- Parenteral Nutrition in Neonates

Содержание
- 2. Parenteral Nutrition in Neonates Prepared By Neveen Hassan Abdel Aal Clinical Pharmacist at NICU Assuit University
- 3. Parenteral Nutrition: Definition & Goals. Types of PN Admixtures. Routes of Administration of PN. Nutritional Components
- 4. Parenteral Nutrition PN is the administration of intravenous nutrition in patients with a Non- functioning or
- 5. Parenteral Nutrition Goals (1) Weight maintenance or promoting growth. (2) Preservation of lean body mass& visceral
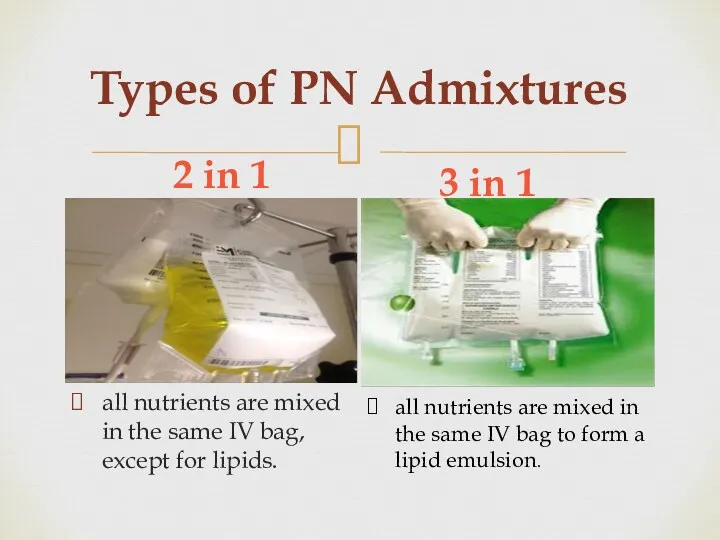
- 6. Types of PN Admixtures 2 in 1 3 in 1 all nutrients are mixed in the
- 7. Routes of Administration of PN
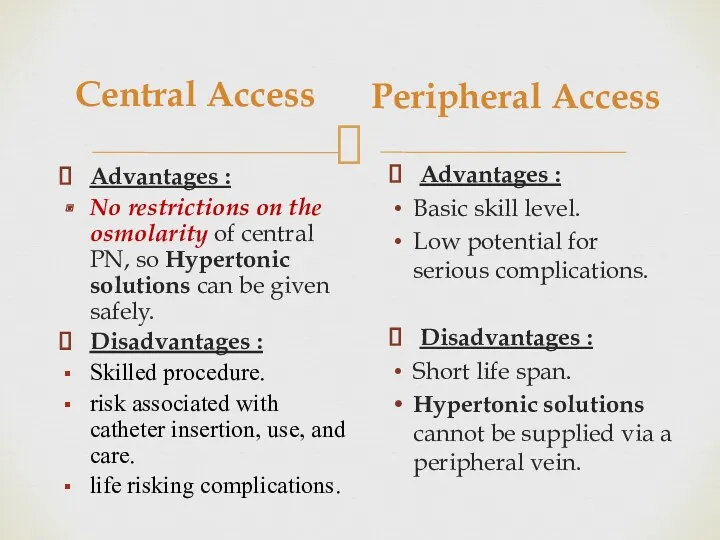
- 8. Central Access Advantages : No restrictions on the osmolarity of central PN, so Hypertonic solutions can
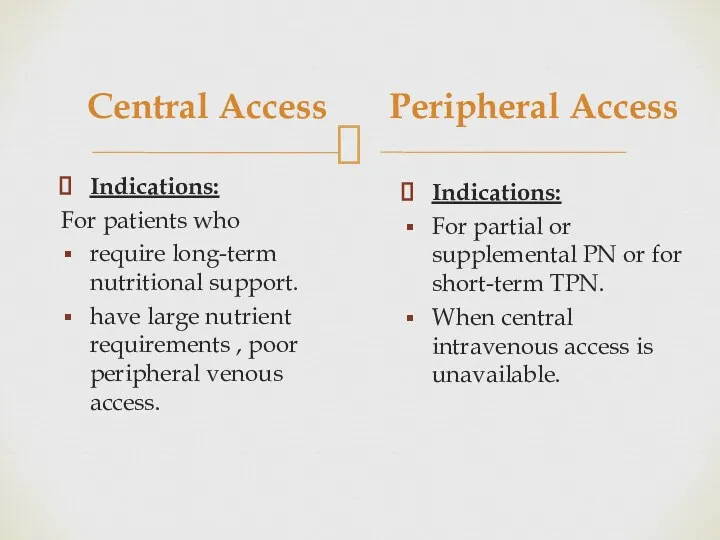
- 9. Central Access Indications: For patients who require long-term nutritional support. have large nutrient requirements , poor
- 10. Criteria for Peripheral Administration Osmolarity must not exceed 900 mOsm/L. Final dextrose concentration should be ˂10%
- 11. Nutritional Components of PN Formulation PN should provide a balanced nutritional intake of 1) Macronutrients including
- 12. Estimating the Osmolarity of Parenteral nutrients ● Peripheral TPN: ● Central TPN: 1500 - 2800 mOsm/L
- 13. Calculating the Osmolarity of a Parenteral Nutrition Solution Multiply the grams of dextrose per liter by
- 14. Developing a Regimen for PN Administration Through Central Line
- 15. I. Evaluation of patient case PN components should be adjusted individually to each patient according to:
- 16. I. Evaluation of patient case First of all Review: Patient Age, weight ( Kg). Make sure
- 17. Evaluation of patient case continue 4. Assessment of degree of hydration. Signs of dehydration: Reduced urine
- 18. II. Start Calculating Components of PN Formula Steps of Calculation Fluid need/tolerated (Subtract drugs, Blood, O.R.S,
- 19. 1.Determine Fluid Requirements
- 20. Daily maintenance of fluids intake on body weight basis AACN Advanced Critical Care Volume 23, Number
- 21. The Neonatal adaptation processes after birth may be divided into three major phases: Phase I: transition.
- 22. Recommended Parenteral fluid intake (ml/kg /day) During the first postnatal week During the intermediate phase prior
- 23. Variations in Fluid Requirements Do not use PN for fluid replacement but for maintenance fluid only.
- 24. Suggested initial adjustment in specific situations Fever…..+12% for each degree >37 c. High humidity…..0.7 × maintenance.
- 25. Adjustment of Fluid Requirements in case of Kidney Dysfunction TFR= I.W.L + U.O.P Insensible water loss
- 26. 2. Determine Caloric Requirements
- 27. Parenteral energy needs may be roughly estimated using the following ranges J Pediatr Gastroenterol Nutr, Vol.
- 28. Further aspects need to be taken into account according to clinical parameters: Weight gain in regard
- 29. Variations in Caloric Requirements Patient require increased caloric needs in case of fever, inflammation, sepsis, burn,
- 30. Factors that increase caloric requirements
- 31. The Caloric balance of PN Formula Caloric needs are met by a proper balance of carbohydrates,
- 32. 3.Determine Protein Requirements Proteins are the major structural and functional components of all cells in the
- 33. Protein requirements of neonates and children depend on age and weight J Pediatr Gastroenterol Nutr, Vol.
