- Neuro-oncology

Содержание
- 2. Primary tumor brain spinal Secondary tumor brain spinal Paraneoplastic syndrome
- 3. Imaging for Brain Tumors Skull X-rays: Rarely necessary. Useful in demonstrating calcification, erosion, or hyperostosis CT:
- 4. MRI brain T1 vs T2
- 5. Epidemiology
- 8. Infratentorial vs Supratentorial Tumors
- 9. infratentorial
- 10. MENINGIOMA1,2,3 Epi: 2nd most common primary brain tumor after gliomas, incidence of ~ 6/100,000 Usual age
- 11. MENINGIOMA On Imaging CT: isodense or hypodense, homogenous extra-axial mass with smooth or lobulated, clearly demarcated
- 12. GLIOMAS Arise from Glial Cells Astrocytomas Astocytomas fall on a gradient that ranges from benign to
- 13. Diffuse Low Grade Astrocytoma Epi: 15% of Astrocytomas Young Adults Facts: Widely Infiltrate surrounding tissue Location:
- 14. High Grade glioma: Glioblastoma Epi: The 2-nd place of primary brain tumor in adults Age of
- 15. High Grade glioma: Glioblastoma On Imaging: Variable CT: Hypodense or Isodense Central hypodense area of necrosis
- 16. High Grade glioma: Glioblastoma Treatment: steroids surgical removal radiotherapy chemotherapy (temozolomide) anticonvulsive drugs
- 17. Survival
- 18. OLIGODENDROGLIOMA Epi: 5-10% of primary brain tumors Mean age of onset 40 years Facts: Distinguished pathologically
- 19. OLIGODENDROGLIOMA On Imaging: CT: Well circumscribed, hypodense lesions with heavy calcification Cystic degeneration is common but
- 20. OLIGODENDROGLIOMA Treatment: Surgical excision radiation therapy anticonvulsive drugs The median survival over 7 years.
- 21. INFRATENTORIAL TUMORS Choroid plexus papillomas Cerebellar astrocytomas Medulloblastomas Hemangioblastomas Ependymomas Brainstem gliomas Schwannomas Pituitary adenomas Craniopharyngiomas
- 22. CEREBELLAR ASTROCYTOMA Epi: Most often occurs in childhood Facts: Most potentially curable of the astrocytomas Location:
- 23. MEDULLOBLASTOMAS Epi Represent 7% of primary brain tumors 2nd most common posterior fossa tumor in children
- 24. MEDULLOBLASTOMAS Imaging MRI reveals a contrast-enhancing midline or paramedian tumor which often compresses the 4th ventricle;
- 25. EPENDYMOMAS Epi Accounts for 10% of CNS lesions; Male=Female Median age at diagnosis is 5 years
- 26. EPENDYMOMA Imaging Usually well demarcated with frequent areas of calcification, hemorrhage, and cysts; CT: Appear hyperdense
- 27. SCHWANNOMAS Epi Female>male Median age at diagnosis is 50 Account for 80-90% of cerebellopontine angle tumors
- 28. SCHWANNOMAS Imaging MRI: with gadolinium is more sensitive in detection of Schwannomas (when compared to CT);
- 29. Sella/suprasellar In this region it is important to keep the possibility of an aneurysm in the
- 30. PITUITARY ADENOMAS Epi Most common tumors of pituitary gland Represent 8% of primary brain tumors Facts
- 31. PITUITARY ADENOMAS Imaging: Plain x-ray may show an enlarged sella turcica; CT scan will detect only
- 32. BRAINSTEM GLIOMAS Epi Male=Female Account for 10-20% on all CNS tumors More common in children (account
- 33. BRAINSTEM GLIOMAS Imaging MRI is the method of choice to image those tumors (brainstem glioma appears
- 34. 4th ventricle In adults tumors in the 4th ventricle are uncommon. Metastases, followed by hemangioblastomas, choroid
- 35. Metastatic tumors Parenchymal meta – most common masses in the in supratentorial and infratentorial spaces (more
- 36. Hemorrhagic meta Breast Choriocarcinoma lung Melanoma RCC Thyroid retinoblastoma
- 37. Secondary tumors-MTS Lung cancer (NSCCa) Breast cancer Melanoma Kidney Thyroid
- 38. Carcinomatous Meningitis (Meningeal Carcinomatosis) Dissemination of tumor cells throughout the meninges and ventricles. 5 percent of
- 40. Скачать презентацию
Primary tumor
brain
spinal
Secondary tumor
brain
spinal
Paraneoplastic syndrome
Primary tumor
brain
spinal
Secondary tumor
brain
spinal
Paraneoplastic syndrome
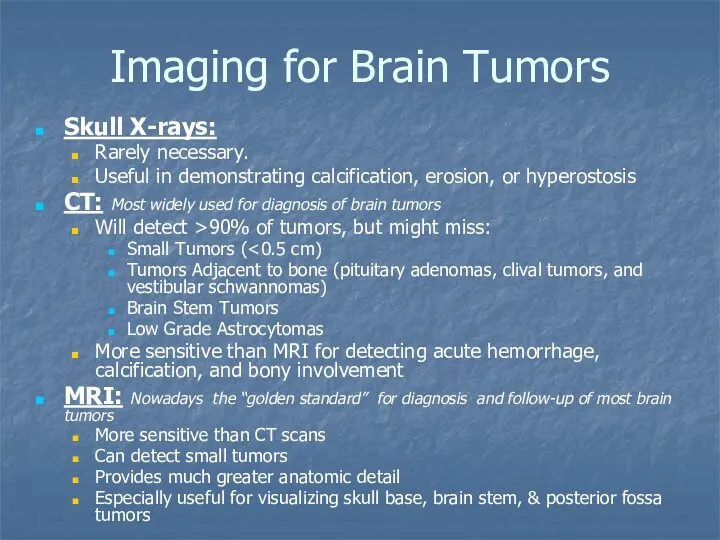
Imaging for Brain Tumors
Skull X-rays:
Rarely necessary.
