- Postpartum haemorrhage and obstetric shock

Содержание
- 2. Content: Definition Causes Predisposing factor How to evaluate haemorrhage Prevention Management Definition of Obstetric shock Systemic
- 3. DEFINITION OF PPH: Blood loss in excess of 500 mls during the first 24 hours after
- 4. Causes: Uterine atony Genital tract trauma Retained placental tissue Low placental implantation Uterine inversion Coagulation disorders
- 5. I – Uterine Atony (75% - 80%) Causes: General anesthesia: Halogenated hydrocarbon Over distended uterus large
- 6. II – Genital tract trauma It is usually suspected if bleeding persists in the presence of
- 7. PREDISPOSING FACTOR OF TRAUMA: Delivery of a large baby Mid forceps delivery Intra uterine manipulation Vaginal
- 8. VULVOVAGINAL HEMATOMA Hematoma can be associated with early or late haemorrhage Classification: Vulvar haematoma classified according
- 9. and limited from spread to the thigh by colle’s facia and facia lata. The central tendon
- 10. RETAINED PLACENTAL TISSUE Retained placenta is a common cause of bleeding late in the puerperium inspection
- 11. PLACENTA ACCRETA, INCRETA, PERCRETA As the consequence of partial or total absence of the decidua basalis
- 12. ETIOLOGY Implantation in the lower uterine segment over previous cesarean section scar, or other uterine incision,
- 13. LOW PLACENTA IMPLANTATION Due to the relative decrease in the Content musculature in the lower uterine
- 14. UTERINE INVERSION It is due to premature strong traction on an umbilical cord attached to a
- 15. CLASSIFICATION Acute Sub acute Chronic
- 16. COAGULATION DISORDERS Abruptio placenta Amniotic fluid embolism Retained dead fetus Inherited coagulopathy (Von-Wille brand’s disease) DIC
- 17. CLASSIFICATION OF HAEMORRHAGE 4 CLASSES depend on volume lost 60 Kg pregnant woman has a blood
- 18. 3. Class III: Is defined as blood loss sufficient to cause overt hypotension Blood loss of
- 19. PREVENTION Identify patient at risk of postpartum haemorrhage Prepare blood at least 4 units of packed
- 20. 4. Use of oxytocin infusion after placental delivery 5. Carefully inspection of the placenta and membrane
- 21. MANAGEMENT OF UTERINE ATONY Patient showing signs of class II or greater volume loss should receive
- 22. 4. Inform anesthesia and keep patient nil per mouth 5. Ask for assistant 6. Bimanual compression
- 23. If failed prostaglandin F2α the total dose is 1 – 2 mg diluted in 10 –
- 24. SURGICAL METHOD Ligation of the ascending branch of the uterine arteries Ligation of hypogastric artery Hysterectomy
- 25. OBSTETRIC SHOCK Hypotension without significant external bleeding Causes: Concealed haemorrhage Uterine inversion Amniotic fluid embolism
- 26. CAUSE OF CONCEALED HAEMORRHAGE Spontaneous uterine rupture 2. Retroperitoneal bleeding from vaginal tears 3. Perineal hematoma
- 27. AMNIOTIC FLUID EMBOLISM Rare, 1 of 30,000 deliveries Mortality rate is 50% The definitive diagnosis of
- 28. CLINICAL PRESENTATION Respiratory distress Cyanosis Cardio vascular collapse Haemorrhage Coma
- 29. TREATMENT Endotracheal intubation and maximum ventilation and oxygenation Restore cardio vascular equilibrium Central monitoring of fluid
- 30. MASSIVE BLOOD TRANSFUSION It is the replacement of a patient entire blood volume in 24 hours
- 31. COMPLICATION OF MASSIVE TRANSFUSION If more than 4 units of packed RBC,platelet count will drop, there
- 32. PROGNOSIS OF POSTPARTUM HAEMORRHAGE Women with postpartum haemorrhage should not die Renal failure from prolong hypotension
- 33. BLOOD PRODUCTS Whole blood Packed red blood cells, most effective and efficient way to provide increase
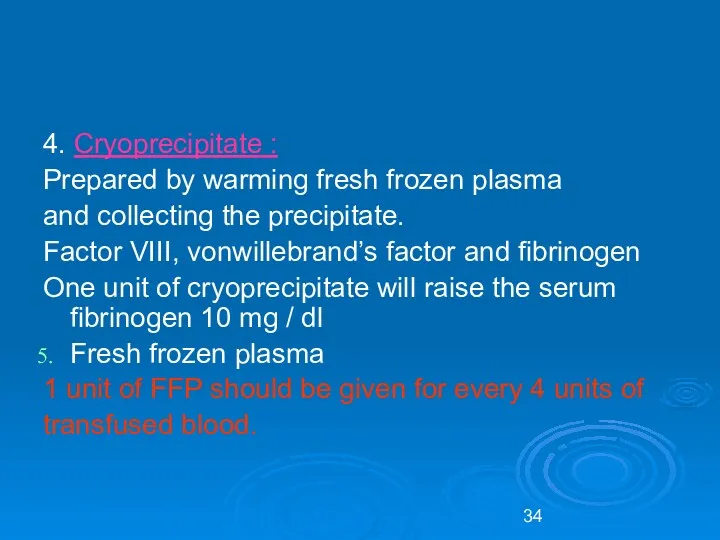
- 34. 4. Cryoprecipitate : Prepared by warming fresh frozen plasma and collecting the precipitate. Factor VIII, vonwillebrand’s
- 36. Скачать презентацию
Content:
Definition
Causes
Predisposing factor
How to evaluate haemorrhage
Prevention
Management
Content:
Definition
Causes
