- Public health. Medicare and medicaid. Law and poverty

Содержание
- 3. Insurance Coverage - US 60% Private Insurance 19% Have No Insurance – 46 million 27% Public/
- 4. Rising Healthcare Costs Since 2000, the cost of family health insurance has risen 87% Since 2000,
- 5. Declining Employer Coverage of Insurance In 2000, 69% of businesses gave some of their workers health
- 6. Medicare What is it? What kind of law is it? How is a person eligible? What
- 7. What is Medicare? Federal Law Medicare is a nationwide federal health insurance program for the aged
- 8. Eligibility for Medicare Depends on part Part A- hospital insurance almost all persons over 65, (those
- 10. What is Medicare Benefit? Very much like insurance with co-pays, deductibles, etc. Part A: inpatient hospital
- 11. Administration of Medicare? CMS, within the Dept of Health and Human Services; CMS=Center for Medicare and
- 12. Who pays for Medicare? Part A: recips pay a deductible Financed by HI, (hospital insurance) part
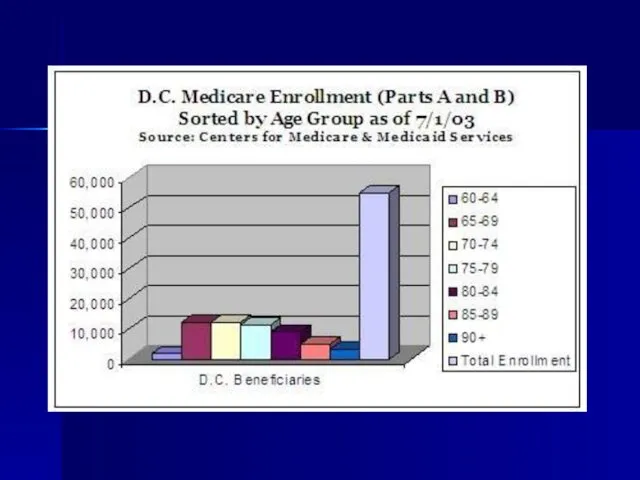
- 13. What is Medicare’s Constituency? Over 41 million people enrolled in Medicare as of 2003 35 Million
- 14. Medicare Coverage
- 15. Medicare History Enacted in 1965, the Medicare program immediately covered 19.1 million people when it went
- 16. Medical Care in Other Countries In 1883, Germany passed a sickness insurance law which created mandatory
- 17. Who are collateral beneficiaries?
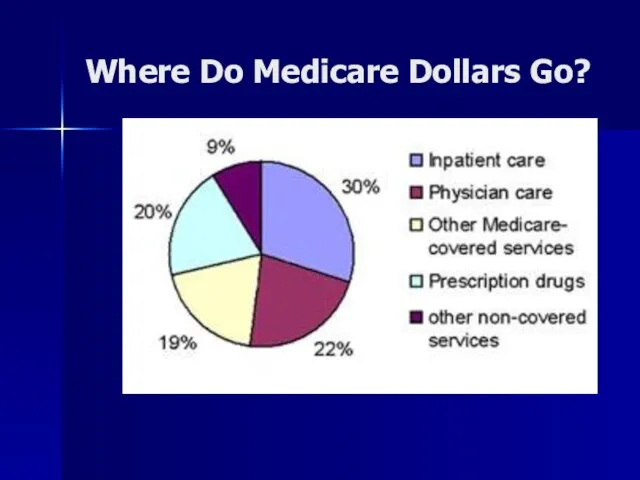
- 18. : Where Do Medicare Dollars Go?