Useful in demonstrating calcification,
Imaging for Brain Tumors
Skull X-rays:
Rarely necessary.
Useful in demonstrating calcification,
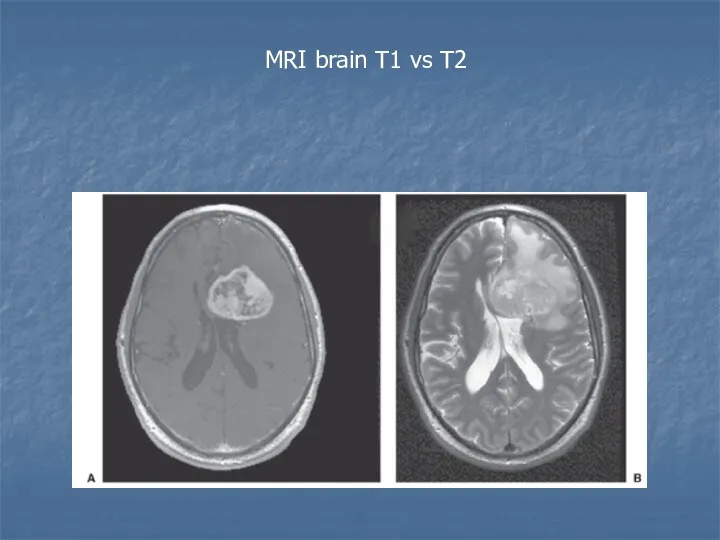
MRI brain T1 vs T2
MRI brain T1 vs T2
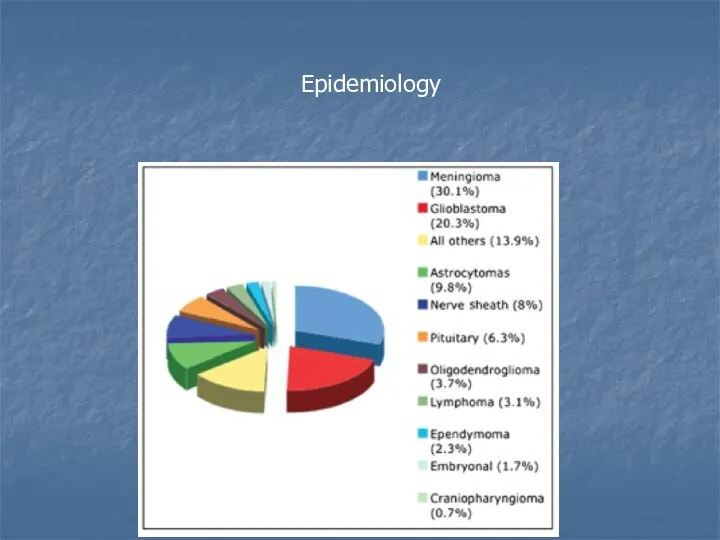
Epidemiology
Epidemiology

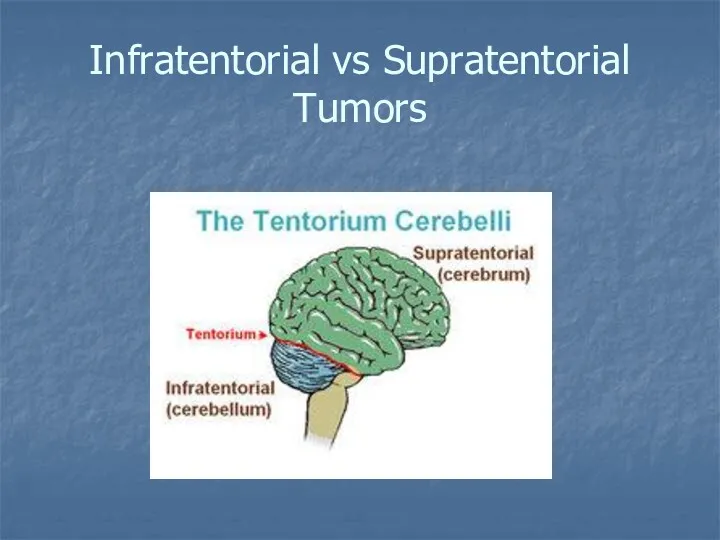
Infratentorial vs Supratentorial Tumors
Infratentorial vs Supratentorial Tumors
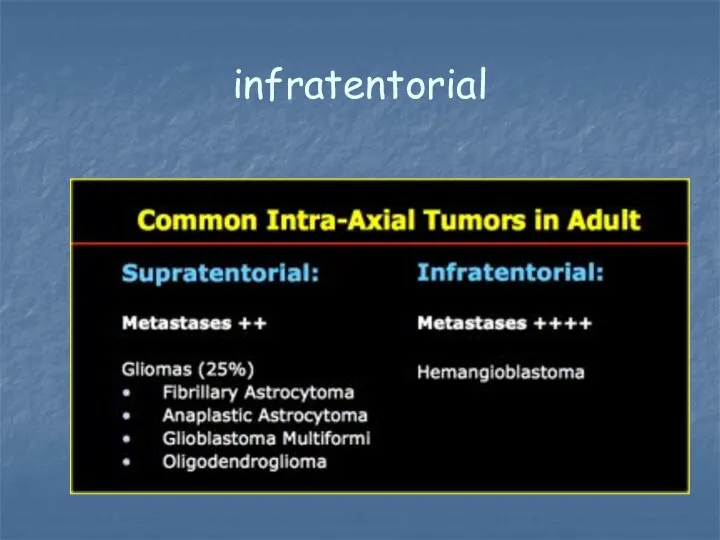
infratentorial
infratentorial
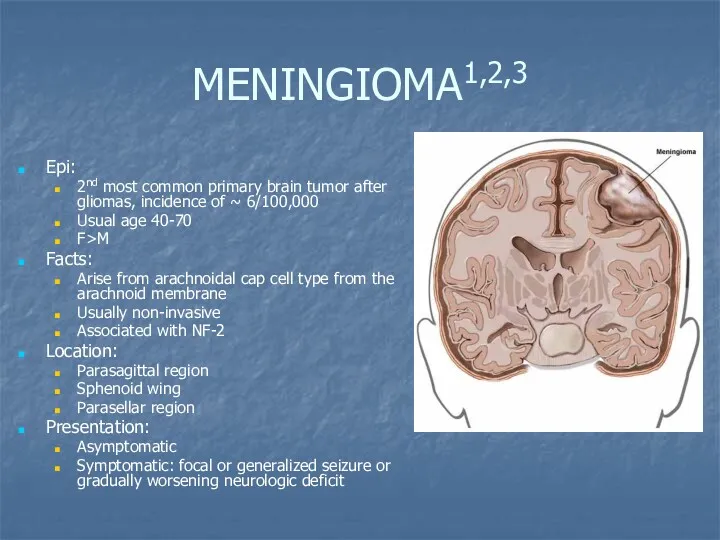
MENINGIOMA1,2,3
Epi:
2nd most common primary brain tumor after gliomas, incidence of
MENINGIOMA1,2,3
Epi:
2nd most common primary brain tumor after gliomas, incidence of
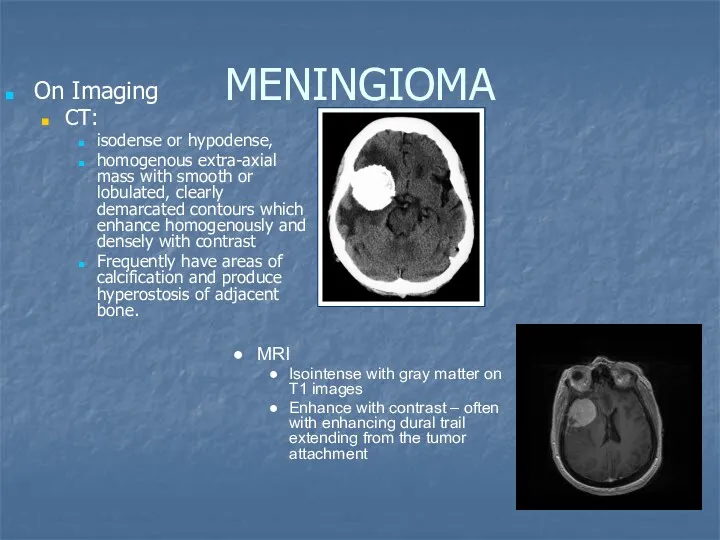
MENINGIOMA
On Imaging
CT:
isodense or hypodense,
homogenous extra-axial mass with smooth or
MENINGIOMA
On Imaging
CT:
isodense or hypodense,
homogenous extra-axial mass with smooth or
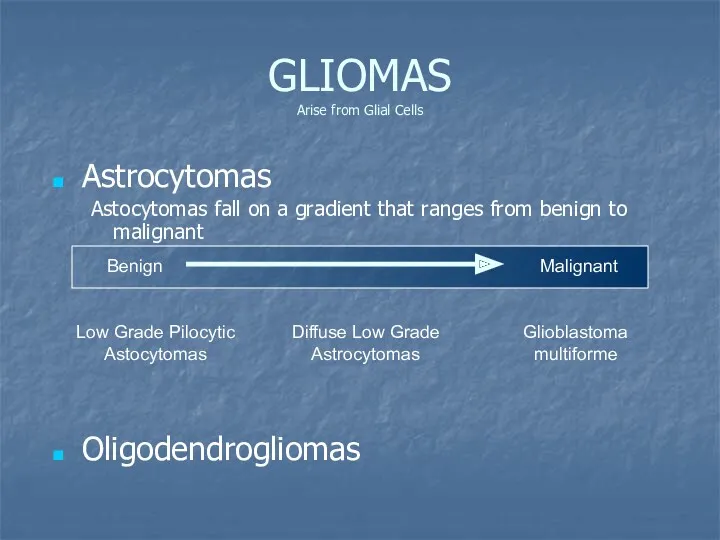