- 34. Regimen of Protein Administration Start with 1.5 gm/kg/d and then increase by 1 gm/kg/d to maximum
- 35. Protein requirements Variations Increased amount of amino acids are required in case of patients with short
- 36. Potential complications and risks of providing IV amino acids 1- Acidosis 2- Elevated BUN 3- Hyper-
- 37. Caloric Value of Proteins Calories from protein (4 kcal/g) Inadequate supplementation of energy from carbohydrates and
- 38. 4.Determine Lipid Requirements Providing fat is essential to Achieve adequate caloric intake in TPN Utilize amino
- 39. The lipid requirements of neonates and children depending on age J Pediatr Gastroenterol Nutr, Vol. 41,
- 40. Regimen of Lipid Administration Starting dose of 1 g/kg/day Titrate toward the goal as tolerated by
- 41. Caloric Value of Lipids Calories from Lipid (10 kcal/g) Maximum fat oxidation occurs when intravenous lipid
- 42. Precautions For Neonates Restrict the dose of lipids in minimum amounts that will provide only the
- 43. Potential complications and risks of providing IV Lipids Hyperlipidemia. Potential increased risk or exacerbation of chronic
- 44. Monitoring Plasma clearance of infused triglycerides can be assessed by measurement of plasma triglyceride concentrations. Checking
- 45. J Pediatr Gastroenterol Nutr, Vol. 41, Suppl. 2, November 2005
- 46. 5. Determine Carbohydrates Requirements Dextrose is major immediate energy source . Several body tissues depend mainly
- 47. Recommended parenteral glucose supply (g/kg/day) Estimation of carbohydrates requirements It is important, especially when prescribing PN
- 48. Carbohydrates Requirements need to be adapted according to Age and clinical situation (e.g. malnutrition, acute illness,
- 49. Regimen of Carbohydrate Administration For neonates: Begin with GIR 4-8 mg/kg/min in preterm 4-6 mg/kg/min in
- 50. Caloric Value of Dextrose Dextrose yields 3.4 kcal/ g Peripheral line: maximum dextrose concentration 12.5%. Central
- 51. Potential complications Hyperglycemia or hypoglycemia. Glycosuria and potential osmotic diuresis. Cholestasis and/or hepatic steatosis (usually from
- 52. Managing Hyperglycemia in Neonates If hyperglycemia develops: ↓GIR insulin may improve glucose tolerance . Do not
- 53. 6. Estimate a Daily Maintenance amount of Electrolytes Vitamins & Trace elements
- 54. A) Electrolytes Initial PN solutions may be started without added electrolytes. Add electrolytes gradually as the
- 55. Electrolytes Requirements If Magnesium Sulfate was administered prior to delivery then leave Mg out of PN
- 56. Recommended Parenteral electrolyte intake *Careful adjustment of water and electrolyte administration is needed in ELBW infants
- 57. Phosphate Normal Ranges by Age Normal values of Phosphate are age related as a result of
- 58. B) Trace Elements Standard trace elements contain selenium, chromium, copper , manganese , and zinc. Neonates
- 59. Trace Elements Requirements
- 60. Pediatrace® Dose: 1 ml/ kg/ day for Premature, Infant & Children with a weight
- 61. C) Vitamins Requirements Similar to trace elements, multivitamins are often standard in PN unless requested otherwise.
- 62. Medication Additives in PN Generally, medications should not be added to PN if it can be
- 63. PN Complications Short term Complications 1- Catheter-related infections 2- Catheter insertion complications 3-Peripheral Thrombophlebitis 4-Gut atrophy
- 64. Short term Complications Continue 7. Refeeding syndrome can occur in acutely or chronically malnourished patients by
