- Peptic Ulcer Diseases

Содержание
- 2. Definitions Ulcer: A lesion on an epithelial surface (skin or mucous membrane) caused by superficial loss
- 3. Definitions Peptic Ulcer An ulcer of the alimentary tract mucosa, usually in the stomach or duodenum,
- 4. Peptic Ulcer Disease
- 5. Pathophysiology A peptic ulcer is a mucosal break, 3 mm or greater in size with depth,
- 6. Pathophysiology Two major variants in peptic ulcers are commonly encountered in the clinical practice: Duodenal Ulcer
- 7. Pathophysiology DU result from increased acid load to the duodenum due to: Increased acid secretion because
- 8. Pathophysiology DU result from increased acid load to the duodenum due to: Smoking impairing gastric mucosal
- 9. Pathophysiology GU results from the break down of gastric mucosa: Associated with gastritis affecting the body
- 10. Etiology The two most common causes of PUD are: Helicobacter pylori infection ( 70-80%) Non-steroidal anti-inflammatory
- 11. Etiology Other uncommon causes include: Gastrinoma (Gastrin secreting tumor) Stress ulceration (trauma, burns, critical illness) Viral
- 12. 1. Etiology – Helicobacter pylori
- 13. H.pylori Epidemiology One half of world’s population has H.pylori infection, with an estimated prevalence of 80-90
- 14. H.pylori as a cause of PUD The majority of PUD patients are H. pylori infected
- 15. H.pylori as a cause of PUD 95% 85%
- 16. Carcinogenic effect of H. pylori H. pylori Host Factors Other environmental Factors Antral gastritis Pangastritis DU