- 19. How Much Does Medicare Cost? 2006 Estimate $345 billion 2004 was $283 billion 1999 was $212
- 21. New Medicare Benefit Prescription Drug Coverage
- 22. Medicare Drug Benefit Choices From January 2006 beneficiaries can choose to (a) stay in traditional Medicare,
- 23. Medicare Drug Benefits Enrollees will have an annual deductible of $250, an estimated premium of $35
- 25. Annual deductible of $250; Premium of $35 a month (may vary in private plans); 25 percent
- 26. Low-Income Drug Subsidies: People eligible for Medicaid and Medicare will pay no premium or deductible and
- 27. People with incomes below about $13,000 ($17,600 for couples) in 2006 and assets of under $6,000
- 29. 2007 Medicare Changes: The Part B premium will be linked to income for the first time,
- 30. Drug Profits – Fortune Magazine
- 31. Medicaid What is it? What kind of law is it? How is a person eligible? What
- 32. Medicaid A federal-state program providing medical assistance to low-income persons who are aged, blind, disabled, members
- 33. Medicaid Law Joint Federal and State Law
- 34. Eligibility for Medicaid FINANCIAL REQUIREMENTS: First must be indigent Income and Resources
- 35. Eligibility Medicaid: Mandatory Families Aid to Families with Dependent Children (AFDC); Supplemental Security Income (SSI) recipients;
- 36. What benefit is conferred? MUST OFFER: inpatient outpatient nursing home care MAY OFFER: eyeglasses prescription drugs
- 37. Administration of Medicaid FEDERAL: CMS AND HHS STATE: Within federal guidelines: each state establishes: eligibility scope
- 38. Medicaid varies considerably among states
- 39. Who Pays for Medicaid? Total of $329 billion Federal funds (out of general budget funds) pays
- 40. Medicaid Financial Problems States pay on average 21% of total state budgets on Medicaid Costs of
- 42. Medicaid Constituency 58 million people receive Medicaid – Some receive both Medicare and Medicaid
- 43. Elderly and Medicaid
- 44. Medicaid & Nursing Homes 34% of Medicaid funds are spent on nursing home care 15-57 70%
- 45. Likelihood of Needing Long Term Care – Gender and Length of Stay
- 46. Long Term Nursing Care by Age
- 47. Likelihood of Nursing Home The U.S. General Accounting Office reported in 2000 that nearly 40% of
- 48. Medicaid Financial Planning? Medicaid Planning, or the act of shifting assets out of a Medicaid recipient's
- 49. How Poor to Qualify for Medicaid? The government will not pay for nursing home care for
- 50. Policy Issues? Policy Decision to Protect the Assets of Wealthy Seniors? but not the others? Contrast
- 52. Policy Issues Recall History of Law and Poverty, FAMILY RESPONSIBILITY: 3 generation responsibility Tension between: Do
- 53. CHIP CHIP: Children’s Health Insurance Program Structure much like Medicaid Federal / State Partnership States have
- 54. Uninsured in US 46 Million People
- 55. What About Uninsured? Twenty-five percent of all working class families in LA have no health insurance
- 56. Consequences of Lack of Health Insurance (part one) ¨ Uninsured Americans get about half the medical
- 57. Consequences (cont) ¨ Only half of uninsured children visited a physician during 2001, compared with three-quarters
- 58. Consequences (cont) ¨ Tax dollars paid for an estimated 85 percent of the roughly $35 billion
- 59. What Happens When Some of the 46 Million Uninsured Get Sick?
- 60. Uninsured - Conclusion ¨ The United States loses the equivalent of $65 billion to $130 billion
- 62. What Happens When Some of the 46 million Uninsured Get REALLY Sick?
- 64. EMTALA Emergency Medical Treatment and Active Labor Act Anti-Dumping Law, 42 usc 1395dd
- 66. History of EMTALA History: Hill-Burton gave hospitals big $, in return asked for uncompensated care; worked,
- 67. Two Duties on Hospitals 1. appropriate medical screening to determine whether patient has emergency medical condition
- 68. All Hospitals? duty on "participating hospitals" (42 usc 1395dd (e)(2)) Take public funds $ and hospitals
- 69. What Emergency Conditions Must Hospital Treat? Q: whether they have an emergency medical condition? i. health
- 70. If Emergency Condition If so, must stabilize prior to transfer or discharge transfer is allowed if
- 71. Remedies for EMTALA Violations? if violated, civil penalties, atty fees, personal injuries action, but most importantly
- 72. Actual Logo of Personal Injury Firm of Friedman, Domiano and Smith, Cleveland, Ohio
- 73. Who pays for the uninsured do for healthcare? Who pays for the cost of uncompensated care?
- 74. National Academy of Sciences says: ¨ Tax dollars paid for an estimated 85 percent of the
- 75. We Do Have A National Healthcare System: * Private insurance (premiums subject to market) – citizens
- 76. Public Policy Considerations? Is This The Best System? Is This The Least Expensive System? Does This
- 77. US Healthcare System To be continued….
