolate
- 26. Individually, both sulfonamide and trimethoprim are bacteriostatic, but the combination becomes bacteriocidal against many organisms. Spectrum
- 27. Uses Urinary tract infections (acute cystitis, prostatitis); Respiratory tract infection caused by gram positive cocci and
- 28. Side effects of cotrimoxazole Nausea, vomiting, stomatitis, headache and Folate deficiency (megaloblastic anaemia). Cotrimoxazole should not
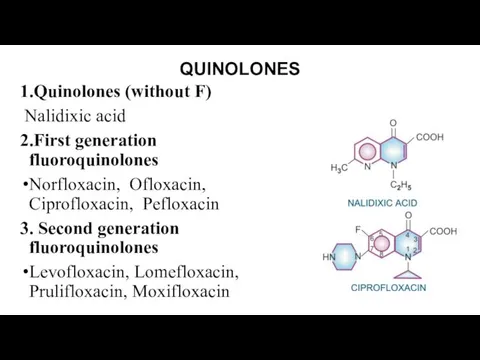
- 29. QUINOLONES 1.Quinolones (without F) Nalidixic acid 2.First generation fluoroquinolones Norfloxacin, Ofloxacin, Ciprofloxacin, Pefloxacin 3. Second generation
- 31. Nalidixic acid It is active against gram-negative bacteria ( E. coli, Proteus, Klebsiella, Enterobacter, Shigella but
- 32. Nalidixic acid is primarily used as a urinary antiseptic. It has also been employed in diarrhoea
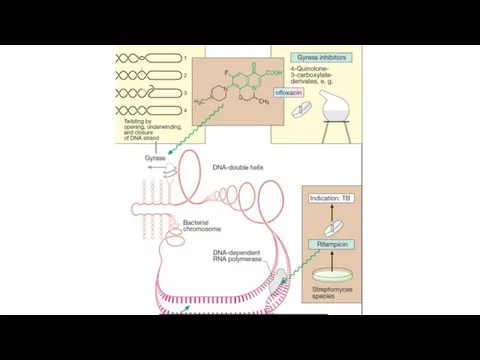
- 33. FLUOROQUINOLONES These preparations exhibit a bactericidal effect. Mechanism of action is associated with the inhibition of
- 34. The spectrum of action of First generation fluoroquinolones Highly susceptible: Neisseria gonorrhoeae; N. meningitidis; E. coli;
- 35. The spectrum of action of 2 generation fluoroquinolones They are more active against gram-positive bacteria. They
- 36. Pharmacokinetics: Drugs are absorbed from the gastrointestinal tract at 60-100%, They bind to proteins of blood.
- 37. Uses Urinary tract infections; Gonorrhoea; Chancroid; Bacterial gastroenteritis: dysentery, salmonellosis, cholera; Typhoid; Bone (osteomyelitis, joint infections),
- 38. Respiratory infections (2nd generation FQs is better); Tuberculosis; Septicaemias; Conjunctivitis; Meningitis
- 40. Side effects Dyspeptic disorders (nausea, vomiting, anorexia, diarrhea); Allergic reactions (rash, itching), photosensitization; Dizziness, headache, insomnia,
- 41. Derivative of 8-hydroxyquinoline – Nitroxoline Mechanism: reducing the activity of enzymes due to the formation of
- 42. Pharmacokinetics. Nitroxoline is administered orally 4 times a day. It is well absorbed from the digestive
- 43. Nitrofuran derivatives Nitrofural : antiseptic Furazolidon: intestinal infections, giardiasis, Trichomonas colpitis Nifuroxazide: intestinal infections. Nitrofurantoin (Furadonin),
- 44. Mechanism: The restoration of the nitro group to the amino group under the influence of reductase
- 45. Pharmacokinetics They are absorbed from the digestive tract at 30 (furazolidon) – 50 %. They penetrate
- 46. Side effects Dyspeptic disorders: nausea, vomiting, diarrhea; Cholestasis; disorders of liver function; Allergic reaction; Headache, dizziness;
- 47. Nitroimidazoles Metronidazole, Tinidazole, Ornidazole Spectrum: Entamoeba histolytica, Trichomonas vaginalis, lamblia, Bact. fragilis, Fusobacterium, Clostridium perfringens, Cl.