- 17. Type of NSAID & Risk of Ulcer
- 18. Clinical Presentation Recurrent epigastric pain (the most common symptom) Burning Occurs 1-3 hours after meals Relieved
- 19. Clinical Presentation Nausea, Vomiting Dyspepsia, fatty food intolerance Chest discomfort Anorexia, weight loss especially in GU
- 20. Diagnosis of PUD
- 21. Peptic Ulcer Disease Diagnosis: Diagnosis of ulcer Diagnosis of H. pylori
- 22. Diagnosis of PUD In most patients routine laboratory tests are usually unhelpful Diagnosis of PUD depends
- 23. Doudenal Ulcer on Endoscopy Doudenal Ulcer Normal doudenal bulb
- 24. Gastric Ulcer on Endoscopy Chronic Gastric Ulcers
- 25. Diagnosis of H. pylori Non-invasive C13 or C14 Urea Breath Test Stool antigen test H. pylori
- 26. Diagnosis of H. pylori Non-invasive 1. C13 or C14 Urea Breath Test The best test for
- 27. Diagnosis of H. pylori Non-invasive Serology for H pylori Serum Antibodies (IgG) to H pylori (Not
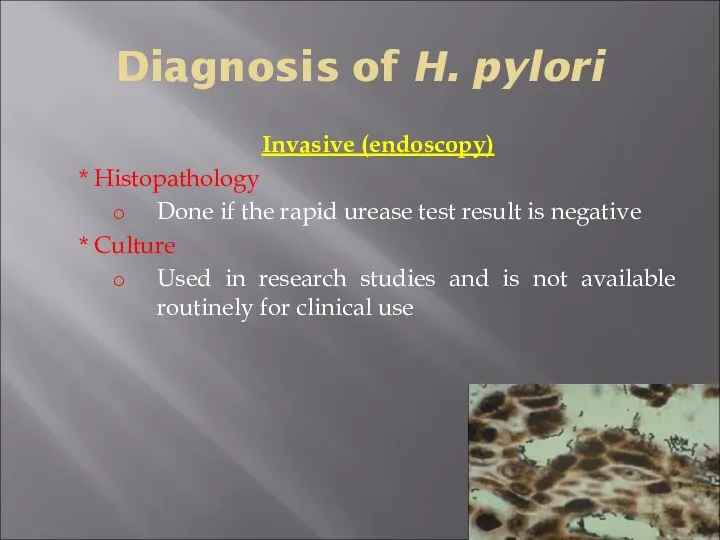
- 28. Diagnosis of H. pylori Invasive Upper GI endoscopy Highly sensitive test Patient needs sedation Has both
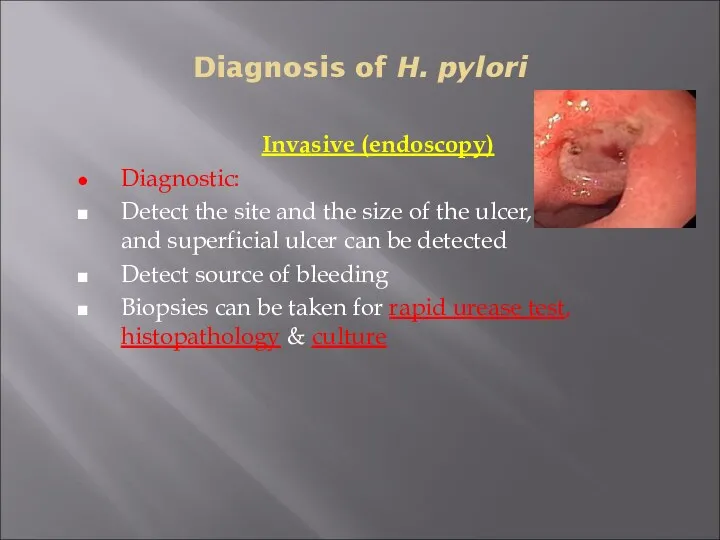
- 29. Diagnosis of H. pylori Invasive (endoscopy) Diagnostic: Detect the site and the size of the ulcer,
- 30. Diagnosis of H. pylori Invasive (endoscopy) Rapid urease test ( RUT) Considered the endoscopic diagnostic test
- 31. Diagnosis of H. pylori Invasive (endoscopy) * Histopathology Done if the rapid urease test result is
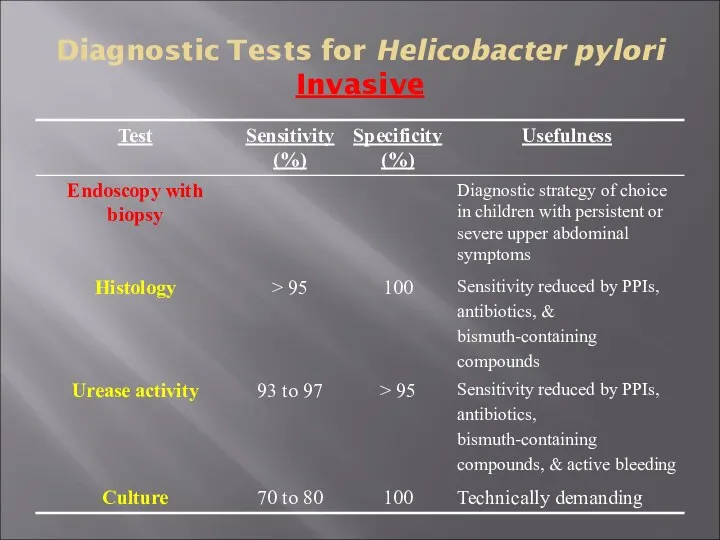