GLIOMAS
Arise from Glial Cells
Astrocytomas
Astocytomas fall on a gradient that ranges
GLIOMAS
Arise from Glial Cells
Astrocytomas
Astocytomas fall on a gradient that ranges
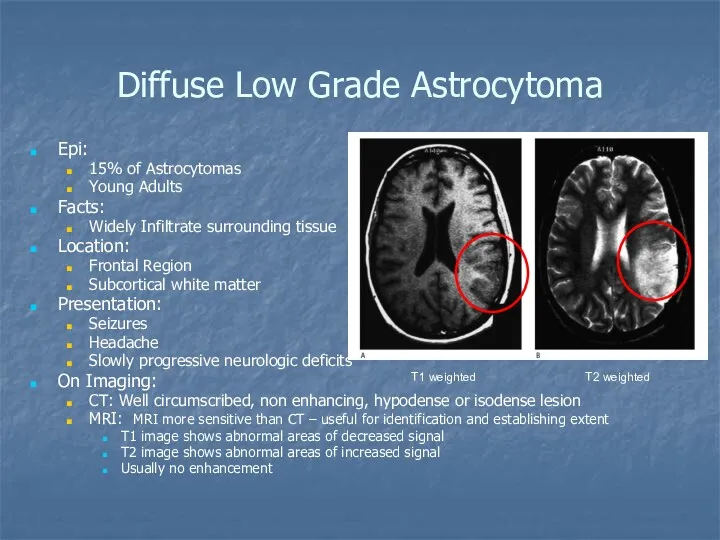
Diffuse Low Grade Astrocytoma
Epi:
15% of Astrocytomas
Young Adults
Facts:
Widely Infiltrate surrounding
Diffuse Low Grade Astrocytoma
Epi:
15% of Astrocytomas
Young Adults
Facts:
Widely Infiltrate surrounding
High Grade glioma: Glioblastoma
Epi:
The 2-nd place of primary brain tumor
High Grade glioma: Glioblastoma
Epi:
The 2-nd place of primary brain tumor
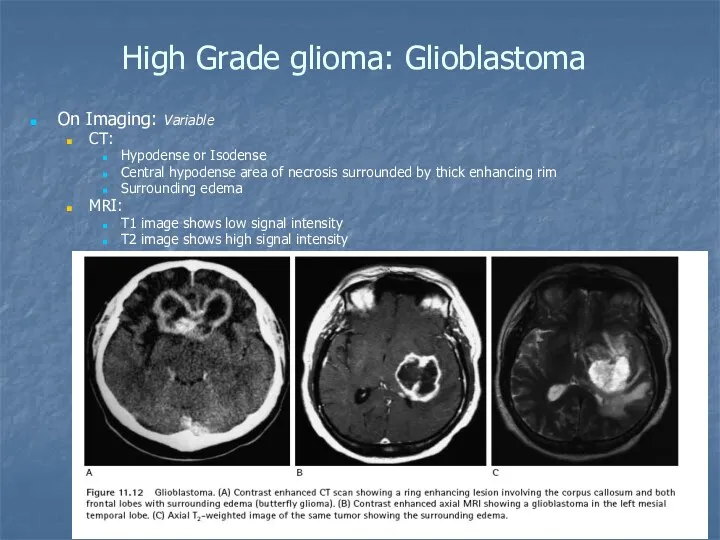
High Grade glioma: Glioblastoma
On Imaging: Variable
CT:
Hypodense or Isodense
Central hypodense
High Grade glioma: Glioblastoma
On Imaging: Variable
CT:
Hypodense or Isodense
Central hypodense
High Grade glioma: Glioblastoma
Treatment: steroids
surgical removal
radiotherapy
chemotherapy (temozolomide)
anticonvulsive