- 49. Mechanism of action Metronidazole is selectively toxic to anaerobic and microaerophilic microorganisms. After entering the cell
- 50. They are almost completely absorbed from the small intestines; little unabsorbed drug reaches the colon. They
- 51. Indications for uses Amoebiasis Giardiasis Trichomonas vaginitis Anaerobic bacterial infections (after colorectal or pelvic surgery, appendicectomy,
- 52. Side effects Anorexia, nausea, metallic taste and abdominal cramps are the most common. Less frequent side
- 53. OXAZOLIDINONE - Linezolid It is active against Staphylococcus aureus, penicillin-resistant Streptococci, M. tuberculosis, Corynebacterium, Listeria, Clostridia
- 54. Linezolid inhibits bacterial protein synthesis by acting at an early step. Linezolid is rapidly and completely
- 55. Quinoxaline derivatives – quinoxidine and dioxidine Spectrum: Proteus, Pseudomonas aeruginosa, intestinal bacteria, cocci, Clostridium, bacteroids. Application:
- 57. Скачать презентацию
Antimicrobial drugs have antimicrobial properties. They are divided into 2 groups:
Antimicrobial drugs have antimicrobial properties. They are divided into 2 groups:
Disinfectants and Antiseptics
Disinfection denotes the inactivation or killing of pathogens (protozoa,
Disinfectants and Antiseptics
Disinfection denotes the inactivation or killing of pathogens (protozoa,
Phenol was the first antiseptics.
Phenol coefficient (the ratio between the
Phenol was the first antiseptics.
Phenol coefficient (the ratio between the
Antisepsis refers to the reduction by chemical agents of germ numbers
Antisepsis refers to the reduction by chemical agents of germ numbers
Disinfectants come from various chemical classes, including oxidants, halogens or halogen-releasing
Disinfectants come from various chemical classes, including oxidants, halogens or halogen-releasing
Applications
Skin “disinfection.” (Reduction of germs before injections or surgical procedures). Useful
Applications
Skin “disinfection.” (Reduction of germs before injections or surgical procedures). Useful
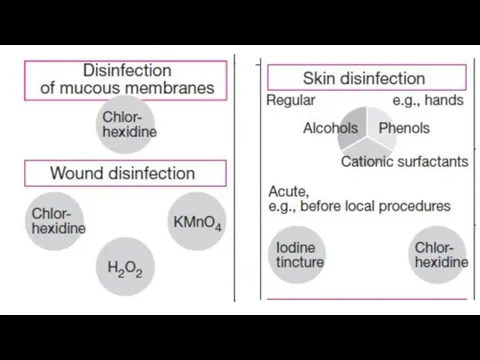
Wound disinfection can be achieved with hydrogen peroxide or with potassium
Wound disinfection can be achieved with hydrogen peroxide or with potassium
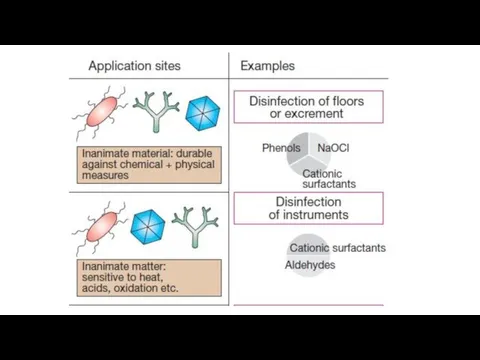
Disinfection of instruments: Instruments that cannot be heat- or steam sterilized
Disinfection of instruments: Instruments that cannot be heat- or steam sterilized
Chemotherapeutic drugs inhibit/kill the infecting organism and have no/minimal effect on
Chemotherapeutic drugs inhibit/kill the infecting organism and have no/minimal effect on
Basic principles of chemotherapy
Early start of treatment.
Determination of the causative agent,
Basic principles of chemotherapy
Early start of treatment.