- 32. Diagnostic Tests for Helicobacter pylori Invasive
- 33. PUD – Complications Bleeding Perforation Gastric outlet or duodenal obstruction Chronic anemia
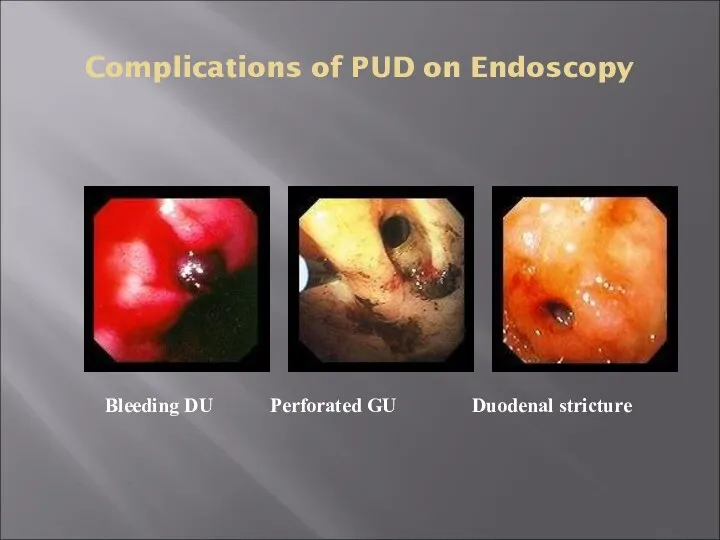
- 34. Complications of PUD on Endoscopy Bleeding DU Perforated GU Duodenal stricture
- 35. PUD Treatment
- 36. Treatment Goals Rapid relief of symptoms Healing of ulcer Preventing ulcer recurrences Reducing ulcer-related complications Reduce
- 37. General Strategy Treat complications aggressively if present Determine the etiology of ulcer Discontinue NSAID use if
- 38. General Strategy Smoking cessation should be encouraged If DU is diagnosed by endoscopy, RU testing of
- 39. Drugs Therapy H2-Receptors antagonists Proton pump inhibitors Cyto-protective agents Prostaglandin agonists Antacids Antibiotics for H. pylori
- 41. Скачать презентацию
Definitions
Ulcer:
A lesion on an epithelial surface (skin or mucous membrane) caused
Definitions
Ulcer:
A lesion on an epithelial surface (skin or mucous membrane) caused
Definitions
Peptic Ulcer
An ulcer of the alimentary tract mucosa, usually in the
Definitions
Peptic Ulcer
An ulcer of the alimentary tract mucosa, usually in the
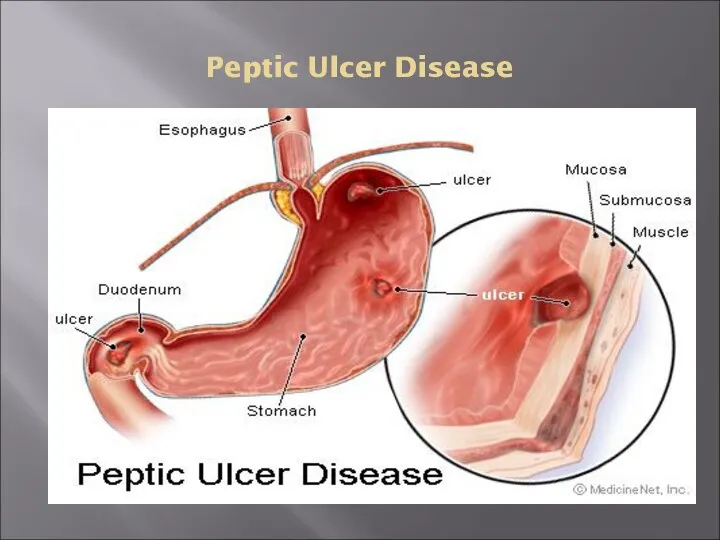
Peptic Ulcer Disease
Peptic Ulcer Disease

Pathophysiology
A peptic ulcer is a mucosal break, 3 mm or greater
Pathophysiology
A peptic ulcer is a mucosal break, 3 mm or greater
Pathophysiology
Two major variants in peptic ulcers are commonly encountered in the
Pathophysiology