High Grade glioma: Glioblastoma
Treatment: steroids
surgical removal
radiotherapy
chemotherapy (temozolomide)
anticonvulsive
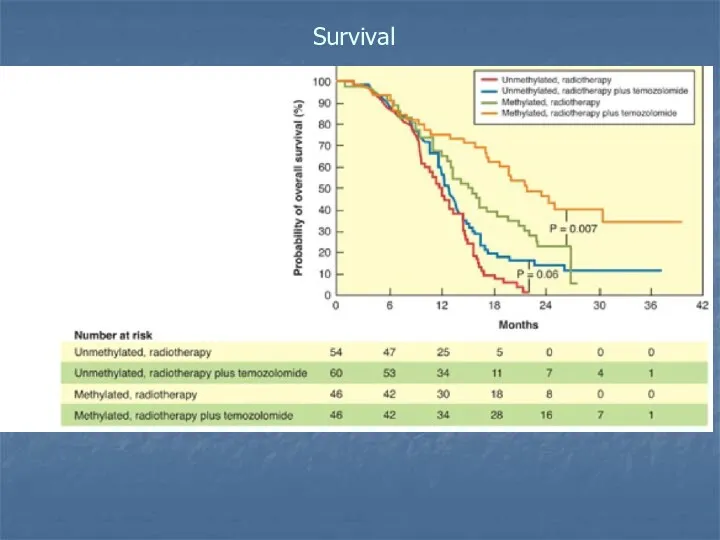
Survival
Survival
OLIGODENDROGLIOMA
Epi:
5-10% of primary brain tumors
Mean age of onset 40 years
Facts:
OLIGODENDROGLIOMA
Epi:
5-10% of primary brain tumors
Mean age of onset 40 years
Facts:
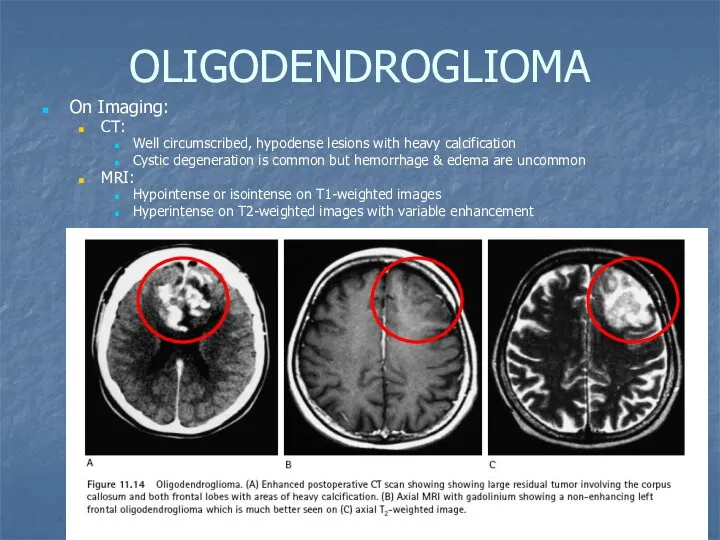
OLIGODENDROGLIOMA
On Imaging:
CT:
Well circumscribed, hypodense lesions with heavy calcification
Cystic degeneration
OLIGODENDROGLIOMA
On Imaging:
CT:
Well circumscribed, hypodense lesions with heavy calcification
Cystic degeneration
OLIGODENDROGLIOMA
Treatment:
Surgical excision
radiation therapy
anticonvulsive drugs
The
OLIGODENDROGLIOMA
Treatment:
Surgical excision
radiation therapy
anticonvulsive drugs
The
INFRATENTORIAL TUMORS
Choroid plexus papillomas
Cerebellar astrocytomas
Medulloblastomas
Hemangioblastomas
Ependymomas