- 65. Long term Complications 1-Hepatobiliary Disorders (includes steatosis, cholestasis, and gallbladder stones) 2-Osteoporosis & osteomalacia associated with
- 66. Monitoring PN Administration 1- Infection: Temperature ,WBC , IV access site 2- Peripheral vein thrombophlebitis (if
- 67. Monitoring Continue 5-Glycemic control(Hyperglycemia and hypoglycemia.) Goal : 150 mg/dl or less 6- Monitor for electrolyte
- 68. Monitoring Laboratory measurement
- 69. Transition to Oral or Enteral Nutrition When initiating enteral or oral nutrition , monitor for glucose,
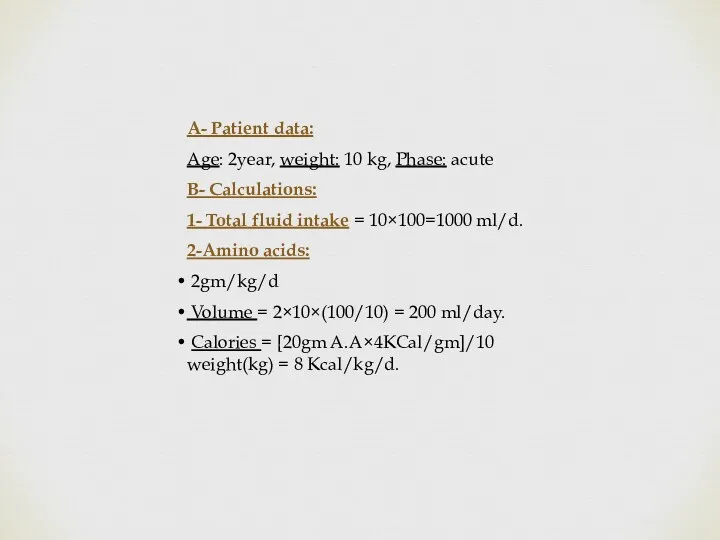
- 71. A- Patient data: Age: 2year, weight: 10 kg, Phase: acute B- Calculations: 1- Total fluid intake
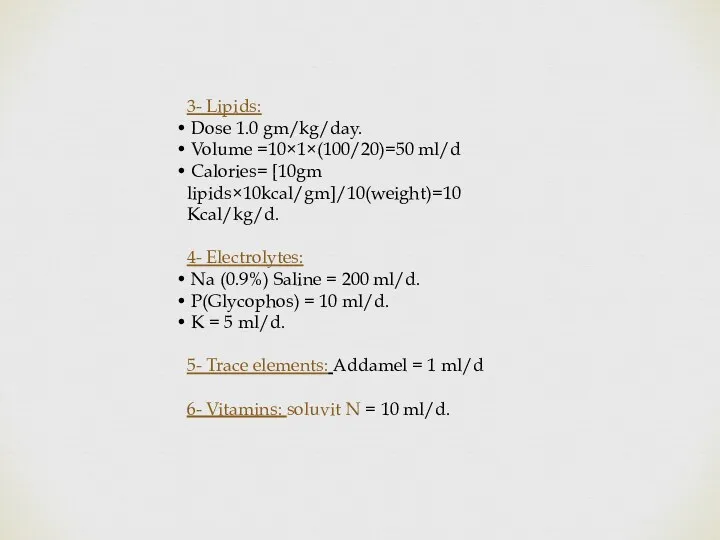
- 72. 3- Lipids: Dose 1.0 gm/kg/day. Volume =10×1×(100/20)=50 ml/d Calories= [10gm lipids×10kcal/gm]/10(weight)=10 Kcal/kg/d. 4- Electrolytes: Na (0.9%)
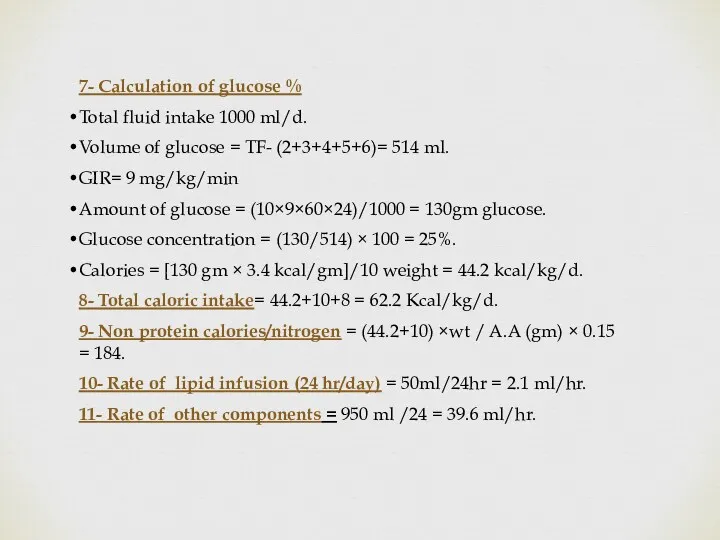
- 73. 7- Calculation of glucose % Total fluid intake 1000 ml/d. Volume of glucose = TF- (2+3+4+5+6)=
- 74. Preterm and Term Infants During the Transition Phase Sodium, chloride and potassium should be supplemented in
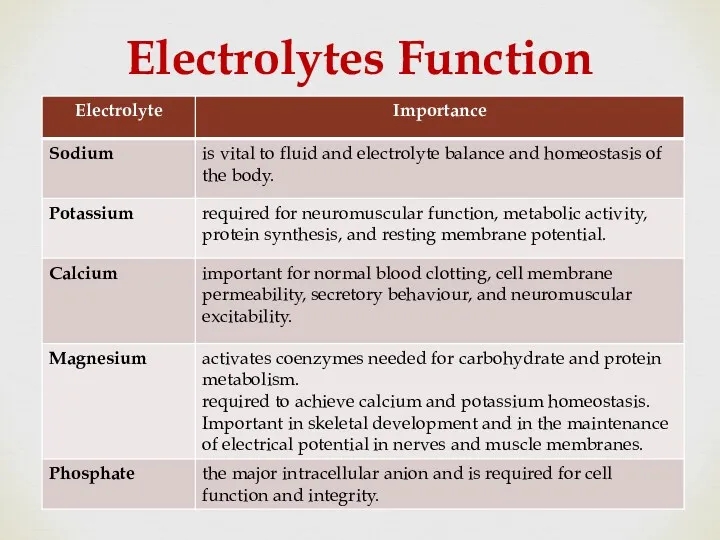
- 75. Electrolytes Function
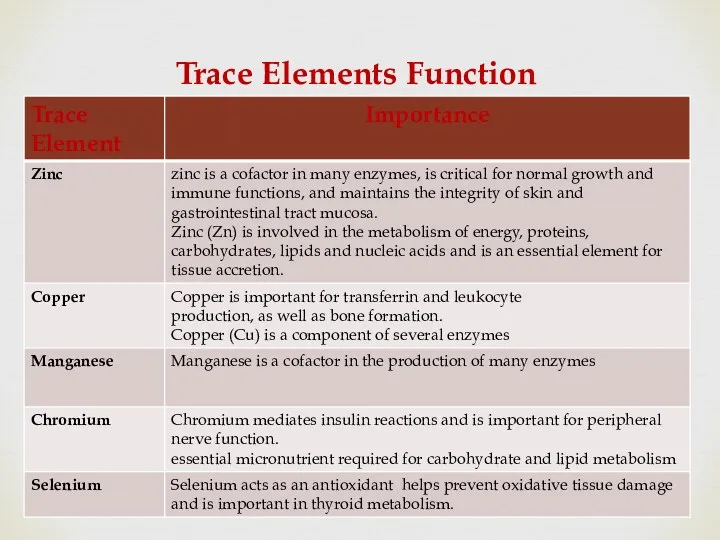
- 76. Trace Elements Function
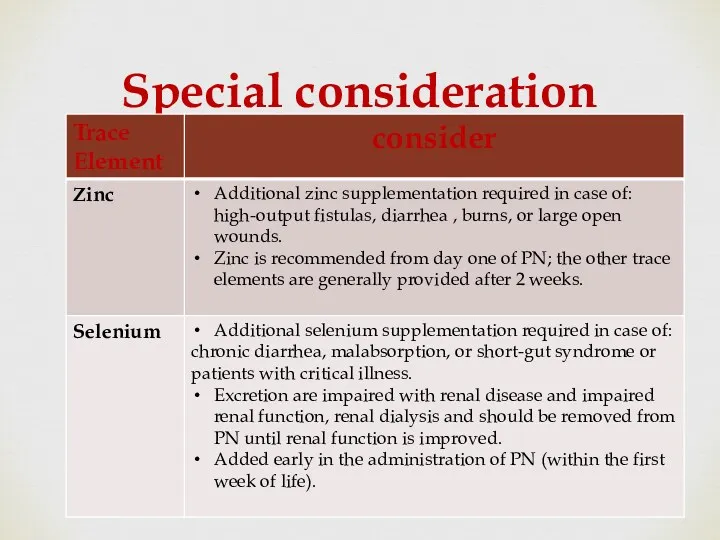
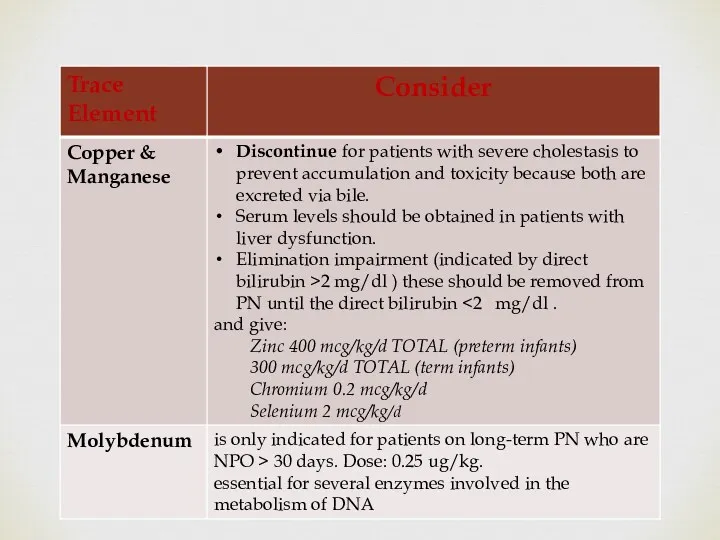
- 77. Special consideration
- 79. Medication Additives Continue Heparin: may be added to the TPN solutions in (0.5 - 1 unit/mL
- 80. There is no proven benefit of heparin for the prevention of thrombotic occlusion of CVC’s under
- 81. Medication Additives Continue Carnitine Should be added if a patient continues to require PN after 10
- 82. Medication Additives Continue H2 antagonist such as famotidine or ranitidine, may be added to the daily
- 83. Illustrative case A 5-day-old neonate, with gestational age of 28 weeks and birth weight of 900
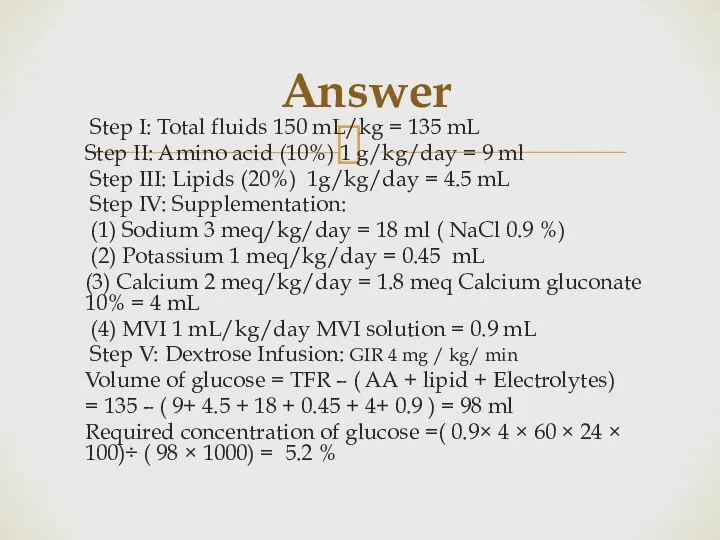
- 84. Answer Step I: Total fluids 150 mL/kg = 135 mL Step II: Amino acid (10%) 1
- 86. Скачать презентацию
Parenteral Nutrition
in Neonates
Prepared By
Neveen Hassan Abdel Aal
Clinical Pharmacist at NICU
Assuit University
Parenteral Nutrition
in Neonates
Prepared By
Neveen Hassan Abdel Aal
Clinical Pharmacist at NICU
Assuit University
Parenteral Nutrition: Definition & Goals.
Types of PN Admixtures.
Routes of Administration of
Parenteral Nutrition: Definition & Goals.
Types of PN Admixtures.
Routes of Administration of
Parenteral Nutrition
PN is the administration of intravenous nutrition in patients
Parenteral Nutrition
PN is the administration of intravenous nutrition in patients
Parenteral Nutrition Goals
(1) Weight maintenance or promoting growth.
(2) Preservation of
Parenteral Nutrition Goals
(1) Weight maintenance or promoting growth.
(2) Preservation of
Types of PN Admixtures
2 in 1
3 in 1
all nutrients are mixed
Types of PN Admixtures
2 in 1
3 in 1
all nutrients are mixed
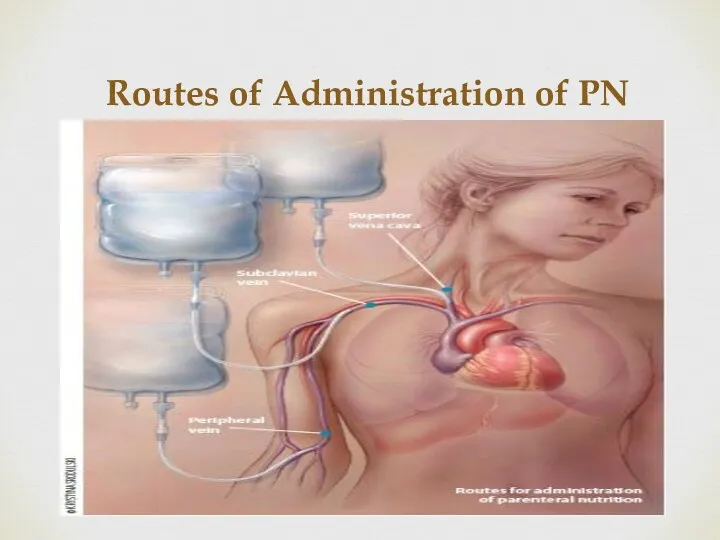
Routes of Administration of PN
Routes of Administration of PN
Central Access
Advantages :
No restrictions on the osmolarity of central PN,
Central Access
Advantages :
No restrictions on the osmolarity of central PN,
Central Access
Indications:
For patients who
require long-term nutritional support.
have large
Central Access
Indications:
For patients who
require long-term nutritional support.
have large
Criteria for Peripheral Administration
Osmolarity must not exceed 900 mOsm/L.