Two major variants in peptic ulcers are commonly encountered in the
Pathophysiology
DU result from increased acid load to the duodenum due to:
Increased
Pathophysiology
DU result from increased acid load to the duodenum due to:
Increased
Pathophysiology
DU result from increased acid load to the duodenum due to:
Smoking
Pathophysiology
DU result from increased acid load to the duodenum due to:
Smoking
Pathophysiology
GU results from the break down of gastric mucosa:
Associated with gastritis
Pathophysiology
GU results from the break down of gastric mucosa:
Associated with gastritis
Etiology
The two most common causes of PUD are:
Helicobacter pylori infection
Etiology
The two most common causes of PUD are:
Helicobacter pylori infection
Etiology
Other uncommon causes include:
Gastrinoma (Gastrin secreting tumor)
Stress ulceration (trauma, burns, critical
Etiology
Other uncommon causes include:
Gastrinoma (Gastrin secreting tumor)
Stress ulceration (trauma, burns, critical
1. Etiology – Helicobacter pylori
1. Etiology – Helicobacter pylori
H.pylori Epidemiology
One half of world’s population has H.pylori infection, with an
H.pylori Epidemiology
One half of world’s population has H.pylori infection, with an
H.pylori as a cause of PUD
The majority of PUD patients
H.pylori as a cause of PUD
The majority of PUD patients
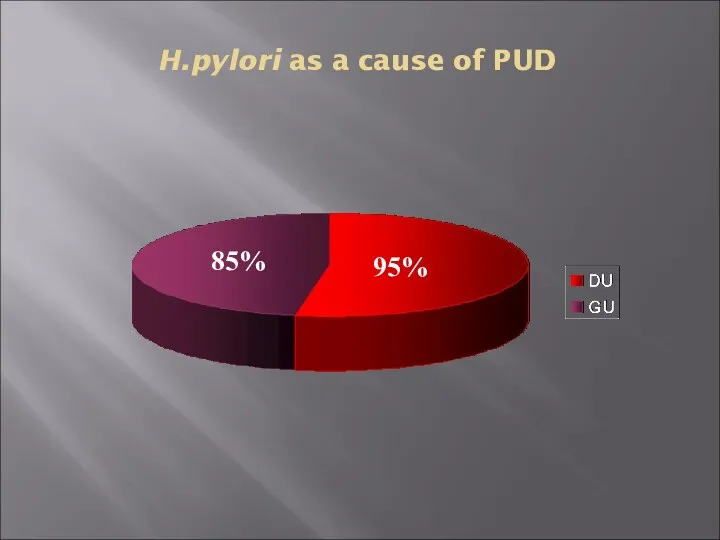
H.pylori as a cause of PUD
95%
85%
H.pylori as a cause of PUD
95%
85%
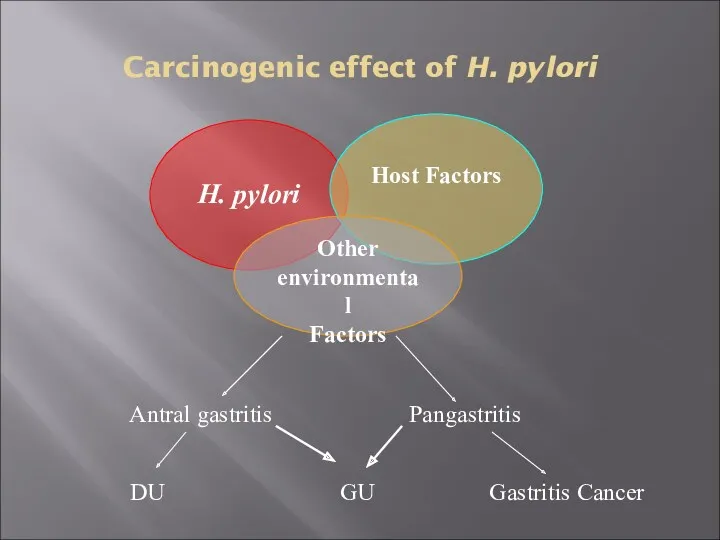
Carcinogenic effect of H. pylori
H. pylori