Determination of the causative agent,
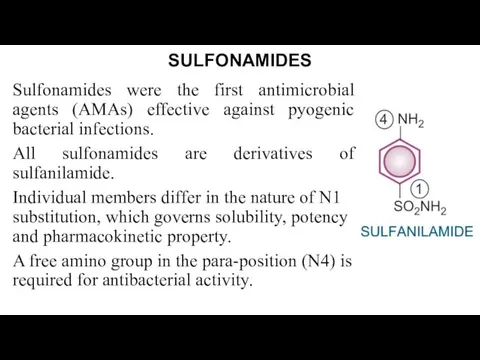
SULFONAMIDES
Sulfonamides were the first antimicrobial agents (AMAs) effective against pyogenic bacterial
SULFONAMIDES
Sulfonamides were the first antimicrobial agents (AMAs) effective against pyogenic bacterial
Sulfonamides are primarily bacteriostatic against many gram-positive and gram-negative bacteria. However,
Sulfonamides are primarily bacteriostatic against many gram-positive and gram-negative bacteria. However,
1. Preparations used for their systemic action:
Short acting (4–8 hr): Sulfadiazine,
1. Preparations used for their systemic action:
Short acting (4–8 hr): Sulfadiazine,
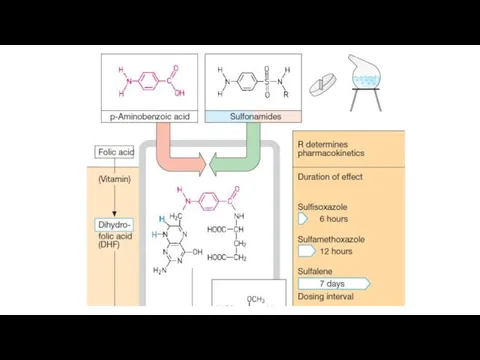
The mechanism is connected with their competitive antagonism with para-aminobenzoic acid
The mechanism is connected with their competitive antagonism with para-aminobenzoic acid
Sulfonamides are rapidly and nearly completely absorbed from G.I.T. Extent of
Sulfonamides are rapidly and nearly completely absorbed from G.I.T. Extent of
Sulfonamides are excreted mainly by the kidney through glomerular filtration. Both
Sulfonamides are excreted mainly by the kidney through glomerular filtration. Both
Side effects:
Nausea, vomiting and epigastric pain.
Crystalluria . Precipitation in
Side effects:
Nausea, vomiting and epigastric pain.
Crystalluria . Precipitation in
USES:
suppressive therapy of chronic urinary tract infection;
ear, throat, nose infections;
USES:
suppressive therapy of chronic urinary tract infection;
ear, throat, nose infections;
The fixed dose combination of trimethoprim and sulfamethoxazole is called cotrimoxazole.
Trimethoprim
The fixed dose combination of trimethoprim and sulfamethoxazole is called cotrimoxazole.
Trimethoprim
Individually, both sulfonamide and trimethoprim are bacteriostatic, but the combination becomes
Individually, both sulfonamide and trimethoprim are bacteriostatic, but the combination becomes
Uses
Urinary tract infections (acute cystitis, prostatitis);
Respiratory tract infection caused by
Uses
Urinary tract infections (acute cystitis, prostatitis);
Respiratory tract infection caused by
Side effects of cotrimoxazole
Nausea, vomiting, stomatitis, headache and
Folate deficiency (megaloblastic
Side effects of cotrimoxazole
Nausea, vomiting, stomatitis, headache and
Folate deficiency (megaloblastic
QUINOLONES
1.Quinolones (without F)
Nalidixic acid
2.First generation fluoroquinolones
Norfloxacin, Ofloxacin, Ciprofloxacin, Pefloxacin
3. Second
QUINOLONES
1.Quinolones (without F)
Nalidixic acid
2.First generation fluoroquinolones
Norfloxacin, Ofloxacin, Ciprofloxacin, Pefloxacin
3. Second
Nalidixic acid
It is active against gram-negative bacteria ( E. coli, Proteus,
Nalidixic acid
It is active against gram-negative bacteria ( E. coli, Proteus,
Nalidixic acid is primarily used as a urinary antiseptic. It has
Nalidixic acid is primarily used as a urinary antiseptic. It has
FLUOROQUINOLONES
These preparations exhibit a bactericidal effect. Mechanism of action is associated
FLUOROQUINOLONES
These preparations exhibit a bactericidal effect. Mechanism of action is associated