Final dextrose
Criteria for Peripheral Administration
Osmolarity must not exceed 900 mOsm/L.
Final dextrose
Nutritional Components of PN Formulation
PN should provide a balanced nutritional intake
Nutritional Components of PN Formulation
PN should provide a balanced nutritional intake
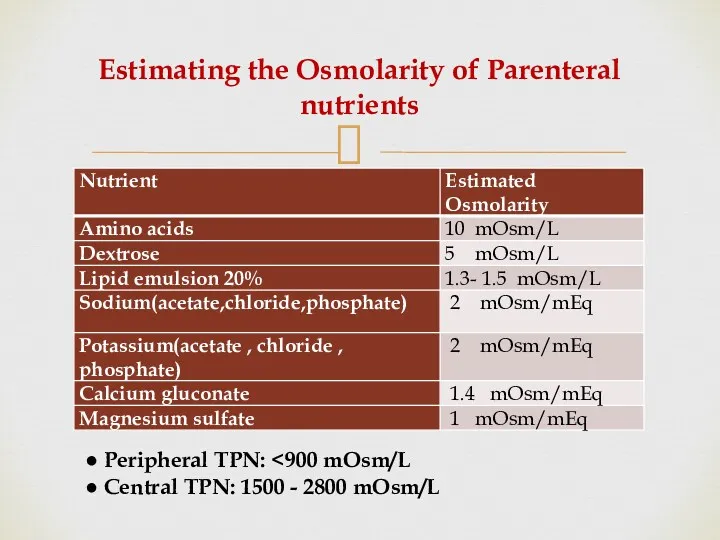
Estimating the Osmolarity of Parenteral nutrients
● Peripheral TPN: <900 mOsm/L
● Central
Estimating the Osmolarity of Parenteral nutrients
● Peripheral TPN: <900 mOsm/L
● Central
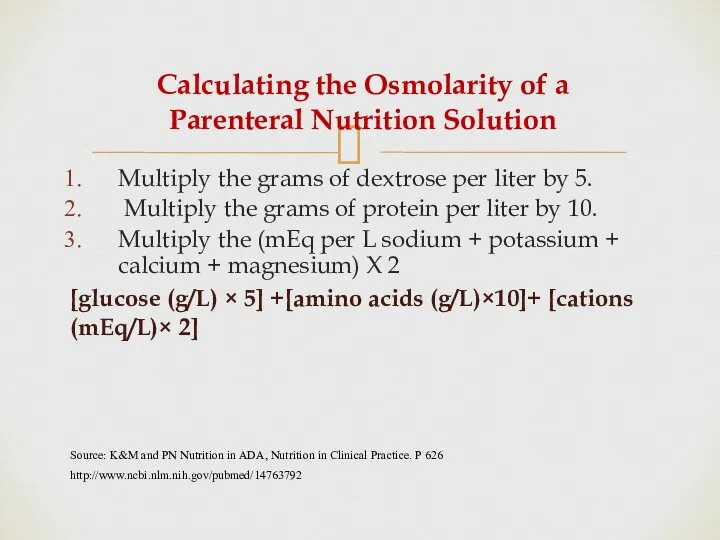
Calculating the Osmolarity of a Parenteral Nutrition Solution
Multiply the grams of
Calculating the Osmolarity of a Parenteral Nutrition Solution
Multiply the grams of
Developing a Regimen for PN Administration
Through Central Line
Developing a Regimen for PN Administration
Through Central Line
I. Evaluation of patient case
PN components should be adjusted individually to
I. Evaluation of patient case
PN components should be adjusted individually to
I. Evaluation of patient case
First of all Review:
Patient Age, weight (
I. Evaluation of patient case
First of all Review:
Patient Age, weight (
Evaluation of patient case continue
4. Assessment of degree of hydration.
Signs of
Evaluation of patient case continue
4. Assessment of degree of hydration.
Signs of
II. Start Calculating Components of PN Formula
Steps of Calculation
Fluid need/tolerated
(Subtract drugs,
II. Start Calculating Components of PN Formula
Steps of Calculation
Fluid need/tolerated
(Subtract drugs,
1.Determine Fluid Requirements
1.Determine Fluid Requirements
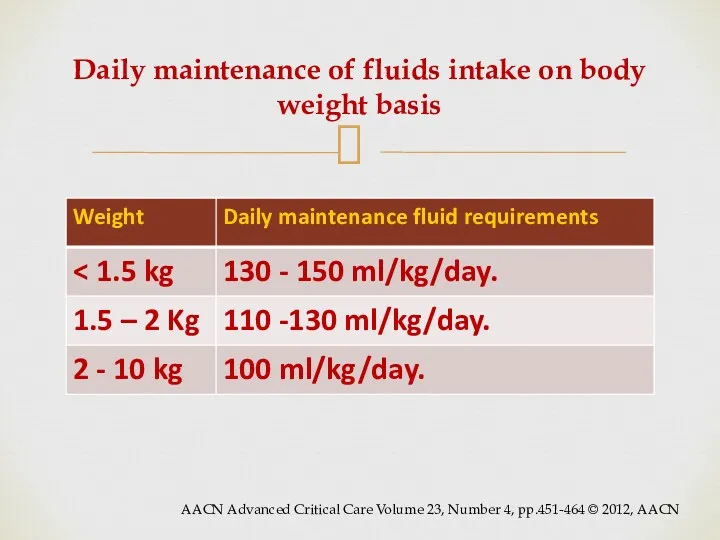
Daily maintenance of fluids intake on body weight basis
AACN Advanced Critical
Daily maintenance of fluids intake on body weight basis
AACN Advanced Critical
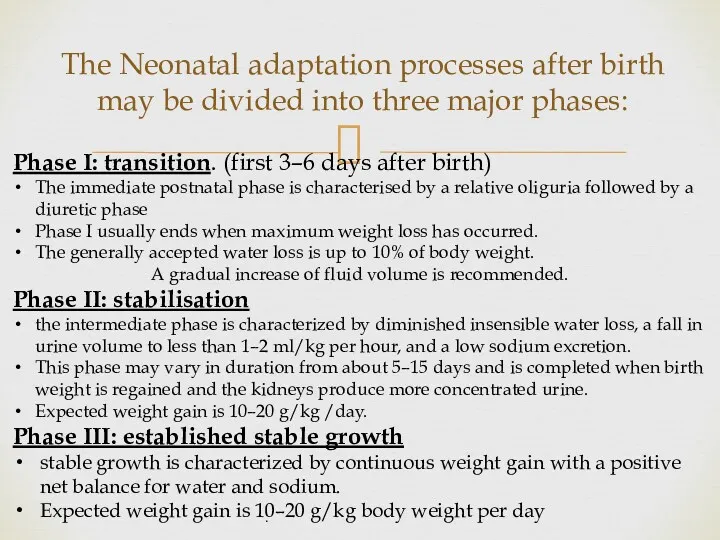
The Neonatal adaptation processes after birth may be divided into three
The Neonatal adaptation processes after birth may be divided into three
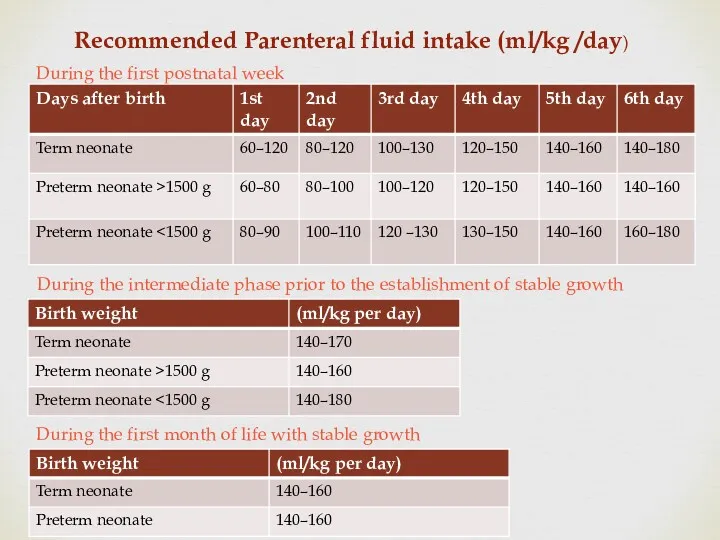
Recommended Parenteral fluid intake (ml/kg /day)
During the first postnatal week
During the
Recommended Parenteral fluid intake (ml/kg /day)
During the first postnatal week
During the
Variations in Fluid Requirements
Do not use PN for fluid replacement but
Variations in Fluid Requirements
Do not use PN for fluid replacement but