Host Factors
Other environmental
Factors
Antral
Carcinogenic effect of H. pylori
H. pylori
Host Factors
Other environmental
Factors
Antral
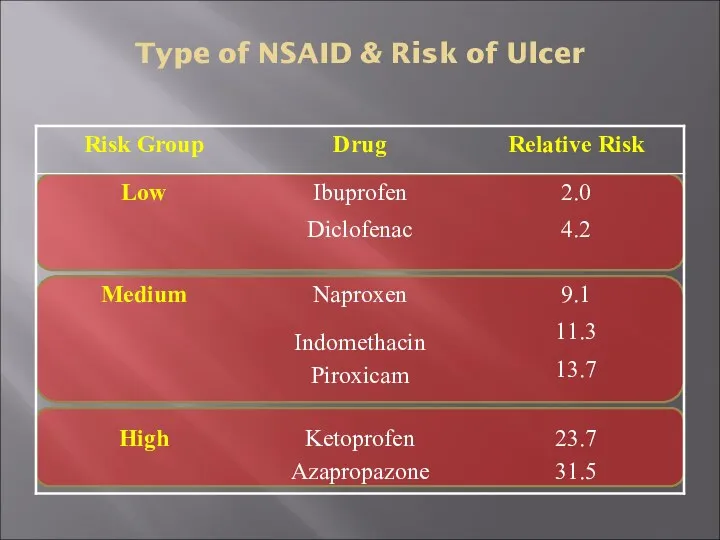
Type of NSAID & Risk of Ulcer
Type of NSAID & Risk of Ulcer
Clinical Presentation
Recurrent epigastric pain (the most common symptom)
Burning
Occurs 1-3 hours after
Clinical Presentation
Recurrent epigastric pain (the most common symptom)
Burning
Occurs 1-3 hours after
Clinical Presentation
Nausea, Vomiting
Dyspepsia, fatty food intolerance
Chest discomfort
Anorexia, weight loss especially in
Clinical Presentation
Nausea, Vomiting
Dyspepsia, fatty food intolerance
Chest discomfort
Anorexia, weight loss especially in
Diagnosis of PUD
Diagnosis of PUD
Peptic Ulcer Disease
Diagnosis:
Diagnosis of ulcer
Diagnosis of H. pylori
Peptic Ulcer Disease
Diagnosis:
Diagnosis of ulcer
Diagnosis of H. pylori
Diagnosis of PUD
In most patients routine laboratory tests are usually
Diagnosis of PUD
In most patients routine laboratory tests are usually
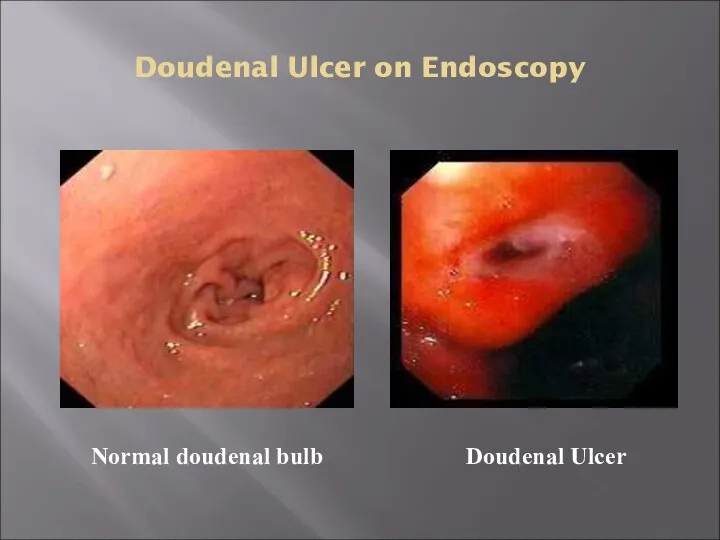
Doudenal Ulcer on Endoscopy
Doudenal Ulcer
Normal doudenal bulb
Doudenal Ulcer on Endoscopy
Doudenal Ulcer
Normal doudenal bulb
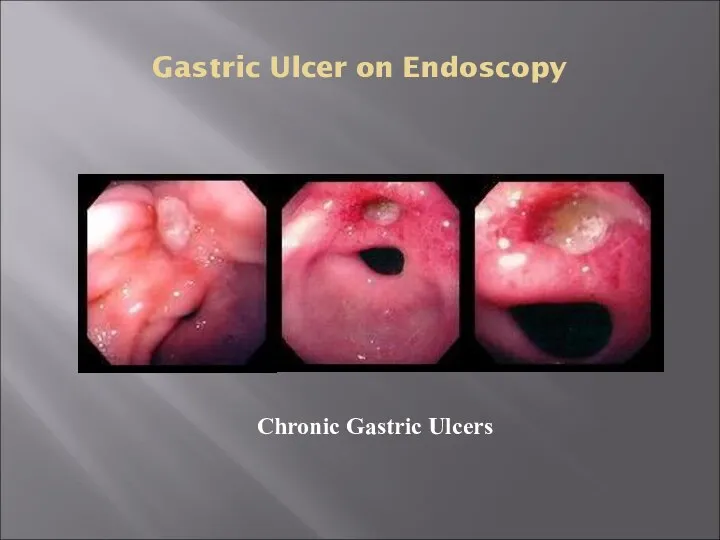
Gastric Ulcer on Endoscopy
Chronic Gastric Ulcers
Gastric Ulcer on Endoscopy
Chronic Gastric Ulcers
Diagnosis of H. pylori
Non-invasive
C13 or C14 Urea Breath Test
Stool antigen test
H.
Diagnosis of H. pylori
Non-invasive
C13 or C14 Urea Breath Test
Stool antigen test
H.