The spectrum of action of First generation fluoroquinolones
Highly susceptible: Neisseria gonorrhoeae;
The spectrum of action of First generation fluoroquinolones
Highly susceptible: Neisseria gonorrhoeae;
The spectrum of action of 2 generation fluoroquinolones
They are more active
The spectrum of action of 2 generation fluoroquinolones
They are more active
Pharmacokinetics:
Drugs are absorbed from the gastrointestinal tract at 60-100%,
They
Pharmacokinetics:
Drugs are absorbed from the gastrointestinal tract at 60-100%,
They
Uses
Urinary tract infections;
Gonorrhoea;
Chancroid;
Bacterial gastroenteritis: dysentery, salmonellosis, cholera;
Typhoid;
Bone (osteomyelitis, joint
Uses
Urinary tract infections;
Gonorrhoea;
Chancroid;
Bacterial gastroenteritis: dysentery, salmonellosis, cholera;
Typhoid;
Bone (osteomyelitis, joint
Respiratory infections (2nd generation FQs is better);
Tuberculosis;
Septicaemias;
Conjunctivitis;
Meningitis
Respiratory infections (2nd generation FQs is better);
Tuberculosis;
Septicaemias;
Conjunctivitis;
Meningitis

Side effects
Dyspeptic disorders (nausea, vomiting, anorexia, diarrhea);
Allergic reactions (rash, itching), photosensitization;
Dizziness,
Side effects
Dyspeptic disorders (nausea, vomiting, anorexia, diarrhea);
Allergic reactions (rash, itching), photosensitization;
Dizziness,
Derivative of 8-hydroxyquinoline – Nitroxoline
Mechanism: reducing the activity of enzymes due
Derivative of 8-hydroxyquinoline – Nitroxoline
Mechanism: reducing the activity of enzymes due
Pharmacokinetics.
Nitroxoline is administered orally 4 times a day.
It is
Pharmacokinetics.
Nitroxoline is administered orally 4 times a day.
It is
Nitrofuran derivatives
Nitrofural : antiseptic
Furazolidon: intestinal infections, giardiasis, Trichomonas colpitis
Nifuroxazide: intestinal infections.
Nitrofurantoin
Nitrofuran derivatives
Nitrofural : antiseptic
Furazolidon: intestinal infections, giardiasis, Trichomonas colpitis
Nifuroxazide: intestinal infections.
Nitrofurantoin
Mechanism:
The restoration of the nitro group to the amino group
Mechanism:
The restoration of the nitro group to the amino group
Pharmacokinetics
They are absorbed from the digestive tract at 30 (furazolidon)
Pharmacokinetics
They are absorbed from the digestive tract at 30 (furazolidon)
Side effects
Dyspeptic disorders: nausea, vomiting, diarrhea;
Cholestasis; disorders of liver function;
Allergic reaction;
Headache,
Side effects
Dyspeptic disorders: nausea, vomiting, diarrhea;
Cholestasis; disorders of liver function;
Allergic reaction;
Headache,
Nitroimidazoles
Metronidazole, Tinidazole, Ornidazole
Spectrum:
Entamoeba histolytica, Trichomonas vaginalis, lamblia,
Bact. fragilis,
Nitroimidazoles
Metronidazole, Tinidazole, Ornidazole
Spectrum:
Entamoeba histolytica, Trichomonas vaginalis, lamblia,
Bact. fragilis,
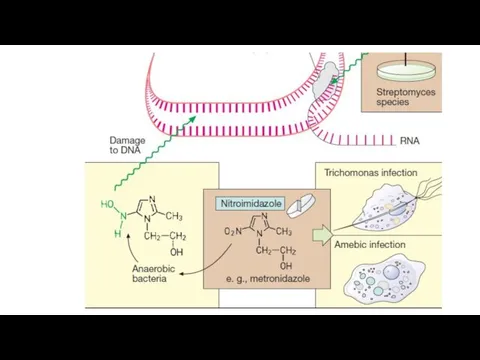
Mechanism of action
Metronidazole is selectively toxic to anaerobic and microaerophilic microorganisms.
Mechanism of action
Metronidazole is selectively toxic to anaerobic and microaerophilic microorganisms.