Brainstem gliomas
Schwannomas
Pituitary adenomas
Craniopharyngiomas
INFRATENTORIAL TUMORS
Choroid plexus papillomas
Cerebellar astrocytomas
Medulloblastomas
Hemangioblastomas
Ependymomas
Brainstem gliomas
Schwannomas
Pituitary adenomas
Craniopharyngiomas
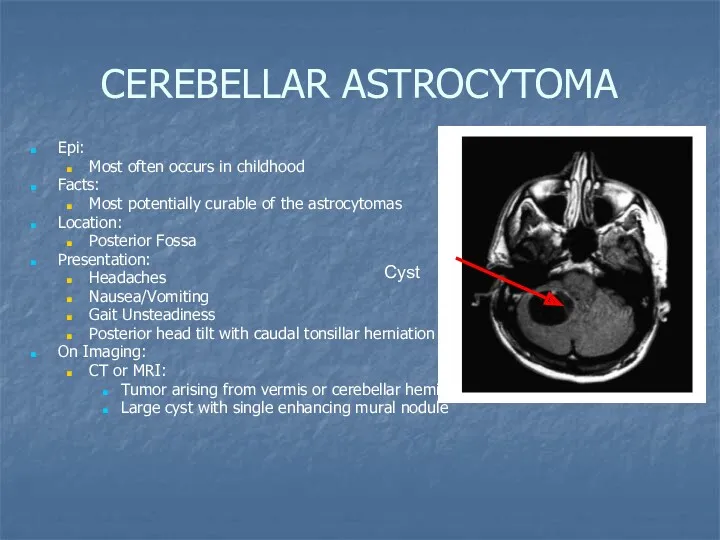
CEREBELLAR ASTROCYTOMA
Epi:
Most often occurs in childhood
Facts:
Most potentially curable of
CEREBELLAR ASTROCYTOMA
Epi:
Most often occurs in childhood
Facts:
Most potentially curable of
MEDULLOBLASTOMAS
Epi
Represent 7% of primary brain tumors
2nd most common posterior fossa tumor
MEDULLOBLASTOMAS
Epi
Represent 7% of primary brain tumors
2nd most common posterior fossa tumor
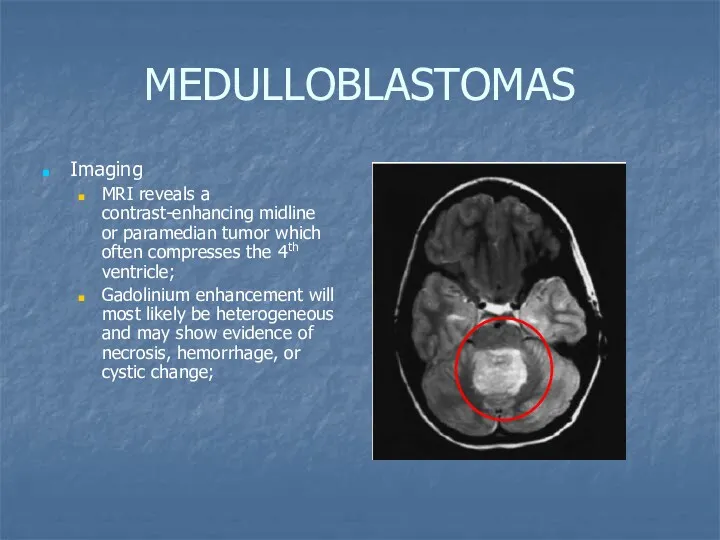
MEDULLOBLASTOMAS
Imaging
MRI reveals a contrast-enhancing midline or paramedian tumor which often compresses
MEDULLOBLASTOMAS
Imaging
MRI reveals a contrast-enhancing midline or paramedian tumor which often compresses
EPENDYMOMAS
Epi