Diagnosis of H. pylori
Non-invasive
1. C13 or C14 Urea Breath
Diagnosis of H. pylori
Non-invasive
1. C13 or C14 Urea Breath
Diagnosis of H. pylori
Non-invasive
Serology for H pylori
Serum Antibodies (IgG) to
Diagnosis of H. pylori
Non-invasive
Serology for H pylori
Serum Antibodies (IgG) to
Diagnosis of H. pylori
Invasive
Upper GI endoscopy
Highly sensitive test
Patient needs sedation
Has both
Diagnosis of H. pylori
Invasive
Upper GI endoscopy
Highly sensitive test
Patient needs sedation
Has both
Diagnosis of H. pylori
Invasive (endoscopy)
Diagnostic:
Detect the site and the size of
Diagnosis of H. pylori
Invasive (endoscopy)
Diagnostic:
Detect the site and the size of
Diagnosis of H. pylori
Invasive (endoscopy)
Rapid urease test ( RUT)
Considered the endoscopic
Diagnosis of H. pylori
Invasive (endoscopy)
Rapid urease test ( RUT)
Considered the endoscopic
Diagnosis of H. pylori
Invasive (endoscopy)
* Histopathology
Done if the rapid urease test
Diagnosis of H. pylori
Invasive (endoscopy)
* Histopathology
Done if the rapid urease test
Diagnostic Tests for Helicobacter pylori
Invasive
Diagnostic Tests for Helicobacter pylori
Invasive
PUD – Complications
Bleeding
Perforation
Gastric outlet or duodenal obstruction
Chronic anemia
PUD – Complications
Bleeding
Perforation
Gastric outlet or duodenal obstruction
Chronic anemia
Complications of PUD on Endoscopy
Bleeding DU Perforated GU Duodenal stricture
Complications of PUD on Endoscopy
Bleeding DU Perforated GU Duodenal stricture

PUD Treatment
Treatment Goals
Rapid relief of symptoms
Healing of ulcer
Preventing ulcer recurrences
Reducing ulcer-related
Treatment Goals
Rapid relief of symptoms
Healing of ulcer
Preventing ulcer recurrences
Reducing ulcer-related
General Strategy
Treat complications aggressively if present
Determine the etiology of ulcer
Discontinue
General Strategy
Treat complications aggressively if present
Determine the etiology of ulcer
Discontinue
General Strategy
Smoking cessation should be encouraged
If DU is diagnosed by
General Strategy
Smoking cessation should be encouraged
If DU is diagnosed by
Drugs Therapy
H2-Receptors antagonists
Proton pump inhibitors
Cyto-protective agents
Prostaglandin agonists
Antacids
Antibiotics for
Drugs Therapy
H2-Receptors antagonists
Proton pump inhibitors
Cyto-protective agents
Prostaglandin agonists
Antacids
Antibiotics for
 Противомикробные средства. Антисептики и дезинфицирующие средства
Противомикробные средства. Антисептики и дезинфицирующие средства Сосудистый шов
Сосудистый шов Анемії. Лейкози гострий і хронічний
Анемії. Лейкози гострий і хронічний Геморрагический шок в акушерстве
Геморрагический шок в акушерстве Жұқпалы аурулар эпидемиологиясы
Жұқпалы аурулар эпидемиологиясы Показания к переводу на искусственную вентиляцию легких. Параметры КЩС. Режимы вентиляции
Показания к переводу на искусственную вентиляцию легких. Параметры КЩС. Режимы вентиляции Пороки развития позвоночника
Пороки развития позвоночника Нейрофизиология. Двигательная функция ЦНС. (Лекция 8)
Нейрофизиология. Двигательная функция ЦНС. (Лекция 8) Анатомия и биомеханика ВНЧС
Анатомия и биомеханика ВНЧС Лечебно-профилактическое и лечебное питание
Лечебно-профилактическое и лечебное питание Общая фармакология
Общая фармакология Перечень действующих документов по профилактике инфекционных заболеваний
Перечень действующих документов по профилактике инфекционных заболеваний Блокады вымени
Блокады вымени Бронх обструктивті синдром
Бронх обструктивті синдром Острый гематогенный остеомиелит, эпифизарный остеомиелит
Острый гематогенный остеомиелит, эпифизарный остеомиелит Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких Остеология. Кости таза и нижних конечностей
Остеология. Кости таза и нижних конечностей Заболеваемость населения. Инвалидность. Физическое развитие. Социально значимые заболевания
Заболеваемость населения. Инвалидность. Физическое развитие. Социально значимые заболевания Умственная отсталость
Умственная отсталость АИТВ/ЖИТС туралы
АИТВ/ЖИТС туралы Постановка периферического венозного катетера
Постановка периферического венозного катетера Quản lí và đánh giá công nghệ y tế
Quản lí và đánh giá công nghệ y tế Острый гломерулонефрит
Острый гломерулонефрит Использование аэрозольного ингалятора флутиказона пропионата в сочетании с сальметеролом в лечении бронхиальной астмы
Использование аэрозольного ингалятора флутиказона пропионата в сочетании с сальметеролом в лечении бронхиальной астмы Синдром длительного сдавления (СДС)
Синдром длительного сдавления (СДС) Дерматомиозит. Симптомы, течение
Дерматомиозит. Симптомы, течение Развитие лица и ротовой полости
Развитие лица и ротовой полости Ведение беременных с бронхиальной астмой
Ведение беременных с бронхиальной астмой