Predisposing factor
How to evaluate haemorrhage
Prevention
Management
DEFINITION OF PPH:
Blood loss in excess of 500 mls during the
DEFINITION OF PPH:
Blood loss in excess of 500 mls during the
Causes:
Uterine atony
Genital tract trauma
Retained placental tissue
Low placental
Causes:
Uterine atony
Genital tract trauma
Retained placental tissue
Low placental
I – Uterine Atony (75% - 80%)
Causes:
General anesthesia: Halogenated
I – Uterine Atony (75% - 80%)
Causes:
General anesthesia: Halogenated
II – Genital tract trauma
It is usually suspected if bleeding persists
II – Genital tract trauma
It is usually suspected if bleeding persists
PREDISPOSING FACTOR OF TRAUMA:
Delivery of a large baby
Mid forceps delivery
PREDISPOSING FACTOR OF TRAUMA:
Delivery of a large baby
Mid forceps delivery
VULVOVAGINAL HEMATOMA
Hematoma can be associated with early or late
VULVOVAGINAL HEMATOMA
Hematoma can be associated with early or late
and limited from spread to the thigh by colle’s facia and
and limited from spread to the thigh by colle’s facia and
RETAINED PLACENTAL TISSUE
Retained placenta is a common cause of bleeding
RETAINED PLACENTAL TISSUE
Retained placenta is a common cause of bleeding
PLACENTA ACCRETA, INCRETA, PERCRETA
As the consequence of partial or total absence
PLACENTA ACCRETA, INCRETA, PERCRETA
As the consequence of partial or total absence
ETIOLOGY
Implantation in the lower uterine segment over previous cesarean section
ETIOLOGY
Implantation in the lower uterine segment over previous cesarean section
LOW PLACENTA IMPLANTATION
Due to the relative decrease in the
Content musculature
LOW PLACENTA IMPLANTATION
Due to the relative decrease in the
Content musculature
UTERINE INVERSION
It is due to premature strong traction on an
UTERINE INVERSION
It is due to premature strong traction on an
CLASSIFICATION
Acute
Sub acute
Chronic
CLASSIFICATION
Acute
Sub acute
Chronic
COAGULATION DISORDERS
Abruptio placenta
Amniotic fluid embolism
Retained dead fetus
Inherited
COAGULATION DISORDERS
Abruptio placenta
Amniotic fluid embolism
Retained dead fetus
Inherited
CLASSIFICATION OF HAEMORRHAGE
4 CLASSES depend on volume lost
60 Kg
CLASSIFICATION OF HAEMORRHAGE
4 CLASSES depend on volume lost
60 Kg
3. Class III: Is defined as blood loss sufficient to cause
3. Class III: Is defined as blood loss sufficient to cause
PREVENTION
Identify patient at risk of postpartum haemorrhage
Prepare blood at
PREVENTION
Identify patient at risk of postpartum haemorrhage
Prepare blood at
4. Use of oxytocin infusion after placental delivery
5. Carefully inspection of
5. Carefully inspection of
MANAGEMENT OF UTERINE ATONY
Patient showing signs of class II or greater
MANAGEMENT OF UTERINE ATONY
Patient showing signs of class II or greater
4. Inform anesthesia and keep patient nil per mouth
5. Ask
4. Inform anesthesia and keep patient nil per mouth
5. Ask
If failed prostaglandin F2α the total dose is 1 – 2
If failed prostaglandin F2α the total dose is 1 – 2
SURGICAL METHOD
Ligation of the ascending branch of the uterine arteries
SURGICAL METHOD
Ligation of the ascending branch of the uterine arteries
OBSTETRIC SHOCK
Hypotension without significant external
bleeding
Causes:
Concealed haemorrhage
Uterine inversion
OBSTETRIC SHOCK
Hypotension without significant external
bleeding
Causes:
Concealed haemorrhage
Uterine inversion
CAUSE OF CONCEALED HAEMORRHAGE
Spontaneous uterine rupture
2. Retroperitoneal bleeding from
CAUSE OF CONCEALED HAEMORRHAGE
Spontaneous uterine rupture
2. Retroperitoneal bleeding from
AMNIOTIC FLUID EMBOLISM
Rare, 1 of 30,000 deliveries
Mortality rate is
AMNIOTIC FLUID EMBOLISM
Rare, 1 of 30,000 deliveries
Mortality rate is
CLINICAL PRESENTATION
Respiratory distress
Cyanosis
Cardio vascular collapse
Haemorrhage
Coma
CLINICAL PRESENTATION
Respiratory distress
Cyanosis
Cardio vascular collapse
Haemorrhage
Coma
TREATMENT
Endotracheal intubation and maximum ventilation and oxygenation
Restore cardio vascular