Accounts for 10% of CNS lesions;
Male=Female
Median age at diagnosis is
EPENDYMOMAS
Epi
Accounts for 10% of CNS lesions;
Male=Female
Median age at diagnosis is
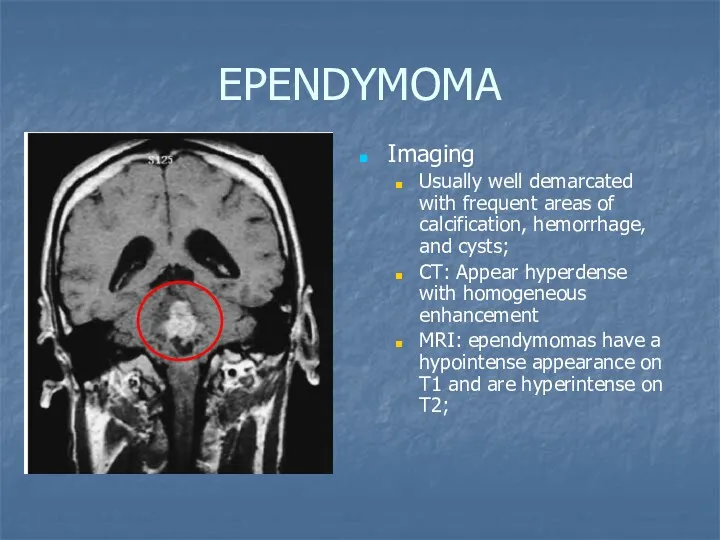
EPENDYMOMA
Imaging
Usually well demarcated with frequent areas of calcification, hemorrhage, and cysts;
CT:
EPENDYMOMA
Imaging
Usually well demarcated with frequent areas of calcification, hemorrhage, and cysts;
CT:
SCHWANNOMAS
Epi
Female>male
Median age at diagnosis is 50
Account for 80-90% of cerebellopontine angle
SCHWANNOMAS
Epi
Female>male
Median age at diagnosis is 50
Account for 80-90% of cerebellopontine angle
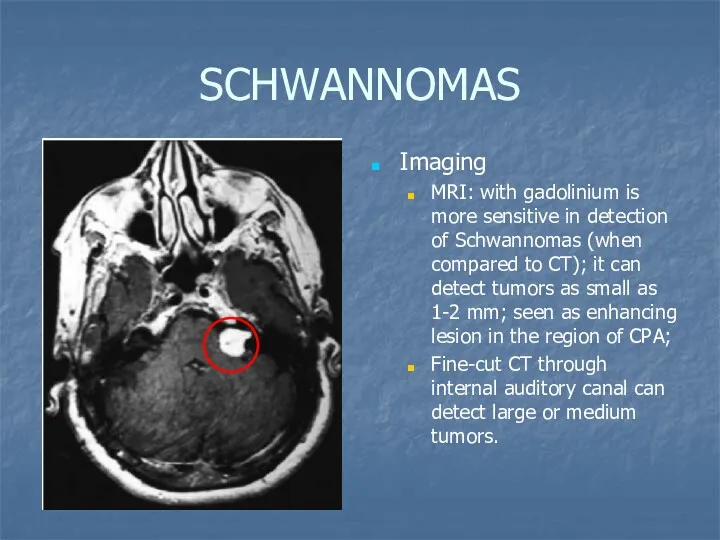
SCHWANNOMAS
Imaging
MRI: with gadolinium is more sensitive in detection of Schwannomas (when
SCHWANNOMAS
Imaging
MRI: with gadolinium is more sensitive in detection of Schwannomas (when
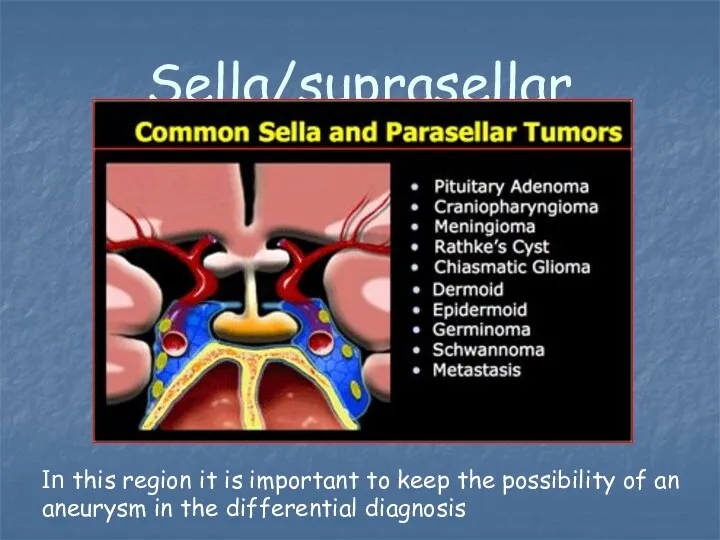
Sella/suprasellar
In this region it is important to keep the possibility of