Suggested initial adjustment in specific situations
Fever…..+12% for each degree >37
Suggested initial adjustment in specific situations
Fever…..+12% for each degree >37
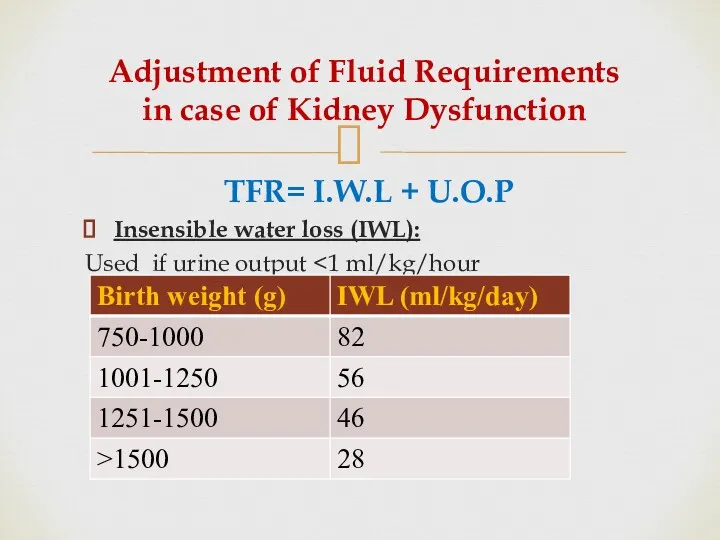
Adjustment of Fluid Requirements in case of Kidney Dysfunction
TFR= I.W.L +
Adjustment of Fluid Requirements in case of Kidney Dysfunction
TFR= I.W.L +
2. Determine Caloric Requirements
2. Determine Caloric Requirements
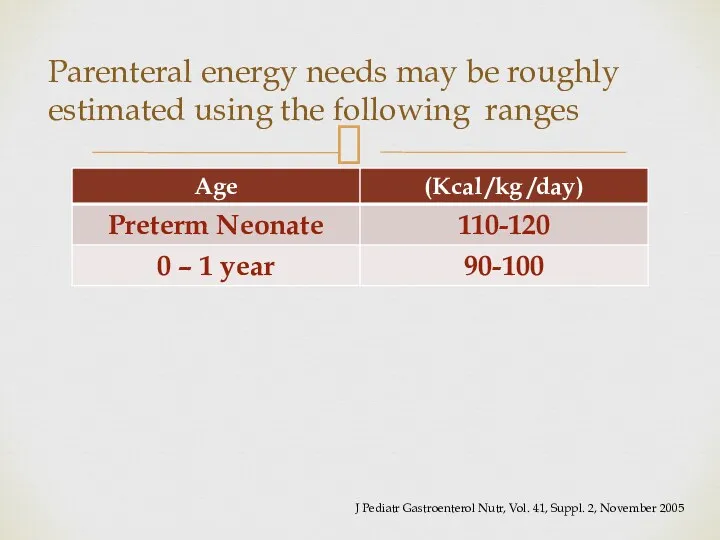
Parenteral energy needs may be roughly estimated using the following ranges
J
Parenteral energy needs may be roughly estimated using the following ranges
J
Further aspects need to be taken into account according to clinical
Further aspects need to be taken into account according to clinical
Variations in Caloric Requirements
Patient require increased caloric needs in case of
fever,
Variations in Caloric Requirements
Patient require increased caloric needs in case of
fever,
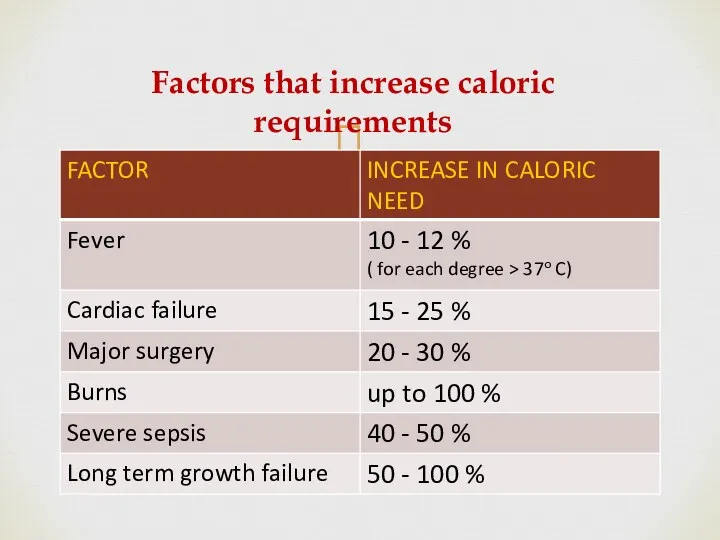
Factors that increase caloric requirements
Factors that increase caloric requirements
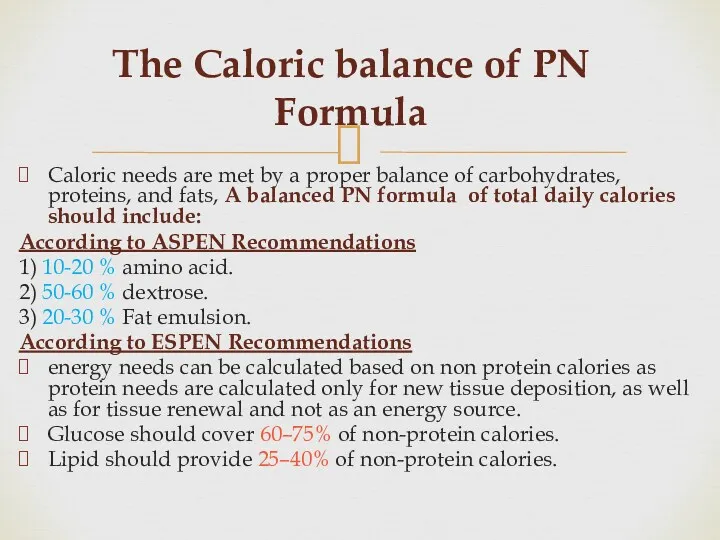
The Caloric balance of PN Formula
Caloric needs are met by a
The Caloric balance of PN Formula
Caloric needs are met by a
3.Determine Protein Requirements
Proteins are the major structural and functional components of
3.Determine Protein Requirements
Proteins are the major structural and functional components of
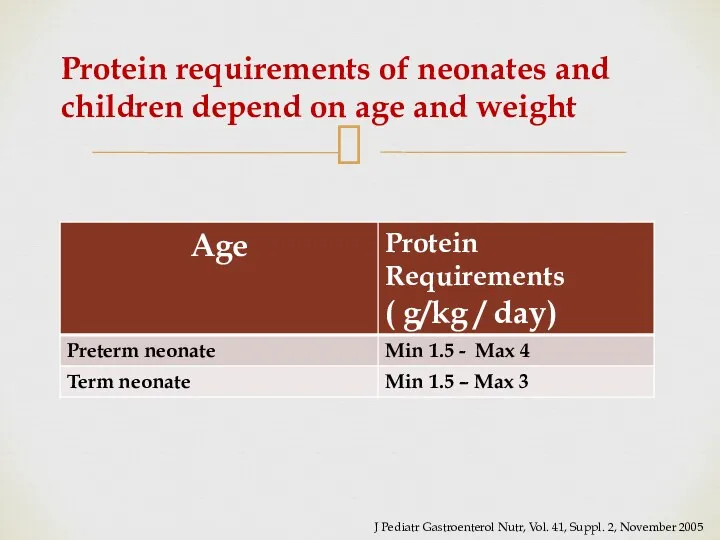
Protein requirements of neonates and children depend on age and weight
Protein requirements of neonates and children depend on age and weight
Regimen of Protein Administration
Start with 1.5 gm/kg/d and then
increase by
Regimen of Protein Administration
Start with 1.5 gm/kg/d and then
increase by
Protein requirements Variations
Increased amount of amino acids are required in case
Protein requirements Variations
Increased amount of amino acids are required in case
Potential complications and risks of providing IV amino acids
1-
Potential complications and risks of providing IV amino acids
1-
Caloric Value of Proteins
Calories from protein (4 kcal/g) Inadequate supplementation of
Caloric Value of Proteins
Calories from protein (4 kcal/g) Inadequate supplementation of
4.Determine Lipid Requirements
Providing fat is essential to
Achieve adequate caloric intake
4.Determine Lipid Requirements