They are almost completely absorbed from the small intestines; little unabsorbed
They are almost completely absorbed from the small intestines; little unabsorbed
Indications for uses
Amoebiasis
Giardiasis
Trichomonas vaginitis
Anaerobic bacterial infections (after colorectal or pelvic surgery,
Indications for uses
Amoebiasis
Giardiasis
Trichomonas vaginitis
Anaerobic bacterial infections (after colorectal or pelvic surgery,
Side effects
Anorexia, nausea, metallic taste and abdominal cramps are the most
Side effects
Anorexia, nausea, metallic taste and abdominal cramps are the most
OXAZOLIDINONE - Linezolid
It is active against Staphylococcus aureus, penicillin-resistant Streptococci, M.
OXAZOLIDINONE - Linezolid
It is active against Staphylococcus aureus, penicillin-resistant Streptococci, M.
Linezolid inhibits bacterial protein synthesis by acting at an early step.
Linezolid
Linezolid inhibits bacterial protein synthesis by acting at an early step.
Linezolid
Quinoxaline derivatives – quinoxidine and dioxidine
Spectrum: Proteus, Pseudomonas aeruginosa, intestinal
Quinoxaline derivatives – quinoxidine and dioxidine
Spectrum: Proteus, Pseudomonas aeruginosa, intestinal
 Гастроэзофагальды рефлюкс ауруы, визуальды диагностикасы
Гастроэзофагальды рефлюкс ауруы, визуальды диагностикасы Циррозы печени
Циррозы печени Жыныстық зорлық-зомбылықты анықтау
Жыныстық зорлық-зомбылықты анықтау Поражения жкт при приеме НПВП
Поражения жкт при приеме НПВП Психиатриядағы және наркологиядағы сараптама түрлері
Психиатриядағы және наркологиядағы сараптама түрлері Общая характеристика трематод. Фасциолезы животных
Общая характеристика трематод. Фасциолезы животных Эмбриологияның даму тарихы
Эмбриологияның даму тарихы Imitation of biological processes. Medical simulations and analysis
Imitation of biological processes. Medical simulations and analysis Влияние стресса на организм человека
Влияние стресса на организм человека Оказание первой помощи
Оказание первой помощи Детский массаж до года. (Занятие 2)
Детский массаж до года. (Занятие 2) Digestive system
Digestive system Предмет и объект патопсихологии. Представления о клиническом методе
Предмет и объект патопсихологии. Представления о клиническом методе Жүректің жүрекше мен қарынша гипертрофиясының визуальды диагностикалау әдістері
Жүректің жүрекше мен қарынша гипертрофиясының визуальды диагностикалау әдістері Лечение язвенной болезни желудка и 12-перстной кишки
Лечение язвенной болезни желудка и 12-перстной кишки Иммунитет. Тканевая совместимость. Переливание крови
Иммунитет. Тканевая совместимость. Переливание крови Өкпе артериясының тромбоэмболиясы
Өкпе артериясының тромбоэмболиясы Применение УФ-излучения в медицинской практике
Применение УФ-излучения в медицинской практике Применение препарата Аспаркама во вторичной профилактике аритмий и осложнений у пациентов страдающих гипертонической болезнью
Применение препарата Аспаркама во вторичной профилактике аритмий и осложнений у пациентов страдающих гипертонической болезнью Адам организіміндегі қышқыл мен тұз. Организмнің қышқылдануы және тез қартаюы
Адам организіміндегі қышқыл мен тұз. Организмнің қышқылдануы және тез қартаюы Учение А.Р. Лурия о трех функциональных блоках мозга
Учение А.Р. Лурия о трех функциональных блоках мозга Инновационная экономика и технологическое предпринимательство
Инновационная экономика и технологическое предпринимательство Государственная служба Украины по лекарственным средствам. Установление критериев приемлемости. Аспекты валидации очистки
Государственная служба Украины по лекарственным средствам. Установление критериев приемлемости. Аспекты валидации очистки Амбулаторное отделение медицинской реабилитации. Дневной стационар медицинской реабилитации
Амбулаторное отделение медицинской реабилитации. Дневной стационар медицинской реабилитации Оказание медицинской помощи при кровотечениях
Оказание медицинской помощи при кровотечениях Остеоартроз. Фактори ризику
Остеоартроз. Фактори ризику Денсаулық сақтау жүйесі үлгілері: мемлекеттік,жеке меншіктік, медициналық сақтандыру
Денсаулық сақтау жүйесі үлгілері: мемлекеттік,жеке меншіктік, медициналық сақтандыру Лечение шизофрении
Лечение шизофрении