Sella/suprasellar
In this region it is important to keep the possibility of
PITUITARY ADENOMAS
Epi
Most common tumors of pituitary gland
Represent 8% of primary brain
PITUITARY ADENOMAS
Epi
Most common tumors of pituitary gland
Represent 8% of primary brain
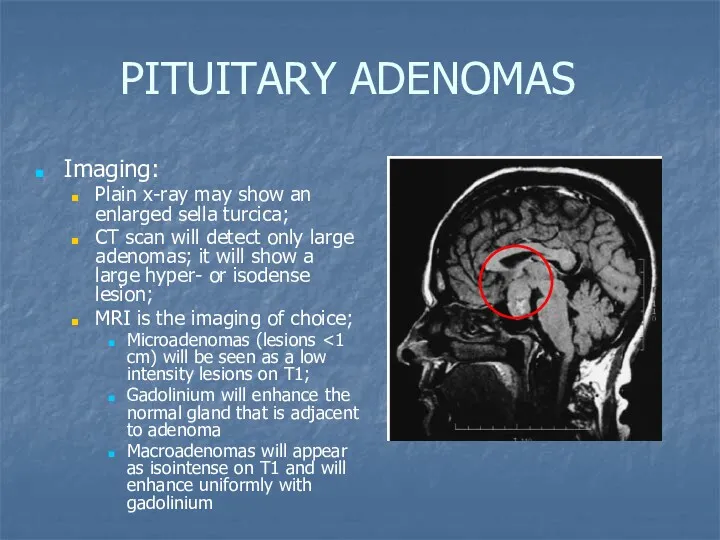
PITUITARY ADENOMAS
Imaging:
Plain x-ray may show an enlarged sella turcica;
CT scan
PITUITARY ADENOMAS
Imaging:
Plain x-ray may show an enlarged sella turcica;
CT scan
BRAINSTEM GLIOMAS
Epi
Male=Female
Account for 10-20% on all CNS tumors
More common in children
BRAINSTEM GLIOMAS
Epi
Male=Female
Account for 10-20% on all CNS tumors
More common in children
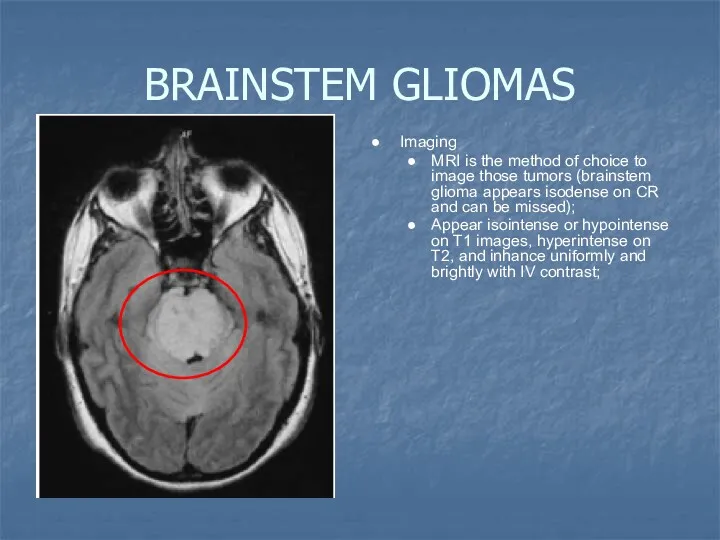
BRAINSTEM GLIOMAS
Imaging
MRI is the method of choice to image those tumors
BRAINSTEM GLIOMAS
Imaging
MRI is the method of choice to image those tumors
4th ventricle
In adults tumors in the 4th ventricle are uncommon.