Providing fat is essential to
Achieve adequate caloric intake
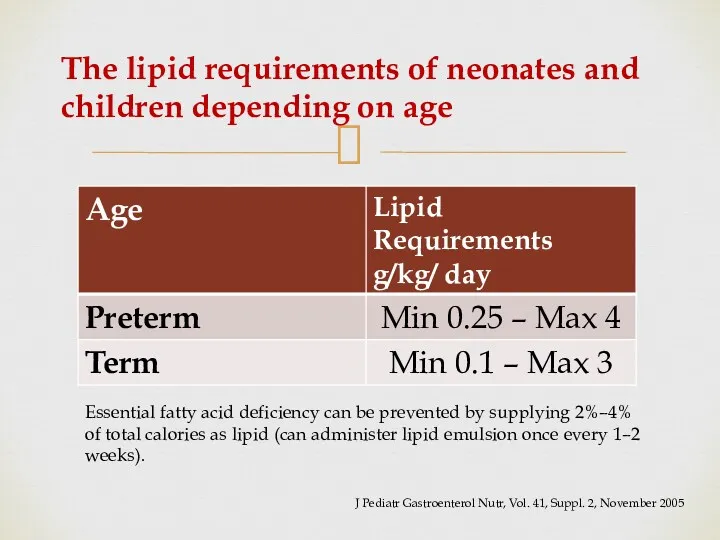
The lipid requirements of neonates and children depending on age
J
The lipid requirements of neonates and children depending on age
J
Regimen of Lipid Administration
Starting dose of 1 g/kg/day
Titrate toward the
Regimen of Lipid Administration
Starting dose of 1 g/kg/day
Titrate toward the
Caloric Value of Lipids
Calories from Lipid (10 kcal/g)
Maximum fat oxidation occurs
Caloric Value of Lipids
Calories from Lipid (10 kcal/g)
Maximum fat oxidation occurs
Precautions For Neonates
Restrict the dose of lipids in minimum amounts
Precautions For Neonates
Restrict the dose of lipids in minimum amounts
Potential complications and risks of providing IV Lipids
Hyperlipidemia.
Potential increased risk
Potential complications and risks of providing IV Lipids
Hyperlipidemia.
Potential increased risk
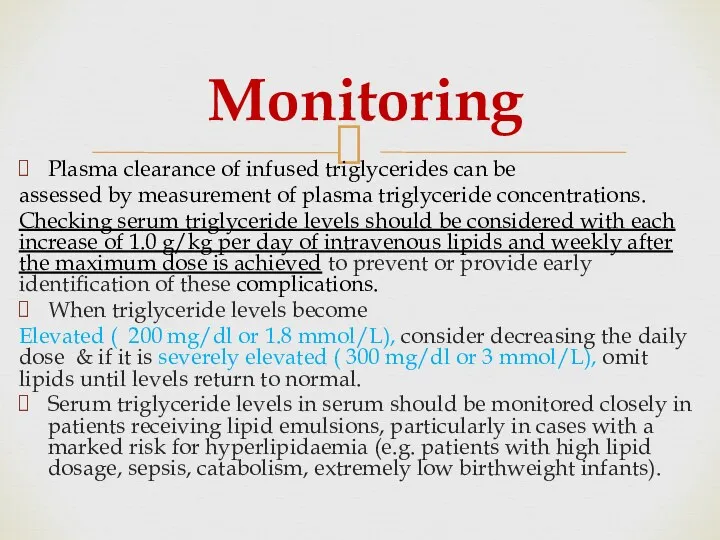
Monitoring
Plasma clearance of infused triglycerides can be
assessed by measurement of plasma
Monitoring
Plasma clearance of infused triglycerides can be
assessed by measurement of plasma
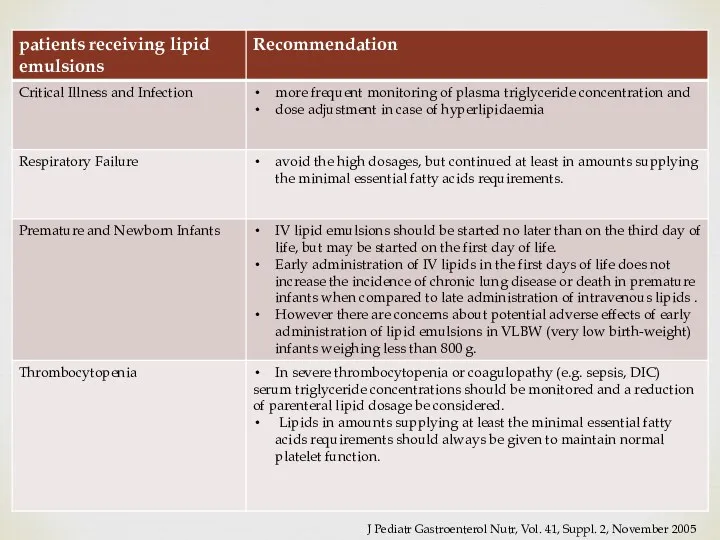
J Pediatr Gastroenterol Nutr, Vol. 41, Suppl. 2, November 2005
J Pediatr Gastroenterol Nutr, Vol. 41, Suppl. 2, November 2005
5. Determine Carbohydrates Requirements
Dextrose is major immediate energy source .
5. Determine Carbohydrates Requirements
Dextrose is major immediate energy source .
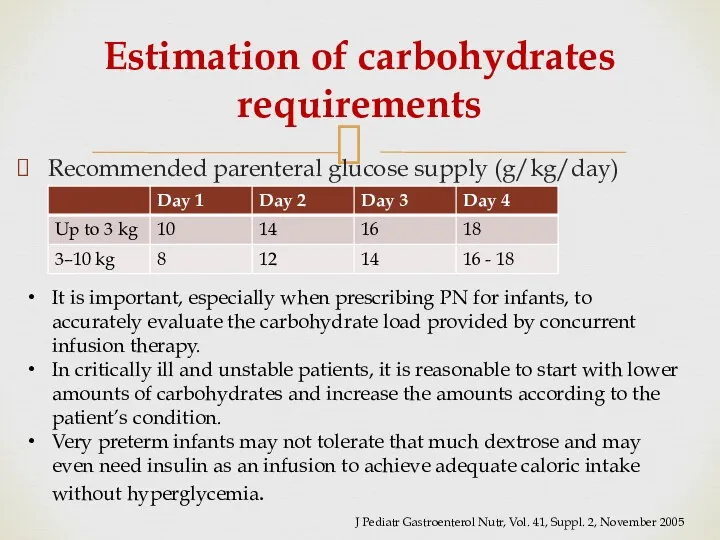
Recommended parenteral glucose supply (g/kg/day)
Estimation of carbohydrates requirements
It is important, especially
Recommended parenteral glucose supply (g/kg/day)
Estimation of carbohydrates requirements
It is important, especially
Carbohydrates Requirements need to be adapted according to
Age and clinical
Carbohydrates Requirements need to be adapted according to
Age and clinical
Regimen of Carbohydrate Administration
For neonates: Begin with GIR
4-8 mg/kg/min in preterm
Regimen of Carbohydrate Administration
For neonates: Begin with GIR
4-8 mg/kg/min in preterm
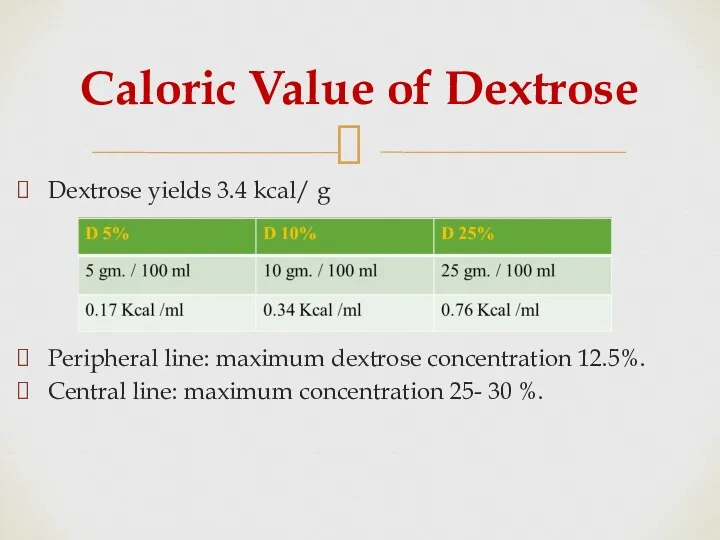
Caloric Value of Dextrose
Dextrose yields 3.4 kcal/ g
Peripheral line: maximum dextrose
Caloric Value of Dextrose
Dextrose yields 3.4 kcal/ g
Peripheral line: maximum dextrose
Potential complications
Hyperglycemia or hypoglycemia.