TREATMENT
Endotracheal intubation and maximum ventilation and oxygenation
Restore cardio vascular
MASSIVE BLOOD TRANSFUSION
It is the replacement of a patient entire blood
MASSIVE BLOOD TRANSFUSION
It is the replacement of a patient entire blood
COMPLICATION OF MASSIVE TRANSFUSION
If more than 4 units of packed RBC,platelet
COMPLICATION OF MASSIVE TRANSFUSION
If more than 4 units of packed RBC,platelet
PROGNOSIS OF POSTPARTUM HAEMORRHAGE
Women with postpartum haemorrhage should not die
PROGNOSIS OF POSTPARTUM HAEMORRHAGE
Women with postpartum haemorrhage should not die
BLOOD PRODUCTS
Whole blood
Packed red blood cells, most effective and efficient
BLOOD PRODUCTS
Whole blood
Packed red blood cells, most effective and efficient
4. Cryoprecipitate :
Prepared by warming fresh frozen plasma
and collecting the
4. Cryoprecipitate :
Prepared by warming fresh frozen plasma
and collecting the
 Средства, угнетающие холинергические синапсы
Средства, угнетающие холинергические синапсы Средства, влияющие на систему крови
Средства, влияющие на систему крови 20 апреля – День донора
20 апреля – День донора Модели организации скорой медицинской помощи в стационарных условиях
Модели организации скорой медицинской помощи в стационарных условиях Диспансерная группа пациентов с факторами риска в отделениях, кабинетах медицинской профилактики
Диспансерная группа пациентов с факторами риска в отделениях, кабинетах медицинской профилактики Расстройства пищевого поведения. Ожирение, медицинские и психологические последствия, проблемы лечения и коррекции. Занятие 7
Расстройства пищевого поведения. Ожирение, медицинские и психологические последствия, проблемы лечения и коррекции. Занятие 7 Здоровый образ жизни
Здоровый образ жизни Псориаз. Особенности клинического течения у детей. Красный плоский лишай. Пиодермии у детей. Чесотка
Псориаз. Особенности клинического течения у детей. Красный плоский лишай. Пиодермии у детей. Чесотка Врожденные дисплазии соединительной ткани
Врожденные дисплазии соединительной ткани Особенности познавательных процессов у лиц с ДЦП
Особенности познавательных процессов у лиц с ДЦП Ошибки диагностики и лечения при сочетанной травме
Ошибки диагностики и лечения при сочетанной травме Врожденные пороки развития челюстно-лицевой области
Врожденные пороки развития челюстно-лицевой области Аллергический ринит
Аллергический ринит Летательные аппараты разных времен
Летательные аппараты разных времен Нейрофизиологические аспекты речи
Нейрофизиологические аспекты речи Признаки блокады ножек пучка гиса на ЭКГ
Признаки блокады ножек пучка гиса на ЭКГ Воспалительные заболевания сосудистой оболочки
Воспалительные заболевания сосудистой оболочки Лабораторная диагностика нарушений гемостаза
Лабораторная диагностика нарушений гемостаза Современные принципы сердечно-легочной реанимации и профилактики внезапной сердечной смерти
Современные принципы сердечно-легочной реанимации и профилактики внезапной сердечной смерти Омолаживающие операции на лице и шее
Омолаживающие операции на лице и шее Биоматериал для исследования
Биоматериал для исследования Радиоактивті индикаторларды халық шаруашылығының әртүрлі салаларында қолданылуы
Радиоактивті индикаторларды халық шаруашылығының әртүрлі салаларында қолданылуы Микробиологическая диагностика стафилококковых и стрептококковых заболеваний
Микробиологическая диагностика стафилококковых и стрептококковых заболеваний Ультразвуковое исследование поджелудочной железы
Ультразвуковое исследование поджелудочной железы Общая пропедевтика мочевыделительной системы
Общая пропедевтика мочевыделительной системы Дыхательная гимнастика по методике Б.С. Толкачева. презентация
Дыхательная гимнастика по методике Б.С. Толкачева. презентация Мамандандырылған және арнайы мамандандырылған медициналық көмек
Мамандандырылған және арнайы мамандандырылған медициналық көмек Системные заболевания опорно-двигательного аппарата у детей
Системные заболевания опорно-двигательного аппарата у детей