Metastases,
4th ventricle
In adults tumors in the 4th ventricle are uncommon.
Metastases,
Metastatic tumors
Parenchymal meta – most common masses in the in supratentorial
Metastatic tumors
Parenchymal meta – most common masses in the in supratentorial
Hemorrhagic meta
Breast
Choriocarcinoma
lung
Melanoma
RCC
Thyroid
retinoblastoma
Hemorrhagic meta
Breast
Choriocarcinoma
lung
Melanoma
RCC
Thyroid
retinoblastoma
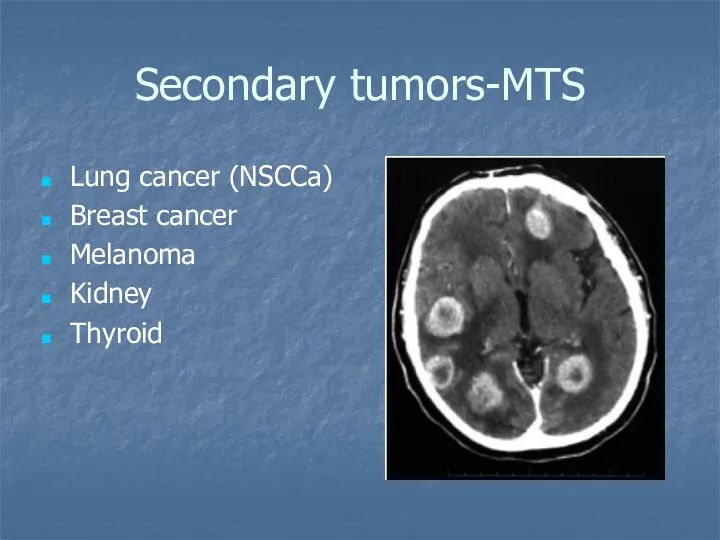
Secondary tumors-MTS
Lung cancer (NSCCa)
Breast cancer
Melanoma
Kidney
Thyroid
Secondary tumors-MTS
Lung cancer (NSCCa)
Breast cancer
Melanoma
Kidney
Thyroid
Carcinomatous Meningitis
(Meningeal Carcinomatosis)
Dissemination of tumor cells throughout the meninges
and ventricles.
5 percent
Carcinomatous Meningitis
(Meningeal Carcinomatosis)
Dissemination of tumor cells throughout the meninges
and ventricles.
5 percent
 Задача №6. Команда Морфий
Задача №6. Команда Морфий Corticosteroids. Steroids: the worst drugs for adverse effects
Corticosteroids. Steroids: the worst drugs for adverse effects Закупка лекарственных средств для нужд государственных и муниципальных организаций. Тема 1
Закупка лекарственных средств для нужд государственных и муниципальных организаций. Тема 1 Гигиена и антисептика рук в медицинском учреждении
Гигиена и антисептика рук в медицинском учреждении История развития отоларингологии
История развития отоларингологии Купероз и Anti-Aging
Купероз и Anti-Aging Акушерськиі операції. Класифікація. Принципи і методи знеболення
Акушерськиі операції. Класифікація. Принципи і методи знеболення Обсессивно-компульсивное расстройство (ОКР)
Обсессивно-компульсивное расстройство (ОКР) Туберкулез лимфатических узлов
Туберкулез лимфатических узлов Childhood Obesity
Childhood Obesity Содержимое аптечки, первичный комплекс сердечно-лёгочной реанимации (СЛР), первая помощь при неотложных состояниях
Содержимое аптечки, первичный комплекс сердечно-лёгочной реанимации (СЛР), первая помощь при неотложных состояниях Куріння та його вплив на організм людини
Куріння та його вплив на організм людини Буынның гипермобильдігі. Майтабан
Буынның гипермобильдігі. Майтабан Введение в доказательную медицину
Введение в доказательную медицину Домедична допомога в умовах бойових дій (тактична медицина). Тема №3.5
Домедична допомога в умовах бойових дій (тактична медицина). Тема №3.5 Wyposażenie torby R1-R2
Wyposażenie torby R1-R2 Жевательный аппарат. Анатомическое строение верхней и нижней челюстей. Височно-нижнечелюстной сустав. Пародонт
Жевательный аппарат. Анатомическое строение верхней и нижней челюстей. Височно-нижнечелюстной сустав. Пародонт Особенности паллиативной медицинской помощи
Особенности паллиативной медицинской помощи Обследование больных с патологией органов кровообращения
Обследование больных с патологией органов кровообращения Синдром Лайелла (токсический эпидермальный некролиз)
Синдром Лайелла (токсический эпидермальный некролиз) Понятие утомление и переутомление
Понятие утомление и переутомление Снотворные средства
Снотворные средства Рак тела матки
Рак тела матки Снотворные средства
Снотворные средства Тактика ведения ревматологических больных при беременности
Тактика ведения ревматологических больных при беременности Sistemul circulator limfatic organele hematopoietice
Sistemul circulator limfatic organele hematopoietice Коклюш
Коклюш Черный мор (чума)
Черный мор (чума)