Glycosuria and potential osmotic diuresis.
Cholestasis and/or
Potential complications
Hyperglycemia or hypoglycemia.
Glycosuria and potential osmotic diuresis.
Cholestasis and/or
Managing Hyperglycemia in Neonates
If hyperglycemia develops:
↓GIR
insulin may improve
Managing Hyperglycemia in Neonates
If hyperglycemia develops:
↓GIR
insulin may improve
6. Estimate a Daily Maintenance amount of Electrolytes Vitamins &
Trace elements
6. Estimate a Daily Maintenance amount of Electrolytes Vitamins &
Trace elements
A) Electrolytes
Initial PN solutions may be started without added electrolytes.
Add
A) Electrolytes
Initial PN solutions may be started without added electrolytes.
Add
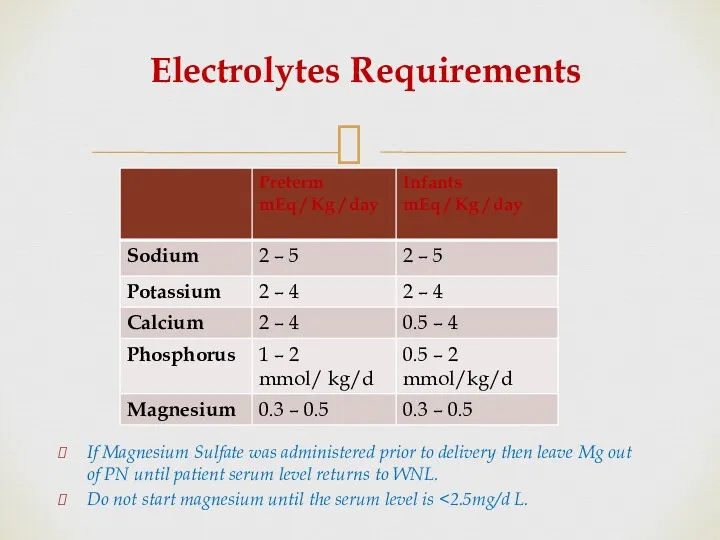
Electrolytes Requirements
If Magnesium Sulfate was administered prior to delivery then leave
Electrolytes Requirements
If Magnesium Sulfate was administered prior to delivery then leave
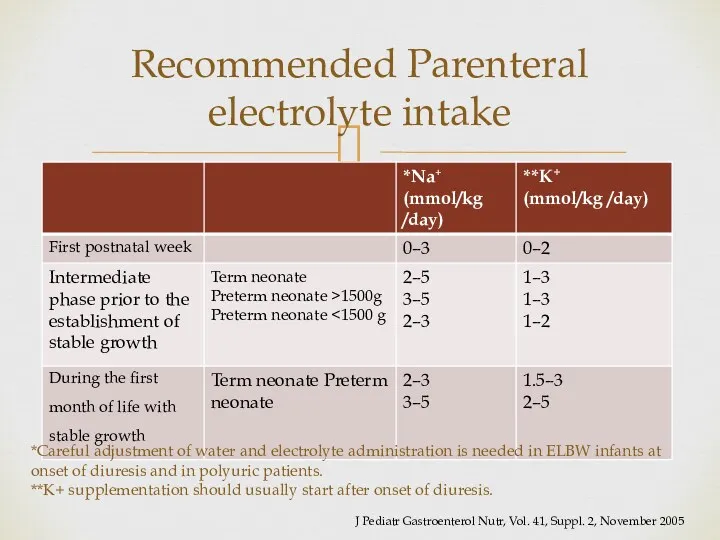
Recommended Parenteral electrolyte intake
*Careful adjustment of water and electrolyte administration
Recommended Parenteral electrolyte intake
*Careful adjustment of water and electrolyte administration
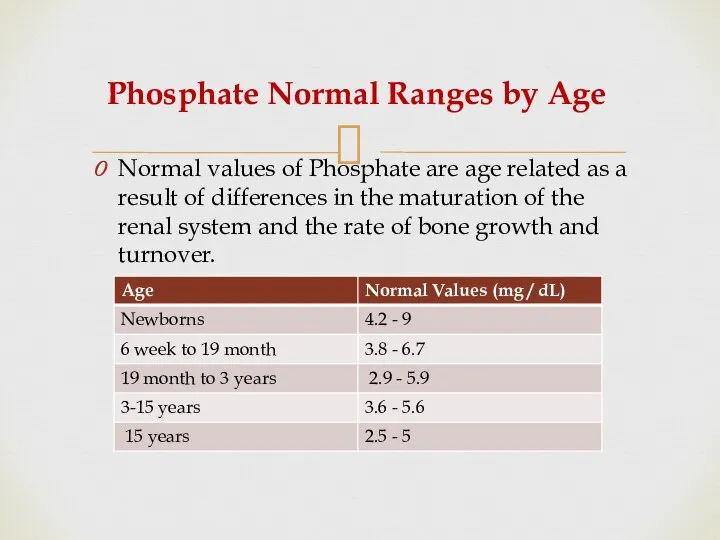
Phosphate Normal Ranges by Age
Normal values of Phosphate are age
Phosphate Normal Ranges by Age
Normal values of Phosphate are age
B) Trace Elements
Standard trace elements contain selenium, chromium, copper , manganese
B) Trace Elements
Standard trace elements contain selenium, chromium, copper , manganese
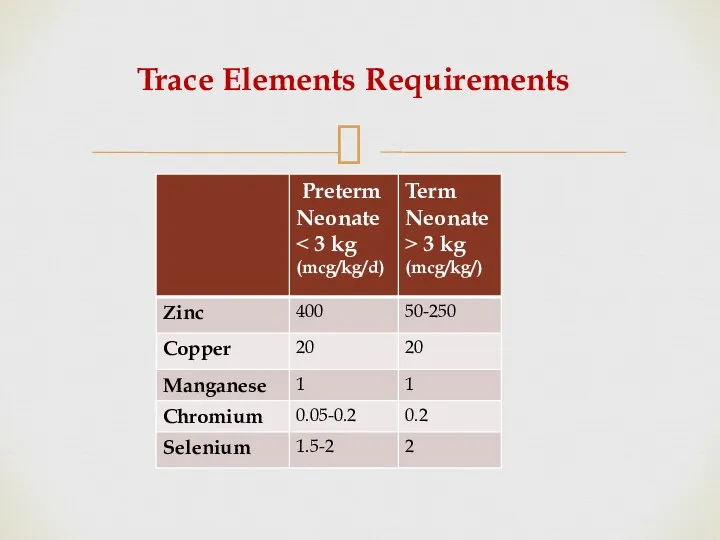
Trace Elements Requirements
Trace Elements Requirements
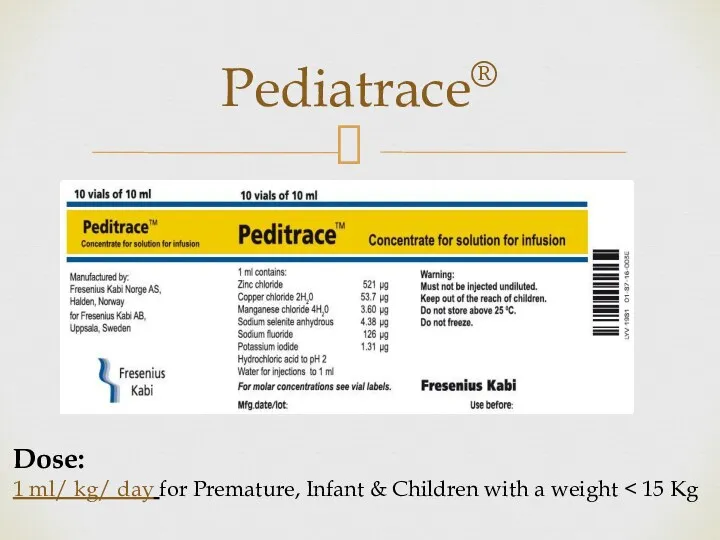
Pediatrace®
Dose:
1 ml/ kg/ day for Premature, Infant & Children with a
Pediatrace®
Dose:
1 ml/ kg/ day for Premature, Infant & Children with a
C) Vitamins Requirements
Similar to trace elements, multivitamins are often standard in
C) Vitamins Requirements
Similar to trace elements, multivitamins are often standard in
Medication Additives in PN
Generally, medications should not be added to PN
Medication Additives in PN
Generally, medications should not be added to PN
PN Complications
Short term Complications
1- Catheter-related infections
2- Catheter insertion complications
3-Peripheral Thrombophlebitis
4-Gut
PN Complications
Short term Complications
1- Catheter-related infections
2- Catheter insertion complications
3-Peripheral Thrombophlebitis
4-Gut
Short term Complications Continue
7. Refeeding syndrome
can occur in acutely or chronically
Short term Complications Continue
7. Refeeding syndrome
can occur in acutely or chronically
Long term Complications
1-Hepatobiliary Disorders
(includes steatosis, cholestasis, and gallbladder stones)
2-Osteoporosis &
Long term Complications
1-Hepatobiliary Disorders
(includes steatosis, cholestasis, and gallbladder stones)
2-Osteoporosis &
Monitoring PN Administration
1- Infection: Temperature ,WBC , IV access site
2- Peripheral
Monitoring PN Administration
1- Infection: Temperature ,WBC , IV access site
2- Peripheral
Monitoring Continue
5-Glycemic control(Hyperglycemia and hypoglycemia.)
Goal : 150 mg/dl or less
6- Monitor
Monitoring Continue
5-Glycemic control(Hyperglycemia and hypoglycemia.)
Goal : 150 mg/dl or less
6- Monitor
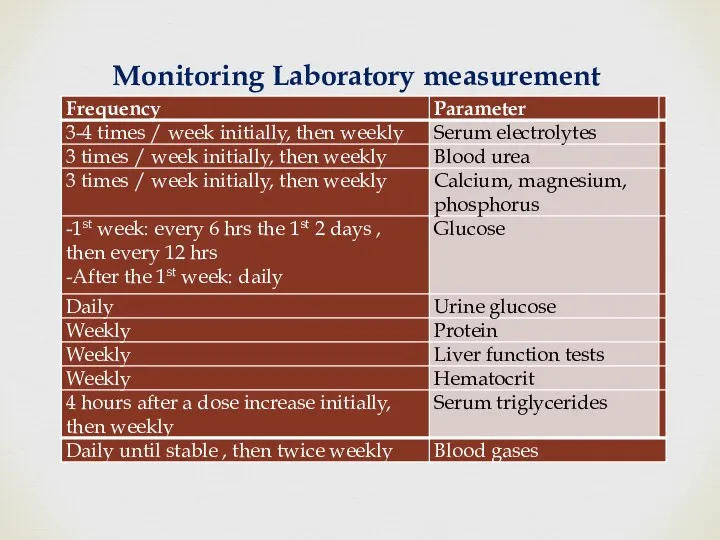
Monitoring Laboratory measurement
Monitoring Laboratory measurement
Transition to Oral or Enteral Nutrition
When initiating enteral or oral nutrition
Transition to Oral or Enteral Nutrition
When initiating enteral or oral nutrition

A- Patient data:
Age: 2year, weight: 10 kg, Phase: acute
B- Calculations:
1- Total
A- Patient data:
Age: 2year, weight: 10 kg, Phase: acute
B- Calculations:
1- Total
3- Lipids:
