- Polymyalgia rheumatica

Содержание
- 2. Introduction Polymyalgia rheumatica (PMR) is an inflammatory rheumatic condition Characterized clinically by : aching and morning
- 4. Epidemiology Disease of adults over the age of 50, with a prevalence that increases progressively with
- 5. Association with GCA PMR occurs in about 50% of patients with GCA The percentage of patients
- 6. Pathogenesis The cause of polymyalgia rheumatica (PMR) is unknown Both environmental and genetic factors appear to
- 7. Signs and Symptoms Aching and morning stiffness Shoulders, hip girdle, neck, and torso are involved Patients
- 9. Signs and Symptoms Morning stiffness > 30 minutes Stiffness at the shoulders and hips may cause
- 10. Signs and Symptoms Shoulder pain is more common at presentation than hip pain Pain is worse
- 11. Laboratory findings Elevated ESR, CRP (although can be normal) Normocytic anemia Thrombocytosis Serologic tests, such as
- 12. Imaging Routine radiographs of inflamed joints do not show abnormalities in patients with PMR MRI and
- 13. Extra-articular involvement Biceps tenosynovitis subdeltoid bursitis
- 14. Evaluation of the patient Medical history Anemnesis Physical examination Assessment of the response to low-dose glucocorticoids.
- 15. Diagnosis No pathognomonic test or established diagnostic criteria for polymyalgia rheumatica (PMR) Presence of all of
- 16. Evaluation for GCA Patients with clinically "pure" PMR lack the classic findings of GCA: temporal artery
- 17. Diffrential Diagnosis Rheumatoid arthritis - symmetric polyarthritis of the small joints of the hands and feet,
- 19. Скачать презентацию
Introduction
Polymyalgia rheumatica (PMR) is an inflammatory rheumatic condition
Characterized clinically by :
aching
Introduction
Polymyalgia rheumatica (PMR) is an inflammatory rheumatic condition
Characterized clinically by :
aching

Epidemiology
Disease of adults over the age of 50, with a prevalence
Epidemiology
Disease of adults over the age of 50, with a prevalence
Association with GCA
PMR occurs in about 50% of patients with GCA
Association with GCA
PMR occurs in about 50% of patients with GCA
Pathogenesis
The cause of polymyalgia rheumatica (PMR) is unknown
Both environmental and genetic
Pathogenesis
The cause of polymyalgia rheumatica (PMR) is unknown
Both environmental and genetic
Signs and Symptoms
Aching and morning stiffness
Shoulders, hip girdle, neck, and
Signs and Symptoms
Aching and morning stiffness
Shoulders, hip girdle, neck, and

Signs and Symptoms
Morning stiffness > 30 minutes
Stiffness at the shoulders and
Signs and Symptoms
Morning stiffness > 30 minutes
Stiffness at the shoulders and
Signs and Symptoms
Shoulder pain is more common at presentation than hip
Signs and Symptoms
Shoulder pain is more common at presentation than hip
Laboratory findings
Elevated ESR, CRP (although can be normal)
Normocytic anemia
Thrombocytosis
Serologic tests, such
Laboratory findings
Elevated ESR, CRP (although can be normal)
Normocytic anemia
Thrombocytosis
Serologic tests, such
Imaging
Routine radiographs of inflamed joints do not show abnormalities in patients
Imaging
Routine radiographs of inflamed joints do not show abnormalities in patients
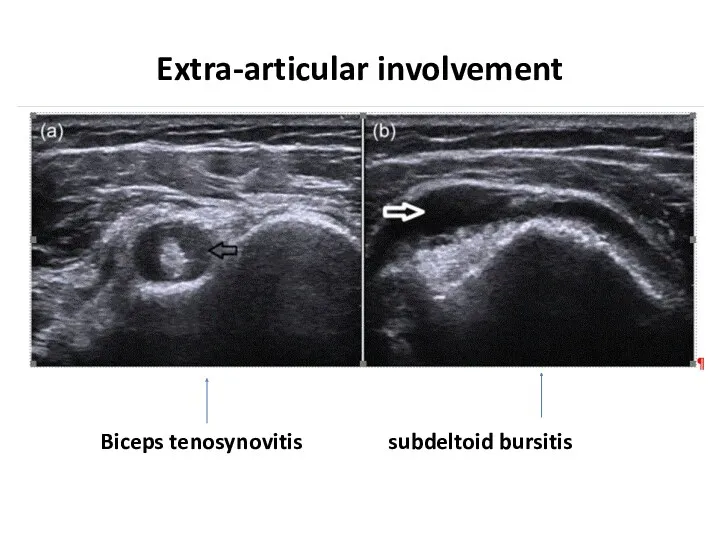
Extra-articular involvement
Biceps tenosynovitis subdeltoid bursitis
Extra-articular involvement
Biceps tenosynovitis subdeltoid bursitis
Evaluation of the patient
Medical history
Anemnesis
Physical examination
Assessment of the response to low-dose
Evaluation of the patient
Medical history
Anemnesis
Physical examination
Assessment of the response to low-dose
Diagnosis
No pathognomonic test or established diagnostic criteria for polymyalgia rheumatica (PMR)
Presence
Diagnosis
No pathognomonic test or established diagnostic criteria for polymyalgia rheumatica (PMR)
Presence
Evaluation for GCA
Patients with clinically "pure" PMR lack the classic findings
Evaluation for GCA
Patients with clinically "pure" PMR lack the classic findings
Diffrential Diagnosis
Rheumatoid arthritis - symmetric polyarthritis of the small joints of
Diffrential Diagnosis
Rheumatoid arthritis - symmetric polyarthritis of the small joints of
 Державна санітарно-епідеміологічна експертиза, як елемент соціально-гігієнічного моніторингу. Основні положення та організація
Державна санітарно-епідеміологічна експертиза, як елемент соціально-гігієнічного моніторингу. Основні положення та організація Операции на органах шеи
Операции на органах шеи Физиология паращитовидных желёз
Физиология паращитовидных желёз Повреждения и заболевания мочеполовых органов
Повреждения и заболевания мочеполовых органов Хирург Н.Н. Бурденко
Хирург Н.Н. Бурденко Арбовирусты инфекциялар. Кенелік энцефалит вирусы
Арбовирусты инфекциялар. Кенелік энцефалит вирусы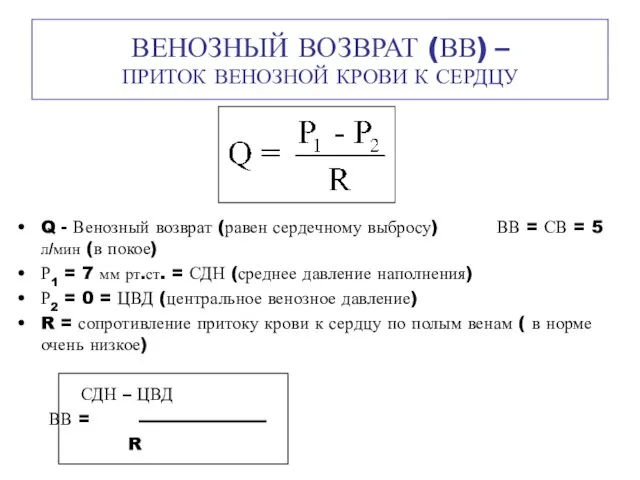 Венозный возврат (ВВ) – приток венозной крови к сердцу
Венозный возврат (ВВ) – приток венозной крови к сердцу Шум и вибрация
Шум и вибрация Алкогольный цирроз
Алкогольный цирроз Возрастные особенности системы крови и иммунитета
Возрастные особенности системы крови и иммунитета Неврозы
Неврозы Противоаритмические лекарственные средства
Противоаритмические лекарственные средства Здоровье на работе. Что должен знать о ВИЧ/СПИДе каждый?
Здоровье на работе. Что должен знать о ВИЧ/СПИДе каждый? Гигиена аптечных заведений
Гигиена аптечных заведений Гиперчувствительность. Иммунодефициты. Аутоиммунные процессы
Гиперчувствительность. Иммунодефициты. Аутоиммунные процессы Послеродовые депрессии
Послеродовые депрессии Аллергия. Стоматология
Аллергия. Стоматология 84-я Всероссийская научная конференция студентов и молодых ученых. Отчет. Секция: Общая хирургия
84-я Всероссийская научная конференция студентов и молодых ученых. Отчет. Секция: Общая хирургия Клинико-экономические исследования
Клинико-экономические исследования Химиотерапевтические лекарственные препараты, макролиды и азалиды
Химиотерапевтические лекарственные препараты, макролиды и азалиды Пороки сердца
Пороки сердца Асқорыту жолдарының қатерлі және қатерсіз ісіктері
Асқорыту жолдарының қатерлі және қатерсіз ісіктері Мировые демографические показатели рождаемость, смертность в развитых и развивающихся странах. Демографическая ситуация в Росси
Мировые демографические показатели рождаемость, смертность в развитых и развивающихся странах. Демографическая ситуация в Росси Классификация геморрагического васкулита
Классификация геморрагического васкулита Белки
Белки ЦМК СД в акушерстве и гинекологии ,
ЦМК СД в акушерстве и гинекологии , Medical Education in Japan
Medical Education in Japan Заболевания органов пищеварения у пожилых людей
Заболевания органов пищеварения у пожилых людей