- 79. Скачать презентацию
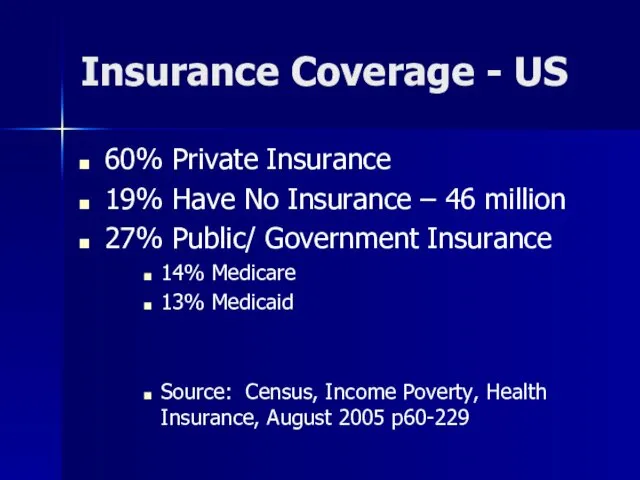
Insurance Coverage - US
60% Private Insurance
19% Have No Insurance –
Insurance Coverage - US
60% Private Insurance
19% Have No Insurance –
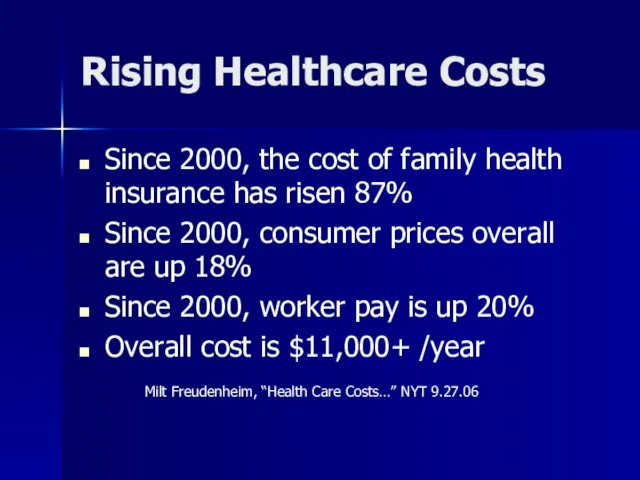
Rising Healthcare Costs
Since 2000, the cost of family health insurance has
Rising Healthcare Costs
Since 2000, the cost of family health insurance has
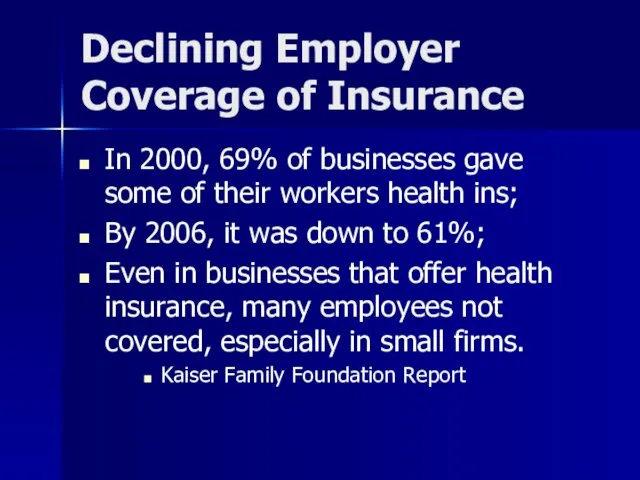
Declining Employer Coverage of Insurance
In 2000, 69% of businesses gave some
Declining Employer Coverage of Insurance
In 2000, 69% of businesses gave some
Medicare
What is it?
What kind of law is it?
How is a person
Medicare
What is it?
What kind of law is it?
How is a person
What is Medicare?
Federal Law
Medicare is a nationwide federal health insurance program
What is Medicare?
Federal Law
Medicare is a nationwide federal health insurance program
Eligibility for Medicare
Depends on part
Part A- hospital insurance
almost all persons over
Eligibility for Medicare
Depends on part
Part A- hospital insurance
almost all persons over
What is Medicare Benefit?
Very much like insurance with co-pays, deductibles, etc.
What is Medicare Benefit?
Very much like insurance with co-pays, deductibles, etc.
Administration of Medicare?
CMS, within the Dept of Health and Human Services;
Administration of Medicare?
CMS, within the Dept of Health and Human Services;
Who pays for Medicare?
Part A: recips pay a deductible
Financed by HI,
Who pays for Medicare?
Part A: recips pay a deductible
Financed by HI,
What is Medicare’s Constituency?
Over 41 million people enrolled in Medicare as
What is Medicare’s Constituency?
Over 41 million people enrolled in Medicare as
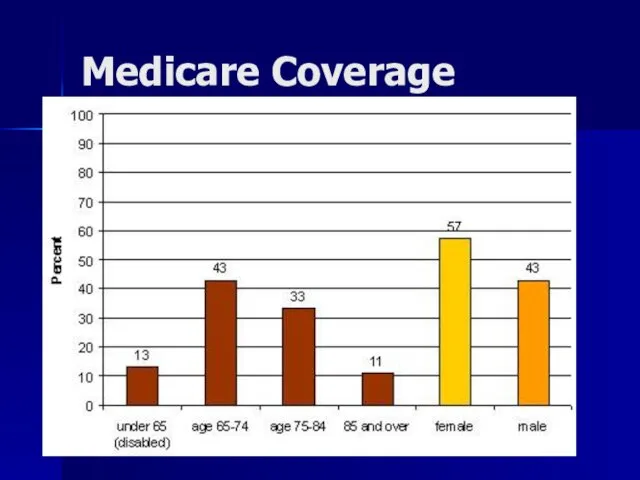
Medicare Coverage
Medicare Coverage
Medicare History
Enacted in 1965, the Medicare program immediately covered 19.1 million
Medicare History
Enacted in 1965, the Medicare program immediately covered 19.1 million
Medical Care in Other Countries
In 1883, Germany passed a sickness insurance
Medical Care in Other Countries
In 1883, Germany passed a sickness insurance
Who are collateral beneficiaries?
Who are collateral beneficiaries?
:
Where Do Medicare Dollars Go?
:
Where Do Medicare Dollars Go?
How Much Does Medicare Cost?
2006 Estimate $345 billion
2004 was $283 billion
1999
How Much Does Medicare Cost?
2006 Estimate $345 billion
2004 was $283 billion
1999

New Medicare Benefit
Prescription Drug Coverage
New Medicare Benefit
Prescription Drug Coverage
Medicare Drug Benefit Choices
From January 2006 beneficiaries can choose to
(a)
Medicare Drug Benefit Choices
From January 2006 beneficiaries can choose to
(a)
Medicare Drug Benefits
Enrollees will have an annual deductible of $250,
an
Medicare Drug Benefits
Enrollees will have an annual deductible of $250,
an
Annual deductible of $250;
Premium of $35 a month (may vary in
Annual deductible of $250;
Premium of $35 a month (may vary in
Low-Income Drug Subsidies:
People eligible for Medicaid and Medicare will pay no
Low-Income Drug Subsidies:
People eligible for Medicaid and Medicare will pay no
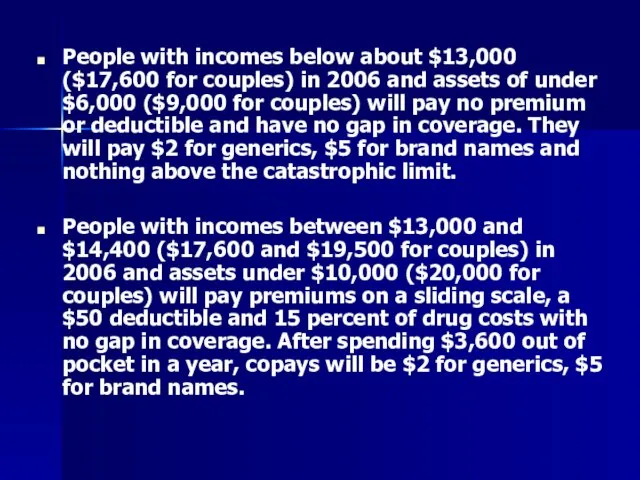
People with incomes below about $13,000 ($17,600 for couples) in 2006
People with incomes below about $13,000 ($17,600 for couples) in 2006
2007 Medicare Changes:
The Part B premium will be linked to
2007 Medicare Changes:
The Part B premium will be linked to
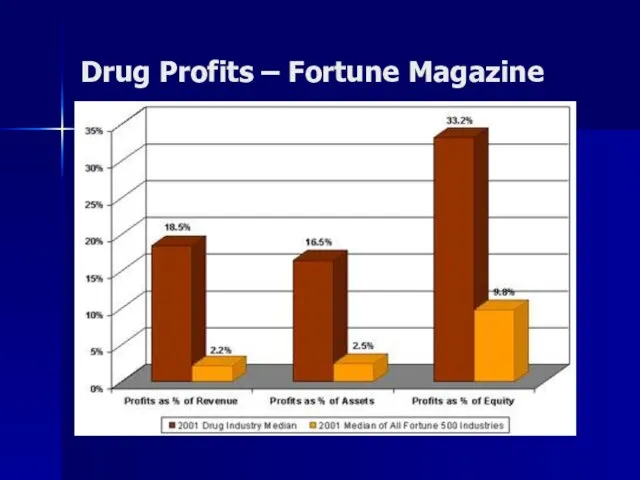
Drug Profits – Fortune Magazine
Drug Profits – Fortune Magazine
Medicaid
What is it?
What kind of law is it?
How is a person
Medicaid
What is it?
What kind of law is it?
How is a person
Medicaid
A federal-state program providing medical assistance to low-income persons who are
Medicaid
A federal-state program providing medical assistance to low-income persons who are
Medicaid Law
Joint Federal and State Law
Medicaid Law
Joint Federal and State Law
Eligibility for Medicaid
FINANCIAL REQUIREMENTS:
First must be indigent
Income and
Resources
Eligibility for Medicaid
FINANCIAL REQUIREMENTS:
First must be indigent
Income and
Resources
Eligibility Medicaid: Mandatory
Families Aid to Families with Dependent Children (AFDC);
Supplemental
Eligibility Medicaid: Mandatory
Families Aid to Families with Dependent Children (AFDC);
Supplemental
What benefit is conferred?
MUST OFFER:
inpatient
outpatient
nursing home care
MAY OFFER:
eyeglasses
prescription drugs
What benefit is conferred?
MUST OFFER:
inpatient
outpatient
nursing home care
MAY OFFER:
eyeglasses
prescription drugs
Administration of Medicaid
FEDERAL: CMS AND HHS
STATE:
Within federal guidelines:
each state establishes:
eligibility
scope of
Administration of Medicaid
FEDERAL: CMS AND HHS
STATE:
Within federal guidelines:
each state establishes:
eligibility
scope of
Medicaid varies considerably among states
Medicaid varies considerably among states
Who Pays for Medicaid?
Total of $329 billion
Federal funds (out of general
Who Pays for Medicaid?
Total of $329 billion
Federal funds (out of general
Medicaid Financial Problems
States pay on average 21% of total state budgets
Medicaid Financial Problems
States pay on average 21% of total state budgets
Medicaid Constituency
58 million people receive Medicaid –
Some receive both Medicare
Medicaid Constituency
58 million people receive Medicaid –
Some receive both Medicare

Elderly and Medicaid
Elderly and Medicaid
Medicaid & Nursing Homes
34% of Medicaid funds are spent on nursing
Medicaid & Nursing Homes
34% of Medicaid funds are spent on nursing
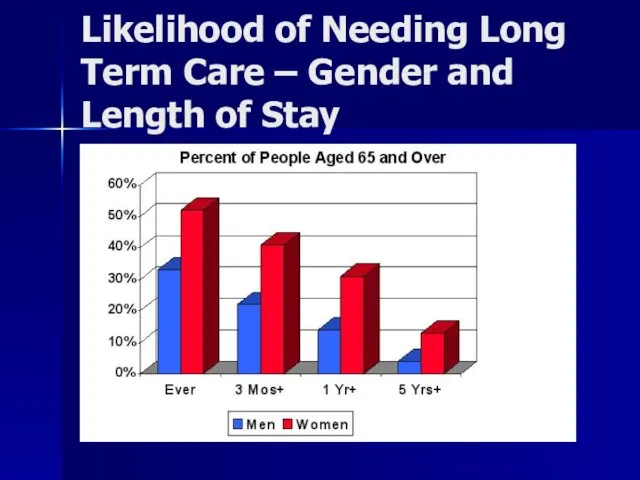
Likelihood of Needing Long Term Care – Gender and Length of
Likelihood of Needing Long Term Care – Gender and Length of
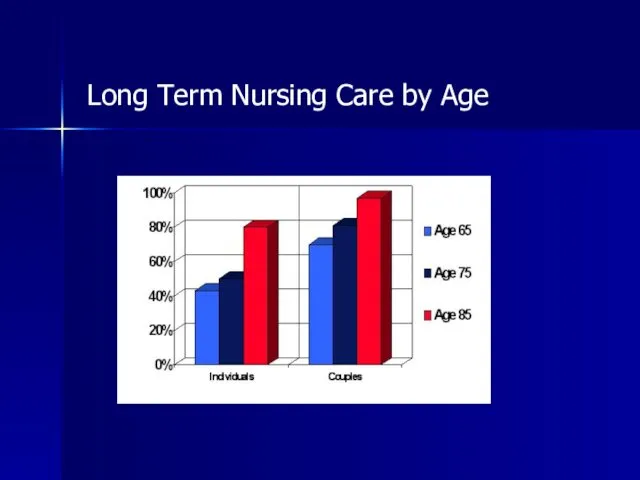
Long Term Nursing Care by Age
Long Term Nursing Care by Age
Likelihood of Nursing Home
The U.S. General Accounting Office reported in
Likelihood of Nursing Home
The U.S. General Accounting Office reported in
Medicaid Financial Planning?
Medicaid Planning, or the act of shifting assets out
Medicaid Financial Planning?
Medicaid Planning, or the act of shifting assets out
How Poor to Qualify for Medicaid?
The government will not pay for
How Poor to Qualify for Medicaid?
The government will not pay for
Policy Issues?
Policy Decision
to Protect the Assets of Wealthy Seniors?
but not
Policy Issues?
Policy Decision
to Protect the Assets of Wealthy Seniors?
but not
Policy Issues
Recall History of Law and Poverty, FAMILY RESPONSIBILITY: 3 generation
Policy Issues
Recall History of Law and Poverty, FAMILY RESPONSIBILITY: 3 generation
CHIP
CHIP: Children’s Health Insurance Program
Structure much like Medicaid
Federal / State Partnership
States
CHIP
CHIP: Children’s Health Insurance Program
Structure much like Medicaid
Federal / State Partnership
States
Uninsured in US
46 Million People
Uninsured in US
46 Million People
What About Uninsured?
Twenty-five percent of all working class families in LA
What About Uninsured?
Twenty-five percent of all working class families in LA
Consequences of Lack of Health Insurance (part one)
¨ Uninsured Americans
Consequences of Lack of Health Insurance (part one)
¨ Uninsured Americans
Consequences (cont)
¨ Only half of uninsured children visited a physician during
Consequences (cont)
¨ Only half of uninsured children visited a physician during
Consequences (cont)
¨ Tax dollars paid for an estimated 85 percent of
Consequences (cont)
¨ Tax dollars paid for an estimated 85 percent of
What Happens When Some of the 46 Million Uninsured Get Sick?
What Happens When Some of the 46 Million Uninsured Get Sick?
Uninsured - Conclusion
¨ The United States loses the equivalent of $65
Uninsured - Conclusion
¨ The United States loses the equivalent of $65

What Happens When Some of the 46 million Uninsured Get REALLY
What Happens When Some of the 46 million Uninsured Get REALLY
EMTALA
Emergency Medical Treatment and Active Labor Act
Anti-Dumping Law, 42 usc
EMTALA
Emergency Medical Treatment and Active Labor Act
Anti-Dumping Law, 42 usc

History of EMTALA
History: Hill-Burton gave hospitals big $, in return asked
History of EMTALA
History: Hill-Burton gave hospitals big $, in return asked
Two Duties on Hospitals
1. appropriate medical screening to determine whether patient
Two Duties on Hospitals
1. appropriate medical screening to determine whether patient
All Hospitals?
duty on "participating hospitals" (42 usc 1395dd (e)(2))
Take public funds
All Hospitals?
duty on "participating hospitals" (42 usc 1395dd (e)(2))
Take public funds
What Emergency Conditions Must Hospital Treat?
Q: whether they have an emergency
What Emergency Conditions Must Hospital Treat?
Q: whether they have an emergency
If Emergency Condition
If so, must stabilize prior to transfer or discharge
transfer
If Emergency Condition
If so, must stabilize prior to transfer or discharge
transfer
Remedies for EMTALA Violations?
if violated, civil penalties, atty fees, personal injuries
Remedies for EMTALA Violations?
if violated, civil penalties, atty fees, personal injuries
Actual Logo of Personal Injury Firm of
Friedman, Domiano and Smith,
Actual Logo of Personal Injury Firm of Friedman, Domiano and Smith,
Who pays for the uninsured do for healthcare?
Who pays for the
Who pays for the uninsured do for healthcare?
Who pays for the
National Academy
of Sciences says:
¨ Tax dollars paid for an estimated
National Academy
of Sciences says:
¨ Tax dollars paid for an estimated
We Do Have A National Healthcare System:
* Private insurance (premiums subject
We Do Have A National Healthcare System:
* Private insurance (premiums subject
Public Policy Considerations?
Is This The Best System?
Is This The Least Expensive
Public Policy Considerations?
Is This The Best System?
Is This The Least Expensive
US Healthcare System
To be continued….
US Healthcare System
To be continued….
 Псевдофакичный КМО (Синдром Ирвина-Гасса)
Псевдофакичный КМО (Синдром Ирвина-Гасса) Психология детей с расстройствами эмоционально-волевой сферы и поведения
Психология детей с расстройствами эмоционально-волевой сферы и поведения Хронический пылевой бронхит
Хронический пылевой бронхит Всё, что вы хотели знать про это. Репродуктивное здоровье подростка
Всё, что вы хотели знать про это. Репродуктивное здоровье подростка Ветеринарно-санитарная экспертиза рыб и рыбопродуктов, меры борьбы и профилактика при гельминтозных заболеваниях
Ветеринарно-санитарная экспертиза рыб и рыбопродуктов, меры борьбы и профилактика при гельминтозных заболеваниях Общая фармакология
Общая фармакология Микст-патология у больных хроническим описторхозом. Тактика ведения
Микст-патология у больных хроническим описторхозом. Тактика ведения Эпидемиологическая ситуация заболеваемости корью. Алгоритм расследования побочных эффектов при вакцинации против кори
Эпидемиологическая ситуация заболеваемости корью. Алгоритм расследования побочных эффектов при вакцинации против кори Аномалии размеров, формы и структуры эмали. Этиология. Клиника. Лечение
Аномалии размеров, формы и структуры эмали. Этиология. Клиника. Лечение Двигательная система. АФО двигательного анализатора. Виды нарушение двигательной чувствительности. Методы исследования
Двигательная система. АФО двигательного анализатора. Виды нарушение двигательной чувствительности. Методы исследования Сенсорні області кори. Роль ретикулярної формації. Ноціцепція. Температурна рецепція
Сенсорні області кори. Роль ретикулярної формації. Ноціцепція. Температурна рецепція Эколого-географические особенности и этиологическая структура лептоспироза животных в Среднем Приобье
Эколого-географические особенности и этиологическая структура лептоспироза животных в Среднем Приобье Правильное и здоровое питание ребёнка
Правильное и здоровое питание ребёнка Геморрой. Предрасполагающие факторы
Геморрой. Предрасполагающие факторы Участие медицинской сестры в профилактике инсульта
Участие медицинской сестры в профилактике инсульта Отравления веществами наркотического действия. Клиника, диагностика, лечение
Отравления веществами наркотического действия. Клиника, диагностика, лечение Семиотика и методы диагностики заболеваний, приводящих к формированию пороков сердца. Ревматизм, бактериальный эндокардит
Семиотика и методы диагностики заболеваний, приводящих к формированию пороков сердца. Ревматизм, бактериальный эндокардит Неспецифический язвенный колит
Неспецифический язвенный колит Методы обезболивания. Виды обезболивания. Аппаратура и инструментарий для проведения анестезии
Методы обезболивания. Виды обезболивания. Аппаратура и инструментарий для проведения анестезии Диагностика и лечение синдрома Гудпасчера
Диагностика и лечение синдрома Гудпасчера Внутрибольничные инфекции. Масштаб, проблемы и структура. Инфекционный процесс
Внутрибольничные инфекции. Масштаб, проблемы и структура. Инфекционный процесс Обмен нуклеотидов. Тема 14
Обмен нуклеотидов. Тема 14 Биоритмология (2)
Биоритмология (2) Vitaminele antiinfectioase
Vitaminele antiinfectioase Железодефицитная анемия у детей. Диспансеризация
Железодефицитная анемия у детей. Диспансеризация Адамның жасы мен жынысына байланысты терінің ерекшеліктері
Адамның жасы мен жынысына байланысты терінің ерекшеліктері Методы исследования больных с заболеваниями органов кроветворения
Методы исследования больных с заболеваниями органов кроветворения Реабилитация при эфферентной моторной афазии
Реабилитация при эфферентной моторной афазии