Dose 1.0 gm/kg/day.
Volume =10×1×(100/20)=50 ml/d
Calories= [10gm lipids×10kcal/gm]/10(weight)=10
3- Lipids:
Dose 1.0 gm/kg/day.
Volume =10×1×(100/20)=50 ml/d
Calories= [10gm lipids×10kcal/gm]/10(weight)=10
7- Calculation of glucose %
Total fluid intake 1000 ml/d.
Volume of glucose
7- Calculation of glucose %
Total fluid intake 1000 ml/d.
Volume of glucose
Preterm and Term Infants During the Transition Phase
Sodium, chloride and potassium
Preterm and Term Infants During the Transition Phase
Sodium, chloride and potassium
Electrolytes Function
Electrolytes Function
Trace Elements Function
Trace Elements Function
Special consideration
Special consideration
Medication Additives Continue
Heparin:
may be added to the TPN solutions in
Medication Additives Continue
Heparin:
may be added to the TPN solutions in
There is no proven benefit of heparin for the prevention of
There is no proven benefit of heparin for the prevention of
Medication Additives Continue
Carnitine
Should be added if a patient continues to
Medication Additives Continue
Carnitine
Should be added if a patient continues to
Medication Additives Continue
H2 antagonist
such as famotidine or ranitidine, may be added
Medication Additives Continue
H2 antagonist
such as famotidine or ranitidine, may be added
Illustrative case
A 5-day-old neonate,
with gestational age of 28 weeks and
Illustrative case
A 5-day-old neonate,
with gestational age of 28 weeks and
Answer
Step I: Total fluids 150 mL/kg = 135 mL
Step
Answer
Step I: Total fluids 150 mL/kg = 135 mL
Step
 Перикардиты. Анатомия перикарда
Перикардиты. Анатомия перикарда Спадкові захворювання нервової системи
Спадкові захворювання нервової системи ВИЧ: вопросы и ответы
ВИЧ: вопросы и ответы Нейтропении у детей
Нейтропении у детей Николай Иванович Пирогов Русский хирург и анатом
Николай Иванович Пирогов Русский хирург и анатом Информационные технологии для фармацевтов
Информационные технологии для фармацевтов Периоды детства
Периоды детства Антипсихотики (нейролептики)
Антипсихотики (нейролептики) Глобальные риски и новейшие медицинские технологии
Глобальные риски и новейшие медицинские технологии Компрессионные синдромы шейного отдела позвоночника
Компрессионные синдромы шейного отдела позвоночника Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау
Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау Інсульт. Причини, симптоми інсульту, перша допомога, поради
Інсульт. Причини, симптоми інсульту, перша допомога, поради Крон ауруы
Крон ауруы Pancreatic Cancer
Pancreatic Cancer Особенности фармакокинетики и фармакодинамики при лечении аллергий
Особенности фармакокинетики и фармакодинамики при лечении аллергий ИБС. Стенокардия
ИБС. Стенокардия Нәрестелердің асфиксиясы
Нәрестелердің асфиксиясы Опухолевый рост
Опухолевый рост Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы
Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы Нарушения сна у младенцев и детей раннего возраста
Нарушения сна у младенцев и детей раннего возраста Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову
Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову Токсикология фосфорорганических соединений (ФОС)
Токсикология фосфорорганических соединений (ФОС) Анатомо-фізіологічні особливості сечовидільної системи у дітей
Анатомо-фізіологічні особливості сечовидільної системи у дітей Өлім, өлім белгілері
Өлім, өлім белгілері Ми қыртысының анатомиялық-гистологиялық құрылымы
Ми қыртысының анатомиялық-гистологиялық құрылымы Воспалительные процессы органов женской половой системы специфической этиологии
Воспалительные процессы органов женской половой системы специфической этиологии Болезнь Крона
Болезнь Крона Respiratory system
